
Abstract
Background
High burden of healthcare expenditure precludes the poor from access to quality healthcare services. In Ethiopia, a significant proportion of the population has faced financial catastrophe associated with the costs of healthcare services. The Ethiopian Government aims to achieve universal health coverage (UHC) by 2030; however, the Ethiopian health system is struggling with low healthcare funding and high out-of-pocket (OOP) expenditure despite the implementation of several reforms in health care financing (HCF). This review aims to map the contributions, successes and challenges of HCF initiatives in Ethiopia.
Methods
We searched literature in three databases: PubMed, Scopus, and Web of science. Search terms were identified in broader three themes: health care financing, UHC and Ethiopia. We synthesised the findings using the health care financing framework: revenue generation, risk pooling and strategic purchasing.
Results
A total of 52 articles were included in the final review. Generating an additional income for health facilities, promoting cost-sharing, risk-sharing/ social solidarity for the non-predicted illness, providing special assistance mechanisms for those who cannot afford to pay, and purchasing healthcare services were the successes of Ethiopia’s health financing. Ethiopia's HCF initiatives have significant contributions to healthcare infrastructures, medical supplies, diagnostic capacity, drugs, financial-risk protection, and healthcare services. However, poor access to equitable quality healthcare services was associated with low healthcare funding and high OOP payments.
Conclusion
Ethiopia's health financing initiatives have various successes and contributions to revenue generation, risk pooling, and purchasing healthcare services towards UHC. Standardisation of benefit packages, ensuring beneficiaries equal access to care and introducing an accreditation system to maintain quality of care help to manage service disparities. A unified health insurance system that providing the same benefit packages for all, is the most efficient way to attain equitable access to health care.
Similar content being viewed by others


Background
High-performance health financing (HPHF) for universal health coverage (UHC) is adequate and sustainable funding with sufficient risk pooling to spread the financial risk of ill-health to assure the desired levels of service coverage [1]. The strategies designed to increase the share of total health spending for all nations that have made substantial progress towards UHC predominantly rely on compulsory funding sources [2, 3]. Compulsion and subsidisation in health financing are guiding principles for health financing policy to speed up the path toward UHC [4]. Despite increasing the overall share of spending from compulsory sources being important for the progress towards UHC, the ways of pooling arrangements for the prepaid fund matter [5]. A given level of funding organised into fewer pools has more redistributive capacity than the same level of funding organised into more pools [4, 5]. Even though the UHC goals and intermediate objectives are broadly shared, each country's starting point and context for health financing are unique [4]. There was no single best health financing model for UHC for all countries. Thus, the best option for a country in a given circumstance may not be relevant for another country [4].
Universal health coverage provides equitable and quality promotive, preventive, curative, rehabilitative and palliative health services to all people without financial hardship [6,7,8]. In 2015, the Ethiopian Government was introduced a 20-year plan to achieve UHC [9]. The three pillars of the current health policy of Ethiopia targeted for UHC include the development of an equitable and acceptable standard of health service, assurance of accessibility of health care for all, and provision of health care for the people on a scheme of payment with special assistance mechanisms [10, 11]. Line-item budget, per capita (capitation), and fee-for-services are among Ethiopia's common payment methods for health care services [12]. Community-based health insurance (CBHI) and social health insurance (SHI) are also alternatives to user fees to access equitable healthcare without financial hardship [13]. Both CBHI and SHI provide free-to-access care in public health facilities, reimbursed through a fee-for-service system. However, in Ethiopia, SHI is not implemented concerning the civil servant’s resistance to paying 3% of their salary [14]. Primary healthcare services have also been delivered free of charge or exempted to all service users irrespective of their income level in Ethiopia [15].
Multiple sources finance Ethiopia’s healthcare sector, including loans and donations from all over the world (46.8%), the Ethiopian Government (16.5%), out-of-pocket (OOP) payments (35.8%), and others (0.9%) [16]. The proportion of health financing from domestic sources (excluding the contribution from donors) has increased from 53% of United States dollars (US$) 1.3 billion in 2008 to 78% of US$ 2.7 billion in 2017 [17]. The country’s total health expenditure also rose to nearly Ethiopia Birr (ETB) 50 billion (over US$2.5 billion) in 2013/14 from ETB 1.45 billion (US$230 million) in 1995/96. The per capita health expenditure reached (US$28.65) in 2013/14 from a mere (US$4.5) in 1995/ 96 [18]. But the amount is still meagre compared with the World Health Organization (WHO) recommendation of US$60 per capita spending for delivery of essential health services by 2015 [19]. Ethiopia's health spending constituted 5.6% of the gross domestic product (GDP) in the last decade [18, 20]. For example, the total annual budget of 2019/20 allocated to health was only 5.3% [21], which was less than the average 7% of WHO estimation for low-income countries (LICs) [22].
Despite various HCF reforms in Ethiopia, the country's healthcare system has suffered from low healthcare funding and high OOP payments [17, 23]. However, comprehensive HCF evidence is still lacking that can have implications for achieving UHC and designing strategies to address the gaps in health financing in Ethiopia. Therefore, this review aims to explore the successes, contributions and challenges of HCF toward UHC in Ethiopia.
Methods
Ethiopia’s healthcare delivery system
Ethiopia’s health service is structured into a three-tier system: primary, secondary and tertiary levels of care. A primary health care unit (PHCU) comprises four health centers (HCs), five health posts within each health center, and a primary hospital. Each health post is responsible for a population of 3,000–5,000 people. A health center provides both preventive and curative services. In addition to what an HC can provide, a primary hospital provides emergency surgical services, including caesarean section and gives access to blood transfusion services. Secondary level of care consists of general hospitals. In addition, it serves as a referral center for primary hospitals. Finally, the tertiary level of care comprises federally-run, specialised hospitals and university hospitals [11, 16] (Fig. 1).

