
Abstract
Background
There have been no studies of air pollution and mortality in Lima, Peru. We evaluate whether daily environmental PM2.5 exposure is associated to respiratory and cardiovascular mortality in Lima during 2010 to 2016.
Methods
We analyzed 86,970 deaths from respiratory and cardiovascular diseases in Lima from 2010 to 2016. Estimated daily PM2.5 was assigned based on district of residence. Poisson regression was used to estimate associations between daily district-level PM2.5 exposures and daily counts of deaths.
Results
An increase in 10 μg/m3 PM2.5 on the day before was significantly associated with daily cardiorespiratory mortality (RR 1.029; 95% CI: 1.01–1.05) across all ages and in the age group over 65 (RR 1.04; 95% CI: 1.005–1.09) which included 74% of all deaths. We also observed associations with circulatory deaths for all age groups (RR 1.06; 95% CI: 1.01–1.11), and those over 65 (RR 1.06; 95% CI 1.00–1.12). A borderline significant trend was seen (RR 1.05; 95% CI 0.99–1.06; p = 0.10) for respiratory deaths in persons aged over 65. Trends were driven by the highest quintile of exposure.
Conclusions
PM2.5 exposure is associated with daily cardiorespiratory mortality in Lima, especially for older people. Our data suggest that the existing limits on air pollution exposure are too high.
Similar content being viewed by others

Introduction
Approximately 4.2 million people are estimated to die annually from exposure to fine particles contained in polluted air [1]. Fine particulate matter (PM2.5) is considered the most harmful pollutant to human health, because it penetrates deep into the lungs [1]. Epidemiological studies conducted mainly in developing countries have associated PM2.5 with all cause and cause-specific mortality [2,3,4,5,6,7]. These studies have evaluated short-term and long-term PM2.5 exposure on mortality, primarily cardiovascular and respiratory deaths [3, 4, 8], but also some kinds of cancer [9,10,11]. Based on epidemiological evidence, the World Health Organization (WHO) estimated that air pollution is associated with premature deaths related to ischemic heart disease, strokes, chronic obstructive pulmonary disease, acute lower respiratory infections and lung cancer [2,3,4, 6, 7, 9].
Lima, the capital of Peru, is one of the most polluted cities in the Latin American region [12], with annual concentrations of PM2.5 ranging from 35 μg/m3 in the east side of Lima to 16 μg m3 in the districts within the center of Lima. The mean value for 2015 was 26 μg/m3 [13]. The air pollution mainly comes from vehicular emissions, although there is some contribution from industrial activity [14]. The government has implemented some regulations to reduce pollution and established safety thresholds for environmental concentrations [15]. Since then, PM2.5 levels have decreased markedly in the last 20 years, but high levels of pollutant are still observed in some areas of Lima [16, 17].
Gonzales and Steenland [18], analyzed PM2.5 data available from 2001 to 2010, and estimated that air pollution was responsible for 2300 premature deaths related to cardiorespiratory disease in adults, based on relative risk data from other parts of the world. Tapia et al. [19] have shown short-term effects of PM2.5 on emergency room visits in 9 Lima hospitals from 2010 to 2016. However, to date there is no specific epidemiological evidence that show the effects of air pollution on mortality in Peru. In this study, we have conducted daily time-series analysis using district-specific PM2.5 estimates in Lima [20] to evaluate whether daily environmental PM2.5 exposure is associated to respiratory and cardiovascular mortality in Lima during 2010 to 2016.
Methods
Study area
Lima is located on the central coast of Peru, at an average of 150 m above sea level, covers a geographical area of 2819 Km2 and a population density of 3392 inhabitants/km2. Lima has a population of 9,562,000 representing about 30% of the national population [21]. Lima is comprised of 43 districts and divided into four zones: North Lima, Central Lima, East Lima, and South Lima. We excluded 4 districts at high altitude (all above 570 m average altitude) due to uncertainty about the PM2.5 model predictions in these districts. The uncertainty was largely driven by the fact that ground monitoring stations providing inputs to the PM2.5 model were all located below 375 m, requiring a large extrapolation to these four high districts, using the model’s prediction of the altitude effect. These districts (district numbers 150,106, 150,107, 150,109, and 150,118) represented only 4% of the total population of Lima.
