
Abstract
Background
Epidemiological studies have assessed relationships between circulating levels of fatty acid (FA) and blood pressure (BP), and their results remain controversial. Nevertheless, data are sparse on serum FA as biomarker and BP in China. The aim of the study was to investigate the association between serum FA and BP in Chinese populations.
Methods
We conducted a cross-sectional study nested within a community-based cohort of 2447 Chinese participants aged 35–79 years who completed a baseline assessment between October 2012 and April 2013. Baseline assessment included the collection of fasting blood samples, anthropometric measurements and a personal interview using a validated questionnaire. Serum FA was determined by gas-liquid chromatography. Exploratory factor analyses were employed to identify FA-factor as a reflection of serum FA pattern. A multiple regression model was conducted to estimate adjusted mean of BP with 95 % confidence interval (CI) by tertile groups of the generated FA-factor scores.
Results
Hypertensive patients have significantly higher serum 14:0, 16:0, 16:1n-7, 18:3n-6, 20:3n-6 and Δ6-desaturase index (18:3n-6/18:2n-6) as well as lower 18:2n-6, 22:6n-3 and Δ5-desaturase index (20:4n-6/20:3n-6) compared with normotensive participants. Factor 1 (low linoleic acid/high saturated FA pattern: 14:0, 16:0, 16:1n-7, 18:2n-6, 18:3n-6, 20:3n-6) and Factor 2 (n-3 PUFA pattern: 20:5n-3, 22:5n-3, 22:6n-3, 18:1n-9) were identified as indicators of the serum FA pattern. After adjustment for age, gender, body mass index, hypertension treatment, smoking, alcohol intake, education, profession, exercise habit, salt intake, family history of hypertension, heart rate, blood lipids and fasting blood-glucose levels, per a standard deviation (SD) increment of Factor 1 scores was associated with an increment of 2.44 (95 % CI: 1.73, 3.15) mm Hg for systolic BP, whereas per a SD increment of Factor 2 scores was associated with a reduction of 1.40 (95 % CI: 0.80, 2.04) mm Hg for diastolic BP.
Conclusions
The serum FA pattern characterized by low proportions of 14:0, 16:0, 16:1n-7 and 18:3n-6 as well as high 18:2n-6 and 22:6n-3 was beneficially associated with BP levels in this Chinese population. This evidence well supports the current dietary recommendations in the communities to replace saturated fat with polyunsaturated fat.
Similar content being viewed by others

Background
Adverse blood pressure (BP) levels remain a major public-health problem worldwide, and almost 2.11 million cardiovascular deaths are attributable to greater BP in China annually [1]. Data from meta-analyses [2, 3] and clinical trials [4, 5] have suggested that n-3 polyunsaturated fatty acid (PUFA) supplement can dose-dependently lower BP in hypertensive patients but not in normotensive individuals. A large-scale, population-based International Study of Macro/Micronutrients and Blood Pressure (INTERMAP) suggested that dietary intake of n-3 PUFA was inversely associated with BP levels in middle-aged normotensive persons [6]. However, its potential limitations are likely to be dietary measurement errors or bias with consequent limited ability to classify dietary intake of individuals accurately and underestimation of effect size attributable to limited reliability in dietary estimations.
In contrast to dietary questionnaires, FA levels in circulating blood can provide objective measures that reflect both dietary consumption and relevant biological processes. Additionally, FA biomarker can also permit direct evaluation of individual FA that may have different effects on certain biological pathways or clinical end points. Examples of this have been reported that circulating levels of PUFA were significantly correlated with intake of polyunsaturated fat [7], while circulating levels of 14:0, 16:0, 18:0 and monounsaturated FA (MUFA) may reflect a diet rich in saturated fat, because of their high correlations with saturated fat [8]. Prior observational studies examined associations between serum/plasma FA as biomarker and BP, and their finding were controversial [9–11]. Possible reasons for the inconsistencies across studies may be BP measurements insufficiently standardized and small sample sizes with a low statistical power. Recently, a large-scale longitudinal study of erythrocyte FA in relation to BP change in 1834 middle-aged and elderly Chinese individuals indicated that erythrocyte long-chain (LC) n-3 PUFA was associated reduced BP levels of individuals [12]. However, the small changes in BP and relatively great errors in BP measurements during follow-up would substantially attenuate the FA-BP associations. Additionally, the amount of each FA is often expressed as a proportion and is a relative measure, which means that many of individual FA are inter-related. A change in the proportion of any specific FA will influence the proportions of several others in blood, which was likely to bias the true association between individual FA and BP. Thus, the association between circulating levels of FA as biomarker and BP of individuals merit further study.
We therefore attempted to employ a method of exploratory factor analyses to identify the specific FA-factors as an indicator of FA patterns [13]. Totally, 2447 community-dwellers (1153 males and 1294 females) aged 35–79 years living in Zhejiang Province, southeast China were recruited through a cross-sectional study nested with in a community-based cohort. The aim of the study was to investigate the association between serum FA patterns and BP levels in this middle-aged and elderly Chinese population.
