
Abstract
Background
Increased risk of cardiovascular events is associated not only with dyslipidemias, but also with abnormalities in glucose metabolism and liver function. This study uses pooled analysis to explore the in-depth effects of pemafibrate, a selective peroxisome proliferator-activated receptor α modulator (SPPARMα) already known to decrease elevated triglycerides, on glucose metabolism and liver function in patients with hypertriglyceridemia.
Methods
We performed a post-hoc analysis of six phase 2 and phase 3 Japanese randomized double-blind placebo-controlled trials that examined the effects of daily pemafibrate 0.1 mg, 0.2 mg, and 0.4 mg on glucose metabolism markers and liver function tests (LFTs). Primary endpoints were changes in glucose metabolism markers and LFTs from baseline after 12 weeks of pemafibrate treatment. All adverse events and adverse drug reactions were recorded as safety endpoints.
Results
The study population was 1253 patients randomized to placebo (n = 298) or pemafibrate 0.1 mg/day (n = 127), 0.2 mg/day (n = 584), or 0.4 mg/day (n = 244). Participant mean age was 54.3 years, 65.4 % had BMI ≥ 25 kg/m2, 35.8 % had type 2 diabetes, and 42.6 % had fatty liver. Fasting glucose, fasting insulin, and HOMA-IR decreased significantly in all pemafibrate groups compared to placebo. The greatest decrease was for pemafibrate 0.4 mg/day: least square (LS) mean change from baseline in fasting glucose − 0.25 mmol/L; fasting insulin − 3.31 µU/mL; HOMA-IR − 1.28. ALT, γ-GT, ALP, and total bilirubin decreased significantly at all pemafibrate doses vs. placebo, with the greatest decrease in the pemafibrate 0.4 mg/day group: LS mean change from baseline in ALT − 7.6 U/L; γ-GT − 37.3 U/L; ALP − 84.7 U/L; and total bilirubin − 2.27 µmol/L. Changes in HbA1c and AST did not differ significantly from placebo in any pemafibrate groups in the overall study population. The decreases from baseline in LFTs and glucose metabolism markers except for HbA1c were notable among patients with higher baseline values. FGF21 increased significantly in all pemafibrate groups compared to placebo, with the greatest increase in the pemafibrate 0.4 mg/day group. Adverse event rates were similar in all groups including placebo.
Conclusions
In patients with hypertriglyceridemia, pemafibrate can improve glucose metabolism and liver function, and increase FGF21, without increasing adverse event risk.
Similar content being viewed by others

Background
Dyslipidemia is frequently associated with type 2 diabetes (T2D) and with non-alcoholic fatty liver disease (NAFLD) [1, 2], and hypertriglyceridemia is a known risk factor for developing newly onset T2D and NAFLD [3, 4]. Cardiovascular events are common not only in patients with T2D and NAFLD [5, 6] but also even in patients with milder abnormalities of laboratory tests such as glucose metabolism and liver function [7, 8], suggesting that insulin resistance may contribute to increased risk of cardiovascular diseases. These findings emphasize the importance of identifying patients with abnormal laboratory results in glucose metabolism, liver function and plasma lipids as part of ongoing efforts toward cardiovascular disease prevention.
Peroxisome proliferator-activated receptor (PPAR) α agonists can reduce triglyceride (TG) and TG-rich lipoprotein cholesterol levels and improve atherogenic dyslipidemia [9]. Pemafibrate, also known as K-877, was developed as a selective PPARα modulator (SPPARMα), which provides a favorable benefit-risk ratio superior to that of other conventional PPARα agonists [10, 11]. The high specificity and selectivity of pemafibrate as SPPARMα are achieved by its Y-shaped molecular structure, which allows pemafibrate to bind optimally to the PPARα ligand binding domain [12, 13]. After binding to the PPARα, pemafibrate up-regulates the expression of specific genes involved in fatty acid metabolism, primarily in human hepatocytes [14]. Pemafibrate reduces TG by 45–51 %, while increasing high-density lipoprotein cholesterol (HDL-C) by 12–20 % [15]. Pemafibrate also decreases the value of liver function tests (LFTs) such as alanine aminotransferase (ALT), γ-glutamyl transferase (γ-GT), and alkaline phosphatase (ALP), and fasting plasma glucose levels, and improves insulin sensitivity [16,17,18,19,20,21,22,23]. Although pemafibrate provides uniquely favorable effects on the parameters of glucose metabolism and liver functions, few reports have addressed these issues systematically. In addition, the effects of pemafibrate on glucose metabolism may be mediated by its effects on plasma levels of fibroblast growth factor (FGF) 21, a member of the FGF family that improves energy metabolism and that is induced in response to fasting or PPARα activation [24,25,26,27,28].
To gain more insight into these effects of pemafibrate, we applied a post-hoc analysis to findings from six placebo-controlled studies of pemafibrate in Japanese hypertriglyceridemic subjects. We focused on how pemafibrate affected glucose metabolism and LFTs in relation to baseline values, the presence of T2D and fatty liver, and changes in TG. We also investigated the relationships between FGF21 and glucose metabolism or liver function in those patients.
Methods
Study design and setting
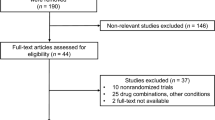
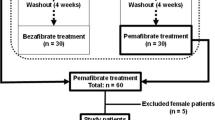
We performed a post-hoc analysis on data combined from six phase 2 and phase 3 Japanese randomized double-blind placebo-controlled studies in patients with hypertriglyceridemia [16,17,18,19, 29]. The studies enrolled a placebo group and pemafibrate groups (0.1 mg/day, 0.2 mg/day, and 0.4 mg/day). The drug was taken twice daily. The six individual studies are summarized in Table S1 in Additional file 1. Each study was approved by the Institutional Review Board for that study site. All studies were conducted in accordance with the Declaration of Helsinki after written informed consent had been obtained from each subject. This pooled analysis was approved by the Ethics Committee of Chiba University Graduate School of Medicine.