Health care system of Ethiopia
Design
A structured narrative review was conducted by reviewing studies published between January 1998 and August 2021 using the three inter-linked HCF framework components.
Search strategy
Electronic databases such as PubMed, Scopus and Web of Science were used to search all published articles. In addition, hand search engines, such as Google search engine and Google Scholar, were also used to search for additional literature on 08 August 2021. The search terms were identified under three themes: healthcare financing, universal health coverage, and Ethiopia. The search strategies were built based on using the “Medical Subject Headings (MeSH)” and “All field” by linking “AND” and “OR” Boolean operator terms as appropriate (Supplementary file 1). In addition, we used the enhancing transparency in reporting the synthesis of qualitative research (ENTREQ) checklist for reporting the findings [24].
Inclusion and exclusion criteria
All retrieved studies were initially imported into the Endnote library to remove the duplicates. After removing the duplicates, we screened the articles by title and abstract based on the eligibility criteria. A quality assessment was done for all eligible retrieved articles by the three independent reviewers using the Joanna Briggs Institute’s (JBI) critical appraisal checklist for qualitative research. Later we discussed in the team, and the last author verified the list of studies. We retained the full texts of all relevant studies found to meet the inclusion criteria for the final synthesis (Table 1).
Data extraction and synthesis
We used Microsoft excel spreadsheet format for data extraction. The excel sheet contained the first author's name, year of publication, title, type of article, and its primary outcomes. In addition, we conducted a double check-up and verification of the extracted information. In this review, we assessed the application of HCF to attain UHC, which includes the provision of equitable and quality health services without financial risk. We used framework analysis to synthesise our extracted data using the three inter-linked HCF framework components: revenue generation, risk pooling/ sharing, and strategic purchasing of services [8, 25]. Explanations of the three inter-linked HCF functions were also presented (Table 2).
Results
Description of the reviewed articles
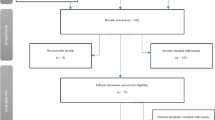
Total of 52 articles (32 quantitative, five qualitative, seven mixed, seven project briefs reports, and 1 policy brief) were eligible for final review (Fig. 2). In addition, we included seven articles in Oromia, 13 in Amhara, six in SNNP, seven in Addis Ababa and the remaining in other regions of Ethiopia.

ENTREQ flow diagram to select articles for HCF towards UHC, 2021
Successes, contributions and challenges of HCF in Ethiopia
We extracted data from all eligible articles related to the contributions and challenges of HCF towards UHC in Ethiopia. We mapped the key successes, contributions and challenges of the eight HCF reforms/initiatives under the three inter-linked HCF framework components. The successes, contributions and challenges of each HCF function towards UHC are indicated (Table 3).
Revenue generation
Of the reviewed articles, 16 described their findings on revenue generations. Various successes were reported in revenue generation/ resource mobilisation. Health facility retained revenue is an additive to the public health facility budgets with major sources including: sale of drugs, medical supplies, consultation fees, non-medical services [26]. Private wing at hospitals also offers additional income for health facilities [27]. Health insurance is another option to mobilise financial resources, increasing the revenue generation of the health institutions [33,34,35].
Health financing strategies in Ethiopia also contribute to revenue generation. Private wings at hospitals generate additional income for health facilities [28,29,30] to provide healthcare services. Health insurance is also another option to generate sustainable resources for health sectors [11, 36]. Health facility governance boards facilitate the linkage of the community to increase resource mobilisation for facilities to solve problems locally [39].
Limited capacity in knowledge and skills of health facility governance related to lack of training and monitoring at federal, regional and woreda levels for planning, difficulty in interpreting the guideline, implementing, and monitoring the HCF [11, 26] were the challenges for revenue generation and utilisation. Low client satisfaction associated with their expectations and high payments were also challenges during private wing implementation [31, 32]. Poor community awareness and costs of premium collection for CBHI concerning the scattered settlement of agricultural households and mobility of the pastoralists were the challenges in revenue collection [11, 13, 37]. Low enrolment rates, high dropouts and weak premium collection for the scheme were additional barriers for CBHI at the community level [11, 38].
Risk pooling/ sharing
In this review, 24 articles reported their findings on risk pooling/ sharing in healthcare services. Health financing initiatives in Ethiopia have various successes in risk pooling. User-fee-setting and revision promote cost-sharing between the Government and users, considering the community’s willingness, ability to pay and cost of services [27]. Health insurance helps the population with special assistance mechanisms for those who can not afford to pay [11]. Health insurance can also help risk pooling/ sharing and social solidarity for the non-predicted illness [40, 41].
Health financing strategies in Ethiopia also contributes to risk pooling. Fee-setting and revision contribute to setting affordable fees and some subsidy by the Government to enhance healthcare access [11]. Health insurance can contribute to financial risk protection for the users [11, 36]. Community-based health-insurance particularly contributes to protecting rural dwellers from facing financial hardship to ensure UHC for all [42,43,44]. It reduces out-of-pocket expenditure (OOP) for healthcare services, reducing catastrophic health expenditure [33,34,35]. Health insurance can also establish financial protection equitably and sustainably for all citizens to enhance healthcare access and achieve UHC by reducing OOP expenditure for healthcare services [14, 29, 45].
