
Abstract
Background
The treatment of Plasmodium vivax infections requires the use of primaquine, which can lead to severe haemolysis in glucose-6-phosphate dehydrogenase (G6PD)-deficient individuals. However, most of the Latin American countries, which are still endemic for vivax malaria, lack information on the distribution of G6PD deficiency (G6PDd). No survey has been performed so far in French Guiana. Herein, 80 individuals of the French Guianan Noir Marron population were scrutinized for red cell surface antigens of six blood group systems (ABO, Rh, Kell, Kidd, Duffy and MNS) and G6PD genetic polymorphisms. First, the sub-Saharan origin of the red cell phenotypes was assessed in relation with the literature. Then, given that the main sub-Saharan G6PDd variants are expected to be encountered, only the G6PD sequences of exons 4, 5, 6 and 9 were screened. This work aims at appraising the G6PD gene variation in this population, and thus, contributing to the G6PD piecemeal information in Latin America.
Results
Ninety-seven percent (97 %) of the red cells are Fy(a− b−), either D+ C− E− c+ e+ or D+ C+ E− c+ e+ and 44 % exhibited the Fya−/Jkb−/S− combined phenotype. Noteworthy is the detection of the G6PD(Val68Met) variant characterized by c.202G > A transition, G6PD(Asn126Asp) variant characterized by c.376A>G transition and G6PD(Asp181Val) variant characterized by c.542A>T transversion of the G6PD gene in 22.5 % of the sample, characteristic of the A−(202), A and Santamaria G6PDd variants, respectively.
Conclusions
French Guianan Noir Marron population represents a pool of Rh-D antigen positive, Duffy-negative and G6PD-deficient erythrocytes, the latter accounting for one in every eight persons. The present study provides the first community-based estimation of the frequency of G6PDd polymorphisms in French Guiana. These results contribute to the G6PD genetic background information puzzle in Latin America.
Similar content being viewed by others


Background
Glucose-6-phosphate dehydrogenase deficiency (G6PDd), an X-linked, hereditary and recessive genetic trait, is the most common genetic enzymopathy in humans. Glucose-6-phosphate dehydrogenase (G6PD) is an enzyme catalyzing the first reaction in the pentose phosphate pathway, providing reducing power to all cells in the form of NADPH (nicotinamide adenine dinucleotide phosphate). In red cells, defense against oxidative damage relies only on NADPH generated by G6PD activity [1]. More than 200 variants and 186 substitutions in the G6PD gene have been described [2, 3]. Though mostly asymptomatic, G6PDd may cause red cell membrane damage, haemoglobin crystals, haemolytic anaemia, neonatal jaundice, or haemoglobinuria in cases of induced oxidative stress from nutrition and drugs. Importantly, primaquine is a major anti-malarial treatment. Individuals who have inherited the G6PDd phenotype can exhibit sensitivity to primaquine, which leads to symptoms that range from moderate to lethal depending on the deficiency class [4, 5], and as such are designated primaquine-sensitive. Clinical relapse due the release of liver hypnozoites is the major characteristic of Plasmodium vivax and amino-8-quinoline-based primaquine and tafenoquine remain the only effective drugs against this parasitic form to date [1, 6]. The concordance of the geographical distribution of G6PDd variants with lower levels of parasitaemia and reduced risk of infection led to the hypothesis that this enzymatic feature is selectively advantageous in past and present malarial endemic areas [7–10]. Though the exact mechanisms remain elusive, G6PDd would favour early phagocytosis of parasitized red blood cells at a stage where the parasite has not yet multiplied [11].
