
Abstract
Background
Cross-sectional studies found that frailty was associated with prevalent diabetic microvascular complications (DMC). Longitudinal evidence in this regard is inconclusive and insufficient. We aimed to prospectively evaluate the association of pre-frailty and frailty with DMC in patients with type 2 diabetes (T2D).
Methods
We included 18,062 adults (mean age 59.4 ± 7.2 years, 37.4% female) with T2D at baseline in the UK Biobank. Frailty was defined using the frailty phenotype according to five components (weight loss, exhaustion, low physical activity, slow gait speed, and low grip strength). DMC, defined as diabetic nephropathy, diabetic neuropathy, or diabetic retinopathy, was identified using hospital inpatient records and death registries. Cox proportional hazard regression models considering competing risks were used to evaluate the associations of frailty phenotype with overall DMC events and subtypes.
Results
Among all participants, 6101 (33.8%) were classified as non-frail, 10,073 (55.8%) were classified as pre-frail, and 1888 (10.4%) were classified as frail. During a median follow-up of 12.0 years, 3678 DMC cases were documented, including 2213 diabetic nephropathy, 1520 diabetic retinopathy, and 673 diabetic neuropathy events. In the multivariable-adjusted model, compared with participants with non-frail, both pre-frailty and frailty were significantly associated with increased risk of overall DMC (HR 1.10, 95% CI: [1.02, 1.18] for pre-frailty and HR 1.52 [95% CI: 1.36, 1.69] for frailty). Similar results were observed in the subtypes of DMC. For each one-point increase in frailty phenotype score, the risk of overall DMC, diabetic nephropathy, diabetic retinopathy, and diabetic neuropathy event increased by 13%, 16%, 10%, and 20%, respectively.
Conclusions
Both pre-frailty and frailty were associated with an increased risk of DMC in patients with T2D. These findings have important implications for integrating early assessment and surveillance of frailty in diabetes and may favor the identification of at-risk patients.
Similar content being viewed by others


Background
Diabetes is one of the fastest-growing global health issues of the twenty-first century, with 537 million adults worldwide now living with diabetes in 2021, and this number is projected to reach 783 million in 2045 [1]. Diabetic microvascular complications (DMC) have emerged as major aftermath of the worldwide diabetes pandemic, leading to loss of visual, renal, and neurologic functions, with profound effects on quality of life, demand for health services, and economic costs [2, 3]. DMC prevalence is high in patients with diabetes, affecting half of the patients with type 2 diabetes (T2D) [4]. About 25% of patients with diabetes will develop diabetic nephropathy [5], almost 34.6% will develop diabetic retinopathy [6], and nearly 50% will develop diabetic neuropathy [7]. Given the high incidence and serious consequences, early recognition and a better understanding of the risk factors for DMC are needed.
Frailty, an emerging public health concern worldwide paralleled with population aging, is characterized by a decline in functioning across multiple physiological systems, with a resultant increased susceptibility to stressors [8, 9]. This condition increases the risk of a range of adverse health outcomes, including disability, falls, fracture, lower quality of life, loneliness, cognitive decline, hospital admission, and mortality [9]. Recently, frailty has attracted widespread attention in the field of diabetes. The prevalence of frailty and pre-frailty in community-dwelling older adults with diabetes was 20.1% and 49.1%, respectively, and adults with diabetes were more susceptible to frailty than those without diabetes [10]. Frailty further increases the risk of adverse outcomes, including disability [11, 12], fractures [13], hospitalization [12, 14, 15], major cardiovascular events [14, 16], and mortality [12, 14, 15] in diabetes.
A cross-sectional study of 146 inpatients aged 60 years or older with T2D found that both pre-frailty and frailty were significantly associated with diabetic nephropathy (odds ratio 4.31 and 4.46, respectively) [17]. Another cross-sectional study of 292,170 individuals with diabetes (mean age 64.7 years) found that frailty was associated with prevalent DMC [18]. However, longitudinal evidence in this regard is inconclusive and insufficient. Two prospective studies suggested that the presence of frailty (defined by the Rockwood frailty index and Clinical Frailty Scale) was independently associated with the risk of overall DMC [16, 19]. However, a population-based, retrospective study found that frailty derived from Johns Hopkins-adjusted clinical groups (weighted comorbidity score identified from electronic medical records) was not associated with overall DMC [20]. Frailty phenotype, described by Fried and colleagues who consider frailty as a clinical presentation of weight loss, weakness, exhaustion, slowness, and low physical activity level [21], has been a dominant criterion in the frailty literature. Compared with other criteria, the frailty phenotype provided a potential standardized definition for frailty, and the clear criteria are relatively easy and inexpensive to apply [21], which have been validated as consistent with a medical syndrome linked to distinct biology [9]. However, to our knowledge, no studies have investigated the association of frailty phenotype with the incidence of overall DMC and its subtypes (diabetic nephropathy, diabetic retinopathy, and diabetic neuropathy). Therefore, to fill these knowledge gaps, we explore the relationship between frailty phenotype and incident DMC in patients with T2D.
Methods
Study population
The UK Biobank is a large population-based cohort of more than 500,000 participants aged 40−69 years, recruited in one of 22 assessment centers between 2006 and 2010 in England, Scotland, and Wales [22]. Participants were invited to complete touchscreen questionnaires, have physical measurements, and provide biological samples at the baseline. All participants provided informed consent, and the study was approved by the North West–Haydock Research Ethics Committee (16/NW/0274).
