
Abstract
Background
Certain factors contribute to healthcare professionals’ adaptive capacities towards risks, challenges, and changes such as attitudes, stress, motivation, cognitive capacity, group norms, and teamwork. However, there is limited evidence as to factors that contribute to healthcare professionals’ adaptive capacity towards hospital standardization. This scoping review aimed to identify and map the factors contributing to healthcare professionals’ adaptive capacity with hospital standardization.
Methods
Scoping review methodology was used. We searched six academic databases to September 2021 for peer-reviewed articles in English. We also reviewed grey literature sources and the reference lists of included studies. Quantitative and qualitative studies were included if they focused on factors influencing how healthcare professionals adapted towards hospital standardization such as guidelines, procedures, and strategies linked to clinical practice. Two researchers conducted a three-stage screening process and extracted data on study characteristics, hospital standardization practices and factors contributing to healthcare professionals’ adaptive capacity. Study quality was not assessed.
Results
A total of 57 studies were included. Factors contributing to healthcare professionals’ adaptive capacity were identified in numerous standardization practices ranging from hand hygiene and personal protective equipment to clinical guidelines or protocols on for example asthma, pneumonia, antimicrobial prophylaxis, or cancer. The factors were grouped in eight categories: (1) psychological and emotional, (2) cognitive, (3) motivational, (4) knowledge and experience, (5) professional role, (6) risk management, (7) patient and family, and (8) work relationships. This combination of individual and group/social factors decided whether healthcare professionals complied with or adapted hospital standardization efforts. Contextual factors were identified related to guideline system, cultural norms, leadership support, physical environment, time, and workload.
Conclusion
The literature on healthcare professionals’ adaptive capacity towards hospital standardization is varied and reflect different reasons for compliance or non-compliance to rules, guidelines, and protocols. The knowledge of individual and group/social factors and the role of contextual factors should be used by hospitals to improve standardization practices through educational efforts, individualised training and motivational support. The influence of patient and family factors on healthcare professionals’ adaptive capacity should be investigated.
Trial registration
Open Science Framework (https://osf.io/ev7az) https://doi.org/10.17605/OSF.IO/EV7AZ.
Similar content being viewed by others


Background
Studies have shown discrepancies between hospital policies and procedures set to improve quality of care and their implementation by healthcare professionals [1, 2]. Why do healthcare professionals not comply with institutional policies, protocols, guidelines, and checklists set to improve quality? Healthcare professionals may be well intentioned and strive to offer quality of care, but they also face challenges such as limited resources, increasing work pressure, and burnout [3,4,5]. Non-compliance is multifactorial due to the complexity of the healthcare system and the quantity of information and hospital policies. Some factors are linked to the individual healthcare professionals, e.g. training, beliefs, habits, psychological factors and other factors are contextual such as social norms, staff workload and competing goals between the individual and the institution.
Adaptation or adaptive capacity is seen as a main pillar in resilience across several disciplines [6,7,8]. Several studies have aimed at exploring and understanding how resilience contributes to healthcare professionals’ adaptive capacities towards challenging work conditions [9,10,11], but still it is poorly understood. According to Smaggus [2] hospital healthcare professionals proactively adapt to compensate for systemic problems such as protocols and technology poorly aligned with their tasks. They do so through their dedication, expertise, and creativity. However, these adaptations might come at a cost to professionals’ well-being as they often include working longer and more intense hours. In the context of this study healthcare professionals’ adaptive capacity is seen as essential for hospital standardization to be successfully practiced thus contributing to quality of care. Adaptations might come in the forms of compliance or non-compliance to standardized guidelines and protocols, or in the forms of adjustment of the contents of the standardization efforts.
There are certain factors that contribute to healthcare professionals’ adaptive capacity such as habits, stress, anxiety, burnout, coping mechanisms, motivation (internal and external), intention, level of knowledge and education, cognitive capacity, perceptions, attitudes, and beliefs (individual and social) [9,10,11]. No evidence was found of literature reviews exploring factors that contribute to healthcare professionals’ adaptive capacity with hospital standardization, except one focusing on hand hygiene guideline adherence [12] and one on nurses’ non-compliance in infection prevention [5].
Therefore, the aim of this scoping review is to identify and map the factors contributing to healthcare professionals’ adaptive capacity with hospital standardization. Specific research questions addressed by this review were:
-
1. In which hospital standardization practices have healthcare professionals’ adaptive capacity been studied?
-
2. What factors influence healthcare professionals’ adaptive capacity with hospital standardization and how can they be categorized?
Methods
A scoping review methodology was chosen because it provides a transparent approach to mapping relevant literature in emerging fields or topics [13, 14] and has a broader “scope” and more expansive inclusion criteria than a systematic review [15, 16]. It also allows for studies using different designs and methods to be included and synthesized, which was considered necessary for this review. We followed the methodological stages outlined by Arksey and O’Malley [13] and Levac et al.’s [17] enhancement to conduct the review. These were: (1) Identifying the research question, (2) Identifying relevant studies, (3) Study selection, (4) Charting the data, (5) Collating, summarizing and reporting the results, and (6) Consulting with relevant stakeholders. A review protocol was developed according to Peters et al. [14] and registered on October 11th 2021 on the Open Science Framework (https://osf.io/ev7az) https://doi.org/10.17605/OSF.IO/EV7AZ. The reporting of the review follows the PRISMA-ScR Checklist [18] (Additional file 1).
Eligibility criteria
Articles were assessed against the following inclusion criteria: English-language, peer-reviewed research articles of any type published in scholarly journals where the full text was available, as well as grey literature not published in peer-reviewed journals. We chose to focus on healthcare professionals above 25 years indicating that they would have a minimum level of clinical experience including experiences with hospital standardization efforts. Furthermore, we chose the hospital setting to be able to possibly compare different standardization efforts identified. For a full description of inclusion and exclusion criteria, see Additional file 2.
Information sources
The focus of the review was on peer-reviewed literature and electronic databases from different disciplines such as biomedicine, psychology, health services research, and nursing were searched on 12.10.2021 to identify relevant studies. The electronic databases searched included Scopus, MEDLINE (Ebsco & Ovid), Web of Science, CINAHL, EMBASE and PsycINFO [19]. Search terms were discussed by the three authors. The preliminary search strategy, search terms and inclusion/exclusion criteria were checked by a research librarian at the University of Stavanger.