Recently, reviews mapped the state-of-the-art of the G6PD variation evidenced at the enzymatic and molecular levels [12–14]. G6PDd seems restricted to Africa, Southern Europe, Asia, and Pacific islands and virtually absent in the Native American populations of the Americas [12, 15]. In Latin America, though drug-induced haemolysis represents most of the acute anaemia, only minimal data is available to accurately address the G6PD geographical distribution among non-urban populations [13]. Most Latin American countries are endemic areas for malarial parasites and transmission vectors [16]. Even if Mexico, Haiti, and Costa Rica would have eliminated malaria, other countries are still in control phase and require the use of primaquine knowing the risk of haemolysis that may result in G6PD-deficient persons. In Latin America but French Guiana, primaquine is prescribed for every patient infected with P. vivax without looking for G6PDd or ethnicity assignment [17]. In French Guiana, P. vivax has become the dominant malaria species with more than 60 % of attacks with a substantial increase of cases since mid-2001, mostly observed in children [18], Amerindian populations [19], gold panners, French armed forces [20], Hmong [21], and to a lesser extent, in the Noir Marron community [22]. Most of the malaria transmission occurs along the two frontier rivers. Along the middle Maroni River—western border with Suriname—Plasmodium falciparum malaria incidence remains higher than P. vivax, particularly in the Noir Marron territory. In contrast, P. vivax is more frequent in the upper reaches of the Maroni River where it infests the Wayana and Emerillon Amerindian populations [22]. Plasmodium vivax is also preponderant along the eastern border with Brazil, Oyapock River, and in the eastern inland areas. Though part of former anthropological studies [23–25], G6PD genetic variation in French Guiana in relation with malaria risk has never been carried out so far [22]. This lack of information prevents implementation of efficient programmes for the control or elimination of P. vivax malaria in Latin America [13].
The present study aims to partially tackle this issue with original data from a well-defined population from French Guiana assumed to carry sub-Saharan genetic polymorphisms. For this aim, the Noir Marron community which has arisen from the merger of slaves who escaped from Dutch plantations [26], was investigated. First, validation of the sub-Saharan origin of the red cells was allowed by the frequencies of antigen phenotypes of six membrane genetic systems linked with a sub-Saharan ancestry. At the same time, knowledge of these main red cell antigen frequencies would be crucial for blood product requirements and minimum stock levels to ensure blood transfusion compatible with recipient blood characteristics. Then the main sub-Saharan G6PDd variants indexed in [2] and assumed to be encountered were screened by molecular biology.
Methods
Sample collection
Study protocol, sample collection and de-identification were approved by the Comité de Protection des Personnes (C.P.P.) Sud-Ouest et Outre-Mer I, file no 1-11-39, ID-RCB no 2011-A00996-35. After approval of the informed consent, venous blood samples were collected in EDTA tubes from 80 Aluku, Ndjuka, Saramaka and Paramaka living in Papaichton, Loka, Boniville and Maripasoula, along the Maroni River. Along with sampling, data relative to sex, age, state of health, place of residence and population memberships have been recorded.
Surface antigen typing
Red cell antigens of the ABO, Rh, Kell, Kidd, Duffy, and MNS blood group systems were investigated. Due to the presence of natural ABO antibodies and strong immunogenicity of the Rh-D antigen, the ABO–D phenotype was typed first, followed by a second level of identification of the Rh–Kell antigenic profiles, ending with extended Duffy, Kidd and Ss (MNS) phenotypes.
Typing was carried out with Diagast (Loos, France) reagents anti-A (Clone 9113D10), -B (Clone 9621A8), -AB (Clones 9113D10 + 152D12), -D (Clones P3 × 61 + P3 × 21223B10 + P3 × 290 + P3 × 35), -Fya, -S, and -s; Eurobio (France) reagents anti-C (Clones MS273), -c (Clone MS35), -E (Clones MS12 + MS260), -e (MS62 + MS69) and -K (Clone AEK4), and Bio-Rad (Marnes-la-Coquette, France) reagents anti-Fyb, -Jka, and -Jkb.
DNA extraction
Genomic DNA was extracted from 200 µl of whole blood using a Blood DNA mini kit (QIAamp, Qiagen, Courtaboeuf, France) according to the manufacturer’s instructions.
Primer design
In order to confirm the sub-Saharan origin of the samples, the red cell antigen phenotypes were confronted with the frequencies encountered in sub-Saharan populations [12, 15]. Previous surveys revealed Central and West Africa as the putative origins of the Noir Marron, as well as no admixture in this population [26, 27]. This assumption allowed the expectation in the samples of the main sub-Saharan G6PDd variants that would have been brought during Atlantic Slave Trade [2]. Hence, G6PD exons 4, 5, 6 and 9 coding for the main sub-Saharan G6PDd variants were sequenced. Protocol is also appropriate for main variants encountered in South East Asia [28], the geographical origin of another French Guianan population with plausible G6PDd, the Hmong [29]. Primers are listed in Table 1 and were designed according to works of [30, 31], the Primer3 [32] and OligoPerfect™ Designer (Life Technologies, Carlsbad, CA, USA) tools.
