
Abstract
Background
Whole-exome sequencing (WES) consists in the capture, sequencing and analysis of all exons in the human genome. Originally developed in the research context, this technology is now increasingly used clinically to inform patient care. The implementation of WES into healthcare poses significant organizational, regulatory, and ethical hurdles, which are widely discussed in the literature.
Methods
In order to inform future policy decisions on the integration of WES into standard clinical practice, we performed a systematic literature review to identify the most important challenges directly reported by technology users.
Results
Out of 2094 articles, we selected and analyzed 147 which reported a total of 23 different challenges linked to the production, analysis, reporting and sharing of patients’ WES data. Interpretation of variants of unknown significance, incidental findings, and the cost and reimbursement of WES-based tests were the most reported challenges across all articles.
Conclusions
WES is already used in the clinical setting, and may soon be considered the standard of care for specific medical conditions. Yet, technology users are calling for certain standards and guidelines to be published before this technology replaces more focused approaches such as gene panels sequencing. In addition, a number of infrastructural adjustments will have to be made for clinics to store, process and analyze the amounts of data produced by WES.
Similar content being viewed by others


Background
Whole-exome sequencing (WES) consists in the capture, sequencing and analysis of all exons of all protein coding genes in the human genome. Instead of analyzing the whole genome, composed of roughly 3 billion base-pairs, WES focuses only on the approximately 30 million base-pairs which are translated into functional proteins, in which mutations are the most likely to have a severe direct phenotypic consequence. WES can therefore be considered a much less costly and more efficient method of identifying all possible mutations in genes, compared to other methods such as genome-wide association studies or whole-genome sequencing (WGS) [1]. WES was originally used mainly to identify rare mutations contributing to Mendelian diseases, as compared with the many variants involved in common complex diseases [2], although this distinction can be considered artificial [3]. Methodologies evolve rapidly, and new software enable this technology to better detect complex genetic changes such as structural variants [4] and copy-number variants [5–7]. The integration of WES into healthcare is already underway, contributing to the development of personalized medicine [2]. It is currently used clinically for numerous purposes, ranging from diagnosis to disease prognosis and treatment decisions [8]. Analysing a patient’s exome through one test is now less costly than testing a number of specific genes, especially when little is known about the genetic background of the disease, although this analysis does “add layers of complexity to test interpretation” [9]. In addition to the technical challenges of making the technology fit for clinical diagnostics (improving exon capture, sequencing coverage, read length, accurate detection of insertion-deletions, and reduction of false positive and false negative rates), numerous hurdles have to be overcome to use WES in routine healthcare. A number of ethical, legal, social and policy challenges have been extensively discussed in the literature by scientific researchers as well as policymakers and professional societies [10–15]. Guidelines have been produced to respond to some of these challenges, notably that of reporting incidental findings (IF). The American College of Medical Genetics and Genomics (ACMG) published a policy recommendation on this topic in 2013 [16], which has been heavily discussed [17–20], and updated in 2014 [21]. The European Society of Human Genetics, in turn, published a recommendation in 2015 [22]. The Canadian College of Medical Geneticists published a position statement in 2015 to frame the “clinical application of genome-wide sequencing for monogenic diseases in Canada” [23]. But in order to design efficient policies aimed at enabling the responsible integration of WES into healthcare, there is the need to systematically identify what the prominent challenges are. To our knowledge no study has yet been published on the implementation hurdles identified directly by scientific researchers and medical doctors (technology users) reporting on the clinical use of WES. With this objective in mind, we designed a systematic review of the literature to identify the most important challenges directly reported by technology users.
Methods
Our systematic literature review methodology was adapted from the PRISMA guidelines [24] and the Petticrew and Roberts practical guide [25]. The completed PRISMA flow diagram and PRISMA checklist, as well as the full articles dataset are available in Additional files 1, 2 and 3.
Studies sources
6 databases were searched to identify the most comprehensive list of publications. The last search was performed on March 31st, 2015.
-
1.
EBSCO host digital archives http://www.ebscohost.com/archives
- 2.
-
3.
NCBI Pubmed http://www.ncbi.nlm.nih.gov/pubmed/
-
4.
Science Direct http://www.sciencedirect.com/
-
5.
Scopus http://www.scopus.com/
-
6.
Web of Science http://apps.webofknowledge.com/
Choice of keywords
Since our objective was to identify reports published by technology users on the clinical use of WES, we used the following keywords in combination to stringently filter out reports from outside the clinical context: Clinical application, Medical application, Healthcare, Clinical care, Medical care, Clinical practice, Clinical diagnostic, Medical practice.
Therefore, the complete search used was the following:
(“exome sequencing” OR “whole-exome sequencing” OR “whole exome sequencing”) AND (“clinical application” OR “medical application” OR “healthcare” OR “clinical care” OR “medical care” OR “clinical practice” OR “clinical diagnostic” OR “medical practice”).
Screening, filtering and selection
We searched for the chosen keywords using the full text of articles and reports without any date or language restrictions. The search resulted in 2275 articles (details available in Table 1). All results were then aggregated in a single Excel file, from which we removed duplicates, resulting in 2094 unique articles.
Further screening was done in two steps:
-
First, we screened out results that were not peer reviewed journal articles (such as abstracts from conference oral presentations or posters, blog articles, or conference programs).
-
We then removed articles that were not written in English, French or Spanish.
At this point, both GB and MH processed with filtering the articles in parallel, according to the following inclusion and exclusion criteria:
-
The articles are written by a technology user, defined as a medical doctor, life science researcher or medical researcher who is directly exposed to the technology in his field of expertise. At this point we excluded articles for which the corresponding author was a researcher in policy or human and social sciences.
-
The articles directly address WES. At this point we excluded articles which, for instance, simply referred to other studies which had used WES. We included articles that talked about other technologies in addition to WES, such as WGS or gene panels.
-
The articles discuss the clinical implementation of WES. At this point we excluded articles which only considered WES in the context of basic research or discovery.
