
Abstract
Background
The recognition of asthma-chronic obstructive pulmonary disease (COPD) overlap (ACO) as a distinct phenotype of COPD or asthma has increased. Although ACO has worse clinical features than non-ACO COPD, limited information is available on long-term outcomes of lung function decline for ACO and non-ACO COPD.
Methods
COPD patients with at least 3 years of follow-up were selected from the Korean Obstructive Lung Disease cohort. ACO was defined based on 3 major criteria: 1) airflow limitation in individuals 40 years of age and older, 2) ≥10 pack-years of smoking history, and 3) a history of asthma or bronchodilator response of > 400 mL in forced expiratory volume in 1 s (FEV1) at baseline; and at least 1 minor criterion: 1) history of atopy or allergic rhinitis, 2) two separated bronchodilator responses of ≥12% and 200 mL in FEV1, or 3) peripheral blood eosinophils ≥300 cells/μL. Lung function decline was compared using a linear mixed effects model for longitudinal data with random intercept and random slope.
Results
Among 239 patients, 47 were diagnosed with ACO (19.7%). During the follow-up period, change in smoking status, use of inhaled corticosteroids (ICS) and long-acting β2-agonists or ICS and at least 2 exacerbations per year were similar between patients with non-ACO COPD and ACO. Over a median follow-up duration of 5.8 years, patients with non-ACO COPD experienced a faster annual decline in pre-bronchodilator FEV1 than patients with ACO (− 29.3 ml/year vs. -13.9 ml/year, P = 0.042), which was persistent after adjustment for confounders affecting lung function decline.
Conclusion
Patients with ACO showed favorable longitudinal changes in lung function compared to COPD patients over a median follow-up of 5.8 years.
Similar content being viewed by others


Background
Recognition of asthma-chronic obstructive pulmonary disease overlap (ACO) as a distinct phenotype of COPD is increasing [1, 2]. The proportion of ACO varies considerably depending on the diagnostic criteria that are applied, but the overall prevalence of asthma-COPD overlap is approximately 15–30% among patients with obstructive airway disease and 2% among adult population samples [3,4,5,6].
Diagnostic criteria for ACO with major and minor criteria were initially proposed by a group of experts in Spain [7]. These have been modified more recently [4]. With growing attention to ACO, a joint project of the Global Initiative for Asthma (GINA) and the Global Initiative for Chronic Obstructive Lung Disease (GOLD) provided a clinical description of asthma-COPD overlap (ACO) that is characterized by persistent airflow limitation with several features usually associated with asthma and several features usually associated with COPD. From the list of common features of asthma and COPD, a diagnosis of ACO is suggested if a similar number of features are found for both asthma and COPD [8]. Due to the imprecise and complicated approach to using the proposed ACO criteria, an operational definition of ACO for clinical and epidemiological application has been advocated by expert consensus from a round table discussion [9].
These attempts to define and diagnose ACO are attributed to different health-care burden and treatment implications. Compared with non-ACO COPD, patients with ACO experience more frequent symptoms of dyspnea and exacerbations with hospitalizations, leading to frequent use of healthcare services and higher healthcare costs [10,11,12]. Accordingly, patients with ACO are considered to have greater disease severity and a worse prognosis than patients with non-ACO COPD. However, some studies have found the opposite with ACO patients having similar or better prognosis than non-ACO COPD patients [4, 13, 14]. Lung function decline is often used to assess disease progression in COPD and the data on the impact of ACO on disease progression as defined by loss of lung function over time is controversial owing to differences in case definitions of ACO and relative inhomogeneity of the study populations [15,16,17]. Thus, we aimed to investigate lung function decline between ACO and non-ACO COPD by using a standardized (albeit imperfect) definition of ACO from an expert consensus panel [9] in a relatively homogenous sample of largely male COPD patients in Korea.