PCR amplification
Exons were independently amplified from 50 ng of genomic DNA in a reaction mix containing 1 X buffer, 1.5 M of magnesium ions, 0.05 mM of each dNTP, 0.16 μM of each primer and 1 unity (U) of Taq polymerase (Invitrogen™, Cergy Pontoise, France). Amplifications were carried out in a 96-Well Veriti® (Applied Biosystem®, Courtaboeuf, France) or DNAEngine Peltier thermal cyclers (Bio-RAD, Marnes-la-Coquette, France). Temperature profile was 96 °C for 5 min (min.), followed by 30 cycles of 96 °C for 1 min., 60 °C for 1 min., 72 °C for 1 min., and a final extension step of 7 min. at 72 °C. PCR products were controlled through electrophoresis on 2 % agarose gels stained with ethidium bromide.
PCR purification and sequence reaction
Five µl of PCR products were purified in an enzymatic mix of 1 U of Thermosensitive Alkaline Phosphatase combined with 10 U of Exonuclease 1 (Euromedex). Purification steps were 15 min. at 37 °C ending with 15 min. at 85 °C in a Veriti™ 96-Well thermal cycler (Applied Biosystems).
After purification, forward fragments of exons 4, 5 and 6, and reverse strand of exon 9 were sequenced using primers listed in Table 1 and the BigDye™ terminator Cycle Sequencing Ready Reaction v1.1 (Applied Biosystem®, Courtaboeuf, France) following manufacturer’s protocol. After a Sephadex™ gel filtration, strands were segregated by capillary electrophoresis in a ABI PRISM 3130 genetic analyzer (Applied Biosystem®, Courtaboeuf, France) using POP-4® polymer and 36-cm length capillary.
Sequence alignment and allele estimation
Sequences were aligned to the G6PD reference sequence (accession number X55448.1) using CodonCode Aligner 3.5.3 (CodonCode Corporation, www.codoncode.com) and BioEdit 7.2.5 [33] following caution highlighted in [34] for exons 4 and 5. In order to assess heteroplasmy, the signature of heterozygous individuals, both forward and reverse DNA strand was sequenced and electrophoregrams proofread. G6PD allele frequencies were calculated by direct counting.
Ethics approval and consent to participate
Study protocol, sample collection and de-identification were approved by the Comité de Protection des Personnes (C.P.P.) Sud-Ouest et Outre-Mer I, file no 1-11-39, ID-RCB no 2011-A00996-35. The veinous blood samples were collected after approval of the informed consent of the 80 individuals Aluku, Ndjuka, Saramaka and Paramaka.
Results
Table 2 presents the occurrence of red cell phenotypes. Fifty-nine samples were O type and all were D+ but one. The most frequent Rh phenotype was D+ C− E− c+ e+ (49 cases out of 80) followed by D+ C+ E− c+ e+ (19 cases). The only D− phenotype was D− C− E− c+ e+. All samples carried the Cellano phenotype (K− k+) of the Kell system, 90 % the Jka antigen and all samples but one (98.8 %) were positive for the s antigen. As far as Duffy is concerned, 98.1 % were Fy(a− b−) and three Duffy positive individuals were found. Taken together, the Fya−/Jkb−/S− red cells account for 44 % of the sample.
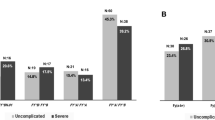
Table 3 presents the observed G6PD genotypes and Table 4 the inferred G6PD allele frequencies. Non-mutated sequences represent 77.5 % of the sample studied. Variants account for 22.5 % of the chromosomes sequenced. The most frequent G6PDd variants are A and A−(202) (10.9 %). One case of Santamaria (G6PD(A376G) transition, G6PD(Asp181Val) variant characterized by c.542A>T transversion) has been detected. Full enzymatic-deficient individuals which include males and homozygous females, represent 12.5 % of our sample. Neither the G6PD(Ser188Phe) Mediterranean variant characterized by c.563C>T transition nor the G6PD(Leu323Pro) Betica variant characterized by c.968T>C transition was detected. None of the three Duffy-positive samples were carrier of a G6PDd variant.