Variations in regional laws and discrepancies in adherence to regional legislation in terms of mandating the user fee revisions and settings were the challenges to maintaining the consistency of HCF in Ethiopia. For instance, the mandate of user fee revisions and settings in Amhara and Oromia gave to the regional council, while SNNP allowed health facilities to introduce user fee revisions [11, 26, 27]. Moreover, the provincial law gave the mandate of user fee revision to the provincial (regional) council in the Amhara region, but some health facilities revised user fees on their own [27]. The adverse selection associated with voluntary based CBHI, inability to afford the premium, inadequate benefit packages; preference for OOP payment, and considering only family size without their level of income for premium load [46,47,48] were the challenges during CBHI implementation. The constraints of implementing SHI are the high burden of payroll contributions to SHI, long bureaucracy in reimbursement, under-coverage of the poor, low contract renewal rate and expected returns [13, 51, 52]. Unclear benefit packages, high cost of living and the burden of other deductions from salary were the obstacles to initiating SHI [49, 50]. Free health care services for healthcare providers and frustration of illness associated with high SHI contribution [49, 53] could be the challenges to introducing SHI.
Purchasing of healthcare services
Forty articles from the reviewed articles described the strategic purchasing of healthcare services. Health financing initiatives in Ethiopia have various successes in purchasing healthcare services. Revenue retention can increase resource availability for service provision by using retained revenue to procure drugs and medical supplies and implement oversight [11, 27]. Fee waiver system provides free of charge to the poorest segments of the population to access the full range of health services [29]. Public hospitals' private wings offer more services to the service users [27]. Outsourcing non-clinical services at public hospitals encourages hospitals to outsource non-clinical services, such as laundry, security, and catering, by contracting with local vendors that improve the hospital’s efficiency and reduce the hospital management burden [29]. A clear action plan for healthcare delivery and the introduction of accountable and transparent regulatory frameworks facilitate HCF implementation [26, 73].
Health facility revenue retention could improve infrastructures, diagnostic capacity, procure medical equipment, supplies, medical supplies, drugs, information systems, management procedures, water supply, electricity, and training to enhance quality of healthcare services [11, 27, 54]. It assisted in availing essential medicines; reduce stock-outs of essential drugs; improve health facilities' diagnostic capacity, maintaining continual quality of care; improving water supply, electricity to health facilities; and health infrastructures [27, 54]. Exempted healthcare also helped to deliver the package of services free of charge to all citizens for certain critical public health services to enhance coverage and equity [29]. These services include TB and leprosy diagnosis and treatment; antenatal care; delivery, postnatal care, family planning, leprosy, HIV care, treatment for malaria, immunisation services; HIV/ AIDS diagnosis, care and support, and epidemics [11, 60]. In addition, outsourcing non-clinical services at public hospitals assisted to improve hospitals’ efficiency, reduce internal administrative burden, control costs, enable health facilities to focus on core clinical services, and increase effectiveness and quality of services [27, 29, 63].
Access to healthcare services free health care for poor households through fee waiver systems increases financial protection and ensures UHC for all [27, 43]. Fee waiver systems increase healthcare service utilisation and reduce inequalities in accessing healthcare services for the poor [29, 55]. Private wing at hospitals can raise the motivation of medical professionals, staffs’ sense of hospitals ownership and a decline the turnover rate could help offer more choices and quality of care [27,28,29,30]. Health insurance is reduced inequitable healthcare services for all citizens and improves healthcare delivery [11, 29, 36] and facilitates the path toward UHC [14, 45]. Community-based health insurance also contributes to avail essential drugs, good quality of care and treatment of choice to the users [64, 65]. Health facility governance autonomy is instrumental in increasing facility performance, fair resource allocation and quality of healthcare services to achieve better health outcomes [39, 74]. Community-based health insurance could enhance access to healthcare services and quality of life [40, 41, 66]. It also guaranteed access to equitable quality healthcare services among dwellers of the informal and rural areas [33,34,35, 42].
High non-medical costs, including transportation, lodging, food, and opportunity costs, were the barriers for the poor to access healthcare [56]. Lack of consistency and common understanding of selection criteria, poor training on procedures, low coverage of the poor, inclusion of those able to pay, delay or non-reimbursement of the costs to health facilities, and corruption [11, 57, 58] were also the challenges during fee waiver implementation. Non-consideration of the household's income in proportion to the family size and their expenses for basic needs in the fee waiver guideline were the challenge to select the eligible households [57, 58]. For instance, the guideline excluded households with seven members and got ETB 400 per month. On the other hand, households with four members who earned ETB 300 per month were eligible regardless of the income generated by the family members [57]. The absence of a clear income level cut-off for granting fee waivers; renewal of the waiver card without revision of economic status; healthcare disparity between fee waivers and cash payers; and non-consideration of households with chronic disease within the family were the other barriers to protect the poor from financial hardship [58, 59]. In addition, restriction of fee waiver certification only in a single health facility precludes services for the poor [56]. Shortage of drugs and medical supplies, absence of clear guidance, incurred additional costs, inadequate support, charging for health delivery-related services and supplies by health facilities were also challenges in exempted health services [27].
Lack of understanding of the working procedures and fear of accountability led to health facilities being reluctant to use the retained revenues and demonstrated a loss of efficiency in the healthcare service delivery [11]. The absence of rewarding systems for staff based on performance, poor physical and healthcare infrastructures, provider behaviours, high expectations, and low awareness about alternative options of the private wing at the hospital were the challenges to its utilisation [28, 61, 62]. During its implementation, conflicts between hospitals and service providers regarding the quality of non-clinical services and poor contract specifications were common challenges [63]. Service disparity, low-quality health services, inadequate equipment and staff, lack of trained personnel, adverse selection, moral hazard, fraud, and corruption were the barriers affecting health insurance delivery [13]. Exclusion of family members above 18 years from insurance beneficiaries [49] and health facilities unable to fulfil the criteria to provide the insurance service [67] also challenged healthcare delivery. Demands extraordinary drugs; tend to collect more drugs, and give their card to non-insured patients from the client side while overestimating the cost of services. The charge of undelivered insurance services from service providers' perspective were frequently occurred moral hazards to deliver healthcare services by CBHI [68]. Low awareness and benefit packages, poor perception of quality of health services, and lack of trust of the management [69,70,71,72] were the challenges to enrol CBHI membership. High turnover of board members, absenteeism, inappropriate delegation, lack of capacity, and confusion about the governing body's role hampered leadership and community ownership [11, 26, 27].