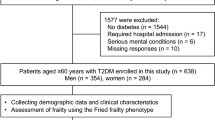
Prevalent T2D at baseline was identified using UK Biobank algorithms by Eastwood et al. through hospital inpatient records, self-reported medical history, and medication, which is a reliable measurement with 96% accuracy [23]. We further considered the biochemical examination for glycated hemoglobin A1c (HbA1c) based on the algorithms. We used the cutoffs of HbA1c for defining diabetes, 48 mmol/mol (6.5%). The definitions for prevalent diabetes are presented in Additional file 1: Table S1. We compared the date of the patients’ first-time diabetes diagnosis and the date of entry to the study. Those who had self-reported or were diagnosed with diabetes before or on the cohort entry were recognized as baseline diabetes. We excluded participants who withdrew their information (n = 99). Those without diabetes at baseline (n = 471,048), who had been diagnosed with type 1 diabetes or diagnosed with diabetes before 30 years old (n = 3434), had DMC at baseline (n = 2983), and those who had no data for frailty phenotype were further excluded (n = 6879). Finally, 18,062 individuals with T2D were included in the present analysis (Additional file 1: Fig. S1).
Assessment of frailty phenotype
The original definition of frailty phenotype was described and applied in the Cardiovascular Health Study by Fried and colleagues [21], and the items have been adapted in the UK Biobank [24, 25]. Weight loss was self-reported as the question “Compared with one year ago, has your weight changed?” (response: yes, lost weight = 1; others = 0). Exhaustion was self-reported according to the question “Over the past 2 weeks, how often have you felt tired or had little energy?” (response: more than half the days or nearly every day = 1; others = 0). Physical activity was assessed using the International Physical Activity Questionnaire short form, which computed the sum of walking, moderate activity, and vigorous activity to estimate the total metabolic equivalents (MET) minutes per week. Physical activity was categorized into quintiles of sex- and age-specific levels of total MET minutes per week, in which the lowest quintile was identified as “low physical activity.” Slow gait speed was self-reported with the question “How would you describe your usual walking pace?” (response: slow = 1; others = 0). Hand grip strength was measured by using a Jamar J00105 hydraulic hand dynamometer. The measured grip strength was expressed in kilograms by sex- and BMI-adjusted, and the cutoff points have referenced the points by Fried and colleagues [21]. The detailed definition of frailty phenotype was described in Additional file 1: Table S2. Participants were classified as frail (fulfilled ≥ 3 criteria), pre-frail (fulfilled 1–2 criteria), or non-frail (fulfilled 0 criteria).
Ascertainment of outcomes
The primary outcome of interest was overall incident DMC, a composite indicator of the first occurrence of diabetic nephropathy, diabetic neuropathy, and/or diabetic retinopathy. Secondary outcomes included the incidence of three DMC subtypes (diabetic nephropathy, diabetic neuropathy, and diabetic retinopathy). DMC was identified using cumulative hospital inpatient records and death record linkage to national death registries. The definition was described according to the 9th and 10th revisions of the International Classification of Diseases (ICD-9 and ICD-10) and self-reported data fields with choice-, disease-, or procedure-specific codes (Additional file 1: Table S3). We compared the date of the first diagnosis of DMC with the baseline date to distinguish between baseline and incident DMC. Participants diagnosed with DMC after the baseline visit date were identified as incident DMC. At the time of analysis, hospital admission data was available until 30 September 2021 for England, 31 July 2021 for Scotland, and 28 February 2018 for Wales.
Covariates
Sociodemographic factors, lifestyle factors, and health and medical history were acquired using touch screen questionnaires at the baseline. Socioeconomic deprivation was evaluated by Townsend deprivation index scores, and higher scores represent higher levels of socioeconomic deprivation [26]. We defined a healthy diet score based on dietary priorities for cardiovascular disease, diabetes, and obesity [27]. A higher score indicates healthier dietary habits. Definitions of each component of a healthy diet score were described in Additional file 1: Table S4. Smoking status was categorized as ever, former, or current smokers. Alcohol consumption was calculated based on the frequency and alcohol equivalent of different drinks consumed on a typical day/week/month. Height, weight, and blood pressure were measured by a trained nurse during the initial assessment center visit. Body mass index (BMI) was determined as weight in kilograms divided by the square of height in meters. Mean arterial pressure (MAP) was calculated by the following formula: MAP = diastolic blood pressure + 1/3(systolic blood pressure − diastolic blood pressure). HbA1c, lipid profiles (total cholesterol [TC], low-density lipoprotein cholesterol [LDL-C], high-density lipoprotein cholesterol [HDL-C], and triglycerides [TG]), serum creatinine, and cystatin C were measured in the blood sample collected at recruitment. The estimated glomerular filtration rate (eGFR) was calculated from serum creatinine and cystatin C [28]. Considering that long-term chronic diseases are associated with frailty [24], we included a number of long-term conditions [24, 29] as covariates. Given that this study was conducted in patients with diabetes, we exclude diabetes from the number of long-term conditions. The detailed definitions of long-term conditions are shown in Additional file 1: Table S5.
Statistical analysis
Cox proportional hazard regression models considering competing risks (non-DMC-related deaths) by using the cause-specific hazard function model [30] were used to evaluate the associations of frailty phenotype with overall DMC events and subtypes (diabetic nephropathy, diabetic neuropathy, or diabetic retinopathy). The results were presented as hazard ratios (HRs) with 95% confidence intervals (CIs). The time to events was calculated from the date of baseline recruitment to the date of first-time DMC diagnosis, lost to follow-up, death, or the censoring date (30 September 2021 for England, 31 July 2021 for Scotland, 28 February 2018 for Wales), whichever occurred first. Frailty phenotype was assessed as a categorical variable (frail, pre-frail, or non-frail), and the category of “non-frail” was set as the referent in each model or a continuous variable. Frailty phenotype scores were used as a continuous variable in multivariate models when testing the linear trend (per frailty phenotype score increase). The dose–response shape of the association of frailty phenotype score with incident DMC events and subtypes was presented by using the restricted cubic spline model (rms, hmisc, lattice, and survival packages in the R software).