The electronic database searches were then conducted by one researcher (FTK) and included all citations published before October 2021. A combination of Title, Subject, Subject headings, MeSH terms, and Keywords/Text words was used. The search strategy was adapted to individual databases. An example of a search strategy is presented in Table 1.
To reduce the likelihood that relevant articles were overlooked we also hand searched reference lists of included articles and did an additional snowball-search. To further ensure that all relevant information was captured we conducted a targeted search of the grey literature in Google Scholar and in the following grey literature databases: Grey Literature Report (https://www.greylit.org/) and OpenGrey (http://www.opengrey.eu/). Hand searches, snowball-search, and grey literature resulted in an additional 19 records. All the search results were imported into EndNote bibliographic software and merged.
Selection of sources of evidence
The review process consisted of three levels of screening: (1) title, (2) abstract, and (3) full text. For the first level of screening, one researcher (FTK) screened the titles of retrieved citations. Abstract and full text screening involved two researchers (FTK and KA) who shared and independently assessed the articles to determine if they met the inclusion/exclusion criteria. Articles considered relevant by the reviewers were included in the full-text review. Discrepancies about study eligibility at the full-text review stage was solved through discussion for 14 studies. Consensus was achieved between the two researchers making it unnecessary to involve the third researcher (SW) at this stage.
Quality assessment of the included studies did not form part of the current scoping review [13]. Therefore, all studies were included in the analysis as they would potentially contribute to mapping the knowledge base.
Data charting process and data items
An electronic data charting form was developed in excel to guide data charting from included articles. Data concerning study characteristics, e.g., authors, year of publication, and the methodology, e.g., design, data collection, participants, results were charted in addition to information related to the aim of the review, i.e., hospital standardization type, factors of adaptive capacity, individual level, group/social level, and reviewers’ notes (Table 2).
The initial data charting sheet was validated by two reviewers (FTK and KA) with three articles each to corroborate consistency, as recommended by Daudt, van Mossel and Scott [20]. All data was extracted by two researchers (FTK, KA) independently and then agreed and merged with input and discussion by the third researcher (SW).
Synthesis of results
Results were synthesised and presented using frequency counting as well as summarised in text as categories. The data were compared and synthesised to summarise study characteristics, hospital standardization effort, and factors affecting healthcare professionals’ adaptive capacity. All three authors were involved in the process of synthesizing and describing the results in a suitable format.
Consultation with stakeholders
According to Levac et al. [17], we conducted the optional stage of consulting with relevant stakeholders once the results were synthesized. The researchers of the Centre for Resilience in Healthcare SHARE, University of Stavanger were identified as relevant and knowledgeable stakeholders on the topic. Hence, an email with draft results was sent to all 79 centre researchers with a request for feedback and input on any additional sources of information relevant to the research questions of the scoping study. Stakeholders’ literature input was sent to author FTK (one book and three studies) who then assessed the information. No additional studies were included.
Results
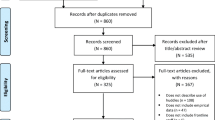
The search resulted in 1414 unique records of which 180 full-text articles were assessed for eligibility and 57 were included in the review [12, 21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76]. From the grey literature four articles met the inclusion criteria. The most common reasons for exclusion were no healthcare professional related factors described, mixed sample with unclear reporting of results for healthcare professionals, not in hospital setting or setting unclear, or not a healthcare professional sample.
A total of 27 qualitative studies, 20 quantitative studies, six literature reviews, and four mixed-method studies were included in the review. Figure 1 demonstrates the inclusion and exclusion of records at each stage of the screening process, using the PRISMA flow diagram [77].

PRISMA flow diagram
Characteristics of studies
The included studies were published between 2000 and 2021, with a tendency towards increased publication frequency over the last five-year period (2017–2021). The studies originated from 26 different countries with all continents represented. Several of the studies were conducted in Australia (n = 5), Jordan (n = 5), USA (n = 5), the Netherlands (n = 4), China (n = 3), and the UK (n = 3). Twenty-nine studies were conducted in developed countries while 19 in developing countries. A total of 9 studies had unspecified country origin, the reason usually being that they were literature reviews.
Hospital standardization practices
The review identified healthcare professionals’ adaptive capacity in numerous standardization practices across hospitals’ specialties. The most common standardization types were clinical or practice guidelines and protocols, precautions, procedures, checklists, policies, forms, and hospital-generic precautions, rules, and regulations. The most common areas of standardization were hand hygiene and infection prevention, personal protective equipment use, surgery, medication administration, cancer, mother and new-born care, falls, asthma, and pneumonia (Table 3). Three studies on personal protective equipment use were conducted during pandemics [51, 52, 54] while two studies explored infection prevention after pandemics [32, 55].
Factors influencing healthcare professionals’ adaptive capacity
The factors influencing healthcare professionals’ adaptive capacity with hospital standardization practices were grouped in eight categories as described in Table 4. The eight categories constitute a combination of individual and group/social factors deciding whether hospital healthcare professionals comply with or adapt hospital standardization practices. Below the eight categories are described in more detail.
Psychological and emotional factors
In many instances professionals choose to adhere to infection prevention guidelines due to the psychological pressure or fear of contracting or spreading infections [23, 32, 41]. Adverse incidents with infection prevention equipment are perceived as stressful and worrying [51], while following standard precautions would decrease their anxiety [41].
Healthcare professionals’ sense of invulnerability and confidence would lead them to adapt hospital standardization [22, 31, 55, 63, 75]. Reasons would differ from physicians considering themselves to be entitled to work independently without protocols to guide them [31], to professionals feeling minor concerns for infection transmission over time when not acquiring any infection [55] to nurses expressing psychological gratification about their own ability to creatively solve problems and work around standardization practices [75].
Cognitive factors
Various attitudes and beliefs were reported in several studies as influencing healthcare professionals’ adaptive capacity or compliance to hospital standardization [28, 29, 33, 37, 41, 45, 47, 48, 52, 55, 61, 62, 69, 73, 75]. Some of these attitudes and beliefs were patient related [41, 45, 52, 62, 69, 74, 75]. For example, in a study on the use of personal protective equipment in the emergency room during the COVID-19 pandemic, there was only a slight difference between healthcare professional beliefs on whether the equipment was protective or not for patients (52% vs. 46%) [52]. In another study, physicians believed that diarrhoea was a low-risk disease with overrepresentation among poor people but adapted the diarrhoea treatment to patients with higher social status [45]. Moreover, nurses justified adaptations when they believed that use of gloves or masks was an exaggeration when treating children considered low risk and not contagious [41].