Discussion
We explored the successes, contributions, and challenges towards UHC concerning revenue generation, risk pooling/ sharing, and strategic purchasing. Successes of healthcare financing initiatives in Ethiopia include generating an additional income for health facilities, promoting cost sharing between Government and users, risk-sharing for the non-predicted illness, providing special assistance mechanisms for those who can not afford to pay, and purchasing healthcare services [11, 26, 27]. Ethiopia's healthcare financing initiatives have made significant contributions to healthcare infrastructures, medical supplies, diagnostic capacity, drugs, financial risk protection, and healthcare services [27, 29, 55]. On the contrary, poor access to equitable quality healthcare services was the major challenges associated with low healthcare funding and high OOP payments in Ethiopia [17, 23, 75, 76]. Adverse selection, moral hazard, low enrolment in CBHI, poor awareness, lack of consistency and fairness in the implementation of HCF initiatives [11, 13, 38, 48] were also identified as the challenges to access healthcare services and disparity. Furthermore, high non-medical costs, including transportation, lodging, food, and opportunity costs, were barriers to fee waivers and exempted service users from receiving health services [27, 56].
In Ethiopia, health insurance is one of the options/ mechanisms for risk pooling and social solidarity to access healthcare for non-predicted illnesses [40, 41]. Nevertheless, low healthcare funding and high OOP payments [17, 23] were Ethiopia's barriers to health financing. In South Africa, the low risk-pooling and social solidarity could be alleviated by reducing fragments of funding sources and directing all possible sources to a centralised well-managed pool [77]. Centralisation in funding sources is essential and critical to providing equity and improving HCF where a single purchaser of health services [78]. Cross-subsidisation is achieved through integrated funding pools because managing separate funds for different groups limited the benefits of cross-subsidies, and it became difficult to merge fragmented pools [77]. A pre-payment scheme, such as SHI funds for formal sectors and direct taxation with the incremental progressive source of HCF, was essential to reduce the burden of OOP payments [79]. Centralisation in funding sources could make Thailand exemplary progress toward UHC with Government subsidisation for the poor [80]. A pro-poor shift of subsidisation is essential where a more progressive HCF mechanism enables equitable health financing and is vital to develop an HCF mechanism to realise UHC [81].
Multiple sources finance Ethiopia’s healthcare sector, including loans and donations, OOP payments (households), and others [16, 82]. But the healthcare expenditure of Ethiopia is among the least compared with the estimated WHO average of LICs (7%) [22] and the Abuja agreement (15%) [83]. This low health care revenue in the country could be associated with low government budgets, corruption, low enrolment and a high dropout rate from CBHI membership [11, 13, 21, 38]. In Malawi, the Debt relief strategy substantially contributes to the country’s steady progress towards the Abuja target [84], making Malawi’s share of GDP to the health sector. It makes Malawi’s share of GDP in the health sector higher than other LICs [85]. In Ghana, refining the premium of the national health insurance (NHI), gradual increment of funds to the health sector, and multi-sectoral advocacy to increase revenues by the Government had a significant impact on the country’s health revenue generation [86]. Thailand has also set a successful, equitable and feasible HCF tax procedure for most of its population [87]. The general tax method was the most progressive source of finance for healthcare. It utilises the finance ministry's existing resources, expertise, and mechanisms to enforce and collect the tax payments in Thailand [79]. The tax financing mechanism was a popular and proven healthcare financing and instrumental in achieving UHC in countries with low tax. Progressive tax practices and a pro-poor tax framework for capital gains and profits might support achieving global health objectives [88].
Healthcare service disparity, adverse selection, low-quality health services, moral hazard, fraud and corruption were the challenges in CBHI implementation in Ethiopia [13]. A study conducted in Southeast Asia and the People’s Republic of China showed that service inequality could be narrowed by applying a -payer health insurance system with a unified benefit package to provide more equitable healthcare services [89]. Client-side moral hazard could also be reduced through a cost-sharing mechanism, such as the co-payment approach, which diminishes non-urgent healthcare visits [90, 91]. Mandatory CBHI was pivotal in setting Rwanda toward UHC and making the country with the highest enrolment in health insurance in sub-Saharan Africa (SSA) [92]. A study conducted in Ethiopia also recommended that a mandatory CBHI approach was essential to address the challenges of adverse selection associated with voluntary participation [47]. Standardisation of benefit packages, ensuring equal access to care, and introducing an accreditation system to ensure the quality of care was also helpful in managing service disparities [93]. High non-medical costs, including transportation, lodging, food, and opportunity costs, were the deterrents for fee waivers and exempted service users to access healthcare services [27, 56]. This high non-medical cost precludes the poor from healthcare service utilisation. In LICs, studies recommended that the poor be waived for user fees and reimbursed, particularly for fee waivers for their access costs to health care, including transportation, lodging, food, and opportunity costs [94, 95] solve the accompanying financial catastrophic shock.
Policy implications
The policy implications for this review focused on the contribution and challenges of the HCF reforms for future improvement in the country. Appropriate health financing strategies that safeguard financial risk protection underpin sustainable health services and attain UHC. This review also has an implication to provide more equitable clinical healthcare services or ensure equal access to healthcare in general. This finding will also help to ensure the quality of care and address the clinical healthcare service disparities in Ethiopia. It advances awareness among health programmers and policymakers about the importance of HCF as a key building block of the health system. It also provides an insight on the critical HCF reforms in Ethiopia, include: revenue retention and utilisation, a fee-waiver system for the poor, exemption services, user fee setting and revision, private wing in public hospitals, outsourcing non-clinical services, health insurance, and promoting health facility governance autonomy to improve its implementation on the health system. The review could help the policymakers and government officials to revise and update its HCF strategies.