Endpoints
The primary endpoints consisted of changes from baseline in glucose metabolism markers (fasting plasma glucose, fasting serum insulin, the homeostatic model assessment of insulin resistance [HOMA-IR], and hemoglobin A1c [HbA1c]) and the LFTs (ALP, aspartate aminotransferase [AST], ALT, γ-GT, and total bilirubin). HOMA-IR was calculated using the following formula: HOMA-IR = fasting serum insulin (µU/mL) × fasting plasma glucose (mmol/L)/22.5.
The secondary endpoints included the changes from baseline in glucose metabolism markers and LFTs as analyzed in subgroups of patients with high baseline levels for glucose metabolism or liver function, and on the presence or absence of T2D or fatty liver. The diagnosis of T2D or fatty liver was made by individual clinicians at each study site. The group with high baseline values for glucose metabolism markers consisted of patients with baseline fasting plasma glucose ≥ 7.0 mmol/L (diabetes as defined by the World Health Organization’s diagnostic criteria) or fasting serum insulin ≥ 15 µU/mL or HOMA-IR ≥ 2.5 (insulin resistance as defined by the Japanese Diabetes Treatment Guideline) [30]. The group with high baseline values for LFTs consisted of patients whose LFTs values exceeded the upper normal limits (AST > 40 U/L, ALT > 45 U/L, γ-GT > 80 U/L for males or > 30 U/L for females, respectively, ALP > 325 U/L, and total bilirubin > 20.5 µmol/L [1.2 mg/dL]). Additional secondary endpoints were the proportion of patients having high baseline LFTs that were reduced to normal levels; the percent changes in TG and HDL-C from baseline; the changes in FGF21 from baseline; the correlation between changes in TG and changes in glucose metabolism and LFTs; and the correlation between changes in FGF21 and changes in glucose metabolism and LFTs. For the safety endpoint, the incidence of adverse events and drug reactions was recorded and analyzed in each group.
Measurements
All markers except FGF21 were measured by LSI Medience Corporation (Tokyo, Japan) using common measurement methods. FGF21 levels were measured using a human FGF21 enzyme linked immunosorbent assay (ELISA) kit (BioVendor, Brno, Czech Republic).
Statistical analysis
The full analysis set (FAS) was used to analyze the efficacy of pemafibrate on glucose metabolism markers and LFTs. Evaluation time points were at 12 weeks last observation carried forward (LOCF). The FAS included all randomized subjects who took at least one dose of the placebo or pemafibrate and for whom a baseline and at least one post-baseline value were available to assess the efficacy endpoints. Least squares (LS) mean with a 95 % confidence interval (CI) was calculated by analysis of covariance (ANCOVA) with the baseline value as the covariate. Similar ANCOVA analyses were performed for the subgroups of the high baseline groups, the groups of patients with and without T2D, and the groups of patients with and without fatty liver. We calculated the percentage of patients whose LFT was normalized by Week 12 (LOCF), based on the above reference range at baseline, and applied Fisher’s exact test to assess the proportion in each pemafibrate group compared to the placebo group. Univariate analyses (Pearson and Spearman) were applied to the changes in TG and FGF21, and to glucose metabolism and LFTs, to obtain correlation coefficients and p-values. All patients who received at least one dose of the placebo or pemafibrate were included in the safety analysis set (SAS). Safety was analyzed descriptively. Multiplicity was not considered in any statistical analysis in this study. SAS ver. 9.4 was used for the analyses.
Results
Patient characteristics
The FAS population consisted of 1253 patients from the six studies, of whom 298 were randomized to placebo, 127 to pemafibrate 0.1 mg/day, 584 to pemafibrate 0.2 mg/day, and 244 to pemafibrate 0.4 mg/day (Additional file 1: Figure S1).
The mean age was 54.3 years, 14.7 % were female, 65.4 % had body mass index (BMI) ≥ 25 kg/m2, 35.8 % were diagnosed with T2D, and 42.6 % had fatty liver. Mean ± standard deviation (SD) values for lipids and other parameters were 3.73 ± 1.52 mmol/L in TG, HDL-C 1.13 ± 0.28 mmol/L, HbA1c 6.26 ± 0.80 %, and estimated glomerular filtration rate (eGFR) 77.9 ± 16.4 mL/min/1.73 m2 (Table 1).
Glucose metabolism
No significant changes were noted in fasting plasma glucose, fasting serum insulin, or HOMA-IR in the placebo group. However, in all populations, these three measurements decreased significantly for pemafibrate compared to placebo. The greatest decrease was seen at the dose of 0.4 mg/day; in that group, fasting plasma glucose values for LS mean (95 % CI) differed from baseline by − 0.25 (− 0.36–−0.14) mmol/L (p < 0.001 vs. placebo); fasting serum insulin by − 3.31 (− 4.37–−2.26) µU/mL (p < 0.001); and HOMA-IR by − 1.28 (− 1.71–−0.84) (p < 0.001) (Fig. 1).

Changes in glucose metabolism markers from baseline to Week 12 (LOCF). * p < 0.05, ** p < 0.01, *** p < 0.001 vs. placebo (ANCOVA with baseline value as covariate). HOMA-IR was calculated using the following formula: HOMA-IR = fasting serum insulin (µU/mL) × fasting plasma glucose (mmol/L)/22.5. HOMA-IR homeostatic model assessment of insulin resistance, HbA1c hemoglobin A1c, SD standard deviation, LS least squares, CI confidence interval, LOCF last observation carried forward, ANCOVA analysis of covariance
The patients with higher baseline values showed greater decreases from baseline in fasting plasma glucose, fasting serum insulin, and HOMA-IR in all pemafibrate groups. Those differences were greatest in the pemafibrate 0.4 mg/day group: fasting plasma glucose values for LS mean (95 % CI) differed from baseline by − 0.61 (− 0.96–−0.27) mmol/L (p < 0.05 vs. placebo); fasting serum insulin by − 9.03 (− 11.97–−6.09) µU/mL (p = 0.065); and HOMA-IR by − 2.04 (− 2.72–−1.37) (p < 0.001) (Fig. 1).