-
The articles list unsolved implementation challenges. We excluded articles which did not mention any challenge linked to the clinical implementation of WES, which listed challenges already solved, or which described them as easy to solve through measures already partly in place. We also excluded articles which we tagged as ‘recommendations’ when they consisted of a list of solutions for the clinical implementation of WES and did not describe any challenge or issue as ‘unsolved’.
After filtering all articles separately, GB and MH compared their selected articles list, discussed any articles selected only by one of them, and agreed on a final decision for each of those articles. Only 10 % of articles required discussion (182 out of 1792 articles).
The full list of selected articles is available in Additional file 1. The results of all screening and filtering steps are described in Table 2.
Coding
Since our objective was to be as comprehensive and unbiased as possible in the identification of unsolved challenges relevant to technology users, the coding of articles was done through inductive content analysis [26, 27]. An initial list of challenges was generated by GB on the basis of an analysis of 30 articles selected at random (20 % of all selected articles). These challenges were then discussed and adjusted by all co-authors together. Some similar challenges were merged, while others were split into separate challenges. Additional challenges were added both by MH and GB over the course of the analysis if five articles or more were found to refer to any specific challenge. For the data analysis, we decided to group challenges along a typical ‘timeline’ ranging from data production, to analysis, reporting and finally sharing.
Results
Studies scope
Publication dates
The first articles selected were published in 2010, which is consistent with the appearance of WES technology in the scientific literature. 3 articles (2 %) were published in 2010, 13 (9 %) in 2011, 31 (21 %) in 2012, 42 (29 %) in 2013, and 46 (31 %) in 2014 and 12 (8 %) in the first trimester of 2015, when we performed the search.
Whole-exome sequencing/Next-generation sequencing/High-throughput sequencing
Among the selected articles, only 48 (34 %) focused exclusively on WES. The other 94 articles either discussed challenges linked to other technologies such as WGS or large gene panels, or discussed challenges linked to Next-Generation Sequencing or High Throughput Sequencing (including WES and other technologies) in general.
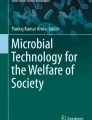
Article types
A graph representing all article types is available in Fig. 1. Of the selected 147 articles, the vast majority (106, 72 %) are review articles in which the authors do not report directly on the way they personally use WES, but rather review the current body of evidence about a certain aspect of the technology. The majority of review articles (66, 62 % of reviews) describe the impact of WES on a specific disease or disease group, and 5 (5 % of reviews) generally discuss its use in the diagnosis of various diseases, whereas 25 (23 % of reviews) review the technology in general, including both its research and clinical applications. 6 articles (6 % of reviews) describe how the technology may impact a specific medical field, such as nursing [28] or pathology [29] while 4 (4 % of reviews) focus on pharmacogenomic applications. 12 articles (8,2 %) report directly on applications of the technology for a specific patient [30, 31], a family [32], a selected group of patients [33–35], or on a larger scale for a particular healthcare service [36–41]. 8 articles (5.4 %) discuss the efficiency of WES compared to other techniques, such as gene panels or WGS. 6 articles (4 %) report on the use of a technology other than WES, and explain this choice by identifying challenges with WES. Finally, 8 articles (5,4 %) focus on challenges linked with WES data processing, analysis and interpretation.

Selected articles types. Review: the authors do not report directly on the way they personally use WES, but rather review the current body of evidence about a certain aspect of the technology. Application: authors report on the application of WES on a specific patient, family, or a larger group of patients in a healthcare service. Data analysis: authors focus on challenges linked with WES data processing, analysis and interpretation. Efficiency: authors compare the efficiency of WES compared to other techniques, such as gene or gene panels sequencing. Report: authors report on the use of a technology other than WES, and explain this choice by identifying challenges with WES
Disease focus
Our first observation was that the articles selected cover an extremely wide range of diseases, from cancer (26, 29 %) to rare diseases (24, 16.3 %) to common disorders such as intellectual disability and developmental delay (6, 4 %). 14 (9.5 %) articles focus on a diversity of heart diseases, 13 (14 %) on neurological diseases, and 3 (2 %) respectively on blood, muscle, and kidney disorders. It is a particularly challenging task to group the diseases addressed by our selection of articles in relevant categories for three main reasons. Firstly, those categories may partly overlap: for instance, cancer in children is considered to be a rare disease. Secondly, a number of articles (9, 6 %) focus generally on genetic or inherited disorders, which may or may not be rare diseases. Thirdly, some articles cover many possible diseases – such as cancer [42, 43] or rare diseases [44, 45] in general - while others focus specifically on one disease [46–48]. A significant number of articles (42, 29 %) did not focus on any diseases in particular, but addressed the impact of WES on all clinical contexts.
Country
We noted the country of the institution of corresponding authors of all selected articles. A total of 19 countries were represented. The majority of articles (92, 62 %) we selected were written in the USA. 25 (17 %) were written in Continental Europe (excluding the UK, which represented an additional 13 articles). The complete distribution of articles per country is represented in Fig. 2.

Number of articles per country of institution of corresponding author
Number of challenges covered
On average, the 147 selected articles covered 8 of the identified challenges. The majority of articles (90, 61.2 %) covered from 1 to 5 challenges. 47 articles (32 %) covered between 6 and 10 challenges, and only 10 articles (6.8 %) covered more than 10 challenges. This steadily decreasing distribution shows the importance of the systematic review methodology in identifying all challenges linked to the clinical implementation of WES as identified by technology users. This distribution is displayed in Fig. 3.

Number of challenges covered across articles
Unsolved challenges identified
From the original 147 studies, we identified 23 unsolved challenges. These were divided into 4 categories, following the ‘samples and data trajectory’, of production, analysis, reporting and sharing.
Table 3 briefly describes the challenges found in all articles. Figure 4 displays the total number of articles covering each challenge. The unsolved challenges reported by technology users are extremely diverse, ranging from very specific challenges, such as the inclusion of WES results in patients electronic health records, to much broader ones, such as the challenges of communicating results with patients and their families and managing their expectations. Three challenges (henceforth referred to as major challenges) were reported by more than 70 (47,6 %) articles:
-
the interpretation of variants and variants of unknown significance (VUS) was reported by 92 (62.6 %) articles
-
challenges linked to incidental findings were reported by 79 (53.7 %) articles
-
the cost of WES and reimbursement of the test by the healthcare system was reported by 72 (49 %) articles.