Mortality data
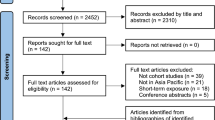
Data on daily mortality were obtained from the Ministry of Health (MoH). Variables included in this data were age, gender, district of residence, district of occurrence of death, cause of death with respective International Classification of Disease 10th revision (ICD-10). Deaths from respiratory (J00-J99) and circulatory (I00-I99) disease were considered for the study. The database included 109,951 recorded deaths from respiratory and circulatory disease, between January 2010 and December 2016. We excluded four districts (10,228 deaths) because the model may be inaccurate above 375 m (as noted above), and also excluded some other observations because pollution on some days could not be estimated due to lack of satellite coverage (12,753 deaths) (see below); the remaining sample was 86,970.
Meteorological and ambient PM2.5 data
Ground-monitoring PM2.5 data in Lima were available from March 2010 through December 2016, from 10 stations from the Servicio Nacional de Meteorología e Hidrología del Perú (SENAMHI, Ministry of the Environment), and 6 stations operated from 2011 to 2012 by Johns Hopkins University [22]. However, these data were not available on a daily basis during our study period, covering only about 10% of days. Hence, the ground-monitoring network was considered too sparse to adequately capture the spatiotemporal variability in PM2.5 levels that occurs in Lima. Thus, we based our PM2.5 exposure data from a model developed by Vu et al. [20]. Briefly, daily PM2.5 concentrations at a 1 km2 spatial resolution for 2010–2016 were estimated using a combination of the available ground measurements plus aerosol optical depth (AOD) data from satellites, and meteorological and land use data chemical transport models. AOD was obtained from NASA, using the MAIAC (Multi-Angle Implementation of Atmospheric Correction) algorithm. Meteorological fields (temperature, wind, and barometric pressure) were obtained from the European Centre for Medium-Range Weather Forecasts (ECMWF) and the Weather Research and Forecasting model coupled with Chemistry (WRF-Chem). A random forest model was used to regress the available ground measurements with 14 variables, including MAIAC AOD, meteorological variables from WRF-Chem and ECMWF, and land use variables. The overall cross-validation R2 value (and root mean square prediction error) was 0.70 (5.97 μg/m3), comparing predicted to observed ground level data. The mean difference between ground and predicted measurements was − 0.09 μg/m3. This regression model was then used to predict daily PM2.5 levels for each km2 grid across Lima. These estimates were then used in epidemiologic analyses, in which daily deaths were aggregated by district, and daily population-weighted average PM2.5 levels were calculated for each district from the 1 km2 data.
On every 16th day throughout the study period, we were unable to estimate PM2.5 due to lack of satellite coverage. Furthermore, PM2.5 estimates for October 15 to December 31, 2015 could not be made because the WRF-Chem model failed to estimate data within reasonable bounds for that period. Hence, we had PM2.5 estimates for 2236 days (91%) out of the 2465 days during the study period. The daily weather data (temperature and relative humidity) also was provided by SENAMHI.
The protocol was approved by Ethics Review Committee of Cayetano Heredia University (SIDISI code 202054).
Statistical analysis
For each death we had the district of residence, which we used to assign PM2.5 daily exposure (or a lagged exposure) to that death. Using our daily estimates of PM2.5 at a 1 square km resolution, as well as estimated population in that same area, we created daily population-weighted PM2.5 averages by district, which were in turn assigned to all daily deaths in that district. Daily deaths in each district were grouped for a Poisson regression analysis.