Methods
Study population
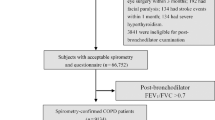
Participants in this study were 239 patients with COPD from the Korean Obstructive Lung Disease (KOLD) cohort. Details of the KOLD study were published previously [18]. Recruitment occurred in pulmonary clinics across 16 hospitals in the Republic of Korea from June 2005 to October 2012. Inclusion criteria for the present study were: 1) 40 years of age and older; 2) COPD, as defined by post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) < 0.7 and more than 10 pack-years of smoking history; 3) no history or radiographic evidence of tuberculosis, bronchiectasis or other pulmonary disorders; and 4) at least 3 years follow-up. At each visit, smoking status was surveyed with a series of questions. Patients were categorized as sustained quitters if they were nonsmokers at each visit. Patients who were smokers at each visit were defined as continued smokers and those whose smoking behavior varied were classified as intermittent quitters. The study protocol was approved by the Institutional Review Board of Asan Medical Center (no. 2005–0010). Written informed consent was obtained from all participants.
Definition of ACO
Among patients with COPD, those who satisfied three major and at least one minor criterion were classified as ACO patients [9]. Major criteria were: 1) post-bronchodilator FEV1/FVC < 0.7, 2) at least 10 pack-years of smoking history, and 3) history of asthma or bronchodilator response to salbutamol/albuterol > 400 mL in FEV1 at baseline. Minor criteria were: 1) history of atopy or allergic rhinitis, 2) two separated bronchodilator responses to salbutamol/albuterol ≥12% and 200 mL in FEV1 during the initial 3-year follow-up period of the cohort, or 3) peripheral blood eosinophils ≥300 cells/uL.
Pulmonary function test and computed tomography data acquisition
Spirometry was performed according to recommendations of the American Thoracic Society/European Respiratory Society (Vmax 22, Sensor-Medics, Yorba Linda, CA, USA; PFDX, MedGraphics, St. Paul, MN, USA) [19]. Absolute values of FVC and FEV1 were obtained, and percentage of the predicted values (% pred) for FEV1 and FVC were calculated from equations obtained with a representative Korean sample [20]. Reversibility was defined as post-bronchodilator increase in FEV1 of at least 12% and 200 mL from baseline values.
Details of computed tomography data acquisition and analysis from the KOLD study were published previously [21]. Using in-house software, whole lung images were extracted automatically and attenuation coefficient of each pixel was measured and calculated. Emphysema was defined as a percentage of lung attenuation less than 950 Hounsfield units. Percent emphysema was determined for total lung.
Statistical analysis
The primary objective of this study was assessing longitudinal changes in pre-bronchodilator FEV1 (mL). We compared serial changes in pre-bronchodilator FEV1 (mL) between patients with non-ACO COPD and ACO using a linear mixed effects model for longitudinal data with random intercepts and random slopes [22]. After enrollment in the KOLD cohort, some patients underwent a 2-week washout period and then received treatment including a 3-month fixed-dose combination inhaler of inhaled corticosteroids (ICS) and long-acting β2-agonists (LABA) [23]. Patients whose condition did not allow cessation of medications did not undergo the washout and maintained original treatment. This decision was made at the discretion of treating physicians. Since patients who underwent 2-week washout and initiated bronchodilators at enrollment often experienced an increase in FEV1 during the first 3 months, we used pre-bronchodilator FEV1 at 3 months as the baseline. Due to absence of post-bronchodilator FEV1 at 3 months, pre-bronchodilator FEV1 was evaluated for lung function decline. We applied three models with increasing degrees of adjustment to account for potential confounding factors. Model 1 was adjusted for baseline age, baseline body mass index (BMI) and smoking status during study period. Model 2 was further adjusted for at least 2 exacerbations per a year during study period. In addition, to evaluate potential mediation of the association between presence of ACO and pre-bronchodilator FEV1 changes, model 3 was further adjusted for use of ICS/LABA or ICS during study period. The use of ICS/LABA or ICS was defined as ICS/LABA or ICS was prescribed longer than two-thirds of a study period. All reported P values were two-sided and the significance level was set at 0.05. Statistical analyses were performed using Stata (version 14; Stata Corp., College Station, TX).