Attitudes and beliefs were also related to the professional group that healthcare professionals belonged to [29, 61]. Physicians and nurses had opposing views on surgical count protocol violations and what constitutes safe clinical practice [61]. Nurses believed that physicians had lower hand hygiene compliance, while physicians believed that they were role models and leaders of hand hygiene and would warn other staff members [29].
Healthcare professionals’ agreement or disagreement with specific guidelines also led to adaptations of hospital standardization. Adaptations were made when for example radiologists considered diagnostic imaging guidelines not useful, too rigid, or that they failed to include specific information about changes [47] or were perceived as inefficient or unnecessary [75], not relevant for the clinical practice [37, 64], or not relevant for certain care systems [48], or when healthcare professionals doubted the effectiveness of isolation precautions to prevent disease contagion [55]. Similarly, a systematic review reported adaptations when guidelines and other standardized practices were considered too generic, promoted 'cookbook medicine', oversimplified, difficult or controversial treatment decisions, or when the evidence they were based on was conflicting [62]. By contrast healthcare professionals complied to standards, protocols and guidelines when believed to be useful tools [49] in clinical decision making and providing uniform care [48, 62], were easy to understand, highly relevant to clinical practice and patient population, and based on credible information sources [62].
Motivational factors
Motivational factors for healthcare professionals’ adaptive capacity are mainly reported in studies on infection prevention and control. Personal motivational drivers such as moral responsibility, obligation and duty are reported by different professional groups related to infection control practices in the emergency room and on hospital wards in general [26, 33], within tuberculosis infection control measures [22], within hand hygiene obligations [29], within venous thromboembolism prophylaxis management [46], within respiratory infectious diseases [24], and with clinical practice guidelines to prevent falls and injuries [71]. The moral responsibility would be directed towards themselves as professionals to reduce transmission of pathogens or expressed as a duty of care to their patients. Motivational factors were most often internally driven in the sense of professionals’ own intent and feelings of psychological safety [30, 75], while some studies reported on external drivers such as a motivational person in their organization [71], the intensity of activity in the clinical setting [30] or organizational neglect of occupational health and safety [60].
Healthcare professionals’ comfort or discomfort with personal protective equipment would influence their motivation to adapt infection prevention and control standardization practices [24, 33, 41, 51, 53, 56].
Knowledge and experience factors
Knowledge and training of standardization practices was described as important and increased compliance among nurses [34, 42, 43] and younger physicians [55], but was not seen as sufficient for physicians and nurses in other studies [25, 44, 47, 50, 55, 58, 59].
Length and type of clinical experience would often lead healthcare professionals to either adapt hospital standardization [35, 41, 55, 59, 61, 67, 73] or to comply with it [43, 68, 71]. For example, experienced senior nurses had more confidence to adapt protocols in intensive care units [59] or during fever management [73], than less experienced nurses with barcode medication administration technology [68]. Among surgical team members, physicians relied on their experience and tactical knowledge [61], nurses on their repeated experience of working daily with the same instrument trays [59] and disregarded surgical count guidelines or made workarounds on surgical safety checklist use [58]. However, in another study increased length of experience was reported as a contributing factor to compliance with hand hygiene for both physicians and nurses [43].
Insufficient knowledge and training led healthcare professionals to make adaptations. For example, knowledge deficits about tuberculosis led healthcare professionals to use ineffective measures in preventing transmission [33]. Similarly, midwives’ limited knowledge of aspects of infection prevention control guidelines [23] or being unaware that national postnatal care protocols had been updated led them to make adaptations based on inappropriate experiential knowledge [60].
For some healthcare professionals, negative experiences during clinical practice increased their compliance with clinical guidelines [71], while experience of lack of consequences led them to continue their adaptations of universal precautions [55].
Professional role factors
In many cases, the clinical role or profession of healthcare workers influenced their ability and desire to adapt hospital standardization [12, 55, 57, 60, 75]. Nurses defined problem solving as part of their job thus contributing to workarounds from standardization practices [75]. Physicians often defined their role in authoritative ways contributing to lower compliance with hospital standardization than other professions, for example within hand hygiene [12], the surgical safety checklist [57, 60], and MRSA precautions [55]. In one study, professional status and reputation were identified to influence physicians’ clinical decision-making [45]. Healthcare professionals’ perception of their own roles also challenged their possibility to intervene in each other’s work tasks and their ability to collectively adapt standardization practices [45, 57].
Furthermore, autonomy and clinical and/or professional judgment were seen as vital elements of healthcare professionals’ adaptive capacity [39, 59, 62, 75]. For example, commitment to infection prevention and control was high in a neonatal unit, however, severely constrained resources made improvisation a vital element of professionals’ clinical judgment and adaptive capacity [23].
Risk management factors
Healthcare professionals adapted their practices to meet hospital standardization due to individual perceptions of risk and belonging personal costs. They adhered to infection prevention guidelines to protect themselves from being infected or from infecting family and others [24, 27, 29, 33, 41, 53, 56], or they wanted to avoid reprimands and litigations [46, 62, 72] or negative media attention [71]. The perceived risk for reprimands or litigations might for example lead to nurses performing fall prevention according to the guideline “just in case” even with non-risk patients [71] p90. The same goes for physicians sending patients for x-rays “just to be safe” [71] p90. However, in another study perceived enforcement of rules in the form of monitoring and threats of punishment or sanctions had no direct or indirect effect on physicians’ compliance [40].
Clinical practice guidelines were adapted or disregarded if healthcare professionals perceived them to constitute a potential risk to patients [59, 67, 69, 75]. This could involve physicians using more highly concentrated medications than recommended to prevent fatal arrhythmia [69] or nurses to disregard the protocol for surgical count of instruments in life-threatening emergencies [59].
Patient and family factors
The main reason for healthcare professionals wanting to adapt hospital standardization was to meet patient needs. In general, this involved deviations from hospital guidelines or policies when they saw them as barriers to patient care and/or patient safety. Patient needs were exemplified as timely care, patient-centred care, quality of patient communication, privacy, improved outcomes [36, 55, 56, 67, 74, 75] and customized care [62,63,64,65,66,67,68,69]. Several studies related to infection prevention including three during pandemic situations pointed at adaptations made to personal protective equipment protocols to improve patient communication, reduce patients’ feeling of isolation, and better establish therapeutic relationships [22, 52, 54,55,56]. This was especially relevant for older patients [55] and children [41, 56]. In emergencies, workarounds of protocols were justified not to jeopardise the patients’ safety [75], while in surgical settings compliance with the checklist protocol was seen as preserving patient safety [60].