Strengths and limitations
This review provides ample evidence on HCF towards UHC in Ethiopia. On the contrary, this review did not include a meta-analysis to estimate the pooled effect of HCF on the progress of healthcare service delivery towards UHC in Ethiopia since a meta-analysis to be valid requires all included studies to be sufficiently similar. However, a narrative review can cover a wide range of subject matter at various levels of completeness and comprehensiveness that may consist of research findings.
Conclusion
The healthcare financing initiatives in Ethiopia have had various successes, including generating additional income for health facilities and promoting cost-sharing between Government and users. Risk-sharing/ social solidarity for the non-predicted illness, providing special assistance mechanisms for those who can not afford to pay, and purchasing healthcare services were also the successes of Ethiopia’s health financing. Ethiopia's health financing has significant contributions to healthcare infrastructures, medical supplies, diagnostic capacity, drugs, financial risk protection, and healthcare services. However, poor access to equitable and quality healthcare services was associated with low healthcare funding and high OOP payments in Ethiopia. Health service disparity, adverse selection, moral hazard, low enrollment in CBHI, poor awareness, fraud and corruption were also barriers to health service delivery. The restriction of fee waiver certificates to a single health facility shall be revised to keep the country's referral loop to facilitate UHC progress. Mobilising domestic and external resources, aligning donor funding into the government system, and evidence-based allocation of available resources are essential to advance HCF systems. Standardising benefit packages, ensuring equal access to care, and introducing an accreditation system to maintain quality of care are also helpful in managing service disparities. Therefore, a robust health care financing system is required to speed up the path towards UHC.
Availability of data and materials
Not applicable.
Abbreviations
- ENTREQ:
-
Enhancing Transparency in Reporting the Synthesis of Qualitative research
- HCF:
-
Health Care Financing
- JBI:
-
Joana Brig's Institute
- NGOs:
-
Non-Governmental Organisations
- UHC:
-
Universal Health Coverage
- SDGs:
-
Sustainable Development Goals
- WHO:
-
World Health Organization
References
Group WB. High-performance health financing for universal health coverage: driving sustainable, inclusive growth in the 21st century. Washington (DC): World Bank; 2019.
Acharya A, Vellakkal S, Taylor F, Masset E, Satija A, Burke M, Ebrahim S. The impact of health insurance schemes for the informal sector in low-and middle-income countries: a systematic review. World Bank Res Observer. 2013;28(2):236–66.
Fuchs VR. What every philosopher should know about health economics. Proc Am Philos Soc. 1996;140(2):186–96.
Kutzin J, Yip W, Cashin C. Alternative financing strategies for universal health coverage. In: World Scientific Handbook of Global Health Economics and Public Policy: Volume 1: The Economics of Health and Health Systems. edn.: World Scientific; 2016: 267–309. https://www.worldscientific.com/doi/pdf/10.1142/9789813140493_0005. Accessed 16 Mar 2019.
Fragmentation in pooling arrangements. Technical Brief Series - Brief No 5. Available at: https://www.who.int/healthsystems/topics/financing/healthreport/FragmentationTBNo5.pdf?ua=1. Accessed 29 Nov 2019.
World Health Organization. Health in 2015: from MDGs, millennium development goals to SDGs, sustainable development goals. 2015.
World Health Organization. SDGs and progress towards universal health coverage. In.: World Health Organization. Regional Office for South-East Asia; 2017. https://apps.who.int/iris/handle/10665/258544. Accessed 18 July 2017.
World Health Organization. The world health report: health systems financing: the path to universal coverage: executive summary. In.: World Health Organization; 2010.
Habtemariam MK, Semegn ST. Setting health sector priorities: a brief overview of Ethiopia’s experience. Cost Effectiveness and Resource Allocation. 2018;16(1):1–3.
Health policy of the transitional Government of Ethiopia. Addis Ababa: Federal Democratic Republic of Ethiopia; 1993. Available from: https://www.cmpethiopia.org/media/health_policy_of_ethiopia_1993. Accessed Sept 1993.
Alebachew A, Yusuf Y, Mann C, Berman P. Ethiopia’s Progress in health financing and the contribution of the 1998 health care and financing strategy in Ethiopia. MA, Addis Ababa: Harvard TH Chan School of Public Health and Breakthrough International Consultancy, PLC; 2015.
Langenbrunner J, Cashin C, O'Dougherty S. Designing and implementing health care provider payment systems: how-to manuals: Washington, DC: World Bank Publications; 2009.
Dibaba A, Hadis M, Ababor S, Assefa Y. Improving health care financing in Ethiopia (SURE policy brief). Addis Ababa: Ethiopian Public Health Institute; 2014.
Lavers T. Towards Universal Health Coverage in Ethiopia’s ‘developmental state’? The political drivers of health insurance. Soc Sci Med. 2019;228:60–7.
Alebachew A, Mitiku W. Financing Exempted Health Services in Ethiopia: Analysis of Potential Policy Options. 2019.
WHO. Primary Health Care Systems (PRIMASYS)-Case Study from Ethiopia, 2017. 2020.
Ethiopia health accounts, 2013/14. Addis Ababa: Federal Ministry of Health; 2017. Available from: https://www.hfgproject.org/ethiopia-health-accounts-201314/. Accessed Aug 2017.
Ethiopia’s Health Financing Outlook: What Six Rounds of Health Accounts Tell Us. Available at: https://www.hfgproject.org/ethiopias-health-financing-outlook-what-six-rounds-of-health-accounts-tell-us/. Accessed June 2018.