We used generalized linear models with Poisson regression to estimate associations between daily district-level PM2.5 levels and daily counts of deaths for the outcomes of interest. PM2.5 effects were assessed using same day (lag 0), previous day (lag 1), 2 day (lag 2), 3 days (lag 3) average PM2.5 for two (0–2), 3 days (0–3) as well as the prior 30 days average; lag 1 was eventually chosen based on superior fit to the data using Akaike’s Information Criteria (AIC). To control for spatially varying factors and allow the analysis to be based on temporal contrasts only, the models included indicator variables for district to represent the geographical area over which deaths counts were spatially aggregated; this also controlled for spatial autocorrelation in the baseline deaths across the districts [23]. The models also included variables included for day of week, daily relative humidity, and maximum daily temperature. We compared two methods for controlling for long-term trends, either via parametric cubic splines with monthly knots, or with variables for month, year and an interaction between these variables (month*year). The latter fit appreciably better via the AIC and was used. The continuous PM2.5 variable was also categorized into quintiles: Q1st: 11.27–17.07 μg/m3; Q2nd: 17.08–18.60 μg/m3: Q3rd: μg/m3 18.61–20.58), Q4th: 20.59–25.23 μg/m3; and Q5th: 25.24–60.18 μg/m3. Mortality was analyzed as a whole, and also stratified by three age groups (< 18, 18–64, 65 years or more). We analyzed combined respiratory and circulatory deaths, and separately, respiratory deaths (ICD10 codes J00-J45), and circulatory mortality deaths (ICD10 codes I00-I99), as well as infectious respiratory disease (IRD)(ICD10 codes 00-J06, J09-J22) and cardiovascular disease (CVD)(ICD10 codes ICD10: I20-I22, I24, I25, I46-I50, I63-I67, I70, I73-I75, I77, I79, G45). Models for several other sub-categories with fewer daily deaths did not converge. Standard errors of coefficients were adjusted for over-dispersion, which generally was very modest. Analyses were conducted using SAS v9.4 PROC GENMOD (SAS Institute Inc., Cary, NC, USA).
Results
The final analysis included 86,970 deaths; 59% were from respiratory causes, and 41% were from circulatory disease. The daily average was 22 deaths from respiratory disease and 15 from circulatory disease. On average, 74% of respiratory and circulatory deaths occurred in people over 65 years (Table 1).
The daily variation of estimated PM2.5 across Lima throughout the period is shown in Fig. 1. An increase in PM2.5 concentrations can be observed during the cold months (June-Sept). These values often exceeded the WHO air quality standards (24-h: 25 μg/m3), but were below the national Peruvian standard (24-h: 50 μg/m3).

Daily average estimated PM2.5 in Lima, 2010–2016
The population-weighted average of PM2.5 estimated for Lima, across all districts during the study period, was 21.0 μg/m3. The highest average PM2.5 concentrations (29.3 ± 4.21 μg/m3) were observed in East Lima and the lowest average concentrations were found in Centre Lima (18.0 ± 1.95 μg/m3) (Table 2).
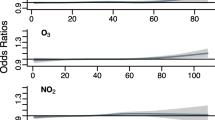
Lag 1 PM2.5 levels generally produced the best fit models, and are presented here. Tables 3, 4 and 5 show the associations of daily PM2.5 with combined respiratory and circulatory deaths, and separate respiratory, and circulatory disease mortality; results are presented as rate ratios (RRs) and 95% confidence intervals (CIs) calculated for 10 μg/m3 increase in PM2.5 across all districts and years.
PM2.5 was significantly positively associated with combined respiratory and circulatory deaths (RR 1.029; CI 95%: 1.005–1.052) and in the age group over 65 (74% of all deaths) (RR 1.048; CI 95%: 1.005–1.093) per 10 μg/m3 increase of PM2.5 (Table 3). Other age groups did not show positive trends. Positive trends were driven by the association in the top quintile, especially for deaths over 65 (RR 1.081, CI 95% 1.014–1.153).
A borderline significant RR (1.048; IC 95% 0.999–1.098; p = 0.06) for respiratory deaths in persons aged over 65 also observed (Table 4). We found significant positive RRs per 10 μg/m3 of increase in PM2.5 for circulatory deaths for all age groups (RR 1.06; CI 95%: 1.008–1.011), and for the group over 65 years (RR 1.06; IC 95% 1.001–1.127) (Table 5). Trends were driven by the top quintile with highest concentrations. Positive associations for CVD, a subset of circulatory disease, was seen in the group over 65 years (RR: 1.10; CI 95% 1.01–1.22) (Table 5). We could not do detailed analyses of other specific causes as deaths were too few and models did not converge.