Methods
Study design
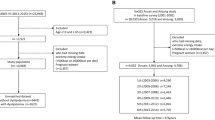
The cross-sectional study with baseline data was conduced within a community-based cohort (Zhejiang Prospective Investigation into Hypertension and Lifestyle, ZPIHL). The study protocol was approved by the Ethics Committee, Zhejiang Hospital, China. All subjects provided their written consent prior to participation in the study. The detailed methods for participant selection are presented elsewhere [14]. Briefly, study participants were recruited from 6 community health centers across 12 counties located in Zhejiang Province, southeast China. Zhejiang province is a well development region with a good medicare system even in remote areas. Totally, 3,500 individuals aged 35–79 years were invited between April and October 2012. Participants are all local Chinese residents, and their complete healthy/medical records were documented in the local community hospitals. To define study participants, we excluded anyone who has no complete medical record, and meet any of the following items: myocardial infarction, coronary heart disease, peripheral vascular disease, angina, cancer, dementia, schizophrenia, deaf or dumb, < 35 years, less than 6 months of living in the local communities. Finally, 3,017 participants with complete health records agreed to participate in the study. Baseline assessment included the collection of fasting blood samples, anthropometric measurements and a personal interview using a validated questionnaire about medical history, socio-demographic and lifestyle characteristics between October 2012 and April 2013. Of those, 2,535 subjects provided fasting blood samples and completed a laboratory assessment, with a participation rate of 84.02 % (2535/3017). Subjects with missing values (n = 56) or implausible data (n = 19) on lifestyle factors from the structured questionnaire and with unreliable data on serum FA (n = 13) were excluded. Afterwards, 2,447 participants (1,153 males and 1,294 females) were finally remained for baseline analyses.
Questionnaire interview
A face-to-face interview was conducted by trained interviewers using a validated questionnaire. We collected data on socio-demographic, medical history, and lifestyle factors. Education levels were categorized as primary (duration of education < 9 years), secondary (9–12 years) and high (>12 years). High-salt intake was defined as salt consumption with > 6 g per day [15]. Regular exercisers were those who sported ≥ 3 times per week for over 6 months. Current smokers were those who smoked ≥18 packs per year, while current drinkers were those who consumed alcoholic beverage ≥ 25 g per day.
Measurements of anthropometric parameters and blood pressure
Anthropometrical measurements were performed by trained nurses using standard protocols. Body weight (kg) and height (m) were measured with participants wearing no shoes and light clothing. Body mass index (BMI) was calculated as the participant’s weight (kg) divided by the square of standing height (m). Before heart rate (HR, beat/min) and blood pressure (BP, mm Hg) measurements, participants were advised to avoid consuming alcohol or tobacco, ingesting tea or coffee, and engaging in exercise for at least 30 min. A standardized mercury sphygmomanometer was used to measure BP by trained physicians, and one of three cuff sizes (regular adult, large or thigh) was chosen based on the circumference of the participant’s arm. BP and HR for each subject were defined as the average of three measurements performed in the subject in sitting position with 2-min intervals at that visit. Prevalent hypertension was ascertained by meeting 1 of 2 criteria: (a) a new physician diagnosis of hypertension (an average systolic BP (SBP) ≥ 140 mm Hg and/or an average diastolic BP (DBP) ≥ 90 mmHg); or (b) self-reported treatment of hypertension with anti-hypertensive drugs.
Laboratory assessment
Fasting blood samples were collected in tubes with serum separator gel. They were left at room temperature for 30 min and then centrifuged at 2500 RCF (g) for 15 mins to isolate serum. Measurement of fasting serum triglycerides (TG), total cholesterol (TC) and glucose (Fbg) levels were determined by standard procedures at the biochemistry laboratory of Zhejiang Hospital. The remaining serum samples were aliquoted into separate tubes (1 mL) and stored at -80 0C until further FA analyses.
Frozen samples were thawed on ice for 40 mins. The total lipid content of the serum was extracted with solvents. The methyl esters of FA in serum were prepared by saponification, and serum compositions of FA were determined by gas-liquid chromatography (GLC) as described previously [16]. The main sources of serum FA are derived from cholesterol esters, phospholipids, and triglycerides. The amount of individual FA was expressed as a percentage of total FA in serum.