Results
In this study, 47 patients (19.7%) fulfilled the definition of ACO (Table 1 and Additional file 1: Table S1). Compared with patients with non-ACO COPD, no significant differences were observed in age, sex, smoking history, education status, modified medical research council ≥2, two or more exacerbations in the previous year and other comorbidities except for bronchial asthma between patients with ACO and non-ACO COPD. While baseline FEV1 was similar between non-ACO COPD and ACO (1471.7 mL vs. 1545.5 mL, P = 0.38; 48.3% pred vs. 49.7% pred, P = 0.56), baseline post-bronchodilator FEV1 was higher for ACO than non-ACO COPD (1816.2 mL vs. 1618.5 mL, P = 0.02; 58.3% pred vs. 53.1% pred, P = 0.04). Reversibility was significantly higher for ACO than non-ACO COPD, while emphysema index was significantly higher for non-ACO COPD than ACO (22.1% vs. 17.1%, P = 0.04). For medications, use of long-acting muscarinic antagonists and ICS/LABA or ICS prescription were similar between non-ACO COPD and ACO (Table 2).
The median time from baseline spirometry to the last spirometry was 5.8 years (maximum 8.8 years). During follow-up, changes in smoking status, use of ICS/LABA or ICS and at least 2 exacerbations per year were similar between non-ACO COPD and ACO patients (Table 3). During follow-up, patients with non-ACO COPD had a significantly faster annual decline in pre-bronchodilator FEV1 than patients with ACO (− 29.26 mL vs. -13.87 mL, P = 0.042) (Table 4 and Fig. 1). The results did not substantially change after adjusting for other confounders such as baseline age, baseline BMI, change in smoking status during study period, exacerbations during study period and use of ICS/LABA or ICS during the study period (Table 4).

Longitudinal Changes in pre-bronchodilator forced expiratory volume in 1 s (mL) during the follow-up period in non-ACO COPD (n = 192) and ACO (n = 47). Error bar represents 95% confidence interval. ACO, asthma-chronic obstructive pulmonary disease overlap syndrome; COPD, chronic obstructive lung disease
Discussion
We found that patients with ACO experienced a slower annual decline in FEV1 compared to patients with non-ACO COPD over a median follow-up period of 5.8 years. This finding persisted after adjustment for confounders affecting lung function decline such as change in smoking status, exacerbations and use of ICS/LABA or ICS during the study. Our data are consistent with those of the Hokkaido COPD cohort study [24], which did not include patients with history of asthma but demonstrated a significantly slower annual lung function decline in COPD patients with the presence of three asthma-like features such as blood eosinophilia, reversibility and atopy compared to COPD without asthma-like features. We extended the data of the Hokkaido COPD cohort study by showing that patients with ACO had a slower annual decline in FEV1 than patients with non-ACO COPD. Our data also affirmed the finding of a cohort study of obstructive airway diseases with more patients and a longer follow-up period. Previous data showed that there was a significant decline in FEV1 over the 4-year period within non-ACO COPD not within ACO, but there were no significant differences in FEV1 changes between two groups. These might be explained by the lack of sufficient power to detect differences in lung function decline due to relatively small sample size (n = 91) and shorter follow-up period [17].