Discussion
The worldwide geographical distribution of membrane, haemoglobin and enzymatic red cell phenotypes is closely associated with P. falciparum and P. vivax [6, 8, 9, 12, 22, 35, 36]. In the New World, Latin America is endemic to P. vivax and P. falciparum and seven mosquito vector species have been identified [16, 37]. While all Native American populations may lack G6PDd, the other Latin American populations may possess G6PD mutations due to their non-Amerindian ancestry. This is especially the case of the Afro-descendant populations of the Amazonian basin whose sub-Saharan ancestry could reach 100 % [38–40].
Appraisal of parasitic loads, vector density and genetic background of the host is crucial to measure the level of transmission and the proportion of primaquine-sensitive individuals in malarial endemic areas. Although anti-malarial cure is unsafe taken with G6PDd, workers have recently pointed out the paucity of detailed information in Latin America [13]. In addition, no survey has been carried out so far in French Guiana [22], a level-4 G6PDd risk area [41]. In order to supply with G6PD information in Latin America, herein is presented the first community-based estimation of the frequency of G6PDd polymorphims in French Guiana.
Notable is the prevalence of the D+ C− E− c+ e+, Fy(a− b−), and the combined Fya−/Jkb−/S− (44 %) phenotypes. These are usually encountered in western sub-Saharan populations where frequencies reach 30 % for Fya−/Jkb−/S−, 70 % for D+ C− E− c+ e+, and up to 100 % for Fy(a− b−) [42, 43]. The present survey also revealed occurrence of G6PD A and A−(202) variants and one case of Santamaria; a variant fortuitously found in this study given its frequency worldwide [44–46]. Founder effect, the mechanism by which a population rose from a small number of founders and thus of alleles, would have thus concentrated sub-Saharan red cell genetic components including membrane antigen and G6PD genetic polymorphisms in the Suriname and Guianese Noir Marron [26].
Fy(a− b−) individuals are putatively insensitive to P. vivax infestation, so unconcerned by primaquine treatment. Nevertheless, several cases of Fy(a− b−) individuals infested by P. vivax have been reported in Malagasy, Africa, and more importantly in Brazil [47–50], making Duffy-negative individuals the novel panel of individuals suitable for primaquine treatment. Hence, estimation of G6PDd may be extended to a priori unconcerned populations such as the ones encountered in Latin America with West African genetic ancestry.
Capture of the human red cell genetic variation provides crucial information for transfusion safety. Transfusion risks are firstly embodied by the ABO-Rh-Kell phenotype variation, further by Duffy, Kidd and Ss phenotype depending on the patient, pathology and risk of alloimmunization. The present sample showed high values of O type, Rh-D antigen positive and Duffy-negative cases (alternatively said, positive for anti-FY antibodies). In addition, it has been reported that G6PDd reduces the efficacy of exchange transfusion in neonates and children recipients [51] with hyperkalaemia from the haemolysis of transfused blood cells and hyperbilirubinaemia due to the inefficient discard of the bilirubin excess by the immature liver, leading in one rare case to dark urine and acute intravascular haemolysis [52]. In patients with sickle cell disease who need repeated transfusions, donor blood G6PDd may also induce haemolysis [51]. Hence, studies recommended a routine screening for G6PDd for these at-risk patients [52], which may be discussed in countries where the prevalence of this deficiency is high like in Mediterranean basin and African ancestry populations. Describing the polymorphism of G6PDd may help to choose which populations have to be screened and what kind of polymorphism have to be detected. To date, in the context where French Guianans could represent a panel of G6PD-deficient donors, the small incidence of the Santamaria variant is not of primary importance given that blood donation is blocked by viral seroprevalence [53–56].
Enzymatic variation could usually be identified by non-molecular methods [57, 58]. Herein, the main sub-Saharan G6PD variants in a population from French Guiana were investigated through the direct screening of four G6PD exon sequences. French Guiana is also inhabited by western European populations in urban centres and a SouthEast asian community—the Hmong—in Cacao and Javouhey [29] for which level of G6PDd remains unknown. Besides exons 4 and 5, the PCR also targeted exons 6 and 9 where the Mediterranean, Mahidol, Rehevot and Viangchan substitutions occur [28]. Thus, the protocol performed may be practicable to the other communities of the area.