Statistical analysis
Statistical analyses of all the data were performed by STATA version 11.0 (Stata CORP, College Station, TX). Descriptive statistics was initially conducted. The distribution of continuous variables was examined for normality by Shapiro-Wilk’s test. Continuous data with the normal distribution were expressed as the mean (standard deviation), while categorical data were expressed as a proportion. The skewed data were expressed as the median (quartile range), and were log-transformed before statistic analyses. Difference in the continuous and categorical variables between two groups was examined by Student’s t-test and chi-square test, respectively. Factor analysis has been a multivariate statistical tool of dimension-reduction to study FA patterns [13], which can be performed to address inter-relations between individual FA content. Individual FA was entered in a factor analysis model followed by variance rotation to identify the specific FA-factors as a measure of FA pattern. The resulting FA-factor pattern was determined by a factor loading, the eigenvalue and the explained proportion of total variance. Factor loading of each individual FA equals the Pearson correlation coefficient between that FA and the generated FA-factor. Factor loading with ≥ |0.40| were considered meaningful for the interpretation of FA-factor [17]. Eigenvalue described the amount of variance attributable to the FA-factors. The powerful FA-factors with eigenvalue > 1 were extracted for further analyses, which explained more than 70 % of the total variance. Factor scores for each FA pattern can be calculated as a sum of the products of factor loading coefficients and the standardized each FA correlated with that FA pattern. To determine if serum FA patterns were associated with BP levels, a multiple regression model was conducted to estimate adjusted mean of BP with 95 % confidence interval (CI) by tertile groups of the generated FA-factor scores. The ordinal numbers 0–2 was assigned to the tertile (T) categories of FA-factor scores, and then a linear trend test was performed by treating the ordinal score variable as a continuous variable in the models. The dependent variables (SBP and DBP), biochemical parameters (TC, TG, and Fbg levels) and anthropometrical data (HR and BMI) were continuous, while socio-demographic (age (≤55, >55), gender, profession (manual, non-manual), and education levels), lifestyle data (smoking habit (current, former/never), alcohol consumption (current, former/never), high-salt diet (yes, no)) and family history of hypertension (yes, no) as the independent variables were categorical. Initial model was adjusted for age, gender, BMI and hypertension treatment; model 1 was adjusted for the covariates in model 1 plus lifestyle factors; model 2 as a full model was adjusted for the covariates in model 2 plus clinical parameters (family history of hypertension, TC, TG, HR and Fbg levels). In addition, to test the robustness of the findings from factor analyses, a multiple regression analysis was repeated to assess associations of individual FA contributing most to FA-factors with BP levels. All statistic tests were two-sided, and P < 0.05 was considered statistically significant.
Results
Baseline characteristics
Totally, 748 hypertensive patients were identified from 2447 community-dwellers aged 35–79 years who completed baseline measurements. Characteristics of study participants according to BP status are presented in Table 1. All participants are comprised of 1153 males (47.12 %) and 1294 females (52.88 %). The proportion of prevalent hypertension was significantly higher in 1,201 middle-aged than in 1,246 elderly participants. Hypertensive patients likely tended to have primary education levels, non-manual labor, high-salt diet, irregular/never sporters, family history of hypertension, higher BMI, BP, HR, TG, TC and Fbg levels compared with normotensive participants (all P < 0.05).
Serum fatty acid profile between hypertensive and normotensive participants
Difference in individual FA between hypertension patients and normotensive persons was presented in Table 2. Compared with normotensive participants, hypertension patients had significantly higher proportions of serum 14:0, 16:0, 18:0, 22:0,16:1n-7, 18:1n-9, 18:3n-6, 20:3n-6 and Δ6-desaturase index (18:3n-6/18:2n-6) as well as lower 18:2n-6, 22:6n-3 and Δ5-desaturase index (20:4n-6/20:3n-6) (P < 0.05, respectively). In addition, lower proportions of total n-3 PUFA, total PUFA and n-3/n-6 ratio as well as higher total SFA and SFA/PUFA ratio in serum were observed in the hypertension patients than in the normotensive participants (P < 0.05, respectively).
Factor analysis of individual FA
Serum compositions of individual FA and rotated factor loadings of the extracted FA-factors were presented in Table 3. The two major FA-factors can be interpreted as a reflection of serum FA patterns, which explained about 68.73 % of individual FA-related variance. Factor 1 as the most powerful factor (eigenvalue = 3.20), termed “low linoleic acid (LA)/high SFA pattern”, comprised a strongly negative loading from 18:2n-6 (linoleic acid) and higher positive loadings from14:0, 16:0, 16:1n-7, 18:1n-9 and 18:3n-6. These non-essential FA can be synthesized endogenously in response to a high intakes of saturated fat. [8] Factor 2 was defined as “n-3 PUFA pattern” (eigenvalue = 1.95), which mainly comprised higher positive loadings from 20:5n-3, 22:5n-3 and 22:6n-3 as well as a strongly negative loading from 18:1n-9.
Serum FA pattern and BP levels
Adjusted mean of SBP and DBP with 95 % CI by tertile groups of the generated FA-factor scores was presented in Table 4. After adjustment for age, gender, BMI, and hypertension treatment, SBP and DBP levels were significantly increased in participants in the upper tertiles of Factor 1 scores (low LA/high SFA pattern: 14:0, 16:0, 16:1n-7, 18:2n-6, 18:3n-6) compared with those in the bottom tertiles (P for trend = 0.006 and 0.019, respectively). Additional adjustment for lifestyle factors (model 1) did not obviously alter theses results (P for trend < 0.007 and = 0.038, respectively). Even after additional adjustment for family history of hypertension, HR, TC, TG, Fbg levels (model 2), the association remained significant, with each a SD increment of Factor 1 score associated with an increment of 2.44 (95 % CI: 1.73, 3.15) mm Hg for SBP and 1.46 (95 % CI: 0.70, 2.22) mm Hg for DBP, respectively. By contrast, participants in the upper tertiles of Factor 2 scores (n-3 PUFA pattern: 20:5n-3, 22:5n-3, 22:6n-3 and 18:1n-9) had significantly decreased DBP levels compared with those in the bottom tertiles (P for trend = 0.026). The association slightly attenuated but remain significant in lifestyle-adjusted model 1 (P for trend = 0.042). The results with additional adjustment for clinical factors in model 2 were similar to those of lifestyle-adjusted model 1 (P for trend = 0.037), and per a SD increment of Factor 2 scores was associated with a reduction of 1.40 (95 % CI: 0.80, 2.041) mm Hg for DBP.