List of unsolved challenges and proportion of articles reporting on them. We highlighted the challenges found in more than 40 % articles (58 total) in red, and challenges found in 30 to 40 % articles (44 to 58) in green
The following sections provide an overview of the terms in which these three challenges are described in the selected articles.
Data analysis challenge: variants of unknown/uncertain significance (VUS)
The most important challenge mentioned by the selected articles was that of the lack of standards and the complexity of variants interpretation, along with the high risk of finding VUS, which Sutton et al., 2012 consider a ‘plague’ to the field of clinical WES [49]. Unlike targeted single gene or gene panel sequencing assays, WES usually generates a long list of mutations, a large number of which have no known significance. VUS are reported to represent the majority of variants identified by next-generation sequencing (NGS) technologies such as WES [38, 50], although much fewer VUS are found in WES than in WGS [51]. It is unsurprising that VUS is the most consistently reported challenge, as it lies at the heart of a network of connected challenges. The assessment of VUS' pathogenicity is a long, complex and expensive research process [52], which requires the collaborative intervention of different highly trained specialists [53] including bioinformaticians, biologists and clinicians [54]. This need for interdisciplinary collaboration, along with the way WES testing may challenge existing professional roles in the clinic, was reported as a challenge by 50 (34 %) articles. To interpret variants, these specialists rely on bioinformatics analysis pipelines made of imperfect algorithms [36, 37, 42, 55], referring to imperfect databases [44, 50, 56, 57]. The need to develop more efficient and standardised bioinformatics tools to filter, analyze and interpret WES variants was reported as a challenge by 44 (29.29 %) articles. The need to share NGS results and to develop more complete, less biased databases containing fewer false positive and false negative variant-phenotype associations was identified as a challenge in 40 (27.2 %) articles. As described by Jongbloed et al., [58], the “only reasonable way to deal with [the ascertainment of VUS] is to pursue maximum data dissemination in the scientific community”, who could accelerate the analysis of VUS by creating and sharing access to large scale databases gathering sequencing results from as many studies as possible. Certainly, the more sequencing results are shared, the less likely it is that variants identified in patients will never have been reported before. This vision is also shared by Xue et al. [50], who assert that “With more individuals from different ethnic groups sequenced through NGS, more rare variants will inevitably be revealed”, and by Lin et al. [59]: “Sifting through the millions of variants in an individual’s genome for the pathogenic mutation seems to be the most urgent task at hand. The creation of dedicated databases specifically for the purpose of clinical interpretation based on NGS results from a large number of normal controls and diagnosed patients will significantly help this endeavor”. Considering the current uncertainty involved in interpreting VUS, they can represent a heavy burden [60] if reported to a patient’s genetic counsellor or physician. Having access to this information may force clinicians to make a ‘judgment call’ [61] in trying to interpret VUS, and potentially report them to patients, which risks causing them unnecessary anxiety [62]. This dilemma is particularly prevalent in screening for mutations contributing to the genetic background of rare diseases. Indeed, some genes are only found to be mutated in 1 or 2 families in the world. It is therefore very difficult to estimate their pathogenicity and their exact impact on patients, which also makes genetic counselling significantly more challenging [63]. According to Rabbani et al. [64], this should be carefully addressed in the consent form, and discussed during the consent process. In Need et al. [35], the decision was taken at the onset of the study to not report any variants of ‘uncertain significance’ to the patients, regardless of whether or not they were later proven to have significance. In comparison, Ream et al. [65] performed a pilot study in which the need to explain VUS to the families of 6 pediatric drug-resistant epilepsy patients represented a significant challenge, which led them to conclude that “WES may raise more questions than it answers for some patients”.
Incidental findings (IF)
The challenge of IF was also consistently mentioned in 92 (53.7 %) of selected articles. IF can be defined as information of clinical relevance which is found during the WES data analysis and which is beyond the scope of the original clinical condition for which the patient was ‘prescribed’ a WES test. According to Sankaran et al. [57], the “identification of actionable, IF during genome-wide DNA sequencing genetic studies is a major concern of many patients, as well as health care providers”, and this can “cause ethical and clinical dilemmas” [66]. The topic of genomic IF is heavily discussed in the literature, and two recently published reviews [67, 68] provide strong evidence showing that there is a lack of consensus on how to define, analyze, and report such variants to patients and research participants. Within our selection of articles, for instance, Lyon et al. [69] consider the term “IF” to be “misleading”. They prefer using the term “secondary findings”, which they argue better represents their importance and could help correct the view that such findings do not require significant time and effort to be analyzed, interpreted, and reported. In 2013, Sankaran et al. [57] stated that there was no consensus on just how frequently they are actually found in NGS data. However, several authors provide different estimates: in 2014, Xue et al. [50] provided references to support the claim that “the rate of reportable IFs can range from 1 to 8.8 %”, while Gecz et al. [70] argued that they range from 1 to 2 % of patients. Regardless of how often IF are found in practice, they have to be addressed in the patient pre-test counselling process [51, 71], and this ‘intensive genetic counseling’ [28] can be a “main issue” in practice [40, 72]. Incidental findings are viewed as a potential “additional burden” [65] and source of anxiety for patients and their families [62, 73, 74].
19 out of the 55 articles published since 2013 which mention IF as a challenge (34.5 %) refer to the American College of Medical Genetics and Genomics (ACMG) recommendation on reporting IF [16, 21]. This recommendation, which provides a list of 56 genes to be systematically searched for ‘actionable variants’, has clearly raised “concerns” [53] and debate on this topic rather than helping to resolve it. Even after mentioning these recommendations, articles published in 2014 refer to the reporting of IF by clinicians as “currently a subject of intense debate” [52], “one of the current, contentious debates” [73], or state that “there remains strong debate” [56] and an “ongoing discussion on how to best proceed with incidental findings” [75]. Malhotra et al. [42] specifically mention that “the methods of providing [incidental findings] to patients are not entirely clear, although some recommendations have recently been made by the American College of Medical Genetics and Genomics”. Even in 2015, this is still considered to be a “current debate” by Goldberg et al. [76], and Bender state that the discussion of this topic “will undoubtedly continue” [77]. This uncertainty on how to define and report IF is described as the justification for using targeted testing over WES and more generally NGS in certain clinical contexts, such as hematology [46] or for heart diseases [78]. The challenge of IF even leads Lohman et al. [75] to refer to WES and WGS as a”curse” as well as a”blessing”.