For patients without T2D, decreases in fasting plasma glucose, fasting serum insulin, and HOMA-IR were significantly greater than placebo at all pemafibrate doses. For patients with T2D, decreases in fasting plasma glucose were significantly greater than placebo in groups treated with 0.2 mg/day or above, and decreases from baseline in fasting serum insulin and HOMA-IR were significantly greater in the 0.4 mg/day group. Regardless of the T2D status, these glucose metabolism markers showed the greatest decrease in the 0.4 mg/day group (Additional file 1: Figure S2).
In the absence of fatty liver, decreases in fasting plasma glucose, fasting serum insulin, and HOMA-IR were significantly greater than placebo at all pemafibrate doses. For patients with fatty liver, decreases in fasting plasma glucose and fasting serum insulin were significantly greater than placebo in groups treated with 0.2 mg/day or above, and decreases in HOMA-IR were significantly greater in the 0.4 mg/day group. Regardless of fatty liver status, these glucose metabolism markers showed the greatest decrease in the 0.4 mg/day group (Additional file 1: Figure S3).
For HbA1c, our analysis showed no statistically significant difference between pemafibrate and placebo, both overall and when stratified by HbA1c at baseline (Fig. 1) or by patients with and without T2D (Additional file 1: Figure S2) or with and without fatty liver (Additional file 1: Figure S3).
LFTs
No significant decreases in AST, ALT, γ-GT, ALP, or total bilirubin were noted among any patients in the placebo group. However, in all populations, the LFTs except for AST decreased significantly for all pemafibrate groups compared to placebo. The greatest decrease from baseline was seen in the pemafibrate 0.4 mg/day group: for ALT, LS mean (95 % CI) values differed by − 7.6 (− 9.3–−6.0) U/L (p < 0.001 vs. placebo), γ-GT by − 37.3 (− 41.6–−32.9) U/L (p < 0.001), ALP by − 84.7 (− 88.9–−80.5) U/L (p < 0.001), and total bilirubin by − 2.27 (− 2.69–−1.85) µmol/L (p < 0.001). Results for AST showed no difference from placebo in any of the pemafibrate groups (Fig. 2).

Changes in liver function tests from baseline to Week 12 (LOCF). * p < 0.05, ** p < 0.01, *** p < 0.001 vs. placebo (ANCOVA with baseline value as covariate). AST aspartate aminotransferase, ALT alanine aminotransferase, γ-GT γ-glutamyl transferase, ALP alkaline phosphatase, SD standard deviation, LS least squares, CI confidence interval, LOCF last observation carried forward, ANCOVA analysis of covariance
Greater decreases in AST, ALT, γ-GT, ALP, and total bilirubin were noted in those patients with high baseline values (Fig. 2). The greatest decrease from baseline was seen at pemafibrate 0.4 mg/day; for ALT, LS mean (95 % CI) values differed by − 20.5 (− 25.3–−15.8) U/L (p < 0.001 vs. placebo), γ-GT by − 82.0 (− 95.5–−68.6) U/L (p < 0.001), ALP by − 146.3 (− 173.5–−119.1) U/L (p < 0.001), and total bilirubin by − 10.87 (− 13.20–−8.54) µmol/L (p < 0.001). In that group, AST values differed by − 12.2 (− 17.8–−6.6) U/L (p < 0.01) (Fig. 2).
In the pemafibrate 0.2 mg/day and 0.4 mg/day groups, a significantly higher proportion of the patients whose baseline ALT, γ-GT, and ALP levels exceeded the upper normal limits had achieved normal levels at Week 12 (LOCF) than in the placebo group. The greatest proportion of improved patients was in the 0.4 mg/day group: AST (58.1 %), ALT (67.2 %), γ-GT (80.6 %), ALP (100 %), and total bilirubin (88.2 %) (Fig. 3).

Percentage of patients whose liver function tests were normalized at Week 12 (LOCF) from above reference range at baseline. * p < 0.05, *** p < 0.001 vs. placebo (Fisher’s exact test). AST aspartate aminotransferase, ALT alanine aminotransferase, γ-GT γ-glutamyl transferase, ALP alkaline phosphatase, LOCF last observation carried forward
For patients without T2D, decreases in ALT, γ-GT, ALP, and total bilirubin were significantly greater than placebo at all pemafibrate doses. For patients with T2D, decreases in γ-GT, ALP, and total bilirubin were significantly greater than placebo in all pemafibrate groups, and decreases in ALT were significantly greater in groups treated with 0.2 mg/day or above. With the exception of ALT in patients without T2D, these decreases were greatest in the 0.4 mg/day group (Additional file 1: Figure S4).
In the absence of fatty liver, the decreases in ALT, γ-GT, ALP, and total bilirubin were significantly greater than placebo at all pemafibrate doses. For patients with fatty liver, the decreases in γ-GT, ALP, and total bilirubin were significantly greater than placebo in all pemafibrate groups, and the decreases in ALT were significantly greater in groups treated with 0.2 mg/day or more. With the exception of ALT in patients without fatty liver, these LFTs showed the greatest decrease in the 0.4 mg/day group (Additional file 1: Figure S5).
TG and HDL-C
TG levels decreased significantly for all pemafibrate doses compared with placebo (LS mean values for percentage changes from baseline: −44.6 % for 0.1 mg/day, − 47.5 % for 0.2 mg/day, − 50.9 % for 0.4 mg/day, p < 0.001 for each vs. placebo) (Fig. 4). HDL-C levels increased significantly for all pemafibrate doses compared to baseline (LS mean values for percentage changes: 16.8 % for 0.1 mg/day, 17.8 % for 0.2 mg/day, 15.8 % for 0.4 mg/day, p < 0.001 for each vs. placebo) (Fig. 4).

