
Abstract
Background
Up to 50% of medicines are not used as intended, resulting in poor health and economic outcomes. Medicines optimisation is ‘a person-centred approach to safe and effective medicines use, to ensure people obtain the best possible outcomes from their medicines’. The purpose of this exercise was to co-produce a prioritised research agenda for medicines optimisation using a multi-stakeholder (patient, researcher, public and health professionals) approach.
Methods
A three-stage, multiple method process was used including: generation of preliminary research questions (Stage 1) using a modified Nominal Group Technique; electronic consultation and ranking with a wider multi-stakeholder group (Stage 2); a face-to-face, one-day consensus meeting involving representatives from all stakeholder groups (Stage 3).
Results
In total, 92 research questions were identified during Stages 1 and 2 and ranked in order of priority during stage 3. Questions were categorised into four areas: ‘Patient Concerns’ [e.g. is there a shared decision (with patients) about using each medicine?], ‘Polypharmacy’ [e.g. how to design health services to cope with the challenge of multiple medicines use?], ‘Non-Medical Prescribing’ [e.g. how can the contribution of non-medical prescribers be optimised in primary care?], and ‘Deprescribing’ [e.g. what support is needed by prescribers to deprescribe?]. A significant number of the 92 questions were generated by Patient and Public Involvement representatives, which demonstrates the importance of including this stakeholder group when identifying research priorities.
Conclusions
A wide range of research questions was generated reflecting concerns which affect patients, practitioners, the health service, as well the ethical and philosophical aspects of the prescribing and deprescribing of medicines. These questions should be used to set future research agendas and funding commissions.
Similar content being viewed by others


Background
Globally, medicines are the most commonly used healthcare intervention [1]. In the United Kingdom (UK), for example, over 1 billion prescription items are dispensed annually in the community, many for chronic health conditions [2]. Up to 50% of medicines are not used as intended [3] and, as a result, health outcomes are sub-optimal. Both over- and under- use of medicines leads to diminished benefits, greater costs and increased harms [3], and is viewed by the World Health Organisation (WHO) as a global patient safety problem [4].
Medicines optimisation, ‘a person-centred approach to safe and effective medicines use, to ensure people obtain the best possible outcomes from their medicines’ [5], focuses on ensuring that the patient derives the most benefit from their medicines, and requires a holistic approach and an effective partnership between health professionals and patients [5, 6]. It also includes deprescribing, i.e. the process of withdrawing a patient’s medicine to improve health or mitigate against possible adverse side effects [7, 8]. Medicines optimisation is of relevance and importance to a wide range of stakeholders including patients, the public, healthcare professionals, health service commissioners and policymakers. Achieving the optimal use of medicines is complex due to competing priorities and agendas of different stakeholders [9]. The development of relevant policy requires an expansion of the evidence base, which reflects the needs of all stakeholders. This is apposite as medicines optimisation is typically under-represented in current models of care [10].
Involving patients and their advocates in the co-production of health services and research is becoming more commonplace [11]. Co-production leads to differentiated services and choice, increased responsiveness to changing needs, and reduced waste and costs [12]. It emphasises the contribution that all stakeholders can make as initiators or recipients of the service delivery process [12, 13] and is based on egalitarian relationships between experts and lay people, using a process of open exchange and participation [14]. The inclusion of the public and other stakeholders in research agenda setting is increasing [15,16,17] but until now, has not included medicines optimisation. The aim of this exercise was to adopt a multi-stakeholder approach to the co-production of a prioritised research agenda for medicines optimisation. In so doing, the agenda could be used to inform future funding initiatives and activities. This process was undertaken as a GW4 Alliance [18] research initiative; a collaboration between the Universities of Bath, Bristol, Cardiff and Exeter.
Method
Study design
The prioritisation process involved multiple stages and methods. These included identification of a broad range of stakeholders, face-to-face meetings to generate initial research questions, and a one-day workshop to prioritise the research questions generated. The overall process was based on a modified Nominal Group Technique (NGT) [19,20,21]. The NGT is usually conducted with homogenous groups [22].