Discussion
In this study, we estimated PM2.5 data using a satellite-driven PM2.5 exposure model [20] which provided daily population-weighted average PM2.5 concentrations for all districts of Lima, from 2010 to 2016. We then examined PM2.5 short-term exposure in relation to cardiorespiratory mortality (ICD 10 I00-J99) in Lima, one of the most polluted cities in Latin America [12]. We observed positive associations of daily PM2.5 exposure with cardiorespiratory mortality, with an increase of 1.8% per 10 μg/m3 increase in PM2.5 concentration, driven largely by those over 65 years of age. Our results are congruent with previous findings of statistically associations of PM2.5 with combined respiratory and circulatory deaths [1, 3, 24]. In a systematic review of seven time series studies of all-cause deaths, the researchers found an increase of 1.4% per 10 μg/m3 increment in PM2.5 [24]. In another systematic review of 37 studies, the researchers reported a 0.9% increase in all-cause mortality per 10 μg/m3 increase in PM2.5 [2].
For circulatory mortality, our results show an increase of 3.7% per 10 μg/m3 increase in PM2.5 for both mortality for all ages, and 3.8% those over 65 years. We also found increased risk with CVD, a large subset of circulatory disease. Newell, in a systematic review of 91 published studies, found a 0.47% increase in cardiovascular mortality per 10 μg/m3 increase in PM2.5 [25]. Likewise, Zhao et al. observed an increased CVD mortality risk (0.68%) associated with a 10 μg/m3 increase in PM2.5 [7].
For respiratory mortality, we found an association only for the elderly group, which was borderline significant. Our results showed a slight increased risk of 3% per 10 μg/m3 increase of PM2.5. One systematic review reported positive effects, with a 10 μg/m3 increment in PM2.5 being associated with 1.51% (95% IC 1.01 to 2.01) in all cause respiratory mortality [24].
In our data adverse health effects were driven by high rate ratios in the 5th quintile. The exposure contrast between the 5th and 4th quintile (mean 29.2 μg/m3 vs 22.6 μg/m3) was 6.6 μg/m3, larger than the inter-quartile range (IQR) of 6.2 μg/m3 for the entire population. Important exposure effects would have been lost with the use of broader categories in our categorical analyses.
Our study showed that PM2.5 exposure has a significant impact on the health of people in Lima, in particular among elderly people. The population structure is changing [21]; the number of individuals over 65 years is increasing. PM2.5 exposure along with a pre-existing condition, such as cardiometabolic disorders [26] or diabetes [27], has been shown to increase the risk of CVD deaths. Elderly people are more likely to have more of these conditions and be more vulnerable to the effects of air pollution.
Our study has several strengths. Firstly, we used a predictive model that estimated daily PM2.5 concentrations for 39 districts of Lima and for the entire study period, which replaced the relative scarce data from ground monitoring. Second, the allocation of PM2.5 concentrations to each death according to the district of residence allowed us to reduce possible exposure measurement by using district-specific PM2.5 estimates than using city-wide average data, thereby avoiding bias in our RR estimates. Third, we used the data of people who had habitual residence in Lima and died there. Limitations in our study included missing some exposure data (9% of days), some inaccuracy in our 1 km2 exposure estimates, and our inability to assign exposure estimates at a spatial resolution smaller than the district, due to lack of exact addresses. Another limitation is our lack of data regarding occupation, which will have led to some mismeasurement of estimated air pollution exposure for person who worked outside of their district.
Our study provides evidence regarding the effects of PM2.5 on cardio-respiratory deaths in moderate concentrations. The local recommendations for daily PM2.5 established by the Peruvian Ministry of Environment, are currently 25 μg/m3, compared to the recommendations given by WHO, which are 10 μg/m3. We believe that these recommendations for air quality in Peru are likely to be too high, and probably needs to be reviewed.
Conclusions
The results of our study show that the short-term PM2.5 exposure is associated with all cause, respiratory and circulatory disease mortality, especially in the elder population. This result was observed at PM2.5 concentration, which is well below the daily limit established by the Ministry of Environment (MINAM in Spanish) in Lima.