The major individual FA and BP levels
Adjusted mean of SBP and DBP with 95 % CI by tertile groups of individual FA composition in serum was presented in Additional file 1: Table S1. After controlling for age, gender, BMI and hypertension treatment, SBP and DBP levels significantly increased with increasing in serum proportions of 16:0, 16:1n-7, 18:1n-9 and 18:3n-6 (all P for trend <0.05), whereas SBP significantly decreased only with 18:2n-6 increasing (P for trend <0.001). Decreased DBP levels were associated with increased proportions of 20:5n-3 and 22:6n-3 (P for trend = 0.017 and 0.010, respectively). Additional adjustment for smoking, drinking, high-salt diet, education and profession (model 1) did not appreciably alter these associations, except for 18:1n-9. The results with additional adjustment for family history, TC, TG, HR and Fbg levels (model 3) were similar to those of model 2. A significant positive association of SBP was observed with 16:0, 16:1n-7 and 18:3n-6 (P for trend = 0.034, 0.006 and 0.024, respectively), whereas an inverse association was observed for 18:2n-6 (P for trend = 0.021). Both SBP and DBP levels were significantly decreased in participants with the top tertiles of 22:6n-3 compared with those with the bottom tertiles (P for trend = 0.032 and 0.024, respectively).
Discussion
In the present study, serum FA profile in hypertensive participants has been found to be typically characterized by higher 14:0, 16:0, 16:1n-7, 18:3n-6, 20:3n-6 and Δ6-desaturase index (18:3n-6/18:2n-6) as well as lower 18:2n-6, 22:6n-3 and Δ5-desaturase index (20:4n-6/20:3n-6) compared with normotensive participants. Factor analyses showed that Factor 1 (low LA/high SFA pattern: 14:0, 16:0, 16:1n-7, 18:3n-6, 18:2n-6) and Factor 2 (n-3 PUFA pattern: 20:5n-3, 22:5n-3, 22:6n-3, 18:1n-9) were identified as an indicator of the serum FA pattern. Serum low LA/high SFA pattern was adversely associated with both SBP and DBP, whereas n-3 PUFA pattern was beneficially associated with DBP. These associations cannot be apparently altered even after adjustment for age, gender, BMI, hypertension, lifestyle and clinical factors. Such findings further build and extend on the relationship between serum FA as biomarker and BP levels in Chinese.
A prior cross-sectional study of 1081 urban Italian women aged 20–69 years [18] and a large prospective cohort study of 4652 subjects aged 35–63 years from France [19] suggested that no significant association was found between intake of n-3 PUFA and BP levels. A possible explanation would be underestimated association due to diet assessment errors and recall bias during a dietary questionnaire. In contrast, circulating levels of individual FA can reflect both dietary consumption and relevant biological processes, which can be regarded as a helpfully complementary tool for food frequency questionnaire (FFQ) to closely assess diet intakes. Previous studies of FA biomarkers suggested that increased BP levels were associated with a high content of SFA and low n-3 PUFA in blood [11, 20, 21]. Nevertheless, to date, data of serum/plasma FA in relation to BP levels of individuals are scarce in China. Accumulating evidence has showed that a serum FA pattern characterized by high proportions of 16:0, 16:1n-7, 20:3n-6 and low 18:2n-6 was associated with stroke [22] and left ventricular hypertrophy [23]. In agreement with the previous findings, we found that the serum low LA/high SFA pattern was strongly associated with increased SBP. It is known that dyslipidemia and BMI were associated with greater BP levels [24, 25]. Increased levels of blood TG can damage endothelial function mediated by nitric oxide production as well as accelerate structural changes in large arteries [26]. A higher BMI can increase BP through elevated cardiac output, expanded blood volume, and boosted peripheral vascular resistance [27]. However, the positive association of low LA/high SFA pattern with BP levels did not apparently altered even after additional adjustment for these cardiometabolic risk factors in the present study. Accordingly, we speculated that the adverse effects might be attributable to the main contribution made by individual 16:0, 16:1n-7 and 18:3n-6. The multivariable analysis of tertile groups of individual FA showed that SBP levels trend to increase as increasing in serum composition of 16:0, 16:1n-7 and 18:3n-6, which was concordant with results from many investigators of circulating individual FA in relation to BP [9, 10, 28]. Serum SFA and MUFA may be highly correlated with dietary intakes of saturated fat in persons that consumed a high-SFA diet [7]. Circulating levels of 18:3n-6 trend to increase on a high-SFA diet, possibly because dietary saturated FA can influence enzymes involved in its metabolism [29]. Thus, the serum FA pattern characterized by high 16:0, 16:1n-7, 18:3n-6 and 20:3n-6 as well as low 18:2n-6 perhaps reflected a diet high in saturated fat relative to polyunsaturated fat in this middle-aged and elderly Chinese population.