Jowett M, Brunal MP, Flores G, Cylus J. Spending targets for health: no magic number. In.: World Health Organization; 2016.
Ethiopia's Fifth National Health Accounts, 2010/11. https://www.hfgproject.org.uploads2014/04.pdf. Accessed Apr 2014.
Analysis of the 2019/20 Federal Budget Proclamation. Available at: https://www.unicef.org/ethiopia/reports/analysis-201920-federal-budget-proclamation. Accessed Nov 2019.
World Health Organization. New perspectives on global health spending for universal health coverage. In.: World Health Organization; 2017.
Ali EE. Health care financing in Ethiopia: implications on access to essential medicines. Value in health regional issues. 2014;4:37–40.
Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012;12(1):1–8.
Thinking about equity in health financing: a framework. Available at: http://pubdocs.worldbank.org/en/870381524235352323/Health-financing-and-equity-framework-FINAL-20180417-1750.pdf. Accessed 17 Apr 2018.
Health Care Finance Reform End-line Survey Synthesis Report. Available at: https://publications.jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=13211&lid=3. Accessed Sept 2008.
Zelelew H. Health care financing reform in Ethiopia: improving quality and equity. Health Systems. 2014;20:20.
The role of private wing set up in public hospitals in reducing medical professionals’ turnover. Avaiable at: https://internationaljournalofresearch.com/2016/11/17/the-role-of-private-wing-set-up-in-public-hospitals-in-reducing-medical-professionals-turnover/. Accessed 18 Oct 2018.
Ethiopia Health Sector Financing Reform/HFG: End-of-Project Report. Available at: https://www.hfgproject.org/ethiopia-health-sector-financing-reform-hfg-end-of-project-report/. Accessed 18 Nov 2020.
Practices and Challenges of Private Wing in Addis Ababa Hospitals. Available at: http://localhost:80/xmlui/handle/123456789/9231. Accessed 2 Nov 2018.
Geberu DM, Biks GA, Gebremedhin T, Mekonnen TH. Factors of patient satisfaction in adult outpatient departments of private wing and regular services in public hospitals of Addis Ababa, Ethiopia: a comparative cross-sectional study. BMC Health Serv Res. 2019;19(1):1–13.
Ambelie YA, Demssie AF, Gebregziabher MG. Patients’ satisfaction and associated factors among private wing patients at Bahirdar Felege Hiwot Referral Hospital, North West Ethiopia. Sci J Public Health. 2014;2(5):417–23.
Mekonen AM, Gebregziabher MG, Teferra AS. The effect of community based health insurance on catastrophic health expenditure in Northeast Ethiopia: A cross sectional study. PLoS ONE. 2018;13(10):e0205972.
Shigute Z, Mebratie AD, Sparrow R, Alemu G, Bedi AS. The effect of ethiopia’s community-based health insurance scheme on revenues and quality of care. Int J Environ Res Public Health. 2020;17(22):8558.
Mebratie AD, Sparrow R, Yilma Z, Abebaw D, Alemu G, Bedi AS. The impact of Ethiopia’s pilot community based health insurance scheme on healthcare utilization and cost of care. Soc Sci Med. 2019;220:112–9.
Asfaw A, Von Braun J. Innovations in health care financing: New evidence on the prospect of community health insurance schemes in the rural areas of Ethiopia. Int J Health Care Finance Econ. 2005;5(3):241–53.
Nageso D, Tefera K, Gutema K. Enrollment in community based health insurance program and the associated factors among households in Boricha district, Sidama Zone, Southern Ethiopia; a cross-sectional study. PLoS ONE. 2020;15(6):e0234028.
Eseta WA, Lemma TD, Geta ET. Magnitude and Determinants of Dropout from Community-Based Health Insurance Among Households in Manna District, Jimma Zone, Southwest Ethiopia. ClinicoEconomics and Outcomes Research: CEOR. 2020;12:747.
Ageze L. Health facility governance in the Ethiopian health system. Bethesda: Health Systems; 2012. p. 20:20.
Demissie B, Negeri KG. Effect of community-based health insurance on utilization of outpatient health care services in Southern Ethiopia: a comparative cross-sectional study. Risk Manage Healthcare Policy. 2020;13:141.
Tilahun H, Atnafu DD, Asrade G, Minyihun A, Alemu YM. Factors for healthcare utilization and effect of mutual health insurance on healthcare utilization in rural communities of South Achefer Woreda, North West Ethiopia. Health Econ Rev. 2018;8(1):1–7.
Garedew MG, Sinkie SO, Handalo DM, Salgedo WB, Kehali KY, Kebene FG, Waldemarium TD, Mengesha MA. Willingness to Join and Pay for Community-Based Health Insurance Among Rural Households of Selected Districts of Jimma Zone, Southwest Ethiopia. ClinicoEconomics and outcomes research: CEOR. 2020;12:45.
Obse AG, Ataguba JE. Assessing medical impoverishment and associated factors in health care in Ethiopia. BMC Int Health Hum Rights. 2020;20(1):1–9.
Atnafu DD, Tilahun H, Alemu YM. Community-based health insurance and healthcare service utilisation, North-West, Ethiopia: a comparative, cross-sectional study. BMJ Open. 2018;8(8):e019613.
Badacho AS, Tushune K, Ejigu Y, Berheto TM. Household satisfaction with a community-based health insurance scheme in Ethiopia. BMC Res Notes. 2016;9(1):1–10.
Setegn A, Andargie G, Amare G, Debie A. Willingness to Pay for Social Health Insurance Among Teachers at Governmental Schools in Gondar Town, Northwest Ethiopia. Risk Manage Healthcare Policy. 2021;14:861.
