
Abstract
Facing chloroquine drug resistance, Angola promptly adopted artemisinin-based combination therapy as the first-line to treat malaria. Currently, the country aims to consolidate malaria control, while preparing for the elimination of the disease, along with others African countries in the region. However, the remarkable capacity of Plasmodium to develop drug resistance represents an alarming threat for those achievements. Herein, the available, but relatively scarce and dispersed, information on malaria drug resistance in Angola, is reviewed and discussed. The review aims to inform but also to encourage future research studies that monitor and update the information on anti-malarial drug efficacy and prevalence of molecular markers of drug resistance, key fields in the context and objectives of elimination.
Similar content being viewed by others

Background
Plasmodium falciparum malaria is one of the most important public health problems in Angola, with more than three million cases confirmed between 2000–2013 and 7300 attributed deaths in 2013 [1]. Accordingly, in 2004 the country adopted artemisinin-based combination therapy (ACT) as the first-line treatment to uncomplicated malaria cases, specifically artemether-lumefantrine (AL, Coartem®, Novartis, Basel), having reached full territory implementation between 2007–2008 [2]. Additionally, considerable efforts have been made by the Angolan authorities, which have set a five-fold increase in public financing for malaria control [3]. Thus, the country has also become a signatory of the Malaria Elimination Eight (E8) network in 2009, aiming to consolidate malaria control and prepare for the ambitious elimination of the disease in the West-Southern African countries [1, 4].
Highly efficient treatments (ACT), have been a key factor for the improvements on the global control of malaria, and will be cornerstone in the transition to the elimination phase. Unfortunately, the remarkable capacity of the parasite to develop drug resistance represents a threat for these objectives. In this context, the present knowledge of malaria drug resistance in Angola is herein reviewed.
From quinine to chloroquine resistance
The first available anti-malarial drug in Angola, as in all the Western World, was quinine mono-therapy, introduced during the Portuguese colonial times. Albeit clinical failure with quinine therapies had been known for decades, there are no reliable reports of drug resistance when used in the country during the first decades of the 20th Century. This apparently sustained efficacy might be related to the limited deployment of the drug, partly due to its historical low supplies [5–7].
During the 1950s, few clinical trials were conducted in Huambo province (south Angola), testing the efficacy of pyrimethamine with weekly doses during 24 weeks, motivated by the low cost of this drug [8]. No evidence of resistance was documented, as all treated subjects were parasite free after the completion of the trial. In the same decade, chloroquine (CQ) was introduced in Angola, in line with the Global Malaria Eradication Programme and following the successful elimination of the disease in Portugal [9]. This event was the first significant malaria control effort targeting large sectors of the population.
In the late 1950s, CQ resistance emerged from foci in both South East Asia and South America. From the Asian focus, resistant P. falciparum progressively expanded in a western direction and by the start of the 1970s signs of possible CQ resistance were reported in the African continent [10–12]. The reports were unclear until the end of the decade, but unequivocal evidences of endemic CQ resistance were confirmed in Africa in 1979 [13, 14]. It is now assumed that CQ resistance then expanded in an east–west direction [15]. In 1984/1985, the first cases of CQ resistance were identified in Angola, particularly among European travellers [16, 17].
In vivo drug resistance
Trials supporting the use of ACT
Efficacy clinical trials, recommended to be conducted every 2 years, constitute the gold standard for the monitoring of drug efficacy, identification of anti-malarial drug resistance and to guide drug policy. Such studies were not systematically performed in Angola for an extended period of time, due to social instability. Thereafter, in 2001, the Ministry of Health conducted a series of in vivo anti-malarial efficacy trials in several provinces. In two of the implementation sites (Huambo and Bié provinces) the follow-ups were extended to 28 days and ACT was tested in a population of children below 5 years of age [18, 19]. A detailed report was published, showing that CQ [25 mg/Kg, 3 day course, 10 mg/Kg/day, first 2 days, 5 mg/Kg on the last day (IDA, Netherland)] and sulfadoxine-pyrimethamine (SP) (25 mg/Kg sulfadoxine + 1.25 mg/Kg pyrimethamine, one dose) had low efficacy, justifying the presence of resistant parasites among the children infected [19]. Inter-site average clinical and parasitological failures were above 80 % for CQ and >30 % for SP, upon PCR-correction through pfmsp1 and pfmsp 2 analysis. Amodiaquine [AQ, 30 mg/Kg, 3 day course, 10 mg/Kg/day (Camoquin®, Park-Davis, Senegal)] was associated with about 20 % of failure rate. On the other hand, the two ACT formulations tested, artesunate (AS) + SP (artesunate 4 mg/Kg/day, 3 days + 25 mg/Kg sulfadoxine, 1.25 mg/Kg pyrimethamine 3 days) and artesunate-amodiaquine [ASAQ: AS, 4 mg/Kg/day, 3 days (Arsumax®, Sanofi Winthrop, France) + AQ, 10 mg/kg/day, 3 days] were highly successful, with cure rates of 98.5 % for both [19]. Nevertheless, the low efficacy of SP therapy motivated the authors to recommend ASAQ as a better option for the post-chloroquine upgrade of the Angolan national malaria programme. This Médecins sans Frontières driven study, was extended in the following year with the objective to compare ASAQ with the artemether-lumefantrine (AL) fixed combination (Coartem®, Novartis, Basel) [18]. Also performed in the Huambo Province, this small study demonstrated that both ASAQ or AL were highly efficacious and no PCR-corrected (pfmsp1/2 + gulp) clinical failures were observed. It should be noted that others have demonstrated the occurrence of recrudescence 28 days after treatment initiation (especially with AL) [20–22]. Following this, Angola has (since 2007–2008) fully implemented ACT as the first-line mainstay for the national malaria control programme.