From 2011 to 2015, we noted a steady increase in the proportion of selected articles discussing the challenge of IF. Indeed, it rose from 46.2 % of articles published in 2011, to 75 % in 2015. This trend is opposed to that of the proportion of articles discussing VUS, as displayed in Fig. 5. Since the total number of selected articles published per year is variable and relatively small, it is difficult to attest the significance of this trend. However, we can make the following hypothesis: as software tools and reference databases have improved, the interpretation of WES variants has become less and less challenging for technology users. On the other hand, the publication of recommendations and guidelines in the USA [16], Canada [23] and Europe [22] has polarized the debate on the challenge of identification, classification and reporting of IF, which may help explain why it was increasingly mentioned in our selection of articles.

Proportion of articles addressing VUS and IF per year. In parenthesis next to the year of publication of articles, we indicated the total number of selected articles published that year
Cost and reimbursement
The challenge of WES’ cost and of test reimbursement is reported in 49 % of articles (72). It includes a number of sub-challenges along the WES data trajectory from production to analysis and interpretation. Although they do not provide much detail, a number of articles published in 2014 and 2015 consider that WES is still too expensive to be implemented as a standard of care in different contexts such as epilepsy [54], acute myeloid leukemia [52], axonopathies [79], sudden unexplained death [80] and cardiac arrhythmia [78]. Since sequencing costs have fallen drastically over time, it is notable that even in 2014 some authors consider that it is the sequencing itself that is too expensive [37, 81–83]. Other justifications for the high price of these tests mentioned by authors include the cost of data storage [84] and necessary Sanger validation of WES results [50]. Data interpretation in general is another reason provided to explain the higher costs of WES compared to more targeted sequencing [50, 85, 86]. Focusing on the possibility of using WES in newborn screening, Beckmann et al. [87], provide a more detailed assessment of costs which leads them to conclude that “From a cost perspective, generalization of this practice with current procedures would entail a monumental effort that is likely to ruin our social healthcare programs.” Those “important social, economic, and human costs” are linked to the increased time clinicians would have to spend interpreting and reporting WES results to patients and families.
The large-scale application of WES in the clinic will only be possible if it is integrated fully into the healthcare system as a standard of care for certain conditions. This requires a thorough economic evaluation of possible funding sources and strategies to reimburse this sort of analysis. According to many articles from the USA, UK and Germany published after 2014, cost assessment analysis and economic evaluation studies still have to be performed in order to formally establish the relative cost efficiency of WES compared to other techniques [34, 38, 65, 73, 75, 88, 89]. The need for private insurance providers to reimburse these tests is reported as one of the key elements standing in the way of clinical implementation of WES on a larger scale, especially in the USA [39, 51, 89–91]. Not only will the clinical utility [62] and cost efficiency of these tests have to be proven, but insurance companies and the public healthcare system will have to organise the administrative infrastructure needed to reimburse those tests, such as by creating ‘new billing codes’ [39, 92].
Discussion
Our methodology carried a number of limitations. The first challenge of our approach is that we tried to identify elements in publications which had a different primary focus. Indeed, we were looking to identify sections describing unsolved implementation challenges in publications focusing on the description of the actual use of WES in a clinical context. This made the task of identifying those sections more difficult, and may have resulted in failure to identify a number of articles. Indeed, the relevant sections of the selected articles were extremely diverse, ranging from a few words to full titled sections. Another issue which could possibly have led us to miss relevant publications was our choice of search terms. Our keyword combination of (“Clinical application” OR “Medical application” OR “Healthcare” OR “Clinical care” OR “Medical care” OR “Clinical practice” OR “Clinical diagnostic” OR “Medical practice”) may have lacked specificity, leading us to overlook relevant articles because of the very high number of hits we obtained. In addition, the process of filtering all 2095 articles was very lengthy. Since the date at which we performed the search, a number of potentially relevant articles have been published. In addition, the regulatory landscape of clinical WES has evolved, with the publication of a number of guidelines and recommendations which will significantly impact this field, notably in Europe [93], and the USA [94–97]. The speed, efficiency and reproducibility of the data filtering process could be significantly enhanced if this process was partly automated. However, to our knowledge there is no open access software tool that could have performed the search based on keywords and context generation more efficiently than we did. One other limitation lies in the combination of quantitative and qualitative approaches we used to analyze all 23 challenges identified in 147 selected articles. This was a relatively small sample size in which to obtain significant differences between sub-groups of articles. On the other hand, it was a high number of articles to analyze thoroughly, which is why we decided to analyze only the challenges that were most reported by authors. We believe this combination of qualitative and quantitative methodologies is key to making informed policy decisions based on the latest body of evidence regarding technologies such as WES.
Conclusions
A number of challenges need to be resolved before whole exome sequencing can be implemented as a standard of care in the clinical setting. Through this systematic review of the literature, we could identify as many as 23 of these challenges. The three challenges that were most consistently reported by technology users were that of incidental findings, variants of unknown significance, and the cost of the technology. Although a small number of challenges, notably communication with patients, education of clinicians, and patients’ turnaround time, were reported differently in articles focusing on cancer, rare diseases or all diseases, and in articles from different countries, most challenges were discussed similarly across diseases and countries (data not shown). WES is already used in the clinical setting, and may soon be considered the standard of care for specific medical conditions, most notably for the identification of mutations contributing to rare genetic diseases. Clinics in the USA [41], France [98] and the Netherlands [99] already report promising results from the systematic use of NGS in hundreds of patients. Yet, technology users are calling for certain standards and guidelines to be published before this technology replaces more focused approaches such as gene panels sequencing. In addition, it is clear that a number of infrastructural adjustments will have to be made for clinics to store, process and analyze the amounts of data produced by WES. The interpretation of this data requires specially trained staff, and patients and families must also be adequately prepared to deal with WES test results. Some intermediary solutions may be found, such as the one suggested by Topper et al.: “In the near term, we suggest that many of these technical and ethical challenges may be alleviated by a targeted analysis approach, in which the full exome sequence is generated in patients, but analysis is initially limited to those genes already known to play a role in the presenting disorder” [60].