Atafu A, Kwon S. Adverse selection and supply-side factors in the enrollment in community-based health insurance in Northwest Ethiopia: A mixed methodology. Int J Health Plann Manage. 2018;33(4):902–14.
Minyihun A, Gebregziabher MG, Gelaw YA. Willingness to pay for community-based health insurance and associated factors among rural households of Bugna District Northeast Ethiopia. BMC Res Notes. 2019;12(1):1–7.
Gidey MT, Gebretekle GB, Hogan M-E, Fenta TG. Willingness to pay for social health insurance and its determinants among public servants in Mekelle City, Northern Ethiopia: a mixed methods study. Cost Eff Resour Alloc. 2019;17(1):1–11.
Obse A, Hailemariam D, Normand C. Knowledge of and preferences for health insurance among formal sector employees in Addis Ababa: a qualitative study. BMC Health Serv Res. 2015;15(1):1–11.
Mebratie AD, Sparrow R, Yilma Z, Alemu G, Bedi AS. Dropping out of Ethiopia’s community-based health insurance scheme. Health Policy Plan. 2015;30(10):1296–306.
Ashagrie B, Biks GA, Belew AK. Community-Based Health Insurance Membership Dropout Rate and Associated Factors in Dera District, Northwest Ethiopia. Risk Manage Healthcare Policy. 2020;13:2835.
Mekonne A, Seifu B, Hailu C, Atomsa A. Willingness to pay for social health insurance and associated factors among health care providers in Addis Ababa Ethiopia. Biomed Res Int. 2020;2020:8412957.
Hailu Z. Health care financing reform in Ethiopia: improving quality and equity. Washington: USAID; 2012.
Gessesse A, Yitayal M, Kebede M, Amare G. Health Service Utilization Among Out-of-Pocket Payers and Fee-Wavier Users in Saesie Tsaeda-Emba District, Tigray Region, Northern Ethiopia: A Comparative Cross-Sectional Study. Risk Manag Healthc Policy. 2021;14:695.
Chote T, Tushune K, Yitbarek K, Woldie M. The utilization of health services among poor households with user fee payment waiver certificate in Gamo Gofa zone, southern Ethiopia. Divers Equality Health Care. 2017;14(5):243–8.
Zelalem Y. Assessment of fee waiver health care implementation status in the new health care financing strategy in Bahir Dar, North West Ethiopia. 2010.
Tesfaye H. Assessment of Utilization of Fee Waiver System among Beneficiaries in Addis Ababa, Ethiopia, 2017. Addis Ababa: Addis Ababa University; 2017.
Engida E, Mariam DH. Assessment of the free health care provision system in Bahir Dar area, northern Ethiopia. Ethiopian journal of health development. 2002;16(2):173–82.
Essential Health Services in Ethiopia published in July 2015. Available at: https://www.hfgproject.org/essential-package-of-health-services-country-snapshot-ethiopia/. Accessed 16 Nov 2020.
Babure ZK, Jiru FA, Weldemarium TD. Client satisfaction among private wing and regular health care services at Nekemte referral hospital, east Wollega zone, Oromia regional state, Western Ethiopia: a comparative cross-sectional study, 2016. J Public Health Epidemiol. 2018;10(2):43–61.
Mengesha TM. The Effect Of Private Wing Set Up On Work Performance Of Health Professionals At Public Hospitals In Addis Ababa. Addis Ababa: Addis Ababa University; 2018.
Outsourcing Non-clinical Services in Public Hospitals: Achievements and Lessons from Ethiopia. Available at: https://www.hfgproject.org/outsourcing-non-clinical-services-in-public-hospitals-achievements-and-lessons-from-ethiopia/. Accessed 11 Sept 2017.
Fite MB, Roba KT, Merga BT, Tefera BN, Beha GA, Gurmessa TT. Factors associated with enrollment for community-based health insurance scheme in Western Ethiopia: Case-control study. PLoS ONE. 2021;16(6):e0252303.
Atnafu A, Tariku A. Perceived Quality of Healthcare and Availability of Supplies Determine Household-Level Willingness to Join a Community-Based Health Insurance Scheme in Amhara Region Ethiopia. ClinicoEcon Outcomes Res. 2020;12:683.
Gebru T, Lentiro K. The impact of community-based health insurance on health-related quality of life and associated factors in Ethiopia: a comparative cross-sectional study. Health Qual Life Outcomes. 2018;16(1):1–6.
Abazinab S, Woldie M, Alaro T. Readiness of health centers and primary hospitals for the implementation of proposed health insurance schemes in Southwest Ethiopia. Ethiop J Health Sci. 2016;26(5):449–56.
Ayana ID. Investigation of Moral Hazard Deportments in Community-Based Health Insurance in Guto Gida District, Western Ethiopia: A Qualitative Study. ClinicoEcon Outcomes Res. 2020;12:733.
Demissie GD, Atnafu A. Barriers and Facilitators of Community-Based Health Insurance Membership in Rural Amhara Region, Northwest Ethiopia: A Qualitative Study. ClinicoEcon Outcomes Res. 2021;13:343.
Kado A, Merga BT, Adem HA, Dessie Y, Geda B. Willingness to Pay for Community-Based Health Insurance Scheme and Associated Factors Among Rural Communities in Gemmachis District, Eastern Ethiopia. ClinicoEcon Outcomes Res. 2020;12:609.
Bantie GM, Woya AA, Zewdie BM. Community-Based Health Insurance and Associated Factors in North-Western Ethiopia. The Case of Bahir Dar City. Int J Gen Med. 2020;13:1207.
Abdilwohab MG, Abebo ZH, Godana W, Ajema D, Yihune M, Hassen H. Factors affecting enrollment status of households for community based health insurance in a resource-limited peripheral area in Southern Ethiopia Mixed method. PLoS ONE. 2021;16(1):e0245952.