Stage 1: generation of preliminary research questions
The first stage involved the identification of key stakeholders within the GW4 Alliance institutions, e.g. academics with expertise in pharmacy and pharmacology, medical and other healthcare professionals, and patient and public involvement representatives i.e. health service users and organisational representatives. In August 2018, a face-to-face stakeholder meeting was convened (by the corresponding author), to undertake a modified Nominal Group Technique (NGT) [19,20,21]. Participants were provided background information and asked to address thequestion: ‘What are the priority topics/areas that need to be addressed so that medicines optimisation can be realised?’. During the meeting, participants, including the research team, were encouraged to generate as many questions as possible in response to the research question; these were recorded as individual written responses and collated on flip-charts. No discussion was permitted until the generation process was complete. Discussion then followed for the purpose of clarification of questions, removal of duplicates and the identification of common themes. Following the meeting, the questions were reviewed by the research team and refined to produce a distilled list of research questions for consideration in Stage 2. Each question was assigned to one of four categories that reflected common themes: ‘patient concerns’, ‘polypharmacy’, ‘non-medical prescribing’ (NMP), and ‘deprescribing.
Stage 2: consultation with wider stakeholder group
The purpose of Stage 2 was to seek input from a wider stakeholder group regarding the original research questions identified in Stage 1. In addition to Stage 1 participants, an email invitation was sent to 80 individuals identified from relevant literature and policy documents and via the professional networks of the core research team and which included a wide range of local, regional, national, and international stakeholders (e.g. pharmacists, academic pharmacists, physicians, National Health Service (NHS) Trust directors, patients, physicians, health workers, and advocacy organisations (including Age UK and the Patients’ Association)). All questions from Stage 1 were presented in a document, using the four categories, and emailed to all prospective participants. The task for participants was to rank the Stage 1 questions according to their perceived importance, and to add new questions from their own ideas/experiences. For each original question, a mean rank was calculated using the Excel rank function. Additional questions suggested by participants were sense checked with duplicate questions removed or combined and then assigned to one of the original four question categories according to its content.
Stage 3: final prioritisation
Stage 3 comprised a one-day prioritisation workshop in November 2018, held on University of Bath campus and facilitated the lead author (MCW). All respondents in Stages 1 and 2 were invited. Participants and the research team were purposively assigned to one of four groups comprising eight individuals, to ensure that each group included a range of participants, e.g. at least one lay representative, and representatives from each stakeholder group.
The research questions in each of the four categories were discussed within each group with each category being assigned 45-min discussion session. Discussion included the opportunity to reflect on the mean rank of questions from Stage 1.
Following discussion session, the participants rated the importance of each question. TurningPoint software was used, which facilitates live polling and as well as the curation and simple statistical analysis of results [23]. Each question was presented alongside a Likert scale, ranging from one (‘extremely important’), to seven (‘extremely unimportant’). Participants rated each question independently. The process was then repeated for three remaining categories of research questions.
Following the meeting, the questions were presented in ordered rank to derive a definitive list of prioritised research questions (Additional file 1; a list of all 92 questions alongside their rank, how they were rated by PPIs and non-PPIs, and the percentage of ‘extremely important’ and ‘important’ ratings).
Patient and public participants received a participation fee and their travel expenses were reimbursed. Non-PPI participants had their travel expenses reimbursed if requested, but received no additional payment for their involvement.
Ethical approval and consent
Ethical approval was not required for this study (confirmed by the Ethics Officer of the Department of Pharmacy and Pharmacology, University of Bath). As such, signed consent was not sought from any participant. Participation in, and completion of, each stage was accepted as participants’ consent to participate.
Data analysis
A Borda count [24, 25] was used to rank the order of questions prioritised in Stage 3, where the Likert rating ‘extremely important’ was given a weighting of 7, ‘important’ a weighting of 6 and so forth, to ‘extremely unimportant’ weighted as 1. Following weighting, the number of times a question was rated as ‘extremely important’ was combined with the number of times it was rated as ‘important’ etc. For example, if 19 people rated a question as ‘extremely important’, eight rated it as ‘important’, and five rated it ‘somewhat important’, then its overall weighted score would be (19 × 7) + (8 × 6) + (5 × 5) = 206. Weighted question totals were subsequently ranked according to median score.
Using the process described above, the top five questions prioritised in each topic area by PPI participants were compared with the rank given to the selected questions by all other participants (designated as non-PPI). The purpose of this comparison was to determine whether substantial differences existed in the type of question that both types of participants prioritised. Such information provides greater insight into the heterogeneity of different stakeholder types. During ranking exercises, participants often rank their most and least favourite choices, based for example on familiarity with concepts, therefore middle rankings may reflect more arbitrary or indifferent choices [26]. As such, the five highest ranked questions are discussed as this number will likely capture the broad range of what participants have actively considered as most important, while allowing sufficient coverage of the overall question set.