Percentage changes in TG and HDL-C levels. Baseline levels indicate mean ± SD, and bars indicate LS mean percentage change (95 % CI) from baseline to Week 12 (LOCF). *** p < 0.001 vs. placebo (ANCOVA with baseline value as covariate). TG triglyceride, HDL-C high-density lipoprotein cholesterol, SD standard deviation, LS least squares, CI confidence interval, LOCF last observation carried forward, ANCOVA analysis of covariance
FGF21
FGF21 increased significantly for all pemafibrate doses compared to placebo. The greatest increase was noted at pemafibrate 0.4 mg/day, which changed from baseline by + 369.5 pg/mL, p < 0.001 vs. placebo (Fig. 5).

Changes in FGF21 levels. Baseline levels indicate mean ± SD, and bars indicate LS mean change (95 % CI) from baseline to Week 12 (LOCF). *** p < 0.001 vs. placebo (ANCOVA with baseline value as covariate). FGF21 fibroblast growth factor 21, SD standard deviation, LS least squares, CI confidence interval, LOCF last observation carried forward, ANCOVA analysis of covariance
Coefficient of correlation between changes in TG or FGF21 and the glucose metabolism markers or LFTs
There were no substantial correlations between changes in either TG or FGF21 and any of the glucose metabolism markers (fasting plasma glucose, fasting serum insulin, HOMA-IR) (Additional file 1: Table S2).
We found significant positive correlations, but with relatively small coefficients of correlation, for changes in γ-GT and TG (Pearson’s product moment 0.164, Spearman’s rank 0.178) and in ALP and TG (Pearson’s product moment 0.156, Spearman’s rank 0.155). There was a significant negative correlation for changes in total bilirubin and FGF21, again with a relatively small coefficient of correlation (Pearson’s product moment − 0.169, Spearman’s rank − 0.204) (Additional file 1: Table S3). In comparison to all patients, patients with high baseline values showed greater positive correlations for changes in γ-GT and TG (Pearson’s product moment 0.240, Spearman’s rank 0.222). For changes in ALP and FGF21, the correlation coefficient was higher in the high baseline patients than in all patients, but did not reach significance (Pearson’s product moment − 0.244, Spearman’s rank − 0.229). Similarly, for changes in total bilirubin and FGF21, the correlation coefficient was higher in the high baseline patients than in all patients but did not reach significance (Pearson’s product moment − 0.313, Spearman’s rank − 0.239) (Additional file 1: Table S3).
Adverse events and adverse drug reactions
Adverse events occurred in 43.0 % (128/298) of patients in the placebo group, 44.1 % (56/127) in the pemafibrate 0.1 mg/day group, 41.4 % (242/584) in the 0.2 mg/day group, and 38.2 % (94/246) in the 0.4 mg/day group. Serious adverse events (SAEs) developed in two patients (0.7 %, embolic stroke and angina pectoris) in the placebo group, three patients (2.4 %, acute myocardial infarction, cervical cancer, and upper limb fracture) in the 0.1 mg/day group, 10 patients (1.7 %; one patient each with ureteral calculus, bile duct stone, malignant lung neoplasm, colon cancer, hematoma of the abdominal wall, lumbar spinal stenosis, varicose vein surgery, and diabetes mellitus, and two patients with enterocolitis) in the 0.2 mg/day group, and two patients (0.8 %, ureteral calculus and myocardial infarction) in the 0.4 mg/day group, plus one death (pulmonary embolism) in the 0.4 mg/day group [15].
Discussion
Our study revealed that glucose metabolism markers (fasting plasma glucose, fasting serum insulin, HOMA-IR) and LFTs (ALT, γ-GT, ALP, and total bilirubin) were significantly reduced by pemafibrate. The change was particularly notable in the subgroups with high baseline values. In the high baseline LFTs subgroup, the 0.4 mg/day group had the highest proportion of patients who achieved normal LFT values. These findings were consistent with previous studies, which also showed pemafibrate-induced improvements in TG and HDL-C and increases in FGF21. Of note, diabetes and NAFLD have been found to correlate closely with abnormal lipid metabolism [1, 2], and pemafibrate not only improves lipid metabolism, but also may beneficially affect glucose metabolism and liver function at a high dose (0.4 mg/day). Related to those findings, we previously published the results of pooled analysis showing that high-dose pemafibrate was associated with marked reductions in ApoB48, ApoC3, ApoC3/ApoC2, small low-density lipoprotein cholesterol (LDL-C), and fibrinogen [15].
In a previous study using diet-induced obese mice, oral glucose tolerance tests (OGTT) showed that post-challenge serum insulin was reduced by pemafibrate, suggesting that pemafibrate improves insulin sensitivity [31]. Findings from another study indicated that pemafibrate enhanced the expression of the ATP-binding cassette transporter A1 (ABCA1) and reduced the level of 8-hydroxy-2’-deoxyguanosine (8-OHdG) in pancreatic β cells, suggesting that pemafibrate may improve insulin secretory capacity in diabetic patients by mitigating lipotoxicity and reducing oxidative stress in the pancreas [32, 33]. Pemafibrate use has also been associated with improved hepatic glucose uptake capacity in patients with hypertriglyceridemia, as evaluated by the glucose clamp technique [29]. Although drugs that activate PPARα do not have a consistent effect on glucose metabolism [34,35,36], we noted improvement in both fasting plasma glucose and insulin sensitivity in this study. There was no notable correlation between changes in glucose metabolism and changes in TG in our study, suggesting that pemafibrate may possibly improve glucose metabolism independently of reduction in TG. Previous studies of pemafibrate in T2D have provided somewhat inconsistent behaviors in HbA1c, glycoalbumin, plasma glucose, and serum insulin [19, 22, 37]. Similarly, our pooled analysis indicated that the increase in HbA1c tended to be about the same for pemafibrate and placebo, even in groups that showed pemafibrate-induced reductions in plasma glucose and serum insulin compared to the placebo control. However, when we consider that HbA1c indicates the plasma glucose over the previous one to two months, and that the data analyzed from our study was collected during a relatively short period of 12 weeks, these apparent inconsistencies may simply represent a divergence between HbA1c and current changes in plasma glucose and serum insulin. It is possible that worsening of postprandial glucose might mitigate the improvement in fasting glucose, neutralizing the effect on HbA1c; however, our previous study of pemafibrate did not show worsening of postprandial glucose level [19]. It is also possible that the natural rise in HbA1c mitigates the expected improvement in HbA1c based on blood glucose values.