Abbreviations
ACMG, The American College of Medical Genetics and Genomics; IF, incidental findings; NGS, next-generation sequencing; VUS, variants of unknown significance; WES, whole-exome sequencing; WGS, whole-genome sequencing
References
Kaname T, Yanagi K, Naritomi K. A commentary on the promise of whole-exome sequencing in medical genetics. J Hum Genet. 2014;59:117–8.
Majewski J, Schwartzentruber J, Lalonde E, Montpetit A, Jabado N. What can exome sequencing do for you? J Med Genet. 2011;48:580–9.
Lyon GJ, O’Rawe J. Human genetics and clinical aspects of neurodevelopmental disorders. In: Mitchell K, editor. The Genetics of Neurodevelopmental Disorders. 1st edition. Hoboken: John Wiley & Sons, Inc.; 2015:289–317.
Hart SN, Sarangi V, Moore R, Baheti S, Bhavsar JD, Couch FJ, Kocher J-PA. SoftSearch: integration of multiple sequence features to identify breakpoints of structural variations. PLoS One. 2013;8:e83356.
Lonigro RJ, Grasso CS, Robinson DR, Jing X, Wu Y-M, Cao X, Quist MJ, Tomlins SA, Pienta KJ, Chinnaiyan AM. Detection of somatic copy number alterations in cancer using targeted exome capture sequencing. Neoplasia. 2011;13:1019–IN21.
Liang D, Peng Y, Lv W, Deng L, Zhang Y, Li H, Yang P, Zhang J, Song Z, Xu G, Cram DS, Wu L. Copy number variation sequencing for comprehensive diagnosis of chromosome disease syndromes. J Mol Diagn. 2014;16:519–26.
Samarakoon PS, Sorte HS, Kristiansen BE, Skodje T, Sheng Y, Tjønnfjord GE, Stadheim B, Stray-Pedersen A, Rødningen OK, Lyle R. Identification of copy number variants from exome sequence data. BMC Genomics. 2014;15:661.
Sastre L. Exome sequencing: what clinicians need to know. Adv Genomics Genet. 2014;4:15–27.
Jayadev S, Smith CO, Bird TD. Neurogenetics: five new things. Neurol Clin Pract. 2011;1:41–8.
Jackson DB, Sood AK. Personalized cancer medicine--advances and socio-economic challenges. Nat Rev Clin Oncol. 2011;8:735–41.
Jamal SM, Yu J-H, Chong JX, Dent KM, Conta JH, Tabor HK, Bamshad MJ. Practices and policies of clinical exome sequencing providers: analysis and implications. Am J Med Genet A. 2013;161A:935–50.
Pokorska-Bocci A, Kroese M, Sagoo GS, Hall A, Burton H. Personalised medicine in the UK: challenges of implementation and impact on healthcare system. Genome Med. 2014;6:28.
DeVita VT, Eggermont AMM, Hellman S, Kerr DJ. Clinical cancer research: the past, present and the future. Nat Rev Clin Oncol. 2014;11:663–9.
Johansen Taber KA, Dickinson BD, Wilson M. The promise and challenges of next-generation genome sequencing for clinical care. JAMA Intern Med. 2014;174:275–80.
McGuire AL, Knoppers BM, Zawati MH, Clayton EW. Can I be sued for that? Liability risk and the disclosure of clinically significant genetic research findings. Genome Res. 2014;24:719–23.
Green RC, Berg JS, Grody WW, Kalia SS, Korf BR, Martin CL, McGuire AL, Nussbaum RL, O’Daniel JM, Ormond KE, Rehm HL, Watson MS, Williams MS, Biesecker LG. ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet Med. 2013;15:565–74.
Allyse M, Michie M. Not-so-incidental findings: the ACMG recommendations on the reporting of incidental findings in clinical whole genome and whole exome sequencing. Trends Biotechnol. 2013;31:439–41.
Townsend A, Adam S, Birch PH, Friedman JM. Paternalism and the ACMG recommendations on genomic incidental findings: patients seen but not heard. Genet Med. 2013;15:751–2.
McCormick JB, Sharp RR, Farrugia G, Lindor NM, Babovic-Vuksanovic D, Borad MJ, Bryce AH, Caselli RJ, Ferber MJ, Johnson KJ, Lazaridis KN, McWilliams RR, Murray JA, Parker AS, Schahl KA, Wieben ED. Genomic medicine and incidental findings: balancing actionability and patient autonomy. Mayo Clin Proc. 2014;89:718–21.
Vayena E, Tasioulas J. Genetic incidental findings: autonomy regained? Genet Med. 2013;15:868–70.
ACMG Board of directors. ACMG policy statement: updated recommendations regarding analysis and reporting of secondary findings in clinical genome-scale sequencing. Genet Med. 2014;17:68–69.
Hehir-Kwa JY, Claustres M, Hastings RJ, van Ravenswaaij-Arts C, Christenhusz G, Genuardi M, Melegh B, Cambon-Thomsen A, Patsalis P, Vermeesch J, Cornel MC, Searle B, Palotie A, Capoluongo E, Peterlin B, Estivill X, Robinson PN. Towards a European consensus for reporting incidental findings during clinical NGS testing. Eur J Hum Genet. 2015;23:1601.