Current American Heart Association dietary guidelines for CVD prevention in the community recommends an increase in both n-6 and n-3 PUFA consumption together with a reduction in SFA. A cross-sectional study conducted in Guangzhou, China has reported that erythrocyte compositions of long-chain n-3 PUFA was associated with reduction of BP levels in a general Chinese population [12]. In line with the study, our data indicated that participants in the upper tertiles of serum 22:6n-3 had significantly decreased BP levels compared with those in the bottom tertiles, which cannot be altered even by multiple adjustments. We therefore still suggest that higher intakes of food n-3 FA will increase exposure in vivo, which can favorably influence BP levels for Chinese persons. Nevertheless, the beneficial impacts by serum n-3 PUFA pattern were not observed on SBP levels with additional adjustment for possible confounders. We also found that no significant association of BP with individual 18:1n-9 in the multivariate-adjusted model. Thus, a possible explanation was that the lower-SBP effects by n-3 PUFA may be offseted by a strongly negative determinant from 18:1n-9 in n-3 PUFA factor. These observed associations together support that the key to dietary fat consumption benefits for BP levels lies not only in supplementations of its quantity, but also in the improvement in its quality.
There is a large number of evidence to suggest that the opposing effects of dietary saturated fat and polyunsaturated fat on BP levels. Dietary saturated fat can adversely influence BP levels by increasing oxidative stress and decreasing nitric oxide (NO) production within the endothelium [30]. Alterations in the metabolism of PUFAs might be a predisposing factor to the development of essential hypertension [31–33]. A case-control study of plasma phospholipids FA profile analysis revealed that higher 16:0, 18:0, 18:3n-6 and lower 18:2n-6 were found in hypertensive patients compared to normal controls [33]. Similar to results from the study, a significant difference in serum FA profile was found between hypertensive and normotensive individuals in the present study, and we also found that Δ6-desaturase index was markedly higher, but Δ5-desaturase index was lower in hypertension patients compared with normotensive persons, suggesting that essential FA and their metabolites may play an important role in the pathobiology of hypertension [34]. Our study indicated that the hypertensive patients consumed lower 18:2n-6 than normal, which was supported by a study by McCarron et al [35]. 18:2n-6 can be converted to 18:3n-6 by Δ6-desaturase in human body, which may be modified by dietary nutrients (e.g., magnesium) as cofactors [32]. 20:5n-3 can block the activity of Δ5-desaturase such that 20:4n-6 levels in tissue will be low. 20:4n-6 can form the precursor of 2-series of PGs that stimulates vascular constriction and smooth muscle contraction, whereas 20:5n-3 is precursor of PGI3 and thromboxane A3 that have been reported to be less active. Thus, increased consumption of marine food rich in 20:5n-3 and 22:6n-3 can competitively inhibit hepatic Δ5-desaturase to reduce circulating levels of metabolites from 20:4n-6 such as PGF2aand thromboxane A2 [36]. Possible mechanisms whereby n-3 FA may favorably influence BP may be multifactorial involving improvements in endothelial vasodilator function [37, 38], reactivity of resistant vessel vascular smooth muscles [39] and arterial compliance [40], along with a cardiac effect mediated by a decrease in heart rate to provide an energy-sparing promotion of diastolic relaxation [41]. In addition, BP and cardiac β-adrenergic receptor responsiveness decreased on a low-fat diet with a high ratio of PUFA/SFA (P/S) [42]. However, the P/S ratio and total dietary fat are often altered in diet, and thus the oppositive mechanisms between saturated fat and polyunsaturated fat have not yet been understood and remain to be further elucidated.
Dietary nutrients as cofactors are necessary for the formation of potent platelet anti-aggregators and vasodilators such as prostaglandin E1 (PGE1) and PGI3, which can prevent the development of hypertension [32]. Lower magnesium can reduce the Δ 6-desaturase activity, leading to an inadequate the conversion of 20:3n-6 to PGE1 [43]. Vitamin C can improve nitric oxide (NO) production and enhance the synthesis of PGE1 in hypertension [44, 45]. Many studies found that higher intake of salt can lead to BP, but sodium seems to act in concert with other nutrients such as calcium, potassium, magnesium, vitamin C, and antioxidants present in fruits and vegetables act together to determine the ultimate degree of BP by regulating the release of PGE1, PGI2 and NO production [32, 46]. We found that higher intake of salt was present in hypertension patients compared with normotensive participants, which was supported by the observation that plasma NO levels decreased in patients with hypertension after salt loading [47], suggesting that excess salt intake can reduce NO production from the endothelial cells in patients with salt-sensitive hypertension. However, we was unable to exclude the effects of total energy intake or the consumption of PUFAs, saturated fats, trans-fats and other food nutrients on BP in the study population, as dietary intakes were not assessed at baseline. A dietary survey of middle-aged nutrient intake in East (China and Japan) Asian and Western (UK and US) persons revealed that Chinese sample population has lower intake of total fat, saturated fat, trans-fatty acid, potassium, vitamin C and calcium as well as higher sodium and sodium/potassium ratio compared to western persons, whereas no marked difference in dietary intake of magnesium were found between the two populations [48]. In addition, peroxidation of unsaturated FA such as 18:3n-3 can result in the formation of aldehydes such as 4-hydroxypentenal causing both hypertension and oxidative stress. Superoxide anion can inactivate PGI2 and NO [49], which can lead to elevated BP by an increase in peripheral vascular resistance. Evidence indicated that the superoxide dismutase activity and vitamin E concentration were found to be lower, whereas plasma superoxide anion and lipid peroxides were found to be higher in patients with uncontrolled hypertension [44, 50]. Thus, the interaction among free-radical, NO, PUFAs, antioxidants and other dietary nutrients on BP in the study population may be helpful for understanding the aetiopathogenesis of hypertension, but its mechanism is presently unclear [51, 52]. Further studies were merited to clarify the biological plausibility related to PUFAs interaction with free radicals, NO and other nutrients in the development of hypertension.