Family factors were related to presence and expectations, and cultural conflicts. Examples of adaptations span from clinicians not complying with the family witnessed resuscitation protocol as they value it as traumatic for relatives with risk of PTSD [72] to pressure for antibiotics and intravenous fluids in diarrheal management [45] to disapproval of pre-operative skin preparation policy due to cultural preferences [76].
Work relationship factors
Most studies reporting on work relationship factors were related to conditions negatively affecting the adaptive capacity of healthcare professionals such as power issues, group norms, hierarchical relationships, and breakdown in communication [21, 23, 31, 41, 57, 59, 61, 65]. This could entail surgeons’ power influencing the practice of the surgical count procedure negatively where nurses felt unable to demand to undertake the count even though it constitutes a crucial safeguard for the outcome of the surgery [59, 61]. Hierarchical relationships were shown to negatively affect the use of the safe surgery checklist as surgeons and anaesthetists would disincline to volunteer information and openly communicate with each other and other team members [57]. Breakdown in communication was identified to negatively influence healthcare professionals’ adaptive capacity within antimicrobial prophylaxis [21], postnatal care protocols [60], and infection outbreaks [55].
A few studies reported on positive effects of work relationship factors such as peer pressure in the forms of healthcare professionals’ reminding each other to wear protective equipment [24], physicians acting as positive role models to other staff members on hand hygiene [29], nurse leaders modelling practicing safety rounds to staff [38] or collegial support from senior medical and nursing staff to junior professionals to improve adherence to standardization practices in the emergency department [70].
Contextual factors influencing healthcare professionals’ adaptive capacity
Based on our synthesis of studies we identified several contextual factors that influenced healthcare professionals’ adaptive capacity with hospital standardization. These were factors “outside” the individual and group/social level. Even though the review did not focus specifically on the organizational or institutional level, the contextual factors formed parts of healthcare professionals’ explanations for degree of adaptation or compliance with hospital standardization.
Guideline “system”
Some studies described characteristics of the guidelines per se to influence how healthcare professionals adapted to them or not [24, 47, 48, 68, 71]. For example, guidelines that were too long and ambiguous or outdated and unclear [24, 47] or complex [64] were considered as barriers as healthcare professionals were confused and unsure how to adhere to them. Moreover, constantly changing guidelines given the time restrictions of daily clinical practice overwhelmed healthcare professionals who could not keep up with the updates or changes [24]. In addition, insufficient guidelines which lacked specific information were seen as a barrier and practical implementation depended on the healthcare professionals’ expertise [48].
However, high usability and guidelines that reflected national or international guidelines facilitated healthcare professionals’ compliance [24, 68].
Cultural norms
Workplace culture was described to influence adaptation or compliance with hospital standardization [24, 33, 41]. For example, adaptations were made when standard precautions were not the routine practice in the clinical department [41], when there was complacency to infection prevention control guidelines [24] or when workplace culture was part of a national culture [33]. When hospital standardization practices were followed by senior colleagues [41] or by all staff the compliance was high [24].
Leadership support
Several studies reported that the level of adaptation or compliance with hospital standardization was influenced by the level of support healthcare professionals received by their clinical leadership [24, 29, 33, 60, 62, 65, 71]. Leadership support was understood as visibility, encouragement, and modeling compliance with standardization practices [24, 29, 38, 65].
Physical environment
Healthcare professionals described various factors in the physical environment that led to adaptations of hospital standardization practices [24, 45, 62, 67, 71]. For example, limited access to treatment services and facilities [62], wards being too crowded, noisy, and dirty [45], lack of adequate ventilation, isolation rooms, and shower facilities to prevent infection transmission [24], narrow hospital bathrooms [71], or lack of vital space in examination cubicles [60].
Time
Time constraints were in several studies described as a reason for adaptations [29, 36, 48, 49, 57, 58]. For example, during emergencies there was no time to either perform proper hand hygiene or proper use of gloves [29], or to perform time-out procedures or safety checklists during surgical operations [57]. However, a systematic review suggested that implementation of the surgical safety checklist reduced time delays as miscommunication and confusion were avoided [60].
Workload issues
Increased workload was mainly reported in studies on infection prevention practices to explain healthcare professionals’ adaptations of hospital standardization [12, 21, 24, 29, 55]. Similarly, in a study on perinatal care obstetricians reported that they were more likely to comply with changes in practice if their workloads did not increase [34]. Staff shortages leading to demanding workloads was also a contributing factor for midwives to collectively decide not to update their knowledge of the new post-natal care protocols, despite training being offered [60].
Discussion
In this paper we have reviewed the literature to identify the factors contributing to healthcare professionals’ adaptive capacity with hospital standardization. We have documented that adaptive capacity is multidimensional according to eight factors: psychological and emotional, cognitive, motivational, knowledge and experience, professional role, risk management, patient and family, and work relationships. This multidimensional aspect is supported by Huey and Palaganas’ [11] emphasizing the influence of individual and workplace cultural factors. Individual traits such as having a higher purpose is in our review specified as motivational, emotional, cognitive, and knowledge-based factors. Our review also adds group/social factors including work relationship, professional role, and physical environment, in line with Toode, Routasalo and Suominen [78]. New in this study is the establishment of the patient and family factor as a main driver for healthcare professionals’ adaptation of hospital standardization.
The eight factors of adaptive capacity are situated within a contextual setting, described by healthcare professionals as the background for their adaptation. Time and workload issues were most frequently described in studies on infection prevention and control and in surgery, with different reasoning. The time issue in infection prevention and control is related to the time-consuming and resource intensive procedures, while in surgery the time issue is related to urgency and acute situations. Both contexts might lead to a need for healthcare professionals having to adapt protocols and guidelines. Individual factors are indisputable engrained in the contextual surroundings meaning that healthcare professionals’ adaptive capacity needs to be understood in light of the guideline system, cultural norms, leadership support, time and workload issues, and the physical environment. This is in line with previous research on the role of context in healthcare [79, 80].
This scoping review covers 26 different countries representing all continents of which 29 studies are from developed countries and 19 from developing countries. We did notice some variation in the extent and type of details reported by healthcare professionals across regions and countries. However, a geographic comparison was not included in our scope and future research comparing continents, regions, or countries based on their economic status and healthcare professionals’ adaptive capacity should be conducted.