Whether improved LFTs are related to improvement in non-alcoholic steatohepatitis (NASH) and NAFLD remains unproven at this point. However, obeticholic acid, a farnesoid X nuclear receptor (FXR) ligand that modulates lipid metabolism, has been associated with improvement in the liver histology of patients with NASH, and also with significant decreases in AST, ALT, γ-GT, and total bilirubin [38]. The effects of pemafibrate on reduction of liver fat and suppression of liver fibrogenesis have been studied in rodent NASH models [39]. A phase 2 study of pemafibrate, currently in process, is using noninvasive methods to measure liver fat content and liver stiffness (ClinicalTrials.gov Identifier: NCT03350165). This study, which focuses on the 0.4 mg/day pemafibrate dose, enrolled patients with liver fat content of 10 % or above, liver stiffness of 2.5 kPa or above, and high ALT. The study is expected to show meaningful effects on liver fat, liver function values, and liver fibrosis.
In addition, pemafibrate may be useful in the treatment of primary biliary cholangitis because, like obeticholic acid, fenofibrate and bezafibrate [40,41,42], pemafibrate decreases both ALP and total bilirubin. The expression of genes related to bile acid metabolism is included in the factors regulated by PPARα, and PPARα agonists may improve cholestasis [43]. Pemafibrate also provides more potent ALP reduction than the conventional PPARα agonist fenofibrate [16, 20], and is expected to be a useful treatment option for primary biliary cholangitis. In our study, the subgroups with high baseline values showed weak positive correlations between changes in TG and changes in ALP and γ-GT, suggesting that decreased TG may contribute to decreases in γ-GT and ALP. However, this study failed to clearly demonstrate a possible role for TG reduction in improving LFTs. Data from pemafibrate case reports of patients with severe hypertriglyceridemia (TG exceeding 1000 mg/dL) showed liver function test values within the normal range [44], suggesting that TG does not necessarily correlate with liver function values.
FGF21 plays a critical role in metabolic regulation [45, 46], and its analog has reportedly improved glucose and lipid metabolism and NAFLD in clinical trials [47, 48]. In our study, the pemafibrate groups showed increased FGF21, with the greatest increase in the 0.4 mg/day group. That group also experienced the greatest reduction in TG and the greatest improvement in LFTs. After administration of an FGF21 analog, FGF21 blood levels were reported to be within a range of 17.5 to 150 ng/mL [47]. However, in our study, FGF21 blood levels ranged from 610.0 pg/mL to approximately 1000 pg/mL (= 1 ng/mL), even for pemafibrate 0.4 mg/day (changed by + 369.5 pg/mL). These results clearly did not reach the level achieved by the FGF21 analog. In addition, although patients with high baseline values tended to show a negative correlation between changes in blood FGF21 and changes in ALP/total bilirubin, the relationship was not statistically significant. However, it remains possible that pemafibrate-induced increases in FGF21 may have beneficial effects on the liver, because FGF21 may affect the liver or local nerve tissue in a paracrine manner [46]. Pemafibrate is also expected to ameliorate NASH by improving lipid turnover, promoting energy metabolism, and reducing insulin resistance and inflammation [39]. Future research is needed to understand how pemafibrate and FGF21 are related to lipid metabolism, glucose metabolism, and liver function improvement.
Limitations
This study had some limitations. It was a post-hoc analysis of pooled data from multiple prospective randomized controlled trials. The study was limited to Japanese hypertriglyceridemic subjects, so the possibility of racial differences needs to be addressed. Further pharmacophysiological research is needed to clarify how pemafibrate improved glucose metabolism and LFTs. In addition, our study did not resolve the question of whether improvement in LFT values would lead to improvement of NASH or NAFLD; we hope that a phase 2 study of pemafibrate on NAFLD, which is currently underway, will provide answers to these questions.
Conclusions
In addition to improving TG and HDL-C, pemafibrate favorably affected glucose metabolism markers, LFTs, and FGF21. These effects were particularly notable among patients with high baseline values for glucose and liver function, and tended to be greatest in the 0.4 mg/day group. Mechanisms of action should be further explored for these effects of pemafibrate.
Availability of data and materials
Data in this study were used under license, and are not publicly available.
Abbreviations
- T2D:
-
Type 2 diabetes
- NAFLD:
-
Non-alcoholic fatty liver disease
- PPAR:
-
Peroxisome proliferator-activated receptor
- TG:
-
Triglyceride
- SPPARMα:
-
Selective PPAR α modulator
- HDL-C:
-
High-density lipoprotein cholesterol
- LFT:
-
Liver function test
- ALT:
-
Alanine aminotransferase
- γ-GT:
-
γ-Glutamyl transferase
- ALP:
-
Alkaline phosphatase
- FGF:
-
Fibroblast growth factor
- HOMA-IR:
-
Homeostatic model assessment of insulin resistance
- HbA1c:
-
Hemoglobin A1c
- AST:
-
Aspartate aminotransferase
- ELISA:
-
Enzyme linked immunosorbent assay
- FAS:
-
Full analysis set
- LOCF:
-
Last observation carried forward
- LS:
-
Least squares
- CI:
-
Confidence interval
- ANCOVA:
-
Analysis of covariance
- SAS:
-
Safety analysis set
- BMI:
-
Body mass index
- SD:
-
Standard deviation
- eGFR:
-
Estimated glomerular filtration rate
- SAE:
-
Serious adverse event
- LDL-C:
-
Low-density lipoprotein cholesterol
- OGTT:
-
Oral glucose tolerance test
- ABCA1:
-
ATP-binding cassette transporter A1
- 8-OHdG:
-
8-Hydroxy-2’-deoxyguanosine
- NASH:
-
Non-alcoholic steatohepatitis
- FXR:
-
Farnesoid X nuclear receptor
References
Vergés B. Pathophysiology of diabetic dyslipidaemia: where are we? Diabetologia. 2015;58(5):886–99.
