
Abstract
Background
Burnout syndrome (BS) is highly prevalent among medical students and is associated with lower empathy and worsening of medical students ́ mental health. The aim of our study was to identify prevalence of BS during internship and its association with self-rated social support and participation in extracurricular activities in one medical school in Brazil.
Methods
This was a cross-sectional study conducted in 2015, with 121 medical students on internship (56% response rate). They were evaluated using the Maslach Burnout Inventory – Human Services (MBI) and assessed about socio demographic data, social support and extracurricular activities.
Results
The overall BS prevalence was 57.5% among medical interns. High emotional exhaustion was present in 33.1% (N = 38) of interns, high depersonalization was observed in 45.7% (N = 58) and 36.2% of participants (N = 46) had low personal accomplishment. Individuals with participation in community services had lower frequency of depersonalization (prevalence ratio 0.61 CI95% 0.42–0.88). BS was not associated with different types of extracurricular activities and no association was found among BS and the behaviour of seeking social support.
Conclusions
We found high prevalence of BS in medical interns, however the behaviour of seeking social support had no association with BS. The interns participating in community activities had lower frequency of high depersonalization.
Resumo
Introdução
A síndrome de Burnout (SB) apresenta alta prevalência entre os estudantes de medicina e está associada a menor empatia e pior saúde mental. O objetivo deste estudo foi identificar a prevalência da SB durante o internato e sua associação com suporte social auto-relatado e atividades extracurriculares em uma faculdade de medicina brasileira.
Métodos
Estudo transversal conduzido em 2015, com 121 internos (taxa de resposta de 56%). Foram avaliados através da escala validada Maslach Burnout Inventory - Human Services (MBI) e questionário sociodemográfico que incluiu informações sobre suporte social e participação em atividades extracurriculares.
Resultados
A prevalência total de SB foi 57,5% entre os estudantes. Alta exaustão emocional foi observada em 33,1% (N = 38) dos alunos, alta despersonalização foi observada em 45,7% (N = 58) e 36,2% dos participantes (N = 46) apresentou reduzida realização pessoal. Indivíduos que participaram de serviços comunitários apresentaram menor frequência de alta despersonalização (razão de prevalência 0,61, intervalo de confiança 95% 0,42-0,88). A SB não apresentou associação com demais grupos de atividades extracurriculares ou com grupos de suporte social.
Conclusões
Foi observada alta prevalência de SB em internos de medicina, no entanto o comportamento de procura de suporte social não se associou com SB. Os internos que apresentavam participação em atividades extracurriculares comunitárias apresentavam menor frequência de alta despersonalização.
Similar content being viewed by others

Background
Burnout syndrome (BS) is highly prevalent among medical students and apparently it was first described by Herbert Freudenberger, a psychologist working with volunteers managing individuals with drug disorders [1,2,3,4]. However, there is evidence that 3 years before, air traffic controllers in United States used the term burnout for exhaustion related to work demands, resulting in decline of production [4].
BS is characterized by a model of emotional suffering regarding work demands and includes three categories of symptoms: emotional exhaustion (EE), depersonalization (DP) and reduced personal accomplishment (PA). EE is described as feeling emotionally depleted and include symptoms of fatigue, low energy and increased sensibility to external stressors. DP is described as negative feelings and perceptions about the patients, including the attempt to distance oneself from patients, resulting in cynicism, lower empathy and indifference. Low PA is characterized by the negative self-evaluation, loss of satisfaction, motivation and efficiency on work related activities [5, 6].
The 11th Revision of the International Classification of Diseases (ICD-11) describes burnout as a specifically occupational syndrome. It is described as chronic workplace stress not successfully managed, with three dimensions: feelings of energy depletion or exhaustion, increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job, and reduced professional efficacy [7].
Burnout syndrome has negative consequences in medical students´ health and is associated with suicidal ideation and psychiatric disorders [2]. Dyrbye et. al. evaluated 545 medical students and found 45% prevalence of BS using Maslach Burnout Inventory (MBI), 35% with high EE, 26% with high DP and 31% with low PA. They also found that 56% had positive depressive disorder screening, 22% had high risk alcohol use and 14.7% had binge drinking. Negative life events (divorce, personal illness, illness in a close family member and/or death) were associated with higher risk of BS (p = 0.016) [8]. Psychological distress (including BS) can also impact negatively on academic performance, and adversely affect the learning process and development of competences during medical training [3, 9,10,11]. BS is associated with lower empathy and worse professional climate among medical students. Brazeau et al. evaluated 127 medical students and found that individuals with higher scores of EE, DP and PA reported worse perception of professional climate (p < 0.01) and lower score of self-rated empathy [12].
BS is expected to be seen in up to half of all medical students during their undergraduate period, with the risk of persisting after graduation. A recent review of BS in medical students and residents using articles from 1990 to 2015 found that the prevalence of BS in medical students ranges from 45 to 56% among different populations, with a range of 35 to 45% of high EE and 26 to 38% of high DP [3]. A review of mental health problems in Brazilian medical students showed only three studies on this population with a pooled prevalence of 13.1% (confidence interval 95% 10.2–16.4) [13]. However, this study was conducted in initial years of the course and used different way to analyse data about BS. A Brazilian study in medical interns showed a 63.2% prevalence of high EE, 53.8% prevalence of high DP and 50.9% prevalence of low PA [14].