Results
Stage 1: generation of preliminary research questions
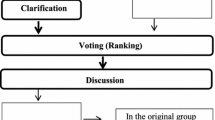
Nineteen individuals participated. Of these, the majority were academics, eight of whom had a pharmacy background (Fig. 1), as well as two GPs and two PPI representatives. Thirty questions were generated and grouped into four categories. All five questions pertaining to patient concerns were generated by PPI representatives.

The identification and prioritisation of medicines optimisation research questions: numbers of participants and questions generated by stage
Stage 2: consultation with wider stakeholder group
Forty stakeholders, including those from Stage 1, participated in Stage 2 (Fig. 1); two Stage 1 participants did not participate in any later stages of this process. Approximately one third of participants were academics and four participants had a medical background. In total, 62 new questions were generated across the four categories: patient concerns (13), polypharmacy (13), non-medical prescribing (14), and deprescribing (22). Of these, 28 were generated by PPI representatives. All the additional questions nominally reflected the four categories. Four suggestions were omitted due to ambiguity of meaning e.g. “Need to do more about process”. Some questions, reflected more than one category. For example, “How is deprescribing, polypharmacy, etc undertaken by NMPs?”. These questions were assigned to the category deemed most relevant to their content.
Stage 3: final prioritisation
In total, 32 of the 40 Stage 2 participants participated in the Stage 3 meeting, comprising academic pharmacists (n = 9), pharmacists including a regional deputy director of the medicines information service and an NHS Trust regional director of pharmacy (n = 9), PPI representatives (n = 7), academic researchers (n = 5), and GPs (n = 2).
Over half of the participants provided a rating of ‘extremely important’ or ‘important’ for 13 of 22 patient concerns questions, 14 of 28 polypharmacy questions, 7 of 17 non-medical prescriber questions, and 15 of 25 deprescribing questions. Two questions from the polypharmacy category, relating to the status of theory and a specific intervention tool, received a rating of ‘unimportant’ or ‘extremely unimportant’ from just under a third of participants. No other question in any category received comparably negative ratings. In all categories, ratings were skewed toward the positive end of the scale; only one question in the category of polypharmacy demonstrated polarisation, i.e. equal numbers of positive and negative ratings. This question pertained to whether clusters of co-morbidities are ‘more important’ than the total number of co-morbidities.
Of the top 20 items identified across the four categories (i.e. five per category) 10 had been identified by the wider stakeholder group during Stage 2; five questions received an ‘extremely important’ or ‘important’ rating from at least three-quarters of participants (Table 1). All Stage 3 questions are presented in Additional file 1.
The comparison of PPI versus non-PPI results demonstrates variation across the different types of participants (Table 2). Only nine of the 20 highest ranked questions by PPI participants were ranked highly by the non-PPI participants.
The greatest similarities between the two types of participants were in the ‘patient concerns ‘category, where four of the top five questions were mutually identified as priorities.
Discussion
To our knowledge, this is the first report of a multi-stakeholder approach to the development and prioritisation of research questions associated with medicines optimisation. Similar processes are used by the James Lind Alliance [27]. The current exercise adopted a systematic approach that incorporated the opinions of a wide range of stakeholders using participatory methods. The value of these stakeholders, rather than limiting the process to academic researchers and the literature, was illustrated by the additional 62 questions that were identified during Stage 2 as a result of including the extended stakeholder group, as well as the comparison of PPI and non-PPI priorities. Ten of the top 20 questions were identified by PPI; i.e. indicating the importance of including these stakeholders. Our results illustrate the importance of patient and public participants to inform research and guideline development in relation to medicines optimisation, as recommended by an earlier review [28]. The priorities identified by this process could be used by: research funders to inform future research funding initiatives; researchers to identify and address priorities in medicines optimisation research; PPI organisations to lobby for change and promote awareness; and health professionals to consider in terms of their medicines optimisation practice. Many of these priorities are likely to be of relevance to the international community despite being generated in the UK and reflect the aforementioned WHO global patient safety concern.