Agency EHI. Evaluation of community‐based health insurance pilot schemes in Ethiopia. 2015.
Argaw MD, Desta BF. Examining governing board functions and health center performances during health system reform: a cross-sectional study in 4 regional states of Ethiopia. Int J Health Policy Manag. 2020. https://doi.org/10.34172/ijhpm.2020.235. Accessed 25 Jan 2021.
Federal Democratic Republic of Ethiopia Ministry of Health. Health Sector Development Program IV: 2010/11–2014/15. In: Ministry of Health Addis Ababa. 2010.
Ataguba JE. Community Health Insurance Scheme as a viable option for rural population in Nigeria. Paper submitted to the Centre for the study of African Economies (CSAE). Oxford: Department of Economics, University of Oxford 2008.
McIntyre D. What healthcare financing changes are needed to reach universal coverage in South Africa? S Afr Med J. 2012;102(6):489–90.
Kutzin J, Jakab M, Shishkin S. From scheme to system: social health insurance funds and the transformation of health financing in Kyrgyzstan and Moldova. In: Innovations in health system finance in developing and transitional economies. edn. Bingley: Emerald Group Publishing Limited; 2009.
Limwattananon S, Vongmongkol V, Prakongsai P, Patcharanarumol W, Hanson K, Tangcharoensathien V, Mills A: The equity impact of Universal Coverage: health care finance, catastrophic health expenditure, utilization and government subsidies in Thailand. Consortium for Research on Equitable Health Systems, Ministry of Public Health; 2011. http://www.crehs.lshtm.ac.uk/thai_biafia_19jul.pdf. Accessed June 2011.
O’donnell O, Van Doorslaer E, Rannan-Eliya RP, Somanathan A, Adhikari SR, Akkazieva B, Harbianto D, Garg CC, Hanvoravongchai P, Herrin AN. Who pays for health care in Asia? J Health Econ. 2008;27(2):460–75.
Ataguba JE. Assessing equitable health financing for universal health coverage: a case study of South Africa. Appl Econ. 2016;48(35):3293–306.
Berman P, Mann C, Ricculli M. Financing Ethiopia’s Primary Care to 2035: A Model Projecting Resource Mobilization and Costs. Boston, Massachusetts: Harvard TH Chan School of Public Health; 2015.
McIntyre D, Gilson L, Mutyambizi V. Promoting equitable health care financing in the African context: Current challenges and future prospects. 2005.
Govender V, McIntyre D, Loewenson R. Progress towards the Abuja target for government spending on health care in East and Southern Africa. Cape Town, SA: EQUINET; 2008.
Spending for Health in Malawi. Current Trends and Strategies to Improve Efficiency and Equity in Health Financing. Available at: https://openknowledge.worldbank.org/handle/10986/35864. Accessed 1 Apr 2021.
Health financing strategy. Avail at: https://www.moh.gov.gh/wp-content/uploads/2016/02/Health-Finance-Strategy-160203045304.pdf. Accessed Feb 2016.
Prakongsai P, Limwattananon S, Tangcharoensathien V. The equity impact of the universal coverage policy: lessons from Thailand. In: Innovations in health system finance in developing and transitional economies. edn. Bingley: Emerald Group Publishing Limited; 2009.
Reeves A, McKee M, Basu S, Stuckler D. The political economy of austerity and healthcare: Cross-national analysis of expenditure changes in 27 European nations 1995–2011. Health Policy. 2014;115(1):1–8.
Myint C-Y, Pavlova M, Thein K-N-N, Groot W. A systematic review of the health-financing mechanisms in the Association of Southeast Asian Nations countries and the People’s Republic of China: lessons for the move towards universal health coverage. PloS one. 2019;14(6):e0217278.
Artiga S, Ubri P, Zur J. The effects of premiums and cost sharing on low-income populations: updated review of research findings. San Francisco: Kaiser Family Foundation. 1 June 2017. 2019.
Artiga S, Ubri P, Zur J: The effects of premiums and cost sharing on low-income populations: updated review of research findings. Henry J Kaiser Family Foundation; 2017.
The political path to universal health coverage: Elite commitment to community-based health insurance in Rwanda. ESID Working Paper No. 72. Manchester, UK: The University of Manchester. Available at www.effectivestates.orgambídez-RamosAlejandro
Tangcharoensathien V, Prakongsai P, Limwattananon S, Patcharanarumol W, Jongudomsuk P: Achieving universal coverage in Thailand: what lessons do we learn? Available at SSRN 1111870. 2007.
Bitran RA, Giedion U. Waivers and exemptions for health services in developing countries: Social Protection, World Bank; 2003.
McPake B, Schmidt A, Araujo E, Kirunga-Tashobya C. Freeing-up Healthcare: A guide to removing user fees. 2008.
Acknowledgements
The first author would like to acknowledge those senior researchers (RBK and YA) for their advice and comments who assisted in shaping the review.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
AD, RBK and YA discussed and conceptualised the ideas. AD was independently extracted the data. RBK and YA verified the extracted information and supplemented their guidance. AD prepared the first draft of the review manuscript. AD, RBK and YA were involved in the data synthesis and review of the article. Finally, AD, RBK and YA authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was not required since the study was a systematic review of articles and published books.
Consent for publication
Not applicable.
Competing of interest
The authors declared that there was no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PubMed search strategy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Debie, A., Khatri, R.B. & Assefa, Y. Contributions and challenges of healthcare financing towards universal health coverage in Ethiopia: a narrative evidence synthesis. BMC Health Serv Res 22, 866 (2022). https://doi.org/10.1186/s12913-022-08151-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-022-08151-7