There is some evidence about protective factors of BS in medical students, as positive life events (marriage, birth or adoption), social support, extracurricular activities and physical activity [8, 15,16,17]. A cross-sectional Spanish study with health professionals found that individuals with higher and moderate self-esteem are associated with higher social support and empathy and lower frequency of BS [18]. Thompson et. al. found that medical students with lower perceived social support had higher rates of EE (p = 0.04) [15]. A good perceived social support can buffer stress related to academic workload or help the students to cope [19, 20] and seeking social support is seen as a functional strategy to cope with BS [21].
The association among BS and extracurricular activities is controversial, although there is evidence pointing to the protective effect of exercise [17, 22, 23]. Fares et. al evaluated medical students ́ extracurricular activities and found no association with BS, except for a protective factor with music related activities (p = 0.045) [22]. Almalki also found no association among extracurricular activities and BS (p = 0.33) [23]. Shadid et. al. did not observed an association between BS and extracurricular activities, however medical students that had none of the extracurricular activities evaluated had higher risk of high stress (Odds Ratio (OR) 1.89 CI 95% 1.23–2.91) [24]. The extracurricular activities could be viewed as an expression of autonomy, increasing students ́ motivation.
Medical undergraduate in Brazil is a six-year duration course because of the absence of pre-medical training on our local educational context. The internship encompasses the last 2 years of medical training in Brazil, with mainly workplace training (primary care, ambulatories and hospital settings). The aim of our study was to identify prevalence of BS during internship and its association with extracurricular activities and social support in one medical school in São Paulo, Brazil.
Methods
This was a cross-sectional study conducted at Faculdade de Ciências Médicas da Santa Casa de São Paulo, a traditional medical school from São Paulo (Brazil) during 2015. The population of interest were internship students (including medical students of 5th and 6th years). The eligibility criteria were to be an internship student during 2015. All the medical students attending internship were invited to participate. The participants were at different rotations (practice in Surgery, Pediatrics, Primary Care, Gynecology, Internal Medicine, Emergency, Orthopedics or Infectology). The students were contacted between July and November of 2015. The population of the internship students at Faculdade de Ciências Médicas da Santa Casa de São Paulo was composed by 216 individuals during 2015.
The students were evaluated regarding socio demographic data, extracurricular activities, self-rated social support and burnout syndrome. It was used the Maslach Burnout Inventory – Human Services for assessment of burnout syndrome, a validated instrument, with three subscales: Emotional Exhaustion; Depersonalization; Personal Accomplishment [5].
For the purposes of this study, the overall prevalence of BS was assessed by the presence of a high score on one or both the subscales EE and DP. High EE was defined by a subscale score on MBI of 27 or higher. DP was defined by a subscale score on MBI of 10 or higher. Low PA was defined as a subscale score of 34 or lower, but it is not included to compose overall prevalence of BS [5, 25,26,27]..
The extracurricular activities were combined in 4 categories: academic programs (which consists of involvement in research or being a part of a study group or participating in courses and academic leagues); political involvement (being a member from the student union or student representative at faculty and college administration meetings); volunteer and community services (to participate in activities or other groups that provide volunteer work) and athletic activities (member from the athletic association or athletic band).
Social support was evaluated by self-reported behaviour of seeking emotional support and with whom they would share their feelings and worries (family, friends outside medical school, friends from their rotation, friends from their school but from different years/rotations and/or with their romantic partner). Sociodemographic data were evaluated such as age, monthly household income (counted by minimum wages, equivalent to R$788,00 or U$252,56 by the time of data collection), parents ́ educational level, and ownership of research grants or scholarships.
Statistical analysis
The analysis included descriptive summary statistics (means and proportions) for demographic data, associated variables and prevalence of BS, EE and DP. Differences among individuals with overall BS, high EE and high DP were evaluated using Chi-square test (Fischer exact test, when indicated). The comparisons among categorical and continuous variables used ANOVA one-way test (for age). The prevalence ratio was calculated with Poisson Test (indicated when prevalence of independent variable higher than 20%) and its confidence intervals. The tests are two sided and were considered a type I error rate of 0.05 (alpha error < 0.05). Data were analysed with STATA/SE software version 13.1.
Ethical considerations
The study was submitted to the Ethics Board of Irmandade da Santa Casa de São Paulo and approved. The study protocol was approved under number CAAE 31151315.5.0000.5479 in March, 2015. All participants that were invited and agreed to participate in the research, signed the informed written consent.
Results
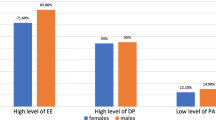
A total of 121 internship medical students agreed to participate and fully answered the questionnaires (56% participation rate). The participants were 68 (56.2%) male students and 53 (43.8%) female students, with similar mean age (25 years; p = 0.08) and monthly household income (p = 0.17). The sample was balanced among first and second year of internship individuals (45.5% of 1th year interns and 54.5% of 2th year interns; p = 0.44). Among men, 31.8% had research grants and the rate was 39.6% among women (p = 0.376). There were gender differences regarding scholarships, with higher frequency for female (54.7%) over male students (35.8%; p = 0.038). For participation on extracurricular activities, both genders had high frequency on academic programs (94.3% of students, p = 0.105). Concerning social support reported by the students, 88.7% of women reported to share their problems with their family, while 72.1% of men reported the same behaviour (p = 0.025) (Table 1). Male students also report lower frequency of seeking support from students in other rotations (p