Katsiki N, Mikhailidis DP, Mantzoros CS. Non-alcoholic fatty liver disease and dyslipidemia: an update. Metabolism. 2016;65(8):1109–23.
Fujihara K, Sugawara A, Heianza Y, Sairenchi T, Irie F, Iso H, et al. Utility of the triglyceride level for predicting incident diabetes mellitus according to the fasting status and body mass index category: the Ibaraki Prefectural Health Study. J Atheroscler Thromb. 2014;21(11):1152–69.
Eguchi Y, Hyogo H, Ono M, Mizuta T, Ono N, Fujimoto K, et al. JSG-NAFLD. Prevalence and associated metabolic factors of nonalcoholic fatty liver disease in the general population from 2009 to 2010 in Japan: a multicenter large retrospective study. J Gastroenterol. 2012;47(5):586–95.
Sarwar N, Gao P, Seshasai S, Gobin R, Kaptoge S, Di Angelantonio E, et al. the Emerging Risk Factors Collaboration. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375(9733):2215–22.
Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol. 2016;65(3):589–600.
Bonora E, Kiechl S, Willeit J, Oberhollenzer F, Egger G, Meigs JB, et al. Insulin resistance as estimated by homeostasis model assessment predicts incident symptomatic cardiovascular disease in Caucasian subjects from the general population: the Bruneck Study. Diabetes Care. 2007;30(2):318–24.
Kunutsor SK, Apekey TA, Khan H. Liver enzymes and risk of cardiovascular disease in the general population: a meta-analysis of prospective cohort studies. Atherosclerosis. 2014;236(1):7–17.
Okopień B, Buldak L, Boldys A. Fibrates in the management of atherogenic dyslipidemia. Expert Rev Cardiovasc Ther. 2017;15(12):913–21.
Fruchart JC. Pemafibrate (K-877), a novel selective peroxisome proliferator-activated receptor alpha modulator for management of atherogenic dyslipidaemia. Cardiovasc Diabetol. 2017;16(1):124.
Fruchart JC, Santos RD, Aguilar-Salinas C, Aikawa M, Al Rasadi K, Amarenco P, et al. The selective peroxisome proliferator-activated receptor alpha modulator (SPPARMα) paradigm: conceptual framework and therapeutic potential: a consensus statement from the International Atherosclerosis Society (IAS) and the Residual Risk Reduction Initiative (R3i) Foundation. Cardiovasc Diabetol. 2019;18(1):71.
Yamamoto Y, Takei K, Arulmozhiraja S, Sladek V, Matsuo N, Han SI, et al. Molecular association model of PPARα and its new specific and efficient ligand, pemafibrate: structural basis for SPPARMα. Biochem Biophys Res Commun. 2018;499(2):239–45.
Kawasaki M, Kambe A, Yamamoto Y, Arulmozhiraja S, Ito S, Nakagawa Y, et al. Elucidation of molecular mechanism of a selective PPARα modulator, pemafibrate, through combinational approaches of X-ray crystallography, thermodynamic analysis, and first-principle calculations. Int J Mol Sci. 2020;21(1):361.
Raza-Iqbal S, Tanaka T, Anai M, Inagaki T, Matsumura Y, Ikeda K, et al. Transcriptome analysis of K-877 (a novel selective PPARα Modulator (SPPARMα))-regulated genes in primary human hepatocytes and the mouse liver. J Atheroscler Thromb. 2015;22(8):754–72.
Yamashita S, Arai H, Yokote K, Araki E, Matsushita M, Nojima T, et al. Efficacy and safety of pemafibrate, a novel selective peroxisome proliferator-activated receptor α modulator (SPPARMα): pooled analysis of phase 2 and 3 studies in dyslipidemic patients with or without statin combination. Int J Mol Sci. 2019;20(22):5537.
Ishibashi S, Yamashita S, Arai H, Araki E, Yokote K, Suganami H, et al. K-877-04 Study Group. Effects of K-877, a novel selective PPARα modulator (SPPARMα), in dyslipidaemic patients: A randomized, double blind, active- and placebo-controlled, phase 2 trial. Atherosclerosis. 2016;249:36–43.
Arai H, Yamashita S, Yokote K, Araki E, Suganami H, Ishibashi S, K-877 Study Group. Efficacy and safety of pemafibrate versus fenofibrate in patients with high triglyceride and low HDL cholesterol levels: a multicenter, placebo-controlled, double-blind, randomized trial. J Atheroscler Thromb. 2018;25(6):521–38.
Arai H, Yamashita S, Yokote K, Araki E, Suganami H, Ishibashi S, K-877 Study Group. Efficacy and safety of K-877, a novel selective peroxisome proliferator-activated receptor α modulator (SPPARMα), in combination with statin treatment: two randomised, double-blind, placebo-controlled clinical trials in patients with dyslipidaemia. Atherosclerosis. 2017;261:144–52.
Araki E, Yamashita S, Arai H, Yokote K, Satoh J, Inoguchi T, et al. Effects of pemafibrate, a novel selective PPARα modulator, on lipid and glucose metabolism in patients with type 2 diabetes and hypertriglyceridemia: a randomized, double-blind, placebo-controlled, phase 3 trial. Diabetes Care. 2018;41(3):538–46.
Ishibashi S, Arai H, Yokote K, Araki E, Suganami H, Yamashita S, K-877 Study Group. Efficacy and safety of pemafibrate (K-877), a selective peroxisome proliferator-activated receptor α modulator, in patients with dyslipidemia: results from a 24-week, randomized, double blind, active-controlled, phase 3 trial. J Clin Lipidol. 2018;12(1):173–84.
Yokote K, Yamashita S, Arai H, Araki E, Suganami H, Ishibashi S, K-877 Study Group. Long-term efficacy and safety of pemafibrate, a novel selective peroxisome proliferator-activated receptor-α modulator (SPPARMα), in dyslipidemic patients with renal impairment. Int J Mol Sci. 2019;20(3):706.