Availability of data and materials
Data of this study is available upon request.
Abbreviations
- AOD:
-
Aerosol optical depth
- CI:
-
Confidence interval
- CVD:
-
Cardiovascular disease
- ECMWF:
-
European Centre for Medium-Range Weather Forecasts
- ICD:
-
International Classification of Disease
- IRD:
-
Infectious respiratory disease
- MAIAC:
-
Multi-Angle Implementation of Atmospheric Correction
- MINAM:
-
Ministry of the Environment
- MoH:
-
Ministry of Health
- PM2.5:
-
Fine particulate matter
- SENAMHI:
-
Servicio Nacional de Meteorología e Hidrología del Perú
- WHO:
-
World Health Organization.
- WRF-Chem:
-
Weather Research and Forecasting model coupled with Chemistry
References
WHO (World Health Organization). Geneva, Switzerland: Public Health, Social and Environmental Determinants of Health Department, World Health Organization; 2018. Burden of disease from Ambient Air Pollution for 2016.
Achilleos S, Kioumourtzoglou M, Wu C, Schwarzt J, Kouutrakis P, Papatheodorou S. Acute effects of fine particulate matter constituents on mortality: a systematic review and meta-regression analysis. Environ Int. 2017;109:89–100.
Fajersztajn L, Saldiva P, Pereirra LAA, Leite VF, Buehler AM. Short-term effects of the fine particulate matter pollution on daily health events in LAtin America: a systematic review and meta-analysis. Int J Public Health. 2017;62(7):729–38.
Li MH, Fan LC, Mao B, Yang JW, Choi AMK, Cao WJ, Xu JF. Short-term exposure to ambient fine particulate matter increases hospitalizations and mortality in COPD: a systematic review and meta-analaysis. Chest. 2016;149(2):447–58.
Luben TJ, Nichols J, Dutton SJ, Ellen K, Owens EO, Laura DW, et al. A systemic review of cardiovascular emergency department visits, Hospital Admissions and Mortality Associatedwith Ambient Black Carbon. Environ Int. 2017;107:154.
Vodonos A, Awad Y, Schwartz J. The concentration-response between long-term PM2.5 exposure and mortality: a meta-regression approach. Environ Res. 2018;166:677–89.
Zhao L, Liang H, Chen F, Zi C, Guan W, Li J. Association between air pollution and cardiovascular mortality in China: a systematic review and meta-analysis. Oncotarget. 2017;8(39):66438–48.
Ren M, Fang X, Li M, Sun S, Pei L, Xu Q, Ye X, Cao Y. Concentration-Response Relationship between PM2.5 and Daily Respiratoy Deaths in China: A Systematic review and Metaregression Analysis of Time-Series Studies. Biomed Res Int. 2017;2017:5806185.
Hamra GH, Guha N, Cohen A, Laden F, Raaschou-Nielsen O, Samet JM, et al. Outdoor particulate matter exposure and lung Cancer: a systematic review and meta-analysis. Environ Health Perspect. 2014;122(9):906–11.
Kim HB, Shim JY, Park B, Lee YJ. Long-term exposure to air pollution and cancer mortality: a meta-analysis of cohort studies. Environ Res Public Health. 2018;15(11):E2608.
Li J, Li X, Bai C, Song Y. Particulate matter-induced epigenetic changes and lung cancer. Clin Respir J. 2017;11:539–46.
WHO. Ambient outdoor air pollution database, by country and city (xlsx file). Geneva: World Health Organization (WHO), Department of Public Health, Environmental and Social Determinants of Health; 2016.
Silva J, Rojas J, Norabuena M, Molina C, Toro R, Leiva-Guzmán M. Particulate matter levels in a south American megacity: the metropolitan area of Lima-Callao, Peru. Environ Monit Asses. 2017;189(12):635.
PE-MINAM. National air quality report. Republic of Peru: Ministry of the Environment (MINAM); 2013-2014.
MINSA. Politica Nacional de Salud Ambiental: 2011–2010. RM No. 258–2011/MINSA. Dirección General de Salud Ambiental. Lima: Ministerio de Salud; 2011.