Many a strengths should be highlighted in our study. Firstly, we used a method of exploratory factor analyses to identify the major FA-factors as indicators of serum FA patterns, facilitating the interpretation of the findings. Additionally, the amount of exogenous and endogenous FA can be closely represented by serum FA, independent of diet records and recalls bias. However, the potential limitations were likely to bias the endings. Firstly, the causal relations cannot be determined. Secondly, we cannot affirm that a dietary pattern of low LA/high SFA can unfavorably influence BP levels, because data are lacking on food FA and BP. Thirdly, the part of the positive association between BMI and BP may depend on dietary fat intakes, considering that BMI is a strong determinant of BP levels. It may be questioned whether controlling for BMI in the multivariate model is appropriate when assessing the strength of the linear association. Fourthly, all participants were recruited from the communities in Zhejiang province located in southeast China, which did not perfectly represent a random sample of a general Chinese population. Thus, caution is required in generalizing the current results to the whole middle-aged and elderly Chinese. Fifthly, participants with prevalent hypertension were identified by self-reported information on anti-hypertensive drugs use, which might be subject to report bias. Sixthly, the clear association between FA-factors and BP can be drawn in the present study, possibly because limited community-dwellers living in the same regions are those who have a similar life style. Thus, it is necessary to further demonstrate whether these effects of individual FA on BP can be general in Chinese adults. Finally, we cannot exclude the possibility that the unknown or incompletely measured valuables modified the findings.
Conclusions
In conclusion, the serum FA pattern characterized by low proportions of 16:0, 16:1n-7 and 18:3n-6 as well as high 18:2n-6 and 22:6n-3 was associated with reduced BP levels in this middle-aged and elderly Chinese population. Such evidence well supports the current dietary recommendations in the communities to replace saturated fat with polyunsaturated fat. A well-designed cohort study is further needed to prospectively confirm the effects of individual FA in circulating blood on BP levels in a larger Chinese population.
Abbreviations
- FA:
-
fatty acid
- BP:
-
blood pressure
- PUFA:
-
polyunsaturated fatty acid
- MUFA:
-
monounsaturated fatty acid
- LC:
-
long-chain
- BMI:
-
body mass index
- HR:
-
heart rate
- SBP:
-
systolic blood pressure
- DBP:
-
diastolic blood pressure
- TG:
-
Triglycerides
- TC:
-
total cholesterol
- Fbg:
-
fasting blood-glucose levels
- GLC:
-
gas-liquid chromatography
- CI:
-
confidence interval
- FFQ:
-
food frequency questionnaire
- SFA:
-
Saturated fatty acid
- LA:
-
linoleic acid
- NO:
-
nitric oxide
- P/S:
-
PUFA/SFA
References
He J, Gu D, Chen J, Wu X, Kelly TN, Huang JF, Chen JC, Chen CS, Bazzano LA, Reynolds K, et al. Premature deaths attributable to blood pressure in China: a prospective cohort study. Lancet. 2009;374:1765–72.
Miller PE, Van Elswyk M, Alexander DD. Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and blood pressure: a meta-analysis of randomized controlled trials. Am J Hypertens. 2014;27:885–96.
Morris MC, Sacks F, Rosner B. Does fish oil lower blood pressure? A meta-analysis of controlled trials. Circulation. 1993;88:523–33.
Root M, Collier SR, Zwetsloot KA, West KL, McGinn MC. A randomized trial of fish oil omega-3 fatty acids on arterial health, inflammation, and metabolic syndrome in a young healthy population. Nutr J. 2013;12:40.
Wang S, Ma AQ, Song SW, Quan QH, Zhao XF, Zheng XH. Fish oil supplementation improves large arterial elasticity in overweight hypertensive patients. Eur J Clin Nutr. 2008;62:1426–31.
Ueshima H, Stamler J, Elliott P, Chan Q, Brown IJ, Carnethon MR, Daviglus ML, He K, Moag-Stahlberg A, Rodriguez BL, et al. Food omega-3 fatty acid intake of individuals (total, linolenic acid, long-chain) and their blood pressure: INTERMAP study. Hypertension. 2007;50:313–9.
Nikkari T, Luukkainen P, Pietinen P, Puska P. Fatty acid composition of serum lipid fractions in relation to gender and quality of dietary fat. Ann Med. 1995;27:491–8.
Ma J, Folsom AR, Shahar E, Eckfeldt JH. Plasma fatty acid composition as an indicator of habitual dietary fat intake in middle-aged adults. The Atherosclerosis Risk in Communities (ARIC) Study Investigators. Am J Clin Nutr. 1995;62:564–71.
Simon JA, Fong J, Bernert Jr JT. Serum fatty acids and blood pressure. Hypertension. 1996;27:303–7.
Uusitupa MI, Sarkkinen ES, Torpstrom J, Pietinen P, Aro A. Long-term effects of four fat-modified diets on blood pressure. J Hum Hypertens. 1994;8:209–18.
Grimsgaard S, Bonaa KH, Jacobsen BK, Bjerve KS. Plasma saturated and linoleic fatty acids are independently associated with blood pressure. Hypertension. 1999;34:478–83.