Araki E, Yamashita S, Arai H, Yokote K, Satoh J, Inoguchi T, et al. Efficacy and safety of pemafibrate in people with type 2 diabetes and elevated triglyceride levels: 52-week data from the PROVIDE study. Diabetes Obes Metab. 2019;21(7):1737–44.
Ida S, Kaneko R, Murata K. Efficacy and safety of pemafibrate administration in patients with dyslipidemia: a systematic review and meta-analysis. Cardiovasc Diabetol. 2019;18(1):38.
Kharitonenkov A, Shiyanova TL, Koester A, Ford AM, Micanovic R, Galbreath EJ, et al. FGF-21 as a novel metabolic regulator. J Clin Invest. 2005;115(6):1627–35.
Inagaki T, Dutchak P, Zhao G, Ding X, Gautron L, Parameswara V, et al. Endocrine regulation of the fasting response by PPARα-mediated induction of fibroblast growth factor 21. Cell Metab. 2007;5(6):415–25.
Badman MK, Pissios P, Kennedy AR, Koukos G, Flier JS, Maratos-Flier E. Hepatic fibroblast growth factor 21 is regulated by PPARα and is a key mediator of hepatic lipid metabolism in ketotic states. Cell Metab. 2007;5(6):426–37.
Kharitonenkov A, Wroblewski VJ, Koester A, Chen YF, Clutinger CK, Tigno XT, et al. The metabolic state of diabetic monkeys is regulated by fibroblast growth factor-21. Endocrinology. 2007;148(2):774–81.
Xu J, Lloyd DJ, Hale C, Stanislaus S, Chen M, Sivits G, et al. Fibroblast growth factor 21 reverses hepatic steatosis, increases energy expenditure, and improves insulin sensitivity in diet-induced obese mice. Diabetes. 2009;58(1):250–59.
Matsuba I, Matsuba R, Ishibashi S, Yamashita S, Arai H, Yokote K, et al. Effects of a novel selective peroxisome proliferator-activated receptor-α modulator, pemafibrate, on hepatic and peripheral glucose uptake in patients with hypertriglyceridemia and insulin resistance. J Diabetes Investig. 2018;9(6):1323–32.
Japan Diabetes Society. Diabetes mellitus: the disease itself. In: Japan Diabetes Society, editor. Treatment guide for diabetes 2020–2021. Tokyo: Bunkodo; 2020. pp. 14–21.
Araki M, Nakagawa Y, Oishi A, Han SI, Wang Y, Kumagai K, et al. The peroxisome proliferator-activated receptor α (PPARα) agonist pemafibrate protects against diet-induced obesity in mice. Int J Mol Sci. 2018;19(7):2148.
Dong T, Lyu J, Imachi H, Kobayashi T, Fukunaga K, Sato S, et al. Selective peroxisome proliferator-activated receptor-α modulator K-877 regulates the expression of ATP-binding cassette transporter A1 in pancreatic beta cells. Eur J Pharmacol. 2018;838:78–84.
Maki T, Maeda Y, Sonoda N, Makimura H, Kimura S, Maeno S, et al. Renoprotective effect of a novel selective PPARα modulator K-877 in db/db mice: a role of diacylglycerol-protein kinase C-NAD(P)H oxidase pathway. Metabolism. 2017;71:33–45.
Simental-Mendía LE, Simental-Mendía M, Sánchez-García A, Banach M, Atkin SL, Gotto AM Jr, et al. Effect of fibrates on glycemic parameters: a systematic review and meta-analysis of randomized placebo-controlled trials. Pharmacol Res. 2018;132:232–41.
Panz VR, Wing JR, Raal FJ, Kedda MA, Joffe BI. Improved glucose tolerance after effective lipid-lowering therapy with bezafibrate in a patient with lipoatrophic diabetes mellitus: a putative role for Randle’s cycle in its pathogenesis? Clin Endocrinol (Oxf). 1997;46(3):365–8.
Belfort R, Berria R, Cornell J, Cusi K. Fenofibrate reduces systemic inflammation markers independent of its effects on lipid and glucose metabolism in patients with the metabolic syndrome. J Clin Endocrinol Metab. 2010;95(2):829–36.
Kusunoki M, Sakazaki T, Tsutsumi K, Miyata T, Oshida Y. The effects of pemafibrate in Japanese patients with type 2 diabetes receiving HMG-CoA reductase inhibitors. Endocr Metab Immune Disord Drug Targets. 2021;21(5):919–24.
Neuschwander-Tetri BA, Loomba R, Sanyal AJ, Lavine JE, Van Natta ML, Abdelmalek MF, et al. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet. 2015;385(9972):956–65.
Honda Y, Kessoku T, Ogawa Y, Tomeno W, Imajo K, Fujita K, et al. Pemafibrate, a novel selective peroxisome proliferator-activated receptor alpha modulator, improves the pathogenesis in a rodent model of nonalcoholic steatohepatitis. Sci Rep. 2017;7:42477.
Nevens F, Andreone P, Mazzella G, Strasser SI, Bowlus C, Invernizzi P, et al. POISE Study Group. A placebo-controlled trial of obeticholic acid in primary biliary cholangitis. N Engl J Med. 2016;375(7):631–43.
Suraweera D, Rahal H, Jimenez M, Viramontes M, Choi G, Saab S. Treatment of primary biliary cholangitis ursodeoxycholic acid non-responders: a systematic review. Liver Int. 2017;37(12):1877–86.
Corpechot C, Chazouilléres O, Rousseau A, Le Gruyer A, Habersetzer F, Mathurin P, et al. A placebo-controlled trial of bezafibrate in primary biliary cholangitis. N Engl J Med. 2018;378(23):2171–81.
Ghonem NS, Assis DN, Boyer JL. Fibrates and cholestasis. Hepatology. 2015;62(2):635–43.
Iitake C, Masuda D, Koseki M, Yamashita S. Marked effects of novel selective peroxisome proliferator-activated receptor α modulator, pemafibrate in severe hypertriglyceridemia: preliminary report. Cardiovasc Diabetol. 2020;19(1):201.