Recent suspicions of in vivo lumefantrine (LUM) resistance
In 2013, an ACT efficacy trial tested the efficacy of AL (20 mg artemether + 120 mg lumefantrine, 3 days) and the efficacy of a second generation ACT dihydroartemisinin-piperaquine (DHA-PPQ, Duo-cotecxin®; Beijing Holley-Cotec, China) in children under 5 years of age, in the Provinces of Zaire and Uíge [23]. DHA-PPQ showed extremely high efficacy, with no observed clinical failures (PCR-corrected), similar to results in other African locations [24]. The most impressive result was the relatively poor AL performance, with a final (corrected) efficacy below the WHO threshold for acceptable ACT efficacy (90 %) [1]. These results prompted a discussion regarding the possibility of AL resistance [25, 26]. On one hand, it should be taken into consideration that this result was mainly observed in one of the sites (Zaire Province) and involving a relatively low number of patients (n = 79). Importantly, as not all the AL doses were supervised, and no LUM blood levels were determined, questions rises if a substantial fraction of the observed clinical failures were due to lack of compliance, which would be consistent with increased cases of treatment failure in AL effectiveness trials [27]. Nevertheless, the results were robustly PCR-corrected, and a higher prevalence of pfmdr1 86N/184F/1246D genotypes, reported to be associated with LUM resistance, were documented among the recrudescence cases (when compared with the reinfections), suggestive of possible resistance [28]. The results of Plucinski et al. need to be followed up with new larger trials specifically designed for the detection of putative resistant infections [27].
In 2015, a small scale AL efficacy study, dispersed in 3 years, was performed in three different health centres of Luanda [29]. This research study also suggested a potential reduction in the AL PCR-corrected cure rates from the 2004 data (99 % towards 91.5 %) [29]. Despite intriguing, the limited size of the study, as well as the fact of being conducted in three different years and several different locations, recommends caution on the interpretation of those results. Even though it is open to discussion, the mere possibility of AL resistance emerging in Angola is worrisome enough, as this combination represents the cornerstone of malaria control in country.
Resistance to artemisinin derivatives
A recent case report, described a malaria patient returning from Luanda to a non-malarious region in Vietnam, showing a poor response to intravenous artesunate, as well as to a following dihydroartemisinin-piperaquine (Sigma-Tau pharmaceuticals, Gaithersburg, USA) treatment [30]. The patient was rescued by treatment with quinine-doxycycline. The very long clearance time of this infection (above 100 h) in the genetic environment of a wild type k13-propeller gene, along with the presence of multiple genotypes, an unusually slow response to all the used drugs and the lack of pharmacokinetic data, has raised questions about the possibility of patient factors justifying the clinical failure, including functional asplenia [31]. Concerns about the quality of the drug used were also raised. The authors argued that the low drug exposure would not justify the long persistence of high parasitaemia (>200,000 parasites/µL), while situation of severe asplenia would prolong the clearance of the parasites for even longer periods, irrespective of the drug used [32]. The rapid effect of the quinine + tetracycline rescue treatment supports this view. As for the raised issues on drug quality, the DHA-PPQ batches were verified directly by the manufacturer.
The case is essentially inconclusive, with the original authors considering that the critical importance of early detection of artemisinin resistance in Africa justifies high sensitivity surveillance, which can be more prone to false positive events than to clinical and epidemiologically more serious false negative situations. It is to note that Plucinski et al. did not find any evidence of a reduction of artemisinin derivative efficacy during their ACT efficacy clinical trial [23].
A compilation of available data on anti-malarial drug efficacy trials conducted in Angola is presented in Table 1.
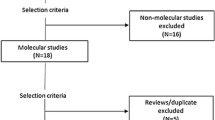
Molecular markers of drug resistance
The first clinical trials by Guthmann et al. showed that the efficacy of all mono-therapies available in Angola was below the minimum benchmark adopted by the World Health Organization (WHO) [19, 33]. These findings motivated a number of studies in the following years investigating molecular markers of resistance in the country (Table 2).