Several of the high priority questions reflected the extent to which patients’ views and experiences are considered during medication reviews. Few tools exist for eliciting patient priorities and preferences during consultations, including medication reviews [29]. As such, this service might benefit from the introduction of a common framework built on equity, confidence, and perceptions of acceptance [30], for defining and classifying patient-mediated interventions. Most of the questions associated with medication reviews related to ‘structural’ elements, i.e. what constitutes a ‘good’ review, and when is the ‘right’ time to undertake a review. The challenge for future work comes from operationalising these questions in objective, less value-laden terminology. This was also reflected with the prioritisation of questions regarding polypharmacy – for example, the nature of information and education that the patient would require to enable them to engage and have ownership of their medication management.
Polypharmacy is of increasing relevance due to the ageing population and the increasing number of people receiving multiple medicines [2]. The top priorities around polypharmacy identified in the present exercise reflect the challenge of how best to involve patients in decision making, especially in relation to medication reviews, and how primary care is best engineered to ensure their effectiveness.
In the UK, a range of non-medical health professionals can prescribe medicines for patient [31]. The growth in numbers of non-medical prescribers reflects the need to mitigate increasing demands on the NHS [32]. The ability to prescribe has the potential to enhance the roles of health care professionals and improve patient care by facilitating treatment provision in settings more accessible to patients and possibly in a more timely manner [33]. The top five research questions in the NMP category included the need to raise patient awareness of NMPs and the extent to which NMP training provides practitioners with the confidence to address complex polypharmacy and deprescribing issues [34]. It has been suggested that educational programmes for NMPs would benefit from considering how best to maintain the currency of practitioners’ knowledge [35], and that education aimed at the public may be warranted, to address concerns and limited awareness with regard to the diagnostic skills and status of NMPs [36].
The top-ranked ‘Deprescribing’ priority was “how to empower patients to take a more active role in self-management and self-monitoring of multiple long-term conditions, including deprescribing?”, which was were ranked ‘extremely important’ or ‘important’ by at least three-quarters of participants, indicating a convergence towards the desire for a broad culture shift i.e. consultations which reflect a more person-centered approach (a core component of medicines optimisation), whereby patient perspectives are an integral part of the decision-making process. Challenges associated with deprescribing include how it is defined, whether it is safe, and how these aspects are communicated to patients and health care professionals alike [37]. This reflects a desire to adopt a holistic approach to medicines optimisation, whereby patient perspectives and values are central to the consultation process, teams are inherently multidisciplinary, and where the general perspectives as well as complexities of individual cases can be addressed [38,39,40].
The PPI research infrastructure has existed for over a decade [41] and the importance of PPI in this prioritisation exercise was reinforced by the many differences between their views and those of the non-PPI participants [42]. Given that patient involvement in healthcare decision-making can lead to better affective, cognitive and health outcomes [43, 44], the value of involving patients in the entire research process is implicit in the top-ranked ‘patient concerns’, ‘Is there a shared decision (with patients) about using each medicine?’
The third WHO Global Patient Safety Challenge, Medication Without Harm, identified medication safety as a priority [45]. A separate consensus exercise identified the need to adopt technology to enhance medication safety, and to develop guidelines and standard operating procedures for high-risk patients, medications and contexts [46]. Within this current prioritisation exercise, it was seldom stated explicitly medication safety but was implicit in many questions. For example, ‘Patient concerns’ ‘What are the advantages and disadvantages of online pharmacy services in relation to access to medicines and safety, patient experience, out-of-pocket expenses, information provision?’ (rank 19), and ‘Deprescribing’ ‘Where are the gaps in education and safety (about deprescribing) and how these can be addressed is key to ensuring deprescribing is safe and effective?’ (rank 4). This observation may reflect the wording of the original NGT question and that the subsequent apportioning of questions across the four categories decreased the salience of ‘safety’. As such, priorities identified in the current exercise may differ substantially from global priorities where, for example, medicine safety is a recognised priority [47].