We considered the following covariates in multivariable models sequentially. Model 1 adjusted for age (continuous), sex (male or female), ethnicity (White, mixed, Asian, Black, Chinese, others, or unknown), educational attainment (college or university, vocational, upper secondary, lower secondary, others, or unknown), Townsend deprivation index (in quintiles), annual household income (< 18,000, 18,000–30,999, 31,000–51,999, 52,000–100,000, or >100,000£), and assessment centers (22 categories). Model 2 additionally adjusted for smoking status (ever, former, or current smokers), alcohol intake (0, 0.1–4.9, 5.0–14.9, 15.0–19.9, 20.0–29.9, or ≥ 30.0 g/day), healthy diet score (in quintiles), and BMI (< 18.5, 18.5–24.9, 25.0–29.9, 30.0–34.9, or ≥ 35.0 kg/m2). Model 3 further adjusted for no. of long-term conditions (0, 1, 2, 3, 4, and ≥ 5). Diabetes duration (< 1, 1–4, 5–9, ≥ 10 years), HbA1c (< 53, ≥ 53 mmol/mol [7%]), diabetes medication use (none, only oral medication, only insulin, or insulin and oral medication), lipid-lowering treatment, antihypertensive medication use, and aspirin use were additionally included in the fully adjusted model (model 4). Missing values were considered as dummy variables in regression models. The analyses for five frailty components and DMC events were further adjusted for other frailty components (mutual adjustment).
Several secondary analyses were performed. First, we conducted the stratified analyses that examined the associations of frailty phenotype and overall DMC events across age, sex, educational attainment, Townsend deprivation index, annual household income, smoking status, healthy diet score, BMI, diabetes duration, diabetes medication use, HbA1c levels, and no. of long-term conditions. The joint test was used to examine the interactions between frailty and these subgroups [31]. Second, we excluded those diagnosed with DMC or who died within 2 years of follow-up to minimize the reverse causality. Third, sensitivity analyses were conducted by sequentially adjusting for lipid profile, MAP, and eGFR at baseline based on model 4. Fourth, we used the Fine and Gray subdistribution hazard model, an alternative approach to taking competing risk of mortality, to examine the associations between frailty and DMC. Fifth, sensitivity analyses were conducted by using an alternative measure of comorbidities, the Charlson Comorbidity Index [32] (Additional file 1: Table S6). We also performed mediation analyses to explore the effect of no. of long-term conditions or Charlson Comorbidity Index on the association between frailty and the risk of DMC. It was conducted by using the SAS mediate macro written by Hertzmark et al. [33].
Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and the restricted cubic spline model was conducted in the R software (the R Foundation, http://www.r-project.org, version 4.1.2). P-value < 0.05 was considered statistically significant (two-sided tests).
Results
Baseline characteristics
We included 18,062 middle-aged and older adults with diabetes (mean age 59.4 ± 7.2 years, 37.4% female), of whom 6101 (33.8%) were classified as non-frail, 10,073(55.8%) were classified as pre-frail, and 1888 (10.4%) were classified as frail (Table 1). Compared with subjects with non-frailty, those with pre-frailty and frailty were more likely to have higher BMI, current smokers, lower educated, lower income, less physical activity, and less alcohol intake. They were also more prone to have a longer duration of diabetes, higher HbA1c levels, more prevalent long-term conditions, use of diabetes medication, antihypertensive medication, lipid-lowering treatment, and aspirin at baseline.
During a median follow-up of 12.0 years (198,711 person-years), 3678 DMC cases were documented, including 2213 diabetic nephropathy, 1520 diabetic retinopathy, and 673 diabetic neuropathy events. Of the 3678 new complications, 3036, 556, and 86 patients had one, two, and three DMC, respectively (Table 1). Compared with subjects with one DMC, those with two and three DMC were more likely to be younger and male, have higher BMI, and be subjected to greater deprivation. They were also more prone to have a longer duration of diabetes, higher HbA1c levels, and more common use of diabetes medication, antihypertensive medication, lipid-lowering treatment, and aspirin at baseline (Additional file 1: Table S7).
Association between frailty phenotype and risk of DMC
The incidence of overall DMC per 1000 person-years for non-frail, pre-frail, and frail was 15.39, 18.35, and 31.01, respectively. In Cox regression analyses, we observed that both pre-frailty and frailty were independently and significantly associated with increased risk of DMC and subtypes (Fig. 1 and Additional file 1: Table S8). In the fully adjusted model (model 4), compared with participants with non-frailty, the HRs of those with pre-frailty and frailty were 1.10 (95% CI: 1.02, 1.18) and 1.52 (95% CI: 1.36, 1.69), respectively (P for trend < 0.0001). Similarly, compared to those without frailty, patients with pre-frailty and frailty had a higher risk of developing diabetic nephropathy events (HR 1.15 [95% CI: 1.04, 2.27] for pre-frailty and HR 1.59 [95% CI: 1.38, 1.83] for frailty). Compared to those without frailty, patients with frailty had a higher risk of developing diabetic retinopathy events (HR 1.32 [95% CI: 1.10, 1.58]) and diabetic neuropathy events (HR 1.87 [95% CI: 1.46, 2.39]). In restricted cubic splines, we observed a positive non-linear relationship between frailty phenotype score and incidence of overall DMC (Poverall < 0.0001 and Pnon-linear = 0.0188) and a linear relationship between frailty phenotype score and incidence of DMC subtypes (all Poverall < 0.001 and Pnon-linear > 0.05, Fig. 2). For each one-point increase in frailty phenotype score, the risk of overall DMC, diabetic nephropathy, diabetic retinopathy, and diabetic neuropathy event increased by 13% (95% CI: 10%, 17%), 16% (95% CI: 11%, 20%), 10% (95% CI: 5%, 16%), and 20% (95% CI: 12%, 29%), respectively (Additional file 1: Table S8).