Pfcrt (Plasmodium falciparum chloroquine resistance transporter)
The pfcrt K76T is strongly linked with in vitro leap increases in IC50 values and clinical failure of CQ canonical regimen (3 day, 25 mg/Kg) [34–36]. The first report on pfcrt mutations in Angola came from the analysis of a small study performed in 1999 among uncomplicated malaria patients in Kifangondo, near Luanda [37]. The 76T SNP was found in 51 out of the 52 analysed infections. This high prevalence was supported by a following larger study in Luanda, where pfcrt 76T was found in all the ca 250 studied samples, and in a subsequent smaller survey in the Uíge Province (with >90 % of the parasites carrying the 76T allele) [38, 39]. The latter study was done through PCR fragment direct sequencing, revealing the common 72–76 haplotype CVIET. In 2010, the study of a set of uncomplicated malaria patient samples, again from Luanda, held a surprise: the key amino acids 72–76 region of the gene was shown to be significantly polymorphic [40]. Contrarily to other African regions, where the Asian originated CVIET haplotype is almost exclusive, the CVMNT, CVINT and even a new one, CVMDT, were detected [15, 40]. More importantly, the most prevalent haplotype reported was the SVMNT, typical of South America regions [41, 42]. Albeit considered rare in Africa, this haplotype has been sporadically found in the East coast of the continent [43]. The importance of the Luanda finding lay in the fact that the pfcrt SVMNT has been robustly associated with decreased parasite response to amodiaquine in vivo and in vitro, and that ASAQ was until recently the second line treatment of uncomplicated malaria in the country [44, 45]. The finding of a significant prevalence of SVMNT haplotype-carrying infections could partly explain the observed relatively low efficacy of AQ monotherapy [17]. Neither way, a more comprehensive survey performed in Bengo province (neighbouring Luanda metropolitan region) failed to find this diversity, as the analysed parasites either carried the Asian CVIET haplotype or (in a smaller fraction) the globally frequent CQ sensitive CVMNK [46]. Similarly, a recent study performed in the southern province of Benguela, also has not detected other pfcrt haplotypes than CVIET and CVMNK [47]. Gama et al. [40] have hypothesized that their exceptional observations were due to imported parasite populations from South America, due to the intense commercial relation between Angola and Brazil and the highly cosmopolitan nature of Luanda. Although such explanation sounds interesting, it is not supported by the results concerning the analysis of the pfmdr1 gene in the same parasites (see below). This aspect, and the previous detection of this haplotype in East Africa, recommends the surveillance of the potential emergence of pfcrt SVMNT carrying parasites, as proposed by Sá and Twu [48]. One positive aspect of the possible circulation of these haplotypes in Angola could be the fact that they have been associated with in vitro increased sensitivity to lumefantrine, when compared to the old World haplotype CVIET [49].
Pfmdr1 (Plasmodium falciparum multidrug resistance 1)
pfmdr1 was initially discovered during the quest for understanding CQ resistance [50]. Generally considered as a secondary factor, pfmdr1 has proved to be a central gene in the ACT era. In Africa, soon after the introduction of this strategy, SNPs in this gene (N86Y, followed by D1246Y and Y184F) were consistently shown to be under selection pressure of AL (the N86/F184/D1246 haplotype) and ASAQ treatment (the 86Y/184Y/1246Y haplotype) [51–54]. In vitro studies confirmed those observations. More recently the importance of the pfmdr1 alleles was reinforced through studies showing the increased capacity of N86/F184/D1246 parasites to invade patients with high lumefantrine blood levels upon AL treatment [28].
Upon a first small report, confirming the presence of CQ resistance associated to pfmdr1 86Y and 1246Y, a larger study conducted in Luanda showed that the large majority (ca. 90 %) of the parasite were carriers of the 86Y allele, similar to results from a smaller subsequent study in the Uíge province [38, 39, 55]. Gama et al. performed a more complete analysis, now also including the polymorphic positions Y184F, S1034C, N1042D, V1109I and D1246Y [40]. The authors struggled to PCR amplify fragments of this gene, with only 28 successful results. From this small sample, the frequency of the pfmdr1 86Y carriers was somewhat lower (ca. 60 %) as compared to the previously observed, while no mutations were detected in the amino acid 1246. Importantly, none of the parasites carried the characteristically New World 1034C or 1042D mutations. Such observation argues against the hypothesis that parasites harbouring pfcrt SVMNT haplotypes are exclusively imported from South American (see [40]).
In the Bengo province, the pfmdr1 SNP frequencies were somewhat different from the previously observed in Luanda, as a dominance of the N86 allele, present in >80 % of the infections, was observed [46]. These differences were interpreted by the authors to a certain extent as the result of the withdrawal of CQ and the introduction of AL as the main anti-malarial in the public health system. To this possibility adds the contribution of different drug exposures between the populations of the more rural Bengo as compared with the capital, where private access to other anti-malarials (namely AQ, which selects the 86Y allele) is significantly facilitated.
Pfmdr1 increased copy number has not been until recently identified in Angola, following the trend of its rarity in Africa [23, 56]. This scenario seems to be changing upon the report of a significant prevalence of this mutation in Luanda by the end of 2015 [29]. In a relatively small group of 101 successfully analysed AL treated patients, the amplification (2–3 copies) was detected in 13 subjects, the highest frequency ever registered in Africa [29]. Albeit that the presence of pfmdr1 increased copy number was not associated with AL clinical failure, the known link between this mutation and multidrug resistance—including lumefantrine—justifies concern [57].