Boycott K, Hartley T, Adam S, Bernier F, Chong K, Fernandez BA, Friedman JM, Geraghty MT, Hume S, Knoppers BM, Laberge A-M, Majewski J, Mendoza-Londono R, Meyn MS, Michaud JL, Nelson TN, Richer J, Sadikovic B, Skidmore DL, Stockley T, Taylor S, van Karnebeek C, Zawati MH, Lauzon J, Armour CM. The clinical application of genome-wide sequencing for monogenic diseases in Canada: Position Statement of the Canadian College of Medical Geneticists. J Med Genet. 2015;52:431–7.
Knobloch K, Yoon U, Vogt PM. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication bias. J Craniomaxillofac Surg. 2011;39:91–2.
Petticrew M, Roberts H. Systematic reviews in the social sciences: a practical guide. Oxford: Blackwell Publishing; 2006.
Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107–15.
Downe-Wamboldt B. Content analysis: method, applications, and issues. Health Care Women Int. 1992;13:313–21.
Vorderstrasse AA, Hammer MJ, Dungan JR. Nursing implications of personalized and precision medicine. Semin Oncol Nurs. 2014;30:130–6.
Williams ES, Hegde M. Implementing genomic medicine in pathology. Adv Anat Pathol. 2013;20:238–44.
Merrill SL, Vaidya A, Pyeritz RE. Ethical challenges of the use of whole exome sequencing in the clinic. World J Pediatr Congenit Heart Surg. 2013;4:58–61.
Mayer AN, Dimmock DP, Arca MJ, Bick DP, Verbsky JW, Worthey EA, Jacob HJ, Margolis DA. A timely arrival for genomic medicine. Genet Med. 2011;13:195–6.
Girolami F, Iascone M, Tomberli B, Bardi S, Benelli M, Marseglia G, Pescucci C, Pezzoli L, Sana ME, Basso C, Marziliano N, Merlini PA, Fornaro A, Cecchi F, Torricelli F, Olivotto I. Novel α-actinin 2 variant associated with familial hypertrophic cardiomyopathy and juvenile atrial arrhythmias: a massively parallel sequencing study. Circ Cardiovasc Genet. 2014;7:741–50.
Takeichi T, Liu L, Fong K, Ozoemena L, McMillan JR, Salam A, Campbell P, Akiyama M, Mellerio JE, McLean WHI, Simpson MA, McGrath JA. Whole-exome sequencing improves mutation detection in a diagnostic epidermolysis bullosa laboratory. Br J Dermatol. 2015;172:94–100.
Carss KJ, Hillman SC, Parthiban V, McMullan DJ, Maher ER, Kilby MD, Hurles ME. Exome sequencing improves genetic diagnosis of structural fetal abnormalities revealed by ultrasound. Hum Mol Genet. 2014;23:3269–77.
Need AC, Shashi V, Hitomi Y, Schoch K, Shianna KV, McDonald MT, Meisler MH, Goldstein DB. Clinical application of exome sequencing in undiagnosed genetic conditions. J Med Genet. 2012;49:353–61.
Coonrod EM, Durtschi JD, Margraf RL, Voelkerding KV. Developing genome and exome sequencing for candidate gene identification in inherited disorders: An integrated technical and bioinformatics approach. Arch Pathol Lab Med. 2013;137:415–33.
Lacroix L, Boichard A, André F, Soria J-C. Genomes in the clinic: the Gustave Roussy Cancer Center experience. Curr Opin Genet Dev. 2014;24:99–106.
Levenson D. Whole-exome sequencing emerges as clinical diagnostic tool: Testing method proves useful for diagnosing wide range of genetic disorders. Am J Med Genet Part A. 2014;164:ix–x.
Lazaridis KN, McAllister TM, Babovic-Vuksanovic D, Beck SA, Borad MJ, Bryce AH, Chanan-Khan AA, Ferber MJ, Fonseca R, Johnson KJ, Klee EW, Lindor NM, McCormick JB, McWilliams RR, Parker AS, Riegert-Johnson DL, Rohrer Vitek CR, Schahl KA, Schultz C, Stewart K, Then GC, Wieben ED, Farrugia G. Implementing individualized medicine into the medical practice. Am J Med Genet C: Semin Med Genet. 2014;166C:15–23.
van Zelst-Stams WA, Scheffer H, Veltman JA. Clinical exome sequencing in daily practice: 1,000 patients and beyond. Genome Med. 2014;6:2.
Jacob HJ, Abrams K, Bick DP, Brodie K, Dimmock DP, Farrell M, Geurts J, Harris J, Helbling D, Joers BJ, Kliegman R, Kowalski G, Lazar J, Margolis DA, North P, Northup J, Roquemore-Goins A, Scharer G, Shimoyama M, Strong K, Taylor B, Tsaih S-W, Tschannen MR, Veith RL, Wendt-Andrae J, Wilk B, Worthey EA. Genomics in clinical practice: lessons from the front lines. Sci Transl Med. 2013;5:194cm5.
Malhotra A, Levine S, Allingham-Hawkins D. Whole exome sequencing for cancer – is there evidence of clinical utility? Adv Genomics Genet. 2014;4:115.
Chang F, Li MM. Clinical application of amplicon-based next-generation sequencing in cancer. Cancer Genet. 2013;206:413–9.
Boycott KM, Vanstone MR, Bulman DE, MacKenzie AE. Rare-disease genetics in the era of next-generation sequencing: discovery to translation. Nat Rev Genet. 2013;14:681–91.
Lee H, Nelson SF. Rethinking clinical practice: clinical implementation of exome sequencing. Per Med. 2012;9:785–7.
Bacher U, Kohlmann A, Haferlach T. Mutational profiling in patients with MDS: ready for every-day use in the clinic? Best Pract Res Clin Haematol. 2015;28:32–42.
Arts HH, Knoers NVAM. Current insights into renal ciliopathies: what can genetics teach us? Pediatr Nephrol. 2013;28:863–74.
Berg JS, Evans JP, Leigh MW, Omran H, Bizon C, Mane K, Knowles MR, Weck KE, Zariwala MA. Next generation massively parallel sequencing of targeted exomes to identify genetic mutations in primary ciliary dyskinesia: implications for application to clinical testing. Genet Med. 2011;13:218–29.