In our review infection prevention and control and practices related to hand hygiene and use of personal protective equipment stand out as the most common standardization practices studied. This is an area with clear individual and organizational targets thus requiring a combination of individual and organizational adaptive capacity [81]. Based on our review and previous research we claim that the field of adaptive capacity and resilience would benefit from incorporating knowledge on individual factors to succeed [82,83,84]. Adaptive capacity for healthcare professionals and healthcare organizations seems to depend on each other more than the research has acknowledged so far and should be the topic of future research.
Implications for hospital management and practice
The new knowledge from this review on individual, group/social factors and contextual factors influencing healthcare professionals’ adaptive capacity should be used by hospitals to improve and tailor make current standardization practices. Efforts should be made to construct educational efforts, individualise training and motivational support, and to address the role of patients and families as the main driver for healthcare professionals’ adaptation of hospital standardization.
Based on the findings of this scoping review, complex standardisation practices should be revised to be easily understandable, as short as possible, and relevant to the professional practice. Healthcare professionals should be involved in standardization development and/or revisions to achieve this. Educational efforts to inform healthcare professionals on new or revised standardisation practices should integrate knowledge building not only on the standardisation measure in itself, but also on how individual, group/social, and contextual factors promote or hamper their compliance to or adaptation of it. This is especially important within the areas of infection control and personal protective equipment as the evidence for healthcare professionals’ adaptation is strong.
Strengths and limitations
The review was conducted in accordance with an acknowledged framework for scoping reviews and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. The scoping methodology allowed information from a broad range of studies, using different designs and methods, to be included and synthesized. The findings highlight individual and group/social factors for healthcare professionals to comply with or adapt hospital standardization practices.
The review was limited to English-speaking literature and the included studies were not assessed for quality. The review does not provide a definitive account of the successful outcomes of healthcare professionals’ adaptive capacity towards standardization practices. Moreover, this scoping review focused on individual factors and group/social factors and did not include a full review of organizational factors as this is done in other studies. Finally, it was not possible to draw any conclusions on how pandemics influence healthcare professionals’ adaptive capacity, as only five studies met the inclusion criteria. This should be followed-up with further research.
Conclusions
Our study identified the following hospital standardization practices where healthcare professionals’ adaptive capacity has been studied: clinical guidelines and protocols, precautions, procedures, checklists, policies, forms, and hospital-generic precautions, rules, and regulations. These are typically studied within infection prevention and control, followed by more disease-specific areas such as for example cancer.
There has been lack of knowledge on factors impacting on healthcare professionals’ adaptation or compliance with hospital standardization. This scoping review stands out by identifying a multidimensional set of eight factors at the individual and group/social level. The main factor influencing healthcare professionals’ adaptation of hospital standardization was patient and family needs. The review also identified surrounding contextual factors influencing healthcare professionals’ adaptive capacity including the guideline system, cultural norms, leadership support, physical environment, time, and workload issues.
Future research needs to investigate the relationship between individual factors for adaptive capacity and their contextual setting, as well as the relationship between individual, group/social, and organizational factors.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PRISMA-ScR:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews
- MeSH:
-
Medical Subject Headings
- MRSA:
-
Methicillin-resistant Staphylococcus aureus
- PTSD:
-
Post traumatic stress disorder
References
Arts DL, Voncken AG, Medlock S, Abu-Hanna A, van Weert HC. Reasons for intentional guideline non-adherence: a systematic review. Int J Med Inform. 2016;89:55–62. https://doi.org/10.1016/j.ijmedinf.2016.02.009.
Smaggus A. Safety-I, safety-II and burnout: how complexity science can help clinician wellness. BMJ Qual Saf. 2019;28(8):667. https://doi.org/10.1136/bmjqs-2018-009147.
Ralefala T, Mokokwe L, Jammalamadugu S, Legobere D, Motlhwa WS, Oyekunle AA, et al. Provider Barriers and Facilitators of Breast Cancer Guideline-Concordant Therapy Delivery in Botswana: A Consolidated Framework for Implementation Research Analysis. Oncologist. 2021:26(12). https://doi.org/10.1002/onco.13935.
Pastores S, Kvetan V, Coopersmith C, Farmer JC, Sessler C, Christman J, et al. Workforce, Workload, and Burnout Among Intensivists and Advanced Practice Providers. Crit Care Med. 2019;47(4):550–7.
McCauley L, Kirwan M, Matthews A. The factors contributing to missed care and non-compliance in infection prevention and control practices of nurses: A scoping review. IJNS Advances 2021;3. https://doi.org/10.1016/j.ijnsa.2021.100039.
Atkinson PA, Martin CR, Rankin J. Resilience revisited. J Psychiatr Ment Health Nurs. 2009;16:137–45. https://doi.org/10.1111/j.1365-2850.2008.01341.x.
Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatol. 2014;1(5). https://doi.org/10.3402/ejpt.v5.25338.
Wiig S, Aase K, Billett S, Canfield C, Roise O, Nja O, et al. Defining the boundaries and operational concepts of resilience in the resilience in healthcare research program. BMC Health Serv Res. 2020;20(1):330. https://doi.org/10.1186/s12913-020-05224-3.
Arrogante O, Aparicio-Zaldivar E. Burnout and health among critical care professionals: the mediational role of resilience. Intensive Crit Care Nurs. 2017;42:110–5. https://doi.org/10.1016/j.iccn.2017.04.010.
McCann CM, Beddoe E, McCormick K, Huggard P, Kedge S, Adamson C, et al. Resilience in the health professions: a review of recent literature. International Journal of Wellbeing. 2013;3(1):60–81.
Huey CWT, Palaganas JC. What are the factors affecting resilience in health professionals? a synthesis of systematic reviews. Med Teach. 2020;42(5):550–60. https://doi.org/10.1080/0142159X.2020.1714020.
Erasmus V, Daha TJ, Brug H, Richardus JH, Behrendt MD, Vos MC, et al. Systematic review of studies on compliance with hand hygiene guidelines in hospital care. Infect Control Hosp Epidemiol. 2010;31(3):283–94.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. https://doi.org/10.1080/1364557032000119616.
Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141–6.
Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. https://doi.org/10.1186/s12874-018-0611-x.