Pfdhfr (Plasmodium falciparum dihydrofolate reductase) and pfdhps (Plasmodium falciparum dihydropteorate synthase)
SP (Fansidar, Roche, Basel) was the ephemeral first solution after the progressive collapse of CQ in Africa. Unfortunately, and following the historical trend for antifolates, resistance against this combination rapidly rose [18]. Despite that SP resistance is spread in large regions of Africa, the drug is still a key mass drug administration tool for malaria intermittent preventive treatment (IPT) during pregnancy, as well as for seasonal malaria chemoprevention programmes.
SP resistance is mainly mediated by genetic mutations modifying its two specific targets, the dihydrofolate reductase and dihydropteorate synthase enzymes, that represent two key members of the folate synthesis pathway [58]. A set of five mutations—pfdhfr: N108T/N51I/C59R + pfdhps A437G/K540E—are linked to SP resistance in Africa, particularly when present as quintuple haplotype [59]. A sixth SNP (I164L), associated with further very high levels of resistance is rare in Africa, but has been occasionally detected [60, 61].
In 1991–1992, the WHO standard ex vivo tests were performed in infections under care at the Russian Hospital in Luanda. 40 % of the subjects carried SP resistance parasites [62]. The first molecular report also emerged from the capital, having been limited to the analysis of the pfdhfr C59R and K540E SNPs, assuming a previously observed high specificity and sensitivity of them (≥90 % for both) for detecting the presence of the quintuple haplotype [25, 39]. The combination of the two SNPs was only found in 9 % of the analysed samples. In a study performed also among uncomplicated malaria patients, this time in the province of Uige, a relatively high prevalence of triple pfdhfr mutants (~25 %) was found. All but one of these were actually quadruple mutants, as they also carried the pfdhps 437G allele. No analysis of the pfdhps 540 a.a. position was performed, precluding conclusions concerning the presence of the quintuple haplotype [38]. A new study, including the analysis of the five positions, was conducted by Gama et al. [63]. The pfdhfr triple mutant was present in 50 % of the samples. The PCR amplification of the pfdhps sequences was significantly less successful, but allowed the detection of the quintuple mutant. Finally, Fortes et al. collected peripheral blood samples from asymptomatic parasite carriers under 5 years of age, in a series of surveys conducted in five different provinces (Cabinda, Uíge, Kwanza Norte. Malange and Huambo) [64]. In total, ca. 450 subjects were enrolled, with the analysis being specifically focused on the five key mutations. The quintuple mutant was shown to exist in very low frequency (<1 %), with only two observations, one in Cabinda and another in Huambo. The pfdhfr triple haplotypes was anyway present in a quarter of the analysed infections, while the resistance associated to pfdhps 437G was the most frequent allele in this position (>80 %) [64]. Also, results from two studies conducted in the south, showed 48 and 29 % of pfdhfr double mutants and 17 % of triple mutants in Huíla province and 20 % of pfdhfr triple negative carriers and 0 % of the pfdhfr/pfdhps quintuple mutant (from 80 asymptomatic infections) in Balombo, Benguela Province (see Table 2) [47, 65].
The most important conclusion of this set of studies was formulated by Fortes et al. [64]. These authors alerted to the fact that the high frequencies of pfdhfr triple and the pfdhps 437G allele configure populations of parasites with a clear potential to rapidly evolve towards the quintuple resistant haplotype. This should be a matter of concern due to the remain importance of SP for intermittent preventive treatments, as well as the recently launched WHO seasonal malaria chemotherapy initiative, based in the mass drug administration of the SP/AQ combination [66]. The later has been associated with the ready selection of SP resistance-associated SNPs [67]. This information is relevant for Angola. Following the expected future reductions in transmission according to the Malaria Elimination Eight (E8) network objectives, some provinces—especially in the southern regions of the country—may likely be targeted for such mass administration programmes in the foreseable future.
pf cytb (Plasmodium falciparum cytochrome b).
The mitochondrial membrane-located cytochrome b is the specific target of atovaquone, the key component of Malarone® (GSK, Brentford, UK). Malarone® (250 mg atovaquone + 100 mg proguanil/tablet) is the most used prophylactic anti-malarial among travellers. In a similar trend as with SP, the parasite develops resistance to this drug by modifying its target. Mutations on cytb codon 268 (T268S/G) have been consistently associated with Malarone® clinical failure, since the early days of the launch of this drug [68, 69]. An hospital-based PCR–RFLP study, performed in 249 malaria patients, in Luanda during 2003–2004, reported that all infections analysed were found to carry wild-type (sensitive) parasites for this a.a. position [70].
pfatp6 [Plasmodium falciparum Ca(2+)−ATPase] and pf kelch13 (Plasmodium falciparum Kelch13 propeller gene)
Both pfATP6, as a potential target of artemisinin, and the Kelch 13 propeller cytoplasmic protein, as a mediator of response against artemisinin action, have been proposed as markers of P. falciparum artemisinin resistance. In pfATP6, the S769N SNP was associated with significant increases in ex vivo determined IC50s in South America [71]. Diversity in the Kelch 13, particularly the C580Y SNP, has been linked with the phenotype of increased time of parasite clearance upon artemisinin-based therapies, in SE Asia [72].