Strengths and limitations
A strength of this prioritisation exercise was the representation at each stage of different stakeholder groups (including PPI, pharmacists, and GPs) to ensure that their different perspectives and experiences were represented throughout the process. This is likely to have improved the relevance and real-world value of the research outcomes, as well as the validity and reliability of the findings [48]. Conversely, however, the high proportion of pharmacist participants could have influenced the results although the overall findings suggest that this did not occur. If this approach was repeated with a wider range of stakeholders, e.g. nurses and other NMPs and health professionals, different priorities could have been generated. Similarly, if repeated at a different time, the outcomes could be influenced by high profile health concerns e.g. COVID-19. An additional limitation relates to the Stage 3 procedure of aggregating ratings into an overall rank. Ascribing a score to each rating and then summing the scores for a set of ratings by any one individual may produce the same magnitude of outcome from quite different sets of ratings. The Borda count employed in Stage 3 overcomes this to some degree in that it takes all the rating preferences into account by attributing weighted scores to each rating. However, this still assumes that scores are interval in nature and does not take into account the actual ‘attitude’ that the respondent may have towards the question content [49]. Nonetheless, to test whether different scoring approaches significantly altered the nature of rankings, different methods of analysis were explored. For example, given that ratings were skewed toward positive assessments, rankings were constructed based on aggregates of only ‘extremely important’ and ‘important’ ratings. While this did not affect overall ranks substantially, it was decided that a full Borda count that incorporated all ratings was more apposite in that it maintained the full range of perspectives from all participants.
Conclusions
We illustrate the value of co-producing a prioritised research agenda for medicines optimisation using a multi-stakeholder approach. Hence, the results and priorities identified are relevant for clinicians, researchers, funding bodies, and policy makers, in terms of the future research agenda. Moreover, the results demonstrate the importance and value of adopting an inclusive approach with agenda-setting for health care.
Availability of data and materials
The datasets used and/or analysed during the current exercise are available from the corresponding author on request.
Abbreviations
- NGT:
-
Nominal group technique
- NHS:
-
National Health Service
- NMP:
-
Non-medical prescribing
- PPI:
-
Public and Patient Involvement
- UK:
-
United Kingdom
- WHO:
-
World Health Organisation
References
Bigdeli M, Peters D, Wagner A: Medicines in health systems: advancing access, affordability and appropriate use. 2014. https://www.who.int/alliance-hpsr/resources/FR_webfinal_v1.pdf.
Guthrie B, Makubate B, Hernandez-Santiago V, Dreischulte T. The rising tide of polypharmacy and drug-drug interactions: population database analysis 1995–2010. BMC Med. 2015;13(1):74.
Duerden M, Avery T, Payne R. Polypharmacy and medicines optimisation. Making it safe and sound. London: The King’s Fund; 2013.
WHO. Medication without harm - global patient safety challenge on medication safety. Geneva: World Health Organisation; 2017.
Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes. https://www.ncbi.nlm.nih.gov/books/NBK305021/pdf/Bookshelf_NBK305021.pdf. Accessed 20 Sept 2019.
Picton C, Wright H. Medicines optimisation: helping patients to make the most of medicines. In: Good practice guidance for healthcare professionals in England Royal Pharmaceutical Society; 2013.
Le Couteur D, Banks E, Gnjidic D, McLachlan A. Deprescribing; 2011.
Jansen J, Naganathan V, Carter SM, McLachlan AJ, Nickel B, Irwig L, Bonner C, Doust J, Colvin J, Heaney A. Too much medicine in older people? Deprescribing through shared decision making. BMJ. 2016;353:6.
Faria R, Barbieri M, Light K, Elliott RA, Sculpher M. The economics of medicines optimization: policy developments, remaining challenges and research priorities. Br Med Bull. 2014;111(1):45–61.
Alldred DP, Kennedy MC, Hughes C, Chen TF, Miller P. Interventions to optimise prescribing for older people in care homes. Cochrane Database Syst Rev. 2016;2(2):CD009095.
Buckley B, Grant AM, Firkins L, Greene AC, Frankau J. Working together to identify research questions. Continence UK. 2007;1(1):76–81.
Batalden M, Batalden P, Margolis P, Seid M, Armstrong G, Opipari-Arrigan L, Hartung H. Coproduction of healthcare service. BMJ Qual Saf. 2015;25(7):9.
Bovaird T, Loeffler E. The role of co-production for better health and wellbeing: why we need to change. In: Loeffler E, Power G, Bovaird T, Hine-Hughes F, editors. Co-production of health and wellbeing in Scotland Governance International, Birmingham, UK; 2013. p. 20–8.
Wehrens R. Beyond two communities–from research utilization and knowledge translation to co-production? Public Health. 2014;128(6):545–51.