Association between frailty phenotype and risk of diabetic microvascular complications. Cox proportional hazards models adjusted for age, sex, ethnicity, educational attainment, Townsend deprivation index, annual household income, assessment centers, smoking status, alcohol intake, healthy diet score, BMI, no. of long-term conditions, diabetes duration, HbA1c, diabetes medication use, lipid-lowering treatment, antihypertensive medication use, and aspirin use

Dose-response curves for frailty phenotype scores and incidence of diabetic microvascular complications. Data are presented as adjusted hazard ratios with the 95% confidence interval shown as shading. The restricted cubic spline models adjusted for age, sex, ethnicity, educational attainment, Townsend deprivation index, annual household income, assessment centers, smoking status, alcohol intake, healthy diet score, BMI, no. of long-term conditions, diabetes duration, HbA1c, diabetes medication use, lipid-lowering treatment, antihypertensive medication use, and aspirin use
Association between frailty components and risk of DMC
The prevalence of weight loss, exhaustion, low physical activity, slow gait speed, and low grip strength in the study population was 26.8%, 17.9%, 20.0%, 19.3%, and 24.9%, respectively (Additional file 1: Table S9). We further analyzed each frailty component per se and the risk of overall DMC and subtypes (Fig. 3 and Additional file 1: Table S10). In the crude model, all five frailty components, except weight loss, were associated with an increased risk of overall DMC and subtypes. After further adjustment for covariates and the five frailty components, the HRs for overall DMC were gradually attenuated, and exhaustion (HR 1.11, 95% CI: 1.02, 1.21), low physical activity (HR 1.09, 95% CI: 1.01, 1.18), slow gait speed (HR 1.37, 95% CI: 1.26, 1.48), and low grip strength (HR 1.08, 95% CI: 1.00, 1.16) were independently associated with risk of over DMC. Exhaustion (HR 1.18, 95% CI: 1.06, 1.31), low physical activity (HR 1.11, 95% CI: 1.00, 1.23), and slow gait speed (HR 1.44, 95% CI: 1.30, 1.60) exhibited a risk association for diabetic nephropathy events. Slow gait speed (HR 1.18, 95% CI: 1.05, 1.33) was associated with higher diabetic retinopathy events. For diabetic neuropathy events, exhaustion (HR 1.20, 95% CI: 1.00, 1.44) and slow gait speed (HR 1.77, 95% CI: 1.47, 2.12) showed a risk association. However, we did not observe a significant association of weight loss with overall DMC and subtypes risk in the mutual adjustment model.

Association between frailty phenotype components and risk of diabetic microvascular complications. Cox proportional hazards models adjusted for age, sex, ethnicity, educational attainment, Townsend deprivation index, annual household income, assessment centers, smoking status, alcohol intake, healthy diet score, BMI, no. of long-term conditions, diabetes duration, HbA1c, diabetes medication use, lipid-lowering treatment, antihypertensive medication use, and aspirin use, and mutually adjusted for other frailty components
Secondary analyses
In stratified analyses, the association between frailty phenotype and incident DMC was not significantly modified by all subgroup factors (all P for interaction > 0.05) (Additional file 1: Table S11). To minimize the reverse causation, we excluded 353 individuals diagnosed with any microvascular complications or who died within 2 years of follow-up, and the results remained robust (Additional file 1: Table S12). In sensitivity analyses, by sequentially adjusting for lipids, MAP, and eGFR based on model 4, pre-frailty and frailty were still associated with a significantly higher risk of DMC (Additional file 1: Table S13). The associations remained robust in the Fine and Gray competing models (Additional file 1: Table S14). The associations remained robust in sensitivity analyses using an alternative measure of comorbidities, the Charlson Comorbidity Index (Additional file 1: Table S15). In mediation analysis, we found that comorbidities, whether the number of long-term conditions or the Charlson Comorbidity Index, significantly mediated the association between frailty phenotype and incident overall DMC, accounting for 19.8% or 13.1% of the proportion mediated (Additional file 1: Table S16).
Discussion
In this study of 18,062 middle-aged and older adults with T2D from the UK Biobank, the prevalence of pre-frailty and frailty, based on a widely used Fried frailty phenotype, was 55.8% and 10.4%, respectively. We observed a positive association between frailty score and incident DMC; with each one-point increase in the score, the risk of overall DMC and subtypes event increased by 10 to 20%. Compared with non-frail patients, those with pre-frailty and frailty had a 10 to 52% higher risk of DMC after considering potential confounders. Such associations remained robust in the subtypes of DMC.
The prevalence of frailty and pre-frailty was 10.4% and 55.8% in middle-aged and older adults with T2D, respectively, which is comparable to the rates reported in a previous study from the UK Biobank [34]. However, the prevalence of frailty was lower than that in similar studies that reported 13.0 to 16.3% of diabetes were subjected to frailty [10, 12]. The main reason we speculated was the selection bias of “healthy volunteers” in the UK Biobank, which may have had better health status [35].