In the only report mentioning pfatp6, the H243Y and the E431K SNPs were found to be present, the former being relatively frequent (~25 %). At the critical 769 position, only the wild type (S769) allele was observed in the set of analysed samples. As for the K13-propeller gene polymorphisms, a recent study have performed a small survey which consisted of 100 uncomplicated malaria patients from before and after the introduction of ACT in the country [73]. All sequences found were wild-type, with the exception of two synonymous SNPs, R471R and R575R. Those results indicate the low genetic variability of the gene in these regions, as well as the apparent lack of selective pressure from the introduction of ACT in the country. The low diversity observed is similar to the observed in the Zaire and Uíge provinces, where all the analysed parasites carried wild-type k13-propeller genes [58].
Conclusions
A number of knowledge gaps
In retrospect, the number of anti-malarial clinical trials performed in Angola has been meagre compared with the public health magnitude of this disease in the country. Additionally, the majority of the molecular studies were focused around Luanda. With its large territorial size, it would be expected that significant variation in the characteristics of the parasite populations may occur throughout its extensive geography.
Meanwhile, the recent increase in investment towards malaria control, expressed to a large extent in the introduction of effective ACT, has led to a significant decrease in the incidence of malaria in Angola in the last 5 years [1]. The country has the ambitious objective of reaching pre-elimination status during the next 5 years and, after decades of civil war, the country has reached a state of social stability compatible with such objectives. With its ample resources, and a relatively small population (comparatively to the standards of large African countries), Angola has the potential of being up to this challenge. However, such a goal still demands ground studies to answer a stream of key questions. Is the efficacy of lumefantrine really decreasing? What is the effectiveness of the other available formulations of ACT in Angola? With the pressure exerted by AL in the last years, is ASAQ now an even better alternative? Was the detection of pfcrt SVMNT a truly rare event or is the haplotype actually present in the country? Is the recently detected pfmdr1 increased copy number also an unusual event, or should it be cause for concern?
These and other questions need to be answered in order to provide the local authorities with hard evidence, essential to support future key decisions towards the objective of elimination.
References
WHO. World malaria report 2014. Geneva: World Health Organization; 2014.
Rowe AK, de Leon GF, Mihigo J, Santelli AC, Miller NP, Van-Dunem P. Quality of malaria case management at outpatient health facilities in Angola. Malar J. 2009;8:275.
Ministério da Saúde da República de Angola. Plano Nacional de Desenvolvimento Sanitário 2012–2025. 2014; 1: 119.
http://www.malariaeliminationgroup.org/resources/regional-and-cross-border-initiatives-elimination/elimination-eight-e8. 12 Nov 2015.
Webb JLA Jr. The long struggle against malaria in tropical Africa. Cambridge University Press; 2014.
Rodrigues Coura J. Development of malaria hematozoa resistant to quinine. By Arthur Neiva, 1910. Mem Inst Oswaldo Cruz. 1987;82:303–9.
da Silva AF, Benchimol JL. Malaria and quinine resistance: a medical and scientific issue between Brazil and Germany (1907-19). Med Hist. 2014;58:1–26.
Cambournac FJ, Gandara AF, Pena AJ. Preventive effects of daraprim in a native community (Catholic Mission of Huambo, Angola) (in Portuguese). An Inst Med Trop (Lisb). 1955;12(3):341–57.
Bruce-Chwatt LJ. Malaria eradication in Portugal. Trans R Soc Trop Med Hyg. 1977;71:232–40.
Mbomo SA, Ochrymowicz J. The possible presence in Cameroon of chloroquine resistant strains of Plasmodium falciparum (in French). Bull World Health Organ. 1970;42:168–70.
Bruce-Chwatt LJ. Resistance of P. falciparum to chloroquine in Africa: true or false? Trans R Soc Trop Med Hyg. 1970;64:776–84.
Bruce-Chwatt LJ, Roberts JM. Chloroquine-resistant malaria? BMJ. 1972;2:108–9.
Pillay N, Bhoola RL. Probable chloroquine-resistant Plasmodium falciparum malaria from Mozambique A case report. S Afr Med J. 1975;49:1443–4.
Campbell CC, Chin W, Collins WE, Teutsch SM, Moss DM. Chloroquine-resistant Plasmodium falciparum from East Africa: cultivation and drug sensitivity of the Tanzanian I/CDC strain from an American tourist. Lancet. 1979;2:1151–4.
Ariey F, Fandeur T, Durand R, Randrianarivelojosia M, Jambou R, Legrand E, et al. Invasion of Africa by a single pfcrt allele of South East Asian type. Malar J. 2006;5:34.
Olsen VV, Jensen T, Jorgensen M. Chloroquine-resistant Plasmodium falciparum malaria from Angola. Lancet. 1984;1:1462–3.
Lindberg J, Sandberg T, Bjorkholm B, Bjorkman A. Chloroquine and Fansidar resistant malaria acquired in Angola. Lancet. 1985;1:765.
Guthmann JP, Cohuet S, Rigutto C, Fortes F, Saraiva N, Kiguli J, et al. High efficacy of two artemisinin-based combinations (artesunate + amodiaquine and artemether + lumefantrine) in Caala, Central Angola. Am J Trop Med Hyg. 2006;75(1):143–5.