Hart AL, Lomer M, Verjee A, Kemp K, Faiz O, Daly A, Solomon J, McLaughlin J. What are the top 10 research questions in the treatment of inflammatory bowel disease? A priority setting partnership with the James Lind Alliance. J Crohn's Colitis. 2016;11(2):204–11.
Finer S, Robb P, Cowan K, Daly A, Shah K, Farmer A. Setting the top 10 research priorities to improve the health of people with type 2 diabetes: a Diabetes UK–James Lind Alliance priority setting partnership. Diabet Med. 2018;35(7):862–70.
Oliver S, Milne R, Bradburn J, Buchanan P, Kerridge L, Walley T, Gabbay J. Involving consumers in a needs-led research programme: a pilot project. Health Expect. 2001;4(1):18–28.
GW4 Alliance. https://gw4.ac.uk/. Accessed 23 Aug 2019.
Rankin NM, McGregor D, Butow PN, White K, Phillips JL, Young JM, Pearson SA, York S, Shaw T. Adapting the nominal group technique for priority setting of evidence-practice gaps in implementation science. BMC Med Res Methodol. 2016;16(1):110.
McMillan SS, King M, Tully MP. How to use the nominal group and Delphi techniques. Int J Clin Pharm. 2016;38(3):655–62.
Manera K, Hanson C, Gutman T, Tong A. Consensus methods: nominal group technique. In: Handbook of research methods in health social sciences; 2018. p. 1–14.
Hutchings HA, Rapport FL, Wright S, Doel MA. Obtaining consensus from mixed groups: an adapted nominal group technique. J Adv Med Med Res. 2013;3(3):491–502.
Turning Point Technology software. https://www.turningtechnologies.com/turningpoint/. Accessed 4 Sept 2019.
Mullen PM. Public involvement in health care priority setting: an overview of methods for eliciting values. Health Expect. 1999;2(4):222–34.
Emerson P. The original Borda count and partial voting. Soc Choice Welf. 2013;40(2):353–8.
Ben-Akiva M, Morikawa T, Shiroishi F. Analysis of the reliabilty of preference ranking data. J Busn Res. 1991;23:253–68.
James Lind Alliance. http://www.jla.nihr.ac.uk/about-the-james-lind-alliance/. Accessed 3 Sept 2019.
Heaton J, Britten N, Krska J, Reeve J. Person-centred medicines optimisation policy in England: an agenda for research on polypharmacy. Prim Health Care Res Dev. 2017;18(1):24–34.
Mangin D, Stephen G, Bismah V, Risdon C. Making patient values visible in healthcare: a systematic review of tools to assess patient treatment priorities and preferences in the context of multimorbidity. BMJ Open. 2016;6(6):e010903.
Fønhus MS, Dalsbø TK, Johansen M, Fretheim A, Skirbekk H, Flottorp SA. Patient-mediated interventions to improve professional practice. Cochrane Database Syst Rev. 2018;9(9):CD012472.
Paterson RE, Redman SG, Unwin R, McElhinney E, Macphee M, Downer F. Non-medical prescribing assessment–an evaluation of a nationally agreed multi method approach. Nurse Educ Pract. 2016;16(1):280–6.
Courtenay M, Carey N, Stenner K. An overview of non-medical prescribing across one strategic health authority: a questionnaire survey. BMC Health Serv Res. 2012;12(1):138.
Carey N, Stenner K. Does non-medical prescribing make a difference to patients? Nurs Times. 2011;107(26):14–6.
Muth C, Blom JW, Smith SM, Johnell K, Gonzalez-Gonzalez AI, Nguyen TS, Brueckle MS, Cesari M, Tinetti ME, Valderas JM. Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: a systematic guideline review and expert consensus. J Intern Med. 2019;285(3):272–88.
Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health. 2010;31:399–418.
Hindi AM, Schafheutle EI, Jacobs S. Patient and public perspectives of community pharmacies in the United Kingdom: a systematic review. Health Expect. 2018;21(2):409–28.
Thillainadesan J, Gnjidic D, Green S, Hilmer SN. Impact of deprescribing interventions in older hospitalised patients on prescribing and clinical outcomes: a systematic review of randomised trials. Drugs Aging. 2018;35(4):303–19.