To our knowledge, this is the first large study concerning the longitudinal association between frailty phenotype and DMC. Our findings that frailty in T2D was associated with increased risk of DMC events are in line with two prospective studies where frailty was defined as Rockwood’s frailty index and Clinical Frailty Scale [16, 19]. A study by Nguyen et al. [16], where a secondary post hoc analysis of the ADVANCE trial, found that Rockwood’s frailty index was independently associated with increased microvascular events (defined as new or worsening diabetic nephropathy or diabetic retinopathy) (n = 11,140, HR: 1.60 [95% CI: 1.42, 1.81]). Another study of 371 diabetes patients aged ≥ 70 years in the Canadian Study of Health and Aging, where frailty was defined using the Clinical Frailty Scale, indicated that frail older adults were 2.62 times (95% CI: 1.36, 5.06) more likely to have a complication of diabetes (diabetic retinopathy, recurrent infections, diabetic nephropathy, and diabetic neuropathy), independent of age, sex, and number of years living with diabetes [19]. However, in a retrospective cohort of 54,505 patients initiating oral antidiabetic drugs from a large US claims and integrated laboratory database, frailty derived from Johns Hopkins-adjusted clinical groups was not associated with new-onset DMC (HR 0.89 [95% CI: 0.70, 1.13]) [20]. Differences in the results may be due to the differences in frailty assessment criteria, study design, and duration of follow-up. In our study, we used the frailty definition described by Fried and colleagues as the clinical manifestations of frailty based on physical phenotypes [21]. They provided a standardized and validated physiologically based definition and clear criteria that are relatively easy and inexpensive to apply and offer a basis for standardized screening for frailty, which now has been one of the most common frailty instruments [8, 9] and the most commonly used measures of frailty in diabetes [12]. We first reported that pre-frailty and frailty based on physical phenotypes were associated with higher DMC risk, and such association remained robust after considering a wealth of covariates, including sociodemographic variables, lifestyles, medical history, medication use, long-term conditions, and glycemic control. In addition, we found consistent results between frailty and diabetic nephropathy, diabetic neuropathy, and diabetic retinopathy, which had not been reported in previous studies that focused only on frailty and overall DMC [16, 19, 20].
In the present study, we found that exhaustion, low physical activity, slow gait speed, and low grip strength were independently associated with an increased risk of overall DMC. Gait speed and handgrip strength are robust predictors of adverse health events in older patients [36, 37]. Previous evidence suggests that physical performance measures are impaired in diabetic patients [38]. Lower grip strength was associated with poor glycemic control in patients with diabetes mellitus (OR: 0.67; 95% CI: 0.47, 0.97) [39]. However, their association with DMC has never been examined, and our study filled this gap and provided new insights into the management of microvascular complications in diabetes.
Although frailty is not currently assessed in routine clinical practice, its importance in diabetes is increasingly recognized in clinical guidelines [40, 41]. Our results support the advocacy of integrating frailty assessment into the routine management of diabetes. In addition to frailty, patients with pre-frailty should be concerned. We found that more than half (55.8%) of T2D have pre-frailty, a higher prevalence than the 49.1% (95% CI: 45.1%, 53.1%) reported in the meta-analysis of community-dwelling older adults with diabetes [10], and they also carried a considerable risk of incident DMC. Pre-frailty is in relation to an increased risk of mortality and cardiovascular events, and imposes greater healthcare expenditure on patients with diabetes [15, 24]. However, few studies have explored the relationship between pre-frailty and incident DMC. More importantly, pre-frailty is a potentially reversible and highly prevalent intermediate state before frailty. Compared to those with no frailty criteria at baseline, individuals with pre-frailty have 2.63 times the risk predisposed to develop into frailty [21]. Our findings fill these evidence gaps that pre-frailty could increase the risk of DMC in patients with diabetes, highlighting the importance of pre-frailty management. Notably, the splines in our results demonstrated a clear positive dose-response correlation between frailty score and overall DMC and three subtypes, implicating that any stage of the frailty progression should be a concern in diabetes management. Regardless of the clinical setting, clinicians are likely to encounter patients with frailty when managing diabetes. In clinical contexts, a nuanced approach (including distinguishing frailty levels and understanding individual patient needs and priorities in the frailty context) may be essential [12]. There is emerging evidence that strategies based on educational, nutritional, and exercise-based interventions seem helpful in delaying or reversing frailty in primary care [42, 43]. As such evidence accumulates, frailty identification, assessment, and management should be part of personalizing treatment for patients with diabetes.
Potential mechanisms
The development of DMC results from a combination of hyperglycemia-induced endothelial damage, oxidative stress, the production of sorbitol and advanced glycation end-products, pro-inflammation cytokines release, chronic inflammation, protein kinase C activation, and transformation growth factor β upregulation [44, 45]. These metabolic injuries lead to changes in blood flow, endothelial permeability, extravascular protein deposition, and coagulation and induce organ dysfunction [44]. Inflammation and insulin resistance are the precursors of frailty [46] and may also act as the common pathophysiology mechanisms shared by frailty and DMC. Frailty may trigger an inflammatory response, promoting inflammation-mediated insulin resistance and endothelial dysfunction. Besides, loss of muscle mass and strength could lead to metabolic dysregulation resulting in reduced insulin sensitivity, altered oxidative defenses, and decreased mitochondrial function [47], which may promote the occurrence of DMC. Notably, compared with T2D patients free of frailty, those with frailty derive fewer benefits from intensive glucose-lowering and blood pressure-lowering treatments [16], which is known that hyperglycemia and hypertension are common pathophysiological and risk factors for DMC [45].