Tricco AC, Zarin W, Ghassemi M, Nincic V, Lillie E, Page MJ, et al. Same family, different species: methodological conduct and quality varies according to purpose for five types of knowledge synthesis. J Clin Epidemiol. 2018;96:133–42.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. https://doi.org/10.1186/1748-5908-5-69.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73. https://doi.org/10.7326/M18-0850.
Bramer WM, Rethlefsen ML, Kleijnen J, Franco OH. Optimal database combinations for literature searches in systematic reviews: a prospective exploratory study. Syst Rev. 2017;6(1):245. https://doi.org/10.1186/s13643-017-0644-y.
Daudt H, van Mossel C, Scott S. Enhancing the scoping study methodology: a large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med Res Methodol. 2013;13:48. https://doi.org/10.1186/1471-2288-13-48.
Bonfait H, Delaunay C, de Thomasson E, Charrois O. Near-miss event assessment in orthopedic surgery: Antimicrobial prophylaxis noncompliance. Orthop Traumatol Surg Res. 2010;96(5):493–9. https://doi.org/10.1016/j.otsr.2010.03.014.
Chapman HJ, Veras-Estevez BA, Pomeranz JL, Perez-Then EN, Marcelino B, Lauzardo M. The Role of Powerlessness Among Health Care Workers in Tuberculosis Infection Control. Qual Health Res. 2017;27(14):2116–27. https://doi.org/10.1177/1049732317731317.
Herbec A, Chimhini G, Rosenberg-Pacareu J, Sithole K, Rickli F, Chimhuya S, et al. Barriers and facilitators to infection prevention and control in a neonatal unit in Zimbabwe - a theory-driven qualitative study to inform design of a behaviour change intervention. J Hosp Infect. 2020;106(4):804–11. https://doi.org/10.1016/j.jhin.2020.09.020.
Houghton C, Meskell P, Delaney H, Smalle M, Glenton C, Booth A, et al. Barriers and facilitators to healthcare workers' adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: A rapid qualitative evidence synthesis. Cochrane Database Syst Rev. 2020;4:1–55. https://doi.org/10.1002/14651858.CD013582.
Suliman M, Aloush S, Aljezawi M, AlBashtawy M. Knowledge and practices of isolation precautions among nurses in Jordan. Am J Infect Control. 2018;46(6):680–4. https://doi.org/10.1016/j.ajic.2017.09.023.
Chapman HJ, Veras-Estévez BA, Pomeranz JL, Pérez-Then EN, Marcelino B, Lauzardo M. Perceived Barriers to Adherence to Tuberculosis Infection Control Measures among Health Care Workers in the Dominican Republic. MEDICC Rev. 2017;19(1):16–22. https://doi.org/10.37757/MR2017.V19.N1.4.
Darawad MW, Al-Hussami M, Almhairat, II, Al-Sutari M. Investigating Jordanian nurses' handwashing beliefs, attitudes, and compliance. Am J Infect Control. 2012;40(7):643–7. https://doi.org/10.1016/j.ajic.2011.08.018.
Jenner EA, Fletcher BC, Watson P, Jones FA, Miller L, Scott GM. Discrepancy between self-reported and observed hand hygiene behaviour in healthcare professionals. J Hosp Infect. 2006;63(4):418–22. https://doi.org/10.1016/j.jhin.2006.03.012.
McLaws ML, Farahangiz S, Palenik CJ, Askarian M. Iranian healthcare workers' perspective on hand hygiene: A qualitative study. J Infect Public Health. 2015;8(1):72–9. https://doi.org/10.1016/j.jiph.2014.05.004.
O'Boyle CA, Henly SJ, Larson E. Understanding adherence to hand hygiene recommendations: the theory of planned behavior. Am J Infect Control. 2001 Dec;29(6):352–60. https://doi.org/10.1067/mic.2001.18405.
Shah N, Castro-Sanchez E, Charani E, Drumright LN, Holmes AH. Towards changing healthcare workers’ behaviour: a qualitative study exploring non-compliance through appraisals of infection prevention and control practices. J Hosp Infect. 2015;90(2):126–34.
Wang Y, Yang J, Qiao F, Feng B, Hu F, Xi ZA, et al. Compared hand hygiene compliance among healthcare providers before and after the COVID-19 pandemic: A rapid review and meta-analysis. Am J Infect Control. 2021. 50(5):563–571. https://doi.org/10.1016/j.ajic.2021.11.030.
Woith W, Volchenkov G, Larson J. Barriers and motivators affecting tuberculosis infection control practices of Russian health care workers. Int J Tuberc Lung Dis. 2012;16(8):1092–6. https://doi.org/10.5588/ijtld.10.0779.
Al-Faouri I, Okour SH, Alakour NA, Alrabadi N. Knowledge and compliance with standard precautions among registered nurses: A cross-sectional study. Ann Med Surg. 2021;62:419–24. https://doi.org/10.1016/j.amsu.2021.01.058.
Flynn AV, Sinclair M. Exploring the relationship between nursing protocols and nursing practice in an Irish intensive care unit. Int J Nurs Pract. 2005;11(4):142–9. https://doi.org/10.1111/j.1440-172X.2005.00517.x.
Kakeeto M, Lundmark R, Hasson H, von Thiele Schwarz U. Meeting patient needs trumps adherence. A cross-sectional study of adherence and adaptations when national guidelines are used in practice. J Eval Clin Pract. 2017;23(4):830–8. https://doi.org/10.1111/jep.12726.
Kotzeva A, Guillamon I, Gracia J, del Campo PD, Gich I, Calderon E, et al. Use of clinical practice guidelines and factors related to their uptake: a survey of health professionals in Spain. J Eval Clin Pract. 2014;20(3):216–24.
Meyer P, Hill C, Baker D. Standardizing Nurse Leader Safety Rounds to Promote Highly Reliable Care. J Nurs Care Qual. 2020;35(3):252–7.
Nissinboim N, Naveh E. Process standardization and error reduction: A revisit from a choice approach. Saf Sci. 2018;103:43–50.
Weske U, Boselie P, van Rensen E, Schneider M. Physician compliance with quality and patient safety regulations: The role of perceived enforcement approaches and commitment. Health Serv Manage Res. 2019;32(2):103–12.
Efstathiou G, Papastavrou E, Raftopoulos V, Merkouris A. Factors influencing nurses' compliance with Standard Precautions in order to avoid occupational exposure to microorganisms: a focus group study. BMC Nurs. 2011;10(1). https://doi.org/10.1186/1472-6955-10-1.