Riordan DO, Walsh KA, Galvin R, Sinnott C, Kearney PM, Byrne S. The effect of pharmacist-led interventions in optimising prescribing in older adults in primary care: a systematic review. SAGE Open Med. 2016;4:2050312116652568.
Hansen CR, O'mahony D, Kearney PM, Sahm LJ, Cullinan S, Huibers C, Thevelin S, Rutjes AW, Knol W, Streit S. Identification of behaviour change techniques in deprescribing interventions: a systematic review and meta-analysis. Br J Clin Pharmacol. 2018;84(12):2716–28.
Marvin V, Ward E, Poots AJ, Heard K, Rajagopalan A, Jubraj B. Deprescribing medicines in the acute setting to reduce the risk of falls. Eur J Hosp Pharm. 2017;24(1):10–5.
Wilson P, Mathie E, Poland F, Keenan J, Howe A, Munday D, Kendall S, Cowe M, Staniszewska S, Goodman C. How embedded is public involvement in mainstream health research in England a decade after policy implementation? A realist evaluation. J Health Serv Res Policy. 2018;23(2):98–106.
Price A, Albarqouni L, Kirkpatrick J, Clarke M, Liew SM, Roberts N, Burls A. Patient and public involvement in the design of clinical trials: an overview of systematic reviews. J Eval Clin Pract. 2018;24(1):240–53.
Shay LA, Lafata JE. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med Decis Mak. 2015;35(1):114–31.
Ng YK, Shah NM, Loong LS, Pee LT, Hidzir SAM, Chong WW. Attitudes toward concordance and self-efficacy in decision making: a cross-sectional study on pharmacist–patient consultations. Patient Prefer Adherence. 2018;12:615.
Donaldson LJ, Kelley ET, Dhingra-Kumar N, Kieny M-P, Sheikh A. Medication without harm: who’s third global patient safety challenge. Lancet. 2017;389(10080):1680–1.
Sheikh A, Rudan I, Cresswell K, Dhingra-Kumar N, Tan ML, Häkkinen ML, Donaldson L. Agreeing on global research priorities for medication safety: an international prioritisation exercise. J Glob Health. 2019;9(1):1–11.
Sheikh A, Dhingra-Kumar N, Kelley E, Kieny MP, Donaldson LJ. The third global patient safety challenge: tackling medication-related harm. Bull World Health Organ. 2017;95(8):546.
Alami H, Gagnon M-P, Fortin J-P. Involving citizen-patients in the development of telehealth services: qualitative study of experts’ and citizen-patients’ perspectives. J Particip Med. 2018;10(4):e10665.
Liddell TM, Kruschke JK. Analyzing ordinal data with metric models: what could possibly go wrong? J Exp Soc Psychol. 2018;79:328–48.
Acknowledgements
The authors wish to acknowledge and dedicate this paper to Mr. Richard Fitzgerald; a co-author and contributor who sadly died in 2019 before the paper was completed. Mr. Fitzgerald was a member of the Peninsula Public Involvement Group and an enthusiastic member of the research team. He was a long-standing advocate for medicines optimisation and health care improvement. He is sadly missed.
Funding
This work was funded by a GW4 initiator grant; reference number GW4-IF10–001. The funder had no involvement in the design, conduct or analysis of this exercise and had no involvement in the writing of this manuscript.
NB was partially funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care South West Peninsula. The NIHR had no involvement in the design, conduct or analysis of this exercise and had no involvement in the writing of this manuscript.
Author information
Authors and Affiliations
Contributions
JF drafted the manuscript and facilitated the prioritisation process. The exercise was conceived and designed by MW, RP, MC, and NB. JF, MW, RP, MC, NB, JV, RD, PD, DM, LT, RF, KW, DG, and KT contributed to the design, data collection and analysis, the preparation of the draft manuscript and provided approval of the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was not required for this exercise as it was not deemed to be research (nor service evaluation) as such, signed consent was not sought from any participant. Participation in, and completion of, each stage was accepted as participants’ consent to participate.
Consent for publication
The views expressed are those of the authors.
Competing interests
The authors declare that they have no conflicts of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fellenor, J., Britten, N., Courtenay, M. et al. A multi-stakeholder approach to the co-production of the research agenda for medicines optimisation. BMC Health Serv Res 21, 64 (2021). https://doi.org/10.1186/s12913-021-06056-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-021-06056-5