Two other studies evaluated lung function decline between ACO and non-ACO COPD [15, 16]. One was a population-based study that used a self-reported definition of asthma [15]. This study showed that lung function decline for ACO was affected by the age of asthma recognition. Compared with non-ACO COPD, decline in FEV1 for ACO with late asthma onset was significantly higher but decline in FEV1 for ACO with early asthma onset was significantly lower. The other study used data from the European Community Respiratory Health Survey (participants aged 20–44 years) and showed that FEV1 change in the ACO group was lower than in the COPD group [16]. On further inspection of these two studies, compared with non-ACO COPD, the numbers for initial FEV1 < 80% of predicted were significantly higher for ACO with early asthma onset (50% vs. 71%) in the former study and ACO patients (16.4% vs. 33.1%) in latter study. Given that lung function decline accelerates in the initial phase of COPD with preserved FEV1 [25], a smaller change in lung function for ACO with early asthma onset in these previous data compared to non-ACO COPD could be attributed to low baseline FEV1. However, in our study, baseline pre-bronchodilator FEV1 was similar for non-ACO COPD and ACO, and post-bronchodilator FEV1 was higher for ACO than non-ACO COPD. In addition, changes in smoking status and numbers of frequent exacerbations during follow-up were similar for ACO and non-ACO COPD, suggesting that favorable lung function decline in ACO compared to non-ACO COPD could be true signal.
The presence of bronchodilator reversibility has been widely used as a criterion in the classification of ACO [4, 7, 17]. Previous studies reported the association between bronchodilator reversibility and lung function decline with conflict results in COPD patients [24, 26,27,28]. Our data showed a higher rate of bronchodilator reversibility for ACO than non-ACO COPD owing to the inclusion of bronchodilator responses in the case definition of ACO that was used in this study, and the variance of FEV1 at each year tended to be wider for ACO than non-ACO COPD (Fig. 1). However, the presence of baseline reversibility in our study did not affect overall lung function decline (data not shown), which was in agreement with the data of the Lung Health Study, Inhaled Steroids in Obstructive Lung Disease in Europe (ISOLDE) study and Hokkaido COPD cohort study [24, 26, 27]. Thus, the effect of bronchodilator reversibility on a slower lung function decline in ACO would not be significant.
When only patients with ACO were analyzed based on ICS/LABA or ICS treatment, a trend towards reduced annual rate of decline in FEV1 was found for patients with ACO receiving ICS/LABA or ICS treatment during follow-up compared with those without ICS/LABA or ICS treatment (Additional file 1: Table S2). However, no significant difference was observed in annual rate of FEV1 decline for patients with ACO based on use of ICS/LABA or ICS, which might be due to the small sample size. Given that our findings were from retrospective observational studies, a prospective study is needed to validate the effects of ICS on ACO.
Our study has several limitations. First, as the KOLD prospective cohort was not originally designed to compare lung function decline between ACO and non-ACO COPD, our study design and analysis had to be retrospective in nature. Accordingly, we did not compare lung function decline for non-ACO COPD with ACO using different ACO criteria. In particular, ACO criteria proposed by a joint project of GINA and GOLD [8] could not be applied because some data were missing to determine ACO or non-ACO COPD. Second, a history of asthma before 40 years of age could not be used because the age of asthma diagnosis was not investigated in the KOLD cohort. Thus, we modified the ACO criteria with “history of asthma”. Further studies are necessary to investigate lung function decline for ACO based on age of asthma diagnosis in the COPD cohort. Third, despite a long-term follow-up, the sample size might be small to make conclusion. A prospective study with a larger sample size is needed to validate these findings. Finally, 97% of the study population was male. This can be explained by the high prevalence of male smokers in Korea [29]. Thus, our results may be limited to a generalization of female patients.
Conclusions
We found that the longitudinal change in lung function was lower in patients with ACO than patients with COPD over a median follow-up of 5.8 years. This finding suggested that ACO has favorable long-term outcomes in lung function decline compared with non-ACO COPD in a cohort of Korean patients with COPD.
Abbreviations
- ACO:
-
Asthma-chronic obstructive pulmonary disease overlap
- BMI:
-
Body mass index
- COPD:
-
Chronic obstructive lung disease
- FEV1 :
-
Forced expiratory volume in 1 s
- FVC:
-
Forced vital capacity
- GINA:
-
Global Initiative for Asthma
- GOLD:
-
Global Initiative for Chronic Obstructive Lung Disease
- ICS:
-
Inhaled corticosteroids
- KOLD:
-
Korean Obstructive Lung Disease
- LABA:
-
Long-acting β2-agonists
References
Barnes PJ. Asthma-COPD overlap. Chest. 2016;149:7–8.