Pacsi S. Spatial and temporal analysis of the air quality determined by particulate matter PM10 and PM2.5 in metropolitan Lima. Anales Cientificos. 2016;77(2):273–83.
Evaluación de la Calidad del Aire en Lima Metropolitana 2014. Servicio Nacional de Meteorologia e Hidrologia del Peru – SENAMHI, Ministerio del Ambiente; Lima-Peru.
Gonzales GF, Steenland K. Environmental health in Peru: outdoor and indoor contamination. Rev Panam Salud Publica. 2014;36(2):141.
Tapia V, Steenland K, Sarnat SE, Vu B, Liu Y, Sánchez-Ccoyllo O, Vasquez V, Gonzales GF. Time-series analysis of ambient PM2.5 and cardiorespiratory emergency room visits in Lima, Peru during 2010-2016. J Expo Sci Environ Epidemiol. https://doi.org/10.1038/s41370-019-0189-3.
Vu BN, Sánchez O, Bi J, Xiao Q, Hansel NN, Checkley W, et al. Developing an Advanced PM2.5 Exposure Model in Lima. Peru. Remote Sens (Basel). 2019;11(6):641.
INEI. Censo Nacional 2017. Peru: Instituto Nacional de Estadistica e Informatica; 2018.
Bose S, Romero K, Psoter KJ, Curreiro FC, Chen C, Johson CM, et al. Association of traffic air pollution and rhinitis quality of life in Peruvian children with asthma. PLoS One. 2018;13(3):e0193910.
Sarnat SE, Sarnat JA, Mulholland J, Isakov V, Özkaynak H, Chang HH, Klein M, Tolbert PE. Application of alternative spatiotemporal metrics of ambient air pollution exposure in a time-series epidemiological study in Atlanta. J Expo Sci Environ Epidemiol. 2013;23(6):593–605.
Atkinson RW, Mills IC, Walton HA, Anderson HR. Fine particle components and health-a systematic review and meta-analysis of epidemiological time series studies of daily mortality and hospital admissions. J Expo Sci Environ Epidemiol. 2015;25(2):208–14.
Newell K, Kartsonaki C, Lam KBH, Kurmi OP. Cardiorespiratory health effects of particulate ambient air pollution exposure in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Planet Health. 2017;1(9):e368–80.
Pope CA, Turner M, Burtnett R, Jerret M, Gapstur S, Diver WR, et al. Relationship between fine particulate air pollution, Cardiometabolic disorders, and cardiovascular mortality. Circ Res. 2015;2:108–15.
Yang BY, Fan S, Thiering E, Seissier J, Nowak D, Dong GH, Heinrich J. Ambient air pollution and diabetes: a systematic review and meta-analysis. Environ Res. 2019;180:108817. https://doi.org/10.1016/j.envres.2019.108817.
Acknowledgements
We thank our colleagues at the Ministry of Health (MINSA) and the Ministry of the Environment (MINAM/SENAMHI) for their collaboration throughout this project.
Funding
The study was founded by Grant U01TW010107 (1/2 Regional GEOHealth hub centered in Peru) from the National Institute of Health of United States (Fogarty Program).
Author information
Authors and Affiliations
Contributions
The author(s) read and approved the final manuscript. Authors Liu and Vu were responsible for developing the exposure model; authors Tapia and Steenland were primarily responsible for data analysis and manuscript preparation; author Vasquez helped gather the mortality data; author Gonzales oversaw the overall project and helped with interpretation.
Authors’ information
VT, VV and GGF are researchers of the Faculty of Sciences, Universidad Peruana Cayetano Heredia, Lima, Perú. KS and YL are professors at Rollins School of Public Health of Emory University, and VB is a PhD student in Rollins School of Public Health at Emory University.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics review board of Universidad Peruana Cayetano Heredia. SIDISI 202054.
Consent for publication
All authors agree in the publication of the final version of this manuscript.
Competing interests
The authors have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tapia, V., Steenland, K., Vu, B. et al. PM2.5 exposure on daily cardio-respiratory mortality in Lima, Peru, from 2010 to 2016. Environ Health 19, 63 (2020). https://doi.org/10.1186/s12940-020-00618-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-020-00618-6