Strengths and limitations
Major strengths of the current study included prospective design, long-term follow-up (12.0 years), and high-quality data from the UK Biobank. However, several limitations should be considered. First, some self-reported indicators of frailty phenotype, such as weight loss, exhaustion, and walking speed, were subject to reporting bias, which is usually the main problem in epidemiology. Second, the diagnosis of DMC mainly relied on self-report and the ICD codes, and the incident rates of DMC and its subtypes might be underestimated. The phenomenon might be explained by the “healthy volunteers” bias in the UK Biobank and difficulties for frailty patients to assess medical care and be diagnosed with DMC. Additionally, participants with pre-frailty and frailty may have had undiagnosed DMC at baseline, which might lead to an overestimation of DMC risk for frailty. However, the association was still robust when we excluded participants who developed any DMC or died within 2 years of follow-up. Third, the diagnosis of DMC was identified using cumulative hospital records and death record linkage to national death registries according to the ICD code. Therefore, the potential for misclassification of patients with incident DMC might attenuate findings toward the null, leading to an underestimation of the magnitudes of the true association. Fourth, although we considered a wide range of potential confounders and performed several sensitivity analyses, the residual confounding and potential bias cannot be completely ruled out due to the nature of the observational study. Fifth, as the participants from the UK were predominantly of European ancestry, our findings may not be directly generalizable to other populations, and thus, more research is needed on other ethnic and racial groups.
Conclusions
In this large prospective cohort of 18,062 diabetes patients, we observed that both pre-frailty and frailty were associated with an increased risk of overall DMC and subtypes, including diabetic nephropathy, diabetic neuropathy, and diabetic retinopathy. The presence of comorbidities partly mediated the association between frailty and the risk of DMC. These findings have important implications for integrating routine clinical assessment and surveillance of frailty into the prevention and management of DMC in diabetes.
Availability of data and materials
Data from the UK Biobank are available to all researchers upon making an application. This research has been conducted using the UK Biobank Resource under Application 63454.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- DMC:
-
Diabetic microvascular complications
- eGFR:
-
Estimated glomerular filtration rate
- HbA1c:
-
Glycated hemoglobin A1c
- HDL-C:
-
High-density lipoprotein cholesterol
- HR:
-
Hazard ratio
- ICD:
-
International classification of diseases
- IQR:
-
Interquartile range
- LDL-C:
-
Low-density lipoprotein cholesterol
- MAP:
-
Mean arterial pressure
- METs:
-
Metabolic equivalent tasks
- SD:
-
Standard deviation
- T2D:
-
Type 2 diabetes
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
References
International Diabetes Federation. IDF Diabetes Atlas, 10th Edition, 2021. Available from https://diabetesatlas.org/en/. Accessed 10 January 2022.
Kähm K, Laxy M, Schneider U, Rogowski WH, Lhachimi SK, Holle R. Health care costs associated with incident complications in patients with type 2 diabetes in Germany. Diabetes Care. 2018;41(5):971–8. https://doi.org/10.2337/dc17-1763.
Chen HY, Kuo S, Su PF, Wu JS, Ou HT. Health care costs associated with macrovascular, microvascular, and metabolic complications of type 2 diabetes across time: estimates from a population-based cohort of more than 0.8 million individuals with up to 15 years of follow-up. Diabetes Care. 2020;43(8):1732–40. https://doi.org/10.2337/dc20-0072.
Litwak L, Goh SY, Hussein Z, Malek R, Prusty V, Khamseh ME. Prevalence of diabetes complications in people with type 2 diabetes mellitus and its association with baseline characteristics in the multinational A1chieve study. Diabetol Metab Syndr. 2013;5(1):57. https://doi.org/10.1186/1758-5996-5-57.
Zelnick LR, Weiss NS, Kestenbaum BR, Robinson-Cohen C, Heagerty PJ, Tuttle K, et al. Diabetes and CKD in the United States population, 2009-2014. Clin J Am Soc Nephrol. 2017;12(12):1984–90. https://doi.org/10.2215/cjn.03700417.
Yau JW, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–64. https://doi.org/10.2337/dc11-1909.
Feldman EL, Callaghan BC, Pop-Busui R, Zochodne DW, Wright DE, Bennett DL, et al. Diabetic neuropathy. Nat Rev Dis Primers. 2019;5(1):42. https://doi.org/10.1038/s41572-019-0097-9.
Dent E, Martin FC, Bergman H, Woo J, Romero-Ortuno R, Walston JD. Management of frailty: opportunities, challenges, and future directions. Lancet. 2019;394(10206):1376–86. https://doi.org/10.1016/s0140-6736(19)31785-4.
Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–75. https://doi.org/10.1016/s0140-6736(19)31786-6.
Kong LN, Lyu Q, Yao HY, Yang L, Chen SZ. The prevalence of frailty among community-dwelling older adults with diabetes: a meta-analysis. Int J Nurs Stud. 2021;119:103952. https://doi.org/10.1016/j.ijnurstu.2021.103952.
Castro-Rodríguez M, Carnicero JA, Garcia-Garcia FJ, Walter S, Morley JE, Rodríguez-Artalejo F, et al. Frailty as a major factor in the increased risk of death and disability in older people with diabetes. J Am Med Dir Assoc. 2016;17(10):949–55. https://doi.org/10.1016/j.jamda.2016.07.013.
Hanlon P, Fauré I, Corcoran N, Butterly E, Lewsey J, McAllister D, et al. Frailty measurement, prevalence, incidence, and clinical implications in people with diabetes: a systematic review and study-level meta-analysis. Lancet Healthy Longev. 2020;1(3):e106–e16. https://doi.org/10.1016/s2666-7568(20)30014-3.
Li G, Prior JC, Leslie WD, Thabane L, Papaioannou A, Josse RG, et al. Frailty and risk of fractures in patients with type 2 diabetes. Diabetes Care. 2019;42(4):507–13. https://doi.org/10.2337/dc18-1965.