Conclusions
Due to the scarcity of the community-based studies led so far, screening of level and nature of G6PDd is a main challenge in Latin America. The present study aimed to fill the blank with original data from a sub-Saharan population living on the border of Suriname and French Guiana. The sub-Saharan origin of the studied red cells was confirmed from six blood group systems. Three G6PD polymorphisms (G6PD(Val68Met) variant characterized by c.202G>A transition, G6PD(Asn126Asp) variant characterized by c.376A>G transition, and G6PD(Asp181Val) variant characterized by c.542A>T transversion) defining three G6PDd variants (A−(202), A and Santamaria) were detected in 22.5 % of the sample. The present survey pointed out that French Guianan Noir Marrons represent a reservoir of Rh-D antigen positive, Duffy-negative and primaquine-sensitive phenotypes, the latter accounting for one in every eight persons.
Abbreviations
- G6PD:
-
glucose-6-phosphate dehydrogenase
- G6PDd:
-
glucose-6-phosphate dehydrogenase deficiency
- NADPH:
-
nicotinamide adenine dinucleotide phosphate
References
Cappellini MD, Fiorelli G. Glucose-6-phosphate dehydrogenase deficiency. Lancet. 2008;371:64–74.
Minucci A, Moradkhani K, Hwang MJ, Zuppi C, Giardina B, Capoluongo E. Glucose-6-phosphate dehydrogenase (G6PD) mutations database: review of the “old” and update of the new mutations. Blood Cells Mol Dis. 2012;48:154–65.
Beutler E, Duparc S. Glucose-6-phosphate dehydrogenase deficiency and antimalarial drug development. Am J Trop Med Hyg. 2007;77:779–89.
Burgoine KL, Bancone G, Nosten F. The reality of using primaquine. Malar J. 2010;9:376.
Douglas NM, Anstey NM, Buffet PA, Poespoprodjo JR, Yeo TW, White NJ, et al. The anaemia of Plasmodium vivax malaria. Malar J. 2012;11:135.
Beutler E. G6PD: population genetics and clinical manifestations. Blood Rev. 1996;10:45–52.
Guindo A, Fairhurst RM, Doumbo OK, Wellems TE, Diallo DA. X-linked G6PD deficiency protects hemizygous males but not heterozygous females against severe malaria. PLoS Med. 2007;4:e66.
Leslie T, Briceno M, Mayan I, Mohammed N, Klinkenberg E, Sibley CH, et al. The impact of phenotypic and genotypic G6PD deficiency on risk of Plasmodium vivax infection: a case–control study amongst Afghan refugees in Pakistan. PLoS Med. 2010;7:e1000283.
Louicharoen C, Patin E, Paul R, Nuchprayoon I, Witoonpanich B, Peerapittayamongkol C, et al. Positively selected G6PD-Mahidol mutation reduces Plasmodium vivax density in Southeast Asians. Science. 2009;326:1546–9.
Ruwende C, Khoo SC, Snow RW, Yates SN, Kwiatkowski D, Gupta S, et al. Natural selection of hemi- and heterozygotes for G6PD deficiency in Africa by resistance to severe malaria. Nature. 1995;376:246–9.
Mason PJ, Bautista JM, Gilsanz F. G6PD deficiency: the genotype-phenotype association. Blood Rev. 2007;21:267–83.
Howes RE, Dewi M, Piel FB, Monteiro WM, Battle KE, Messina JP, et al. Spatial distribution of G6PD deficiency variants across malaria-endemic regions. Malar J. 2013;12:418.
Monteiro WM, Franca GP, Melo GC, Queiroz AL, Brito M, Peixoto HM, et al. Clinical complications of G6PD deficiency in Latin American and Caribbean populations: systematic review and implications for malaria elimination programmes. Malar J. 2014;13:70.
Monteiro WM, Val FF, Siqueira AM, Franca GP, Sampaio VS, Melo GC, et al. G6PD deficiency in Latin America: systematic review on prevalence and variants. Mem Inst Oswaldo Cruz. 2014;109:553–68.