Guthmann JP, Ampuero J, Fortes F, van Overmeir C, Gaboulaud V, Tobback S, et al. Antimalarial efficacy of chloroquine, amodiaquine, sulfadoxine-pyrimethamine, and the combinations of amodiaquine + artesunate and sulfadoxine-pyrimethamine + artesunate in Huambo and Bie provinces, central Angola. Trans R Soc Trop Med Hyg. 2005;99(7):485–92.
Martensson A, Stromberg J, Sisowath C, Msellem MI, Gil JP, Montgomery SM, et al. Efficacy of artesunate plus amodiaquine versus that of artemether-lumefantrine for the treatment of uncomplicated childhood Plasmodium falciparum malaria in Zanzibar, Tanzania. Clin Infect Dis. 2005;41:1079–86.
Martensson A, Ngasala B, Ursing J, Isabel Veiga M, Wiklund L, Membi C, et al. Influence of consecutive-day blood sampling on polymerase chain reaction-adjusted parasitological cure rates in an antimalarial-drug trial conducted in Tanzania. J Infect Dis. 2007;195:597–601.
Venkatesan M, Gadalla NB, Stepniewska K, Dahal P, Nsanzabana C, Moriera C, et al. Polymorphisms in Plasmodium falciparum chloroquine resistance transporter and multidrug resistance 1 genes: parasite risk factors that affect treatment outcomes for P. falciparum malaria after artemether-lumefantrine and artesunate-amodiaquine. Am J Trop Med Hyg. 2014;91:833–43.
Plucinski MM, Talundzic E, Morton L, Dimbu PR, Macaia AP, Fortes F, et al. Efficacy of artemether-lumefantrine and dihydroartemisinin-piperaquine for treatment of uncomplicated malaria in children in Zaire and Uige Provinces, angola. Antimicrob Agents Chemother. 2015;59(1):437–43.
Zani B, Gathu M, Donegan S, Olliaro PL, Sinclair D. Dihydroartemisinin-piperaquine for treating uncomplicated Plasmodium falciparum malaria. Cochrane Database Syst Rev. 2014;1:CD010927.
Hamed K, Kuhen K. No robust evidence of lumefantrine resistance. Antimicrob Agents Chemother. 2015;59:5865–6.
Plucinski MM, Talundzic E, Morton L, Dimbu PR, Macaia AP, Fortes F, et al. Reply to “No Robust Evidence of Lumefantrine Resistance”. Antimicrob Agents Chemother. 2015;59:5867–8.
Ngasala BE, Malmberg M, Carlsson AM, Ferreira PE, Petzold MG, Blessborn D, et al. Efficacy and effectiveness of artemether-lumefantrine after initial and repeated treatment in children <5 years of age with acute uncomplicated Plasmodium falciparum malaria in rural Tanzania: a randomized trial. Clin Infect Dis. 2011;52:873–82.
Malmberg M, Ferreira PE, Tarning J, Ursing J, Ngasala B, Bjorkman A, et al. Plasmodium falciparum drug resistance phenotype as assessed by patient antimalarial drug levels and its association with pfmdr1 polymorphisms. J Infect Dis. 2013;207:842–7.
Kiaco K, Teixeira J, Machado M, do Rosario V, Lopes D. Evaluation of artemether-lumefantrine efficacy in the treatment of uncomplicated malaria and its association with pfmdr1, pfatpase6 and K13-propeller polymorphisms in Luanda, Angola. Malar J. 2015;14(1):504.
Van Hong N, Amambua-Ngwa A, Tuan NQ, do Cuong D, Giang NT, Van Dung N, et al. Severe malaria not responsive to artemisinin derivatives in man returning from Angola to Vietnam. Emerg Infect Dis. 2014;20:1199–202.
Ringwald P, Dondorp AM. Severe malaria not responsive to artemisinin derivatives in man returning from Angola to Vietnam. Emerg Infect Dis. 2015;21:1264–5.
Van Hong N, Amambua-Ngwa A, Tuan NQ, do Cuong D, Giang NT, Van Dung N, et al. Severe malaria not responsive to artemisinin derivatives in man returning from Angola to Vietnam. Emerg Infect Dis. 2015;21:1265.
WHO. World Malaria Report. Geneva; World Health Organization; 2006.
Djimde A, Doumbo OK, Cortese JF, Kayentao K, Doumbo S, Diourte Y, et al. A molecular marker for chloroquine-resistant falciparum malaria. N Engl J Med. 2001;344:257–63.
Fidock DA, Nomura T, Talley AK, Cooper RA, Dzekunov SM, Ferdig MT, et al. Mutations in the P. falciparum digestive vacuole transmembrane protein PfCRT and evidence for their role in chloroquine resistance. Mol Cell. 2000;6:861–71.
Sidhu AB, Verdier-Pinard D, Fidock DA. Chloroquine resistance in Plasmodium falciparum malaria parasites conferred by pfcrt mutations. Science. 2002;298:210–3.
Kryger T, Nahorski W, Wojtacha A, Szostakowska B, Pietkiewicz H, Myjak P. Assessment of clinical course and outcome of Plasmodium falciparum malaria in Angola diagnosed by microscopic and molecular methods. Int Marit Health. 2004;55(1–4):75–85.