Chao CT, Wang J, Chien KL. Both pre-frailty and frailty increase healthcare utilization and adverse health outcomes in patients with type 2 diabetes mellitus. Cardiovasc Diabetol. 2018;17(1):130. https://doi.org/10.1186/s12933-018-0772-2.
Ida S, Kaneko R, Imataka K, Murata K. Relationship between frailty and mortality, hospitalization, and cardiovascular diseases in diabetes: a systematic review and meta-analysis. Cardiovasc Diabetol. 2019;18(1):81. https://doi.org/10.1186/s12933-019-0885-2.
Nguyen TN, Harris K, Woodward M, Chalmers J, Cooper M, Hamet P, et al. The impact of frailty on the effectiveness and safety of intensive glucose control and blood pressure-lowering therapy for people with type 2 diabetes: results from the ADVANCE Trial. Diabetes Care. 2021;44(7):1622–9. https://doi.org/10.2337/dc20-2664.
Li Y, Zou Y, Wang S, Li J, Jing X, Yang M, et al. A pilot study of the FRAIL Scale on predicting outcomes in Chinese elderly people with type 2 diabetes. J Am Med Dir Assoc. 2015;16(8):714.e7–e12. https://doi.org/10.1016/j.jamda.2015.05.019.
McAlister FA, Lethebe BC, Lambe C, Williamson T, Lowerison M. Control of glycemia and blood pressure in British adults with diabetes mellitus and subsequent therapy choices: a comparison across health states. Cardiovasc Diabetol. 2018;17(1):27. https://doi.org/10.1186/s12933-018-0673-4.
Hubbard RE, Andrew MK, Fallah N, Rockwood K. Comparison of the prognostic importance of diagnosed diabetes, co-morbidity and frailty in older people. Diabet Med. 2010;27(5):603–6. https://doi.org/10.1111/j.1464-5491.2010.02977.x.
Simpson SH, Lin M, Eurich DT. Medication adherence affects risk of new diabetes complications: a cohort study. Ann Pharmacother. 2016;50(9):741–6. https://doi.org/10.1177/1060028016653609.
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–56. https://doi.org/10.1093/gerona/56.3.m146.
Sudlow C, Gallacher J, Allen N, Beral V, Burton P, Danesh J, et al. UK Biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015;12(3):e1001779. https://doi.org/10.1371/journal.pmed.1001779.
Eastwood SV, Mathur R, Atkinson M, Brophy S, Sudlow C, Flaig R, et al. Algorithms for the capture and adjudication of prevalent and incident diabetes in UK Biobank. PLoS One. 2016;11(9):e0162388. https://doi.org/10.1371/journal.pone.0162388.
Hanlon P, Nicholl BI, Jani BD, Lee D, McQueenie R, Mair FS. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK Biobank participants. Lancet Public Health. 2018;3(7):e323–e32. https://doi.org/10.1016/s2468-2667(18)30091-4.
Petermann-Rocha F, Lyall DM, Gray SR, Esteban-Cornejo I, Quinn TJ, Ho FK, Pell JP, Celis-Morales C. Associations between physical frailty and dementia incidence: a prospective study from UK Biobank. Lancet Healthy Longev. 2020;1(2):e58–68. https://doi.org/10.1016/S2666-7568(20)30007-6.
Foster HME, Celis-Morales CA, Nicholl BI, Petermann-Rocha F, Pell JP, Gill JMR, et al. The effect of socioeconomic deprivation on the association between an extended measurement of unhealthy lifestyle factors and health outcomes: a prospective analysis of the UK Biobank cohort. Lancet Public Health. 2018;3(12):e576–e85. https://doi.org/10.1016/s2468-2667(18)30200-7.
Mozaffarian D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity: a comprehensive review. Circulation. 2016;133(2):187–225. https://doi.org/10.1161/circulationaha.115.018585.
Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367(1):20–9. https://doi.org/10.1056/NEJMoa1114248.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. https://doi.org/10.1016/s0140-6736(12)60240-2.
Austin PC, Lee DS, Fine JP. Introduction to the analysis of survival data in the presence of competing risks. Circulation. 2016;133(6):601–9. https://doi.org/10.1161/circulationaha.115.017719.
SAS Institute. The PHREG procedure: type 3 tests and joint tests. https://support.sas.com/documentation/cdl/en/statug/67523/HTML/default/viewer.htm#statug_phreg_details32.htm. Accessed Oct 30, 2021. .
Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–51. https://doi.org/10.1016/0895-4356(94)90129-5.
Hertzmark E, Pazaris M, Spiegelman D. The SAS mediate macro: Harvard TH Chan School of Public Health; 2018.
Hanlon P, Jani BD, Butterly E, Nicholl B, Lewsey J, McAllister DA, et al. An analysis of frailty and multimorbidity in 20,566 UK Biobank participants with type 2 diabetes. Commun Med (Lond). 2021;1(1):1–9.
Fry A, Littlejohns TJ, Sudlow C, Doherty N, Adamska L, Sprosen T, et al. Comparison of sociodemographic and health-related characteristics of UK Biobank participants with those of the general population. Am J Epidemiol. 2017;186(9):1026–34. https://doi.org/10.1093/aje/kwx246.
Bohannon RW. Hand-grip dynamometry predicts future outcomes in aging adults. J Geriatr Phys Ther. 2008;31(1):3–10. https://doi.org/10.1519/00139143-200831010-00002.