Cavalli-Sforza LL, Menozzi P, Piazza A. The history and geography of human genes. Princeton: Princeton University Press; 1994.
Sinka ME, Rubio-Palis Y, Manguin S, Patil AP, Temperley WH, Gething PW, et al. The dominant Anopheles vectors of human malaria in the Americas: occurrence data, distribution maps and bionomic precis. Parasit Vectors. 2010;3:72.
WHO. World Malaria Report 2015. Geneva: World Health Organization; 2015.
Carme B. Substantial increase of malaria in inland areas of eastern French Guiana. Trop Med Int Health. 2005;10:154–9.
Nacher M, Stefani A, Basurko C, Lemonnier D, Djossou F, Demar M, et al. The burden of Plasmodium vivax relapses in an Amerindian village in French Guiana. Malar J. 2013;12:367.
Pommier de Santi V, Dia A, Adde A, Hyvert G, Galant J, Mazevet M, et al. Malaria in French Guiana linked to illegal gold mining. Emerg Infect Dis. 2016;22:344–6.
Basurko C, Demattei C, Han-Sze R, Grenier C, Joubert M, Nacher M, et al. Deforestation, agriculture and farm jobs: a good recipe for Plasmodium vivax in French Guiana. Malar J. 2013;12:90.
Hay SI, Snow RW. The malaria Atlas Project: developing global maps of malaria risk. PLoS Med. 2006;3:e473.
Black FL, Santos SE, Salzano FM, Callegari-Jacques SM, Weimer TA, Franco MH, et al. Genetic variation within the Tupi linguistic group: new data on three Amazonian tribes. Ann Hum Biol. 1988;15:337–51.
Callegari-Jacques SM, Salzano FM, Weimer TA, Hutz MH, Black FL, Santos SE, et al. Further blood genetic studies on Amazonian diversity—data from four Indian groups. Ann Hum Biol. 1994;21:465–81.
Salzano FM, Black FL, Callegari-Jacques SM, Santos SE, Weimer TA, Mestriner MA, et al. Genetic variation within a linguistic group: Apalai-Wayana and other Carib tribes. Am J Phys Anthropol. 1988;75:347–56.
Brucato N, Cassar O, Tonasso L, Tortevoye P, Migot-Nabias F, Plancoulaine S, et al. The imprint of the Slave Trade in an African American population: mitochondrial DNA, Y chromosome and HTLV-1 analysis in the Noir Marron of French Guiana. BMC Evol Biol. 2010;10:314.
Brucato N, Tortevoye P, Plancoulaine S, Guitard E, Sanchez-Mazas A, Larrouy G, et al. The genetic diversity of three peculiar populations descending from the slave trade: Gm study of Noir Marron from French Guiana. C R Biol. 2009;332:917–26.
Iwai K, Hirono A, Matsuoka H, Kawamoto F, Horie T, Lin K, et al. Distribution of glucose-6-phosphate dehydrogenase mutations in Southeast Asia. Hum Genet. 2001;108:445–9.
Brucato N, Mazieres S, Guitard E, Giscard PH, Bois E, Larrouy G, et al. The Hmong diaspora: preserved South-East Asian genetic ancestry in French Guianese Asians. C R Biol. 2012;335:698–707.
AlMomen N, AlArrayed SS, AlAlawi A. Molecular homogeneity of G6PD deficiency. Bahrain Med Bull. 2004;26:1–7.
Minucci A, Gentile L, Zuppi C, Giardina B, Capoluongo E. Rapid and simple identification of the commonest glucose-6-phosphate dehydrogenase (G6PD) Italian mutations: from DNA extraction to genotyping. Clin Chim Acta. 2012;413:1018–9.
Untergasser A, Cutcutache I, Koressaar T, Ye J, Faircloth BC, Remm M, et al. Primer3—new capabilities and interfaces. Nucleic Acids Res. 2012;40:e115.
Hall TA. BioEdit: a user-friendly biological sequence alignment editor and analysis program for Windows 95/98/NT. Nucl Acids Symp Ser. 1999;41:95–8.