Luo Y, He GP, Zhou JW, Luo Y. Factors impacting compliance with standard precautions in nursing, China. Int J Infect Dis. 2010;14(12):E1106–E14. https://doi.org/10.1016/j.ijid.2009.03.037.
Nofal M, Subih M, Al-Kalaldeh M. Factors influencing compliance to the infection control precautions among nurses and physicians in Jordan: A cross-sectional study. J Infect Prev. 2017;18(4):182–8.
Adeniyi B, Ilesanmi O, Obaseki D, Desalu O, Betiku B, Erhabor G. Relationship between knowledge and quality of asthma care among physicians in South-West Nigeria. Niger J Clin Pract. 2017;20(5):566–72.
Biswas D, Hossin R, Rahman M, Bardosh KL, Watt MH, Zion MI, et al. An ethnographic exploration of diarrheal disease management in public hospitals in Bangladesh: From problems to solutions. Soc Sci Med. 2020;260:12. https://doi.org/10.1016/j.socscimed.2020.113185.
Chapman NH, Lazar SP, Fry M, Lassere MN, Chong BH. Clinicians adopting evidence based guidelines: a case study with thromboprophylaxis. BMC Health Serv Res. 2011;11:240. https://doi.org/10.1186/1472-6963-11-240.
Gransjøen AM, Wiig S, Lysdahl KB, Hofmann BM. Barriers and facilitators for guideline adherence in diagnostic imaging: an explorative study of GPs' and radiologists' perspectives. BMC Health Serv Res. 2018;18(1):556. https://doi.org/10.1186/s12913-018-3372-7.
Heutinck L, van Gameren M, Verschuuren J, Geurts ACH, Jansen M, de Groot IJM. Clinical Management of Duchenne Muscular Dystrophy in the Netherlands: Barriers to and Proposals for the Implementation of the International Clinical Practice Guidelines. J NeuromusculDis. 2021;8(4):503–12.
Talarico R, Marinello D, Bombardieri S, Burmester G, Fonseca J, Frank C, et al. Clinical practice guidelines adherence, knowledge and awareness in rare and complex connective tissue diseases across Europe: results from the first ERN ReCONNET survey. RMD Open. 2020;6(2):12.
Halm EA, Atlas SJ, Borowsky LH, Benzer TI, Metlay JP, Chang YC, et al. Understanding physician adherence with a pneumonia practice guideline: effects of patient, system, and physician factors. Arch Intern Med. 2000;160(1):98–104.
Chen FF, Zang YL, Liu Y, Wang XM, Lin XF. Dispatched nurses' experience of wearing full gear personal protective equipment to care for COVID-19 patients in China-A descriptive qualitative study. J Clin Nurs. 2021;30(13-14):2001–14. https://doi.org/10.1111/jocn.15753.
Seitz RM, Yaffee AQ, Peacock E, Moran TP, Pendley A, Rupp JD. Self-Reported Use of Personal Protective Equipment among Emergency Department Nurses, Physicians and Advanced Practice Providers during the 2020 COVID-19 Pandemic. Int J Environ Res Public Health. 2021;18(13):6. https://doi.org/10.3390/ijerph18137076.
Chughtai AA, Seale H, Dung TC, Hayen A, Rahman B, Raina MacIntyre C. Compliance with the Use of Medical and Cloth Masks Among Healthcare Workers in Vietnam. Ann Occup Hyg. 2016;60(5):619–30. https://doi.org/10.1093/annhyg/mew008.
Hu X, Zhang Z, Li N, Liu D, Zhang L, He W, et al. Self-reported use of personal protective equipment among Chinese critical care clinicians during 2009 H1N1 influenza pandemic. PLoS One. 2012;7(9):e44723. https://doi.org/10.1371/journal.pone.0044723.
Moore D, Gamage B, Bryce E, Copes R, Yassi A, BC Interdisciplinary Respiratory Protection Study Group. Protecting health care workers from SARS and other respiratory pathogens: organizational and individual factors that affect adherence to infection control guidelines. Am J Infect Control. 2005;33(2):88–96. https://doi.org/10.1016/j.ajic.2004.11.003.
Seale H LJ, Gallard J, Kaur R, Chughtai AA, Tashani M, et, al. “The cookie monster muffler”: perceptions and behaviours of hospital healthcare workers around the use of masks and respirators in the hospital setting. Int J Infect Control. 2014;11(1). https://doi.org/10.3396/ijic.v11i1.13704.
Braaf S, Manias E, Riley R. The "time-out' procedure: an institutional ethnography of how it is conducted in actual clinical practice. BMJ Qual Saf. 2013;22(8):647–55. https://doi.org/10.1136/bmjqs-2012-001702.
Gillespie BM, Marshall AP, Gardiner T, Lavin J, Withers TK. Impact of workflow on the use of the Surgical Safety Checklist: a qualitative study. ANZ J Surg. 2016;86(11):864–7. https://doi.org/10.1111/ans.13433.
Riley R, Manias E, Polglase A. Governing the surgical count through communication interactions: implications for patient safety. Qual Saf Health Care. 2006;15(5):369–74. https://doi.org/10.1136/qshc.2005.017293.
Wangoo L, Ray RA, Ho YH. Compliance and Surgical Team Perceptions of WHO Surgical Safety Checklist; Systematic Review. Int Surg. 2016;101(1-2):35–49.
Warwick VR, Gillespie BM, McMurray A, Clark-Burg KG. The patient, case, individual and environmental factors that impact on the surgical count process: An integrative review. J Perioper Nurs. 2019;32(3):9–19. https://doi.org/10.26550/2209-1092.1057.
Bierbaum M, Rapport F, Arnolda G, Nic Giolla Easpaig B, Lamprell K, Hutchinson K, et al. Clinicians' attitudes and perceived barriers and facilitators to cancer treatment clinical practice guideline adherence: A systematic review of qualitative and quantitative literature. Implement Sci. 2020;15(1). https://doi.org/10.1186/s13012-020-00991-3.
te Boveldt N, Vernooij-Dassen M, Besse K, Vissers K, Engels Y. Adaptation of an evidence-based clinical practice guideline in cancer pain management by medical oncologists: a case vignette study. Support Care Cancer. 2015;23(5):1409–20. https://doi.org/10.1007/s00520-014-2472-0.