Kostikas K, Clemens A, Patalano F. The asthma-COPD overlap syndrome: do we really need another syndrome in the already complex matrix of airway disease? Int J Chron Obstruct Pulmon Dis. 2016;11:1297–306.
Alshabanat A, Zafari Z, Albanyan O, Dairi M, FitzGerald JM. Asthma and COPD overlap syndrome (ACOS): a systematic review and meta analysis. PLoS One. 2015;10:e0136065.
Cosio BG, Soriano JB, Lopez-Campos JL, Calle-Rubio M, Soler-Cataluna JJ, de-Torres JP, et al. Defining the asthma-COPD overlap syndrome in a COPD cohort. Chest. 2016;149:45–52.
Tho NV, Park HY, Nakano Y. Asthma-COPD overlap syndrome (ACOS): a diagnostic challenge. Respirology. 2016;21:410–8.
Menezes AM, Montes de Oca M, Perez-Padilla R, Nadeau G, Wehrmeister FC, Lopez-Varela MV, et al. Increased risk of exacerbation and hospitalization in subjects with an overlap phenotype: COPD-asthma. Chest. 2014;145:297–304.
Soler-Cataluna JJ, Cosio B, Izquierdo JL, Lopez-Campos JL, Marin JM, Aguero R, et al. Consensus document on the overlap phenotype COPD-asthma in COPD. Arch Bronconeumol. 2012;48:331–7.
GINA. Global Strategy for Asthma Management and Prevention (2017 update). Available at http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-management-and-prevention/. Assessed 15 Sept 2017.
Sin DD, Miravitlles M, Mannino DM, Soriano JB, Price D, Celli BR, et al. What is asthma-COPD overlap syndrome? Towards a consensus definition from a round table discussion. Eur Respir J. 2016;48:664–73.
Hardin M, Silverman EK, Barr RG, Hansel NN, Schroeder JD, Make BJ, et al. The clinical features of the overlap between COPD and asthma. Respir Res. 2011;12:127.
Miravitlles M, Soriano JB, Ancochea J, Munoz L, Duran-Tauleria E, Sanchez G, et al. Characterisation of the overlap COPD-asthma phenotype. Focus on physical activity and health status. Respir Med. 2013;107:1053–60.
Sadatsafavi M, Tavakoli H, Kendzerska T, Gershon A, To T, Aaron SD, et al. History of asthma in patients with chronic obstructive pulmonary disease. A comparative study of economic burden. Ann Am Thorac Soc. 2016;13:188–96.
Sorino C, Pedone C, Scichilone N. Fifteen-year mortality of patients with asthma-COPD overlap syndrome. Eur J Intern Med. 2016;34:72–7.
Yamauchi Y, Yasunaga H, Matsui H, Hasegawa W, Jo T, Takami K, et al. Comparison of in-hospital mortality in patients with COPD, asthma and asthma-COPD overlap exacerbations. Respirology. 2015;20:940–6.
Lange P, Colak Y, Ingebrigtsen TS, Vestbo J, Marott JL. Long-term prognosis of asthma, chronic obstructive pulmonary disease, and asthma-chronic obstructive pulmonary disease overlap in the Copenhagen City heart study: a prospective population-based analysis. Lancet Respir Med. 2016;4:454–62.
de Marco R, Marcon A, Rossi A, Anto JM, Cerveri I, Gislason T, et al. Asthma, COPD and overlap syndrome: a longitudinal study in young European adults. Eur Respir J. 2015;46:671–9.
Fu JJ, Gibson PG, Simpson JL, McDonald VM. Longitudinal changes in clinical outcomes in older patients with asthma, COPD and asthma-COPD overlap syndrome. Respiration. 2014;87:63–74.
Park TS, Lee JS, Seo JB, Hong Y, Yoo JW, Kang BJ, et al. Study design and outcomes of Korean obstructive lung disease (KOLD) cohort study. Tuberc Respir Dis (Seoul). 2014;76:169–74.