Menegon M, Pearce RJ, Inojosa WO, Pisani V, Abel PM, Matondo A, et al. Monitoring for multidrug-resistant Plasmodium falciparum isolates and analysis of pyrimethamine resistance evolution in Uige province, Angola. Trop Med Int Health. 2009;14(10):1251–7.
Figueiredo P, Benchimol C, Lopes D, Bernardino L, do Rosario VE, Varandas L, et al. Prevalence of pfmdr1, pfcrt, pfdhfr and pfdhps mutations associated with drug resistance, in Luanda, Angola. Malar J. 2008;7(7):236–50.
Gama BE, Pereira-Carvalho GA, Lutucuta Kosi FJ, Almeida de Oliveira NK, Fortes F, Rosenthal PJ, et al. Plasmodium falciparum isolates from Angola show the StctVMNT haplotype in the pfcrt gene. Malar J. 2010;9(10):174.
Vieira PP, Ferreira MU, Alecrim M, Alecrim WD, da Silva LH, Sihuincha MM, et al. Pfcrt Polymorphism and the spread of chloroquine resistance in Plasmodium falciparum populations across the Amazon Basin. J Infect Dis. 2004;190:417–24.
Echeverry DF, Holmgren G, Murillo C, Higuita JC, Bjorkman A, Gil JP, et al. Polymorphisms in the pfcrt and pfmdr1 genes of Plasmodium falciparum and in vitro susceptibility to amodiaquine and desethylamodiaquine. Am J Trop Med Hyg. 2007;77:1034–8.
Alifrangis M, Dalgaard MB, Lusingu JP, Vestergaard LS, Staalsoe T, Jensen AT, et al. Occurrence of the Southeast Asian/South American SVMNT haplotype of the chloroquine-resistance transporter gene in Plasmodium falciparum in Tanzania. J Infect Dis. 2006;193:1738–41.
Sa JM, Twu O, Hayton K, Reyes S, Fay MP, Ringwald P, et al. Geographic patterns of Plasmodium falciparum drug resistance distinguished by differential responses to amodiaquine and chloroquine. Proc Natl Acad Sci USA. 2009;106:18883–9.
Beshir K, Sutherland CJ, Merinopoulos I, Durrani N, Leslie T, Rowland M, et al. Amodiaquine resistance in Plasmodium falciparum malaria in Afghanistan is associated with the pfcrt SVMNT allele at codons 72 to 76. Antimicrob Agents Chemother. 2010;54:3714–6.
Fancony C, Gamboa D, Sebastiao Y, Hallett R, Sutherland C, Sousa-Figueiredo JC, et al. Various pfcrt and pfmdr1 genotypes of Plasmodium falciparum cocirculate with P. malariae, P. ovale spp., and P. vivax in northern Angola. Antimicrob Agents Chemother. 2012;56(10):5271–7.
Foumane Ngane V, Allico Djaman J, Culeux C, Piette N, Carnevale P, Besnard P, et al. Molecular epidemiology of drug-resistant Plasmodium falciparum in Benguela province, Angola. Malar J. 2015;14(14):113–20.
Sa JM, Twu O. Protecting the malaria drug arsenal: halting the rise and spread of amodiaquine resistance by monitoring the PfCRT SVMNT type. Malar J. 2010;9:374.
Sisowath C, Petersen I, Veiga MI, Martensson A, Premji Z, Bjorkman A, et al. In vivo selection of Plasmodium falciparum parasites carrying the chloroquine-susceptible pfcrt K76 allele after treatment with artemether-lumefantrine in Africa. J Infect Dis. 2009;199:750–7.
Foote SJ, Kyle DE, Martin RK, Oduola AM, Forsyth K, Kemp DJ, et al. Several alleles of the multidrug-resistance gene are closely linked to chloroquine resistance in Plasmodium falciparum. Nature. 1990;345:255–8.
Holmgren G, Hamrin J, Svard J, Martensson A, Gil JP, Bjorkman A. Selection of pfmdr1 mutations after amodiaquine monotherapy and amodiaquine plus artemisinin combination therapy in East Africa. Infect Genet Evol. 2007;7:562–9.
Sisowath C, Stromberg J, Martensson A, Msellem M, Obondo C, Bjorkman A, et al. In vivo selection of Plasmodium falciparum pfmdr1 86 N coding alleles by artemether-lumefantrine (Coartem). J Infect Dis. 2005;191:1014–7.
Sisowath C, Ferreira PE, Bustamante LY, Dahlstrom S, Martensson A, Bjorkman A, et al. The role of pfmdr1 in Plasmodium falciparum tolerance to artemether-lumefantrine in Africa. Trop Med Int Health. 2007;12:736–42.
Humphreys GS, Merinopoulos I, Ahmed J, Whitty CJ, Mutabingwa TK, Sutherland CJ, et al. Amodiaquine and artemether-lumefantrine select distinct alleles of the Plasmodium falciparum mdr1 gene in Tanzanian children treated for uncomplicated malaria. Antimicrob Agents Chemother. 2007;51:991–7.
Pinheiro L, Franco S, Adagu IS, Rosa R, Rosario VE, Warhurst DC. Presence of the double pfmdr1 mutation 86Tyr and 1246 Tyr in clones of a chloroquine-resistant west African isolate of Plasmodium falciparum (in Portuguese). Acta Med Port. 2003;16(4):229–33.