Sutton ALM, Robin NH. Clinical application of whole exome sequencing: not (yet) ready for primetime. Curr Opin Pediatr. 2012;24:663–4.
Xue Y, Ankala A, Wilcox WR, Hegde MR. Solving the molecular diagnostic testing conundrum for Mendelian disorders in the era of next-generation sequencing: single-gene, gene panel, or exome/genome sequencing. Genet Med. 2015;17(6):444–51.
Klein H-G, Hambuch P, Bauer P, Hambuch T. Whole genome sequencing (WGS), whole exome sequencing (WES) and clinical exome sequencing (CES) in patient care. J Lab Med. 2014;38:221–30.
Graubert T, Stone R. AML genomics for the clinician. Semin Hematol. 2014;51:322–9.
Newman WG, Black GC. Delivery of a clinical genomics service. Genes (Basel). 2014;5:1001–17.
Sisodiya SM. Genetic screening and diagnosis in epilepsy? Curr Opin Neurol. 2015;28:136–42.
Marian AJ. Sequencing your genome: what does it mean? Methodist Debakey Cardiovasc J. 2014;10:3–6.
Gillespie RL, Hall G, Black GC. Genetic testing for inherited ocular disease: delivering on the promise at last? Clin Experiment Ophthalmol. 2014;42:65–77.
Sankaran VG, Gallagher PG. Applications of high-throughput DNA sequencing to benign hematology. Blood. 2013;122:3575–82.
Jongbloed JD, Pósafalvi A, Kerstjens-Frederikse WS, Sinke RJ, van Tintelen JP. New clinical molecular diagnostic methods for congenital and inherited heart disease. Expert Opin Med Diagn. 2011;5:9–24.
Lin X, Tang W, Ahmad S, Lu J, Colby CC, Zhu J, Yu Q. Applications of targeted gene capture and next-generation sequencing technologies in studies of human deafness and other genetic disabilities. Hear Res. 2012;288:67–76.
Topper S, Ober C, Das S. Exome sequencing and the genetics of intellectual disability. Clin Genet. 2011;80:117–26.
Desai AN, Jere A. Next-generation sequencing: ready for the clinics? Clin Genet. 2012;81:503–10.
Thomas F, Desmedt C, Aftimos P, Awada A. Impact of tumor sequencing on the use of anticancer drugs. Curr Opin Oncol. 2014;26:347–56.
Rossor AM, Polke JM, Houlden H, Reilly MM. Clinical implications of genetic advances in Charcot-Marie-Tooth disease. Nat Rev Neurol. 2013;9:562–71.
Rabbani B, Tekin M, Mahdieh N. The promise of whole-exome sequencing in medical genetics. J Hum Genet. 2014;59:5–15.
Ream MA, Mikati MA. Clinical utility of genetic testing in pediatric drug-resistant epilepsy: a pilot study. Epilepsy Behav. 2014;37:241–8.
Nigro V, Piluso G. Next generation sequencing (NGS) strategies for the genetic testing of myopathies. Acta Myol. 2012;31:196–200.
Shkedi-Rafid S, Dheensa S, Crawford G, Fenwick A, Lucassen A. Defining and managing incidental findings in genetic and genomic practice. J Med Genet. 2014;51:715–23.
Knoppers BM, Zawati MH, Sénécal K. Return of genetic testing results in the era of whole-genome sequencing. Nat Rev Genet. 2015;16:553–9.
Lyon GJ, Wang K. Identifying disease mutations in genomic medicine settings: current challenges and how to accelerate progress. Genome Med. 2012;4:58.
Gecz J, Corbett M. Developmental disorders: deciphering exomes on a grand scale. Lancet (London, England). 2015;385:1266–7.
Zanolli MT, Khetan V, Dotan G, Pizzi L, Levin AV. Should patients with ocular genetic disorders have genetic testing? Curr Opin Ophthalmol. 2014;25:359–65.
Gallego CJ, Bennette CS, Heagerty P, Comstock B, Horike-Pyne M, Hisama F, Amendola LM, Bennett RL, Dorschner MO, Tarczy-Hornoch P, Grady WM, Fullerton SM, Trinidad SB, Regier DA, Nickerson DA, Burke W, Patrick DL, Jarvik GP, Veenstra DL. Comparative effectiveness of next generation genomic sequencing for disease diagnosis: design of a randomized controlled trial in patients with colorectal cancer/polyposis syndromes. Contemp Clin Trials. 2014;39:1–8.
Jiang Y-H, Wang Y, Xiu X, Choy KW, Pursley AN, Cheung SW. Genetic diagnosis of autism spectrum disorders: the opportunity and challenge in the genomics era. Crit Rev Clin Lab Sci. 2014;51:249–62.
Gibson J, Young S, Leng B, Zreik R, Rao A. Molecular diagnostic testing of cytology specimens: current applications and future considerations. J Am Soc Cytopathol. 2014;3:280–94.
Lohmann K, Klein C. Next generation sequencing and the future of genetic diagnosis. Neurotherapeutics. 2014;11:699–707.
Goldberg A, Curtis CL, Kleim JA. Linking genes to neurological clinical practice: the genomic basis for neurorehabilitation. J Neurol Phys Ther. 2015;39:52–61.
Glade Bender J, Verma A, Schiffman JD. Translating genomic discoveries to the clinic in pediatric oncology. Curr Opin Pediatr. 2015;27:34–43.
Lubitz SA, Ellinor PT. Next-generation sequencing for the diagnosis of cardiac arrhythmia syndromes. Heart Rhythm. 2015;12:1062–70.
Fridman V, Murphy SM. The spectrum of axonopathies: from CMT2 to HSP. Neurology. 2014;83:580–1.
Tang Y, Stahl-Herz J, Sampson BA. Molecular diagnostics of cardiovascular diseases in sudden unexplained death. Cardiovasc Pathol. 2014;23:1–4.
Iacobazzi V, Infantino V, Castegna A, Andria G. Hyperhomocysteinemia: related genetic diseases and congenital defects, abnormal DNA methylation and newborn screening issues. Mol Genet Metab. 2014;113:27–33.