Zeng FF, Sun LL, Liu YH, Xu Y, Guan K, Ling WH, Chen YM. Higher erythrocyte n-3 PUFAs are associated with decreased blood pressure in middle-aged and elderly Chinese adults. J Nutr. 2014;144:1240–6.
Warensjo E, Sundstrom J, Lind L, Vessby B. Factor analysis of fatty acids in serum lipids as a measure of dietary fat quality in relation to the metabolic syndrome in men. Am J Clin Nutr. 2006;84:442–8.
Yang L, Xu X, Yan J, Yu W, Tang X, Wu H, Parkin CL. Analysis on associated factors of uncontrolled hypertension among elderly hypertensive patients in Southern China: a community-based, cross-sectional survey. BMC Public Health. 2014;14:903.
Kupferschmidt K. Epidemiology. Report reignites battle over low-salt diets. Science. 2013;340:908.
Li D, Sinclair A, Mann N, Turner A, Ball M, Kelly F, Abedin L, Wilson A. The association of diet and thrombotic risk factors in healthy male vegetarians and meat-eaters. Eur J Clin Nutr. 1999;53:612–9.
Martinez-Vizcaino V, Martinez MS, Aguilar FS, Martinez SS, Gutierrez RF, Lopez MS, Martinez PM, Rodriguez-Artalejo F. Validity of a single-factor model underlying the metabolic syndrome in children: a confirmatory factor analysis. Diabetes Care. 2010;33:1370–2.
Ciocca S, Arca M, Montali A, Fazio S, Bucci A, Angelico F. Lack of association between arterial blood pressure and erythrocyte fatty acid composition in an Italian population sample. Scand J Clin Lab Invest. 1987;47:105–10.
Dauchet L, Kesse-Guyot E, Czernichow S, Bertrais S, Estaquio C, Peneau S, Vergnaud AC, Chat-Yung S, Castetbon K, Deschamps V, et al. Dietary patterns and blood pressure change over 5-y follow-up in the SU.VI.MAX cohort. Am J Clin Nutr. 2007;85:1650–6.
Virtanen JK, Nyantika AN, Kauhanen J, Voutilainen S, Tuomainen TP. Serum long-chain n-3 polyunsaturated fatty acids, methylmercury and blood pressure in an older population. Hypertens Res. 2012;35:1000–4.
Liu JC, Conklin SM, Manuck SB, Yao JK, Muldoon MF. Long-chain omega-3 fatty acids and blood pressure. Am J Hypertens. 2011;24:1121–6.
Fretts AM, Mozaffarian D, Siscovick DS, Sitlani C, Psaty BM, Rimm EB, Song X, McKnight B, Spiegelman D, King IB, Lemaitre RN. Plasma phospholipid and dietary alpha-linolenic acid, mortality, CHD and stroke: the Cardiovascular Health Study. Br J Nutr. 2014;112:1206–13.
Sundstrom J, Lind L, Vessby B, Andren B, Aro A, Lithell H. Dyslipidemia and an unfavorable fatty acid profile predict left ventricular hypertrophy 20 years later. Circulation. 2001;103:836–41.
Sarafidis PA, Bakris GL. Non-esterified fatty acids and blood pressure elevation: A mechanism for hypertension in subjects with obesity/insulin resistance? J Hum Hypertens. 2007;21:12–9.
Laaksonen DE, Niskanen L, Nyyssonen K, Lakka TA, Laukkanen JA, Salonen JT. Dyslipidaemia as a predictor of hypertension in middle-aged men. Eur Heart J. 2008;29:2561–8.
Urbina EM, Srinivasan SR, Kieltyka RL, Tang R, Bond MG, Chen W, Berenson GS. Correlates of carotid artery stiffness in young adults: The Bogalusa Heart Study. Atherosclerosis. 2004;176:157–64.
Palmieri V, de Simone G, Arnett DK, Bella JN, Kitzman DW, Oberman A, Hopkins PN, Province MA, Devereux RB. Relation of various degrees of body mass index in patients with systemic hypertension to left ventricular mass, cardiac output, and peripheral resistance (The Hypertension Genetic Epidemiology Network Study). Am J Cardiol. 2001;88:1163–8.
Cambien F, Warnet JM, Vernier V, Ducimetiere P, Jacqueson A, Flament C, Orssaud G, Richard JL, Claude JR. An epidemiologic appraisal of the associations between the fatty acids esterifying serum cholesterol and some cardiovascular risk factors in middle-aged men. Am J Epidemiol. 1988;127:75–86.
Lasserre M, Mendy F, Spielmann D, Jacotot B. Effects of different dietary intake of essential fatty acids on C20:3 omega 6 and C20:4 omega 6 serum levels in human adults. Lipids. 1985;20:227–33.
Edirisinghe I, McCormick Hallam K, Kappagoda CT. Effect of fatty acids on endothelium-dependent relaxation in the rabbit aorta. Clin Sci (Lond). 2006;111:145–51.
Das UN. Pre(peri)-natal omega-3 PUFA deficiency-induced hypertension and its broader implications. Hypertens Res. 2012;35:375–9.
Das UN. Nutritional factors in the pathobiology of human essential hypertension. Nutrition. 2001;17:337–46.