Mazieres S, Petit F, Dugoujon JM, Iriart X, Berry A, Carme B, et al. Subtle adjustments of the glucose-6-phosphate dehydrogenase (G6PD) mutation database and reference sequence. Blood Cells Mol Dis. 2013;52:55–6.
Miller LH, Mason SJ, Clyde DF, McGinniss MH. The resistance factor to Plasmodium vivax in blacks: the Duffy-blood-group genotype, FyFy. N Engl J Med. 1976;295:302–4.
Piel FB, Patil AP, Howes RE, Nyangiri OA, Gething PW, Dewi M, et al. Global epidemiology of sickle haemoglobin in neonates: a contemporary geostatistical model-based map and population estimates. Lancet. 2012;381:142–51.
Gething PW, Elyazar IR, Moyes CL, Smith DL, Battle KE, Guerra CA, et al. A long neglected world malaria map: Plasmodium vivax endemicity in 2010. PLoS Negl Trop Dis. 2012;6:e1814.
Ribeiro-dos-Santos AK, Pereira JM, Lobato MR, Carvalho BM, Guerreiro JF, Batista Dos Santos SE. Dissimilarities in the process of formation of Curiau, a semi-isolated Afro-Brazilian population of the Amazon region. Am J Hum Biol. 2002;14:440–7.
Callegari-Jacques SM, Grattapaglia D, Salzano FM, Salamoni SP, Crossetti SG, Ferreira ME, et al. Historical genetics: spatiotemporal analysis of the formation of the Brazilian population. Am J Hum Biol. 2003;15:824–34.
Santana MS, de Lacerda MV, Barbosa M, Alecrim WD, Alecrim M. Glucose-6-phosphate dehydrogenase deficiency in an endemic area for malaria in Manaus: a cross-sectional survey in the Brazilian Amazon. PLoS One. 2009;4:e5259.
Howes RE, Piel FB, Patil AP, Nyangiri OA, Gething PW, Dewi M, et al. G6PD deficiency prevalence and estimates of affected populations in malaria endemic countries: a geostatistical model-based map. PLoS Med. 2012;9:e1001339.
Noizat-Pirenne F. Immunohematologic characteristics in the Afro-caribbean population. Consequences for transfusion safety. Transfus Clin Biol. 2003;10:185–91.
Carritt B, Kemp TJ, Poulter M. Evolution of the human RH (rhesus) blood group genes: a 50 year old prediction (partially) fulfilled. Hum Mol Genet. 1997;6:843–50.
Saenz GF, Chaves M, Berrantes A, Elizondo J, Montero AG, Yoshida A. A glucose-6-phosphate dehydrogenase variant, Gd(−) Santamaria found in Costa Rica. Acta Haematol. 1984;72:37–40.
Hamel AR, Cabral IR, Sales TS, Costa FF, Saad STO. Molecular heterogeneity of G6PD deficiency in an Amazonian population and description of four new variants. Blood Cells Mol Dis. 2002;28:399–406.
De Araujo C, Migot-Nabias F, Guitard J, Pelleau S, Vulliamy T, Ducrocq R. The role of the G6PD AEth376G/968C allele in glucose-6-phosphate dehydrogenase deficiency in the seerer population of Senegal. Haematologica. 2006;91:262–3.
Cavasini CE, Mattos LC, Couto AA, Bonini-Domingos CR, Valencia SH, Neiras WC, et al. Plasmodium vivax infection among Duffy antigen-negative individuals from the Brazilian Amazon region: an exception? Trans R Soc Trop Med Hyg. 2007;101:1042–4.
Menard D, Barnadas C, Bouchier C, Henry-Halldin C, Gray LR, Ratsimbasoa A, et al. Plasmodium vivax clinical malaria is commonly observed in Duffy-negative Malagasy people. Proc Natl Acad Sci USA. 2010;107:5967–71.
Mendes C, Dias F, Figueiredo J, Mora VG, Cano J, de Sousa B, et al. Duffy negative antigen is no longer a barrier to Plasmodium vivax–molecular evidences from the African West Coast (Angola and Equatorial Guinea). PLoS Negl Trop Dis. 2011;5:e1192.