Kliewer SA, Mangelsdorf DJ. A dozen years of discovery: insights into the physiology and pharmacology of FGF21. Cell Metab. 2019;29(2):246–53.
Li X. The FGF metabolic axis. Front Med. 2019;13(5):511–30.
Gaich G, Chien JY, Fu H, Glass LC, Deeg MA, Holland WL, et al. The effects of LY2405319, an FGF21 analog, in obese human subjects with type 2 diabetes. Cell Metab. 2013;18(3):333–40.
Sanyal A, Charles ED, Neuschwander-Tetri BA, Loomba R, Harrison SA, Abdelmalek MF, et al. Pegbelfermin (BMS-986036), a PEGylated fibroblast growth factor 21 analogue, in patients with non-alcoholic steatohepatitis: a randomised, double-blind, placebo-controlled, phase 2a trial. Lancet. 2018;392(10165):2705–17.
Acknowledgements
We acknowledge the investigators and patients who participated in these studies. Medical writing support was provided by EDIT, Inc. (Tokyo, Japan) and was funded by Kowa Company, Ltd.
Funding
This study was funded by Kowa Company, Ltd. The study sponsor had a role in the study design; data collection, analysis, and interpretation; and writing of the report.
Author information
Authors and Affiliations
Contributions
KY, SY, HA, EA, HS, and SI contributed to the concept, design, and execution of the study, and to the interpretation of the data. KY contributed substantially to the writing and critical review of the manuscript. SY, HA, EA, and SI contributed to the critical review of the manuscript. MM, TN, and HS are the guarantors of this work and, as such, had full access to all data in the study and take responsibility for data integrity and the accuracy of data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This pooled analysis was approved by the Ethics Committee of Chiba University Graduate School of Medicine. The sub-studies that constitute this study were approved by the institutional review boards at their respective study sites, and written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
KY has received personal fees and grants from Kowa Company, Ltd., MSD K.K., Astellas Pharma Inc., Mitsubishi Tanabe Pharma Corporation, Takeda Pharmaceutical Company Limited, Ono Pharmaceutical Co., Ltd., Daiichi Sankyo Company, Limited, Sumitomo Dainippon Pharma Co., Ltd., Pfizer Japan Inc., Novo Nordisk Pharma Ltd., Nippon Boehringer Ingelheim Co., Ltd., Eli Lilly Japan K.K., and Taisho Pharmaceutical Co., Ltd., personal fees from Amgen K.K., Sanofi K.K., AstraZeneca K.K., Novartis Pharma K.K., Kyowa Kirin Co., Ltd., and Janssen Pharmaceutical K.K., grants from Kao Corporation, Teijin Pharma Limited, Shionogi & Co., Ltd., and Bayer Yakuhin, Ltd, and holds an endowed chair funded by MSD K.K. SY has received personal fees and grants from MSD K.K., personal fees from Kowa Company, Ltd., Amgen K.K., and Sanofi K.K., and grants from Bayer Yakuhin, Ltd., Nippon Boehringer Ingelheim Co., Ltd., Takeda Pharmaceutical Company Limited, Ono Pharmaceutical Co., Ltd., Astellas Pharma Inc., Mitsubishi Tanabe Pharma Corporation, Hitachi Chemical Diagnostics Systems Co., Ltd., and Rohto Pharmaceutical Co., Ltd. HA has received personal fees from Sanofi K.K., Daiichi Sankyo Company, Limited, Astellas Pharma Inc., MSD K.K., Abbott Japan LLC, Kowa Company, Ltd., Amgen K.K., Pfizer Japan Inc., Takeda Pharmaceutical Company Limited, Otsuka Pharmaceutical Co., Ltd., and UCB Japan Co. Ltd. EA has received personal fees and grants from Kowa Company, Ltd., Sanofi K.K., Mitsubishi Tanabe Pharma Corporation, Sumitomo Dainippon Pharma Co., Ltd., and Novo Nordisk Pharma Ltd., personal fees from AstraZeneca K.K., MSD K.K., and Ono Pharmaceutical Co., Ltd., grants from Astellas Pharma Inc., Daiichi Sankyo Company, Limited, Taisho Pharmaceutical Co., Ltd., Takeda Pharmaceutical Company Limited, Nippon Boehringer Ingelheim Co., Ltd., Eli Lilly Japan K.K., Novartis Pharma K.K., Bayer Yakuhin, Ltd., and Pfizer Japan Inc., and holds an endowed chair funded by MSD K.K., Ono Pharmaceutical Co., Ltd., and Terumo Corporation. MM, TN, and HS are employees of Kowa Company, Ltd. SI has received personal fees from Kowa Company, Ltd., and grants from Ono Pharmaceutical Co., Ltd.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Summary of six randomized double-blind placebo-controlled clinical trials of pemafibrate. Table S2. Correlations between changes in fasting plasma glucose, fasting serum insulin and HOMA-IR, and changes in TG and FGF21 from baseline to Week 12 (LOCF): correlation coefficients from Pearson and Spearman analyses, with the respective p-values. Table S3. Correlations between changes in liver function tests and changes in TG and FGF21 from baseline to Week 12 (LOCF): correlation coefficients from Pearson and Spearman analyses, with the respective p-values. Figure S1. Subject disposition. Figure S2. Changes in glucose metabolism markers, from baseline to Week 12 (LOCF), by presence or absence of type 2 diabetes. Figure S3. Changes in glucose metabolism markers, from baseline to Week 12 (LOCF), by presence or absence of fatty liver. Figure S4. Changes in liver function tests, from baseline to Week 12 (LOCF), by presence or absence of type 2 diabetes. Figure S5. Changes in liver function tests, from baseline to Week 12 (LOCF), by presence or absence of fatty liver.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yokote, K., Yamashita, S., Arai, H. et al. Effects of pemafibrate on glucose metabolism markers and liver function tests in patients with hypertriglyceridemia: a pooled analysis of six phase 2 and phase 3 randomized double‐blind placebo‐controlled clinical trials. Cardiovasc Diabetol 20, 96 (2021). https://doi.org/10.1186/s12933-021-01291-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-021-01291-w