Das UN. Essential fatty acid metabolism in patients with essential hypertension, diabetes mellitus and coronary heart disease. Prostaglandins Leukot Essent Fatty Acids. 1995;52:387–91.
Das UN. Essential fatty acids and their metabolites in the context of hypertension. Hypertens Res. 2010;33:782–5.
McCarron DA. Biomedicine - Diet and blood pressure the paradigm shift. Science. 1998;281:933–4.
Das UN. Can perinatal supplementation of long-chain polyunsaturated fatty acids prevent hypertension in adult life? Hypertension. 2001;38:E6–8.
Goodfellow J, Bellamy MF, Ramsey MW, Jones CJ, Lewis MJ. Dietary supplementation with marine omega-3 fatty acids improve systemic large artery endothelial function in subjects with hypercholesterolemia. J Am Coll Cardiol. 2000;35:265–70.
Yin K, Chu ZM, Beilin LJ. Blood pressure and vascular reactivity changes in spontaneously hypertensive rats fed fish oil. Br J Pharmacol. 1991;102:991–7.
Nyby MD, Matsumoto K, Yamamoto K, Abedi K, Eslami P, Hernandez G, Smutko V, Berger ME, Tuck ML. Dietary fish oil prevents vascular dysfunction and oxidative stress in hyperinsulinemic rats. Am J Hypertens. 2005;18:213–9.
Chu ZM, Yin K, Beilin LJ. Fish oil feeding selectively attenuates contractile responses to noradrenaline and electrical stimulation in the perfused mesenteric resistance vessels of spontaneously hypertensive rats. Clin Exp Pharmacol Physiol. 1992;19:177–81.
Mozaffarian D, Geelen A, Brouwer IA, Geleijnse JM, Zock PL, Katan MB. Effect of fish oil on heart rate in humans: a meta-analysis of randomized controlled trials. Circulation. 2005;112:1945–52.
Vogel RA, Corretti MC, Plotnick GD. Effect of a single high-fat meal on endothelial function in healthy subjects. Am J Cardiol. 1997;79:350–4.
Das UN. Essential Fatty-Acids - Biology and Their Clinical Implications. Asia Pac J Pharmacol. 1991;6:317–30.
Kumar CA, Das UN. Lipid peroxides, anti-oxidants and nitric oxide in patients with pre-eclampsia and essential hypertension. Med Sci Monit. 2000;6:901–7.
Das UN. Hypertension and ascorbic acid. Lancet. 2000;355:1273–3.
Svetkey LP, Simons-Morton D, Vollmer WM, Appel LJ, Conlin PR, Ryan DH, Ard J, Kennedy BM. Effects of dietary patterns on blood pressure: subgroup analysis of the Dietary Approaches to Stop Hypertension (DASH) randomized clinical trial. Arch Intern Med. 1999;159:285–93.
Fujiwara N, Osanai T, Kamada T, Katoh T, Takahashi K, Okumura K. Study on the relationship between plasma nitrite and nitrate level and salt sensitivity in human hypertension - Modulation of nitric oxide synthesis by salt intake. Circulation. 2000;101:856–61.
Zhou BF, Stamler J, Dennis B, Moag-Stahlberg A, Okuda N, Robertson C, Zhao L, Chan Q, Elliott P, Group IR. Nutrient intakes of middle-aged men and women in China, Japan, United Kingdom, and United States in the late 1990s: the INTERMAP study. J Hum Hypertens. 2003;17:623–30.
Das UN, Repossi G, Dain A, Eynard AR. L-arginine, NO and asymmetrical dimethylarginine in hypertension and type 2 diabetes. Front Biosci Landmark. 2011;16:13–20.
Prabha PS, Das UN, Ramesh G, Kumar KV, Kamalakar V. Free radical generation, lipid peroxidation and essential fatty acids in patients with septicemia. Prostaglandins Leukot Essent Fatty Acids. 1991;42:61–5.
Das UN. Long-chain polyunsaturated fatty acids interact with nitric oxide, superoxide anion, and transforming growth factor-beta to prevent human essential hypertension. Eur J Clin Nutr. 2004;58:195–203.
Das UN. Interaction(s) of Polyunsaturated Fatty Acids With Dietary Protein and Its Relationship to the Pathogenesis of Hypertension. Am J Hypertens. 2010;23:111–2.
Acknowledgements
This study was funded by the Ministry of Science and Technology of China (2014BAI08B01); the Medical research projects in Zhejiang province (2010KJY010); the National Basic Research Program of China (973 Program: 2015CB553604), the National Natural Science Foundation of China (NSFC: 81273054), and the PhD Programs Foundation of Ministry of Education of China (20120101110107). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare no conflict of interest.
Authors’ contributions
WY and DL contributed to the concept and data design. JY, XLX and XWY collected data. BY and WY analyzed and interpreted data. BY drafted the article. DL and WY critically revised the article and approved articles. All authors read and approved the final manuscript.
Additional file
Additional file 1: Table S1.
Adjusted blood pressure mean with 95 % confidence interval by tertiles of the major serum FA in subjects (n = 2447). (DOC 132 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Yang, B., Ding, F., Yan, J. et al. Exploratory serum fatty acid patterns associated with blood pressure in community-dwelling middle-aged and elderly Chinese. Lipids Health Dis 15, 58 (2016). https://doi.org/10.1186/s12944-016-0226-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-016-0226-3