Ryan JR, Stoute JA, Amon J, Dunton RF, Mtalib R, Koros J, et al. Evidence for transmission of Plasmodium vivax among a duffy antigen negative population in Western Kenya. Am J Trop Med Hyg. 2006;75:575–81.
Samanta S, Kumar P, Kishore SS, Garewal G, Narang A. Donor blood glucose 6-phosphate dehydrogenase deficiency reduces the efficacy of exchange transfusion in neonatal hyperbilirubinemia. Pediatrics. 2009;123:e96–100.
Renzaho AM, Husser E, Polonsky M. Should blood donors be routinely screened for glucose-6-phosphate dehydrogenase deficiency? A systematic review of clinical studies focusing on patients transfused with glucose-6-phosphate dehydrogenase-deficient red cells. Transfus Med Rev. 2014;28:7–17.
Blanchet D, Breniere SF, Schijman AG, Bisio M, Simon S, Veron V, et al. First report of a family outbreak of chagas disease in French Guiana and posttreatment follow-up. Infect Genet Evol. 2014;28:245–50.
Carneiro AR, Cruz AC, Vallinoto M, Melo Dde V, Ramos RT, Medeiros DB, et al. Molecular characterisation of dengue virus type 1 reveals lineage replacement during circulation in Brazilian territory. Mem Inst Oswaldo Cruz. 2012;107:805–12.
Epelboin L, Douine M, Carles G, Villemant N, Nacher M, Rousset D, et al. [Zika virus outbreak in Latin America: what are the challenges for French Guiana in April 2016?](in French). Bull Soc Pathol Exot. 2016;109:114–25.
Sobesky M, Dabis F, Le Beux P. HIV/AIDS epidemic in French Guiana: 1979–1997. Groupe d’Etude Clinique de l’Infection VIH en Guyane Francaise. J Acquir Immune Defic Syndr. 2000;24:178–81.
Forbes J, Steytler JG, van Heerden R. Agarose gel electrophoresis of glucose-6-phosphate-dehydrogenase isoenzymes. Clin Chim Acta. 1991;199:279–82.
Brewer GJ, Tarlov AR, Alving AS. The methemoglobin reduction test for primaquine-type sensitivity of erythrocytes: a simplified procedure for detecting a specific hypersusceptibility to drug hemolysis. JAMA. 1962;180:386–8.
Authors’ contributions
PB, JC and SM designed the study and acquired the samples. FP performed lab work and analysis of the data. FP and SM drafted the manuscript. PB and JC revised the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors are grateful to the volunteers who participated to the study. The authors thank Anne Corval, former director of CNRS-Guyane, Pr. Gabriel Carle from the Saint Laurent du Maroni hospital, Pr. Bernard Carme, Pr. Mathieu Nacher, Nicolas Pouillot, Dr. Blandine Mulin, associated investigators, Dr. Flavia Grimoir from the Health Center of Grand Santi, Rémi Courbil, Loïc Niel, Pascale Wiquin-Auriel from the Etablissement Français du Sang Guadeloupe-Guyane, and Jean-Michel Dugoujon from the UMR5288 AMIS, for field work and sample logistics. The authors also thank Julia Gouvitsos, Laure Popée, Sophie Beley, Monique Silvy, Julie Di Cristofaro, Audrey Tous, Camille Reymond and Avril Meffray, for lab assistance and constructive discussions.
Authors’ information
FP: Ph.D student with emphasis on gene-environment interactions. PB: Scientific Director of the Etablissement Français du Sang Alpes Méditerranée (EFSAM), head of the molecular hematology research team, “Blood Groups – Biology”. JC: Director of the EFSAM, Professor of hematology, Ph.D in Biological Anthropology. SM: CNRS research fellow in Biological Anthropology.
Competing interests
The authors declare that they have no competing interests.
Funding
This work has benefited from an Investissement d’Avenir grant of the ANR (CEBA: ANR-10-LABX-0025) and Appel à Projet Recherche Etablissement Français du Sang 2016.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Petit, F., Bailly, P., Chiaroni, J. et al. Sub-Saharan red cell antigen phenotypes and glucose-6-phosphate dehydrogenase deficiency variants in French Guiana. Malar J 15, 310 (2016). https://doi.org/10.1186/s12936-016-1365-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-016-1365-8