Ursing J, Kofoed PE, Rombo L, Gil JP. No pfmdr1 amplifications in samples from Guinea-Bissau and Liberia collected between 1981 and 2004. J Infect Dis. 2006;194:716–8 (author reply 718–9).
Price RN, Uhlemann AC, van Vugt M, Brockman A, Hutagalung R, Nair S, et al. Molecular and pharmacological determinants of the therapeutic response to artemether-lumefantrine in multidrug-resistant Plasmodium falciparum malaria. Clin Infect Dis. 2006;42:1570–7.
Gregson A, Plowe CV. Mechanisms of resistance of malaria parasites to antifolates. Pharmacol Rev. 2005;57:117–45.
Kublin JG, Dzinjalamala FK, Kamwendo DD, Malkin EM, Cortese JF, Martino LM, et al. Molecular markers for failure of sulfadoxine-pyrimethamine and chlorproguanil-dapsone treatment of Plasmodium falciparum malaria. J Infect Dis. 2002;185:380–8.
Andriantsoanirina V, Ratsimbasoa A, Bouchier C, Jahevitra M, Rabearimanana S, Radrianjafy R, et al. Plasmodium falciparum drug resistance in Madagascar: facing the spread of unusual pfdhfr and pfmdr-1 haplotypes and the decrease of dihydroartemisinin susceptibility. Antimicrob Agents Chemother. 2009;53:4588–97.
Karema C, Imwong M, Fanello CI, Stepniewska K, Uwimana A, Nakeesathit S, et al. Molecular correlates of high-level antifolate resistance in Rwandan children with Plasmodium falciparum malaria. Antimicrob Agents Chemother. 2010;54:477–83.
Suleimanov SD. Drug-resistant tropical malaria in Angola. Med Parazitol (Mosk). 1994;2(2):8–10.
Gama BE, Pereira-Carvalho GA, Lutucuta Kosi FJ, Almeida de Oliveira NK, Fortes F, Rosenthal PJ, et al. Molecular markers of antifolate resistance in Plasmodium falciparum isolates from Luanda, Angola. Malar J. 2011;10:248.
Fortes F, Dimbu R, Figueiredo P, Neto Z, do VE, Rosario D. Evaluation of prevalence’s of pfdhfr and pfdhps mutations in Angola. Malar J. 2011;10(10):22.
Kaingona EPS. Characterization of genes associated with chemoresistance pfdhps to sulfadoxine/pyrimethamine in isolates of Plasmodium falciparum in Lubango. Angola: Instituto Oswaldo Cruz; 2012.
Cairns M, Roca-Feltrer A, Garske T, Wilson AL, Diallo D, Milligan PJ, et al. Estimating the potential public health impact of seasonal malaria chemoprevention in African children. Nat Commun. 2012;3:881.
Some AF, Zongo I, Compaore YD, Sakande S, Nosten F, Ouedraogo JB, et al. Selection of drug resistance-mediating Plasmodium falciparum genetic polymorphisms by seasonal malaria chemoprevention in Burkina Faso. Antimicrob Agents Chemother. 2014;58:3660–5.
Fivelman QL, Butcher GA, Adagu IS, Warhurst DC, Pasvol G. Malarone treatment failure and in vitro confirmation of resistance of Plasmodium falciparum isolate from Lagos. Nigeria. Malar J. 2002;1:1.
Farnert A, Lindberg J, Gil P, Swedberg G, Berqvist Y, Thapar MM, et al. Evidence of Plasmodium falciparum malaria resistant to atovaquone and proguanil hydrochloride: case reports. BMJ. 2003;326:628–9.
Pimentel S, Nogueira F, Benchimol C, Quinhentos V, Bom J, Varandas L, et al. Detection of atovaquone-proguanil resistance conferring mutations in Plasmodium falciparum cytochrome b gene in Luanda, Angola. Malar J. 2006;5(5):30.
Jambou R, Legrand E, Niang M, Khim N, Lim P, Volney B, et al. Resistance of Plasmodium falciparum field isolates to in vitro artemether and point mutations of the SERCA-type PfATPase6. Lancet. 2005;366:1960–3.
Miotto O, Amato R, Ashley EA, MacInnis B, Almagro-Garcia J, Amaratunga C, et al. Genetic architecture of artemisinin-resistant Plasmodium falciparum. Nat Genet. 2015;47:226–34.
Escobar C, Pateira S, Lobo E, Lobo L, Teodosio R, Dias F, et al. Polymorphisms in Plasmodium falciparum K13-propeller in Angola and Mozambique after the introduction of the ACTs. PLoS One. 2015;10(3):e0119215.
Authors’ contributions
FC and GJP draft the manuscript and BM edited and made a critical review of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors which to thanks the CISA office (Centro de Investigação em Saúde de Angola (CISA), Caxito, Angola) for the support.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Fançony, C., Brito, M. & Gil, J.P. Plasmodium falciparum drug resistance in Angola. Malar J 15, 74 (2016). https://doi.org/10.1186/s12936-016-1122-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-016-1122-z