Ismaila N, Salako O, Mutiu J, Adebayo O. Oncology guidelines usage in a low-and middle-income country. J Glob Oncol. 2018;4:1–6.
Belizan M, Meier A, Althabe F, Codazzi A, Colomar M, Buekens P, et al. Facilitators and barriers to adoption of evidence-based perinatal care in Latin American hospitals: a qualitative study. Health Educ Res. 2007;22(6):839–53.
Muhindo M, Bress J, Kalanda R, Armas J, Danziger E, Kamya MR, et al. Implementation of a Newborn Clinical Decision Support Software (NoviGuide) in a Rural District Hospital in Eastern Uganda: Feasibility and Acceptability Study. JMIR Mhealth Uhealth. 2021;9(2):16.
Yevoo LL, Agyepong IA, Gerrits T, van Dijk H. Improvisation and harm avoidance: An ethnographic study of adherence to postnatal care protocols in two hospitals in Southern Ghana. Midwifery. 2020;82:11. https://doi.org/10.1016/j.midw.2019.102576.
Othman EH, Darawad MW. Nurses’ Compliance With Bar-code Medication Administration Technology: Results of Direct Observation of Jordanian Nurses’ Practice. Comput Inform Nurs. 2020;38(5):256–62.
Uema A, Kitamura H, Nakajima K. Adaptive behavior of clinicians in response to an over-constrained patient safety policy on the administration of concentrated potassium chloride solutions. Saf Sci. 2020;121:529–41. https://doi.org/10.1016/j.ssci.2019.09.023.
McEwan H, Baker R, Armstrong N, Banerjee J. A qualitative study of the determinants of adherence to NICE falls guideline in managing older fallers attending an emergency department. Int J Emerg Med. 2018;11(1):33 https://doi.org/10.1186/s12245-018-0192-9.
Stenberg M, Wann-Hansson C. Health care professionals' attitudes and compliance to clinical practice guidelines to prevent falls and fall injuries. Worldviews Evid Based Nurs. 2011;8(2):87–95. https://doi.org/10.1111/j.1741-6787.2010.00196.x.
Johnson C. A literature review examining the barriers to the implementation of family witnessed resuscitation in the Emergency Department. Int Emerg Nurs. 2017;30:31-5. https://doi.org/10.1016/j.ienj.2016.11.001.
Thompson HJ, Kagan SH. Clinical management of fever by nurses: doing what works. J Adv Nurs. 2011;67(2):359–70. https://doi.org/10.1111/j.1365-2648.2010.05506.x.
Toxopeus DCM, Pell CL, Westrhenen NB-v, Smit C, Wit FWNM, Ondoa P, et al. Compliance with laboratory monitoring guidelines in outpatient HIV care: a qualitative study in the Netherlands. AIDS Care. 2019;31(7):840–7. https://doi.org/10.1080/09540121.2018.1563280.
Debono DS, Greenfield D, Travaglia JF, Long JC, Black D, Johnsonet J. et al. Nurses' workarounds in acute healthcare settings: a scoping review. BMC Health Serv Res. 2013;13(175). https://doi.org/10.1186/1472-6963-13-175.
Yami AAM. Using the Theory of Planned Behaviour to explore the intentions of a multicultural nursing workforce to comply with policies and procedures in the Prince Sultan Military Medical City (PSMMC) [Doctoral Thesis]: University of Southampton Institutional Repository; 2015. Available from: http://eprints.soton.ac.uk/id/eprint/381574.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097.
Toode K, Routasalo P, Suominen T. Work motivation of nurses: A literature review. Int J Nurs Stud. 2011;48(2):246–57. https://doi.org/10.1016/j.ijnurstu.2010.09.013.
Coles E, Anderson J, Maxwell M, Harris FM, Gray NM, Milner G, et al. The influence of contextual factors on healthcare quality improvement initiatives: a realist review. Syst Rev. 2020;9(1):94. https://doi.org/10.1186/s13643-020-01344-3.
Lyng HB, Macrae C, Guise V, Haraldseid-Driftland C, Fagerdal B, Schibevaag L, et al. Exploring the nature of adaptive capacity for resilience in healthcare across different healthcare contexts; a metasynthesis of narratives. Appl Ergon. 2022;104:103810. https://doi.org/10.1016/j.apergo.2022.103810.
Wiig S, O'Hara JK. Resilient and responsive healthcare services and systems: challenges and opportunities in a changing world. BMC Health Serv Res. 2021;21(1):1037. https://doi.org/10.1186/s12913-021-07087-8.
Iflaifel M, Lim RH, Ryan K, Crowley C. Resilient Health Care: a systematic review of conceptualisations, study methods and factors that develop resilience. BMC Health Serv Res. 2020;20(1):324. https://doi.org/10.1186/s12913-020-05208-3.
Berg SH, Akerjordet K, Ekstedt M, Aase K. Methodological strategies in resilient health care studies: An integrative review. Saf Sci. 2018;110:300–12. https://doi.org/10.1016/j.ssci.2018.08.025.
Ellis LA, Churruca K, Clay-Williams R, Pomare C, Austin EE, Long JC, et al. Patterns of resilience: A scoping review and bibliometric analysis of resilient health care. Saf Sci. 2019;118:241–57. https://doi.org/10.1016/j.ssci.2019.04.044.
Acknowledgements
We would like to thank Eline Ree and Adriana Rosenberg of the Centre for Resilience in Healthcare (SHARE) at the University of Stavanger for their contributions and feedback in this scoping review.
Funding
This research was funded by the Centre for Resilience in Healthcare (SHARE) at the University of Stavanger. The funder has played no role in the design and completion of the study.
Author information
Authors and Affiliations
Contributions
FTK: study inception and study design, database searches and title screening. KA & FTK: abstract and full text screening, data extraction, data charting, thematic analysis, synthesis, and description of results. FTK, KA, SW agreed on study design, search strategy, data extraction, thematic analysis, synthesis, and description of the results. All three authors contributed, edited, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The author SW is a member of the editorial board (Associate Editor and Guest
Editor of this special collection). SW had no role in the peer review or in the handling of this manuscript. The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist.
Additional file 2.
Inclusion Exclusion criteria.
Additional file 3.
Table of all studies included in the review.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tsandila-Kalakou, F., Wiig, S. & Aase, K. Factors contributing to healthcare professionals’ adaptive capacity with hospital standardization: a scoping review. BMC Health Serv Res 23, 799 (2023). https://doi.org/10.1186/s12913-023-09698-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09698-9