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–38.
Choi JK, Paek D, Lee JO. Normal predictive values of spirometry in Korean population. Tuberc Respir Dis. 2005;58:230–42.
Oh YM, Jeong BH, Woo SY, Kim SY, Kim H, Lee JH, et al. Association of plasma adipokines with chronic obstructive pulmonary disease severity and progression. Ann Am Thorac Soc. 2015;12:1005–12.
Fitzmaurice GM, Laird NM, Ware JH. Applied longitudinal analysis. 2nd ed. Hoboken: Wiley; 2011.
Lee SY, Park HY, Kim EK, Lim SY, Rhee CK, Hwang YI, et al. Combination therapy of inhaled steroids and long-acting beta2-agonists in asthma-COPD overlap syndrome. Int J Chron Obstruct Pulmon Dis. 2016;11:2797–803.
Suzuki M, Makita H, Konno S, Shimizu K, Kimura H, Kimura H, et al. Asthma-like features and clinical course of chronic obstructive pulmonary disease. An analysis from the Hokkaido COPD cohort study. Am J Respir Crit Care Med. 2016;194:1358–65.
Tantucci C, Modina D. Lung function decline in COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:95–9.
Calverley PM, Burge PS, Spencer S, Anderson JA, Jones PW. Bronchodilator reversibility testing in chronic obstructive pulmonary disease. Thorax. 2003;58:659–64.
Anthonisen NR, Lindgren PG, Tashkin DP, Kanner RE, Scanlon PD, Connett JE, et al. Bronchodilator response in the lung health study over 11 yrs. Eur Respir J. 2005;26:45–51.
Vestbo J, Edwards LD, Scanlon PD, Yates JC, Agusti A, Bakke P, et al. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365:1184–92.
Yoo KH. Smoking cessation and chronic obstructive pulmonary disease. Korean J Intern Med. 2015;30:163–6.
Acknowledgements
We thank members of the Korean Obstructive Lung Disease (KOLD) Study Group for the generous provision of data.
Funding
The KOLD Study was supported by a grant from the Korean Health 21 R&D Project, Ministry of Health and Welfare, Republic of Korea (HI10C2020 and A102065). This study was supported by Samsung Medical Center Foundation for Medical Research (SMX1151371).
Availability of data and materials
Data and materials are available without undue qualifications.
Author information
Authors and Affiliations
Contributions
HYP, S-YL, DK, JC, YBP participated in the design of the study, collected and interpreted the data and wrote the manuscript. HYP, S-YL, YBP, HL, SYL, HIY, SWR, KUK, Y-MO, DDS, S-DL contributed to data analysis/interpretation and manuscript drafting/revision. YBP conceived of the study, and participated in its design and coordination. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of Asan Medical Center (no. 2005–0010). Written informed consent was obtained from all participants.
Consent for publication
The authors give our consent for publication.
Competing interests
H.Y.P. has received lecture fees from AstraZeneca, Novartis and Boehringer-Ingelheim.
D.D.S. is funded by the Canada Research Chair Program and has received honoraria for speaking engagements from Boehringer Ingelheim, AstraZenca, Regeneron and Sanofi Aventis over the past 18 months. He has also received research funding from BI, AZ and Merck during this time.
None declared (S-Y.L., D.K., J.C., H.L., S.Y.L., H.I.Y., S.W.R., K.U.K., Y-M.O., S-D.L., Y.B.P.).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. The component distribution of ACO. Table S2. Longitudinal change of annual forced expiratory volume in 1 s (mL) in ACO by use of ICS/LABA or ICS during follow up (n = 47). (DOCX 15 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Park, H.Y., Lee, SY., Kang, D. et al. Favorable longitudinal change of lung function in patients with asthma-COPD overlap from a COPD cohort. Respir Res 19, 36 (2018). https://doi.org/10.1186/s12931-018-0737-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-018-0737-8