Cesari M, Kritchevsky SB, Newman AB, Simonsick EM, Harris TB, Penninx BW, et al. Added value of physical performance measures in predicting adverse health-related events: results from the Health, Aging And Body Composition Study. J Am Geriatr Soc. 2009;57(2):251–9. https://doi.org/10.1111/j.1532-5415.2008.02126.x.
Yokoyama H, Shiraiwa T, Takahara M, Iwamoto M, Kuribayashi N, Nomura T, et al. Applications of physical performance measures to routine diabetes care for frailty prevention concept: fundamental data with grip strength, gait speed, timed chair stand speed, standing balance, and knee extension strength. BMJ Open Diabetes Res Care. 2020;8(1). https://doi.org/10.1136/bmjdrc-2020-001562.
Choe H, Sung H, Kim GH, Lee O, Moon HY, Kim YS. Associations between grip strength and glycemic control in type 2 diabetes mellitus: an analysis of data from the 2014-2019 Korea National Health and Nutrition Examination Survey. Epidemiol Health. 2021;43:e2021080. https://doi.org/10.4178/epih.e2021080.
Sinclair AJ, Abdelhafiz A, Dunning T, Izquierdo M, Rodriguez Manas L, Bourdel-Marchasson I, et al. An international position statement on the management of frailty in diabetes mellitus: summary of recommendations 2017. J Frailty Aging. 2018;7(1):10–20. https://doi.org/10.14283/jfa.2017.39.
Draznin B, Aroda VR, Bakris G, Benson G, Brown FM, Freeman R, et al. 13. Older adults: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S195–s207. https://doi.org/10.2337/dc22-S013.
Travers J, Romero-Ortuno R, Bailey J, Cooney MT. Delaying and reversing frailty: a systematic review of primary care interventions. Br J Gen Pract. 2019;69(678):e61–e9. https://doi.org/10.3399/bjgp18X700241.
Assar ME, Laosa O, Rodríguez ML. Diabetes and frailty. Curr Opin Clin Nutr Metab Care. 2019;22(1):52–7. https://doi.org/10.1097/mco.0000000000000535.
Vithian K, Hurel S. Microvascular complications: pathophysiology and management. Clin Pract (Lond). 2010;10(5):505–9. https://doi.org/10.7861/clinmedicine.10-5-505.
Valencia WM, Florez H. How to prevent the microvascular complications of type 2 diabetes beyond glucose control. BMJ Med. 2017;356:i6505. https://doi.org/10.1136/bmj.i6505.
Barzilay JI, Blaum C, Moore T, Xue QL, Hirsch CH, Walston JD, et al. Insulin resistance and inflammation as precursors of frailty: the Cardiovascular Health Study. Arch Intern Med. 2007;167(7):635–41. https://doi.org/10.1001/archinte.167.7.635.
Sanz-Cánovas J, López-Sampalo A, Cobos-Palacios L, Ricci M, Hernández-Negrín H, Mancebo-Sevilla JJ, et al. Management of type 2 diabetes mellitus in elderly patients with frailty and/or sarcopenia. Int J Environ Res Public Health. 2022;19(14). https://doi.org/10.3390/ijerph19148677.
Acknowledgements
The authors would like to thank all participants in the UK Biobank for their gratitude and all the staff of the UK Biobank.
Funding
Dr. Chen is supported by the National Key Research and Development Program of China (2020YFC2006300) and the National Natural Science Foundation of China (82003461). Dr. Wu is supported by the National Natural Science Foundation of China (82103835). Dr. Tan is supported by Ake Wiberg Foundation (M18-0169, M19-0266) and Fredrik and Ingrid Thuring Foundation (2019-00488). The funders had no role in the study design, data collection and analysis, publication decision, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
L.C. conceived and designed the study. Y.W. and L.C. analyzed and interpreted the data. Y.W. drafted the manuscript. T.X., X.T., and L.C. revised it critically for important intellectual content. The authors read and approved the final manuscript. The corresponding authors attest that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the North West–Haydock Research Ethics Committee (16/NW/0274). All participants provided informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
Flow of participants in current study. Table S1. The definitions for baseline diabetes. Table S2. Definition of frailty phenotype and cutoff Points. Table S3. Definition of diabetic microvascular complications. Table S4. Definition of each component of a healthy diet score. Table S5. Definition and list of long-term morbidities. Table S6. Definition and list of Charlson Comorbidity Index. Table S7. Baseline characteristics of 3678 patients with type 2 diabetes by number of diabetic microvascular complications. Table S8. Association between frailty phenotype and risk of diabetic microvascular complications. Table S9. Prevalence of frailty phenotype components in percentages. Table S10. Association between frailty components and risk of diabetic microvascular complications. Table S11. Association between frailty and risk of overall diabetic microvascular complications by subgroups. Table S12. Sensitivity analyses of association between frailty phenotype and risk of overall diabetic microvascular complications (exclude individuals diagnosed any microvascular complications within 2 years of follow-up). Table S13. Sensitivity analyses of association between frailty phenotype and risk of overall diabetic microvascular complications by sequentially adjusting for lipid profile, MAP, eGFR. Table S14. Association between frailty phenotype and risk of overall diabetic microvascular complications using Fine & Gray models for competing risk. Table S15. Sensitivity analyses of association between frailty phenotype and risk of diabetic microvascular complications were conducted by using the Charlson Comorbidity Index as an alternative measure of comorbidities. Table S16. Mediating effects of multimorbidity on the association of frailty phenotype with risk of diabetic microvascular complications among type 2 diabetes.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, Y., Xiong, T., Tan, X. et al. Frailty and risk of microvascular complications in patients with type 2 diabetes: a population-based cohort study. BMC Med 20, 473 (2022). https://doi.org/10.1186/s12916-022-02675-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-022-02675-9