Liu Z-J, Li H-F, Tan G-H, Tao Q-Q, Ni W, Cheng X-W, Xiong Z-Q, Wu Z-Y. Identify mutation in amyotrophic lateral sclerosis cases using HaloPlex target enrichment system. Neurobiol Aging. 2014;35:2881. e11–5.
Sanchez M, Levine RL, Rampal R. Integrating genomics into prognostic models for AML. Semin Hematol. 2014;51:298–305.
Smith A, Boycott KM, Jarinova O. Clinical translation of next-generation sequencing requires optimization of workflows and interpretation of variants. Hum Mutat. 2013;2014(35):265–9.
Dacic SMDP, Nikiforova MNMD. Present and future molecular testing of lung carcinoma. Adv Anat Pathol. 2014;21:94–9.
Babkina N, Graham JM. New genetic testing in prenatal diagnosis. Semin Fetal Neonatal Med. 2014;19:214–9.
Beckmann JS. Can we afford to sequence every newborn baby’s genome? Hum Mutat. 2015;36:283–6.
Williams JK, Cashion AK, Veenstra DL. Challenges in evaluating next-generation sequence data for clinical decisions. Nurs Outlook. 2015;63:48–50.
Berg JS. Genome-scale sequencing in clinical care: establishing molecular diagnoses and measuring value. JAMA. 2014;312:1865–7.
Shashi V, McConkie-Rosell A, Schoch K, Kasturi V, Rehder C, Jiang YH, Goldstein DB, McDonald MT. Practical considerations in the clinical application of whole-exome sequencing. Clin Genet. 2016;89(2):173–81.
Atwal PS, Brennan M-L, Cox R, Niaki M, Platt J, Homeyer M, Kwan A, Parkin S, Schelley S, Slattery L, Wilnai Y, Bernstein JA, Enns GM, Hudgins L. Clinical whole-exome sequencing: are we there yet? Genet Med. 2014;16:717–9.
Kamalakaran S, Varadan V, Janevski A, Banerjee N, Tuck D, McCombie WR, Dimitrova N, Harris LN. Translating next generation sequencing to practice: opportunities and necessary steps. Mol Oncol. 2013;7:743–55.
Matthijs G, Souche E, Alders M, Corveleyn A, Eck S, Feenstra I, Race V, Sistermans E, Sturm M, Weiss M, Yntema H, Bakker E, Scheffer H, Bauer P. Guidelines for diagnostic next-generation sequencing. Eur J Hum Genet. 2016;24:2–5.
Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, Grody WW, Hegde M, Lyon E, Spector E, Voelkerding K, Rehm HL, Committee; on behalf of the ACMG Laboratory Quality Assurance. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17:405–23.
Sabatini LM, Mathews C, Ptak D, Doshi S, Tynan K, Hegde MR, Burke TL, Bossler AD. Genomic sequencing procedure microcosting analysis and health economic cost-impact analysis: a report of the association for molecular pathology. J Mol Diagnostics. 2016;18:319–28.
Amendola LM, Jarvik GP, Leo M, McLaughlin HM, Akkari H, Amaral M, Berg JS, Biswas S, Bowling K, Conlin L, Cooper G, Dorschner MO, Dulik M, Ghazani A, Ghosh R, Green RC, Hart R, Horton C, Johnston JJ, Lebo MS, Milosavljevic A, Ou J, Pak C, Patel R, Pung S, Richards C, Salama J, Strande N, Yang Y, Plon SE, et al. Performance of ACMG/AMP variant interpretation guidelines among nine laboratories in the Clinical Sequencing Exploratory Research (CSER) consortium. Am J Hum Genet. 2016;to appear:1–10.
ACMG Board of Directors. Clinical utility of genetic and genomic services: a position statement of the American College of Medical Genetics and Genomics. Genet Med. 2015;17:505–7.
Thevenon J, Duffourd Y, Masurel-Paulet A, Lefebvre M, Feillet F, El Chehadeh-Djebbar S, St-Onge J, Steinmetz A, Huet F, Chouchane M, Darmency-Stamboul V, Callier P, Thauvin-Robinet C, Faivre L, Rivière JB. Diagnostic odyssey in severe neurodevelopmental disorders: Towards clinical whole-exome sequencing as a first-line diagnostic test. Clin Genet. 2016;89(6):700–7.
Vrijenhoek T, Kraaijeveld K, Elferink M, de Ligt J, Kranendonk E, Santen G, Nijman IJ, Butler D, Claes G, Costessi A, Dorlijn W, van Eyndhoven W, Halley DJJ, van den Hout MCGN, van Hove S, Johansson LF, Jongbloed JDH, Kamps R, Kockx CEM, de Koning B, Kriek M, Lekanne Dit Deprez R, Lunstroo H, Mannens M, Nelen M, Ploem C, Rijnen M, Saris JJ, Sinke R, Sistermans E, et al. Next-generation sequencing-based genome diagnostics across clinical genetics centers: implementation choices and their effects. Eur J Hum Genet. 2015;23(9):1142–50.
Acknowledgements
We thank Anne Cambon-Thomsen, Bartha Maria Knoppers, David Rosenblatt and Ma’n Zawati for their guidance in developing the study design. We also thank Derek So for his help on the manuscript, and, Simon Papillon-Cavanagh and Sébastien Lamy for their help with the statistical analysis of the data.
Authors’ contributions
GB conceived the study, designed the search strategy, performed the search and collected all the data, filtered and coded the articles, performed the analysis and wrote the first version of the manuscript. MH filtered and coded the articles, and commented on the manuscript. YJ provided guidance on the design of the study, methodology and analysis. He commented on the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
PRISMA flow diagram. (DOCX 70 kb)
Additional file 2:
PRISMA checklist. (DOCX 28 kb)
Additional file 3:
Full articles dataset. (XLSX 628 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Bertier, G., Hétu, M. & Joly, Y. Unsolved challenges of clinical whole-exome sequencing: a systematic literature review of end-users’ views. BMC Med Genomics 9, 52 (2016). https://doi.org/10.1186/s12920-016-0213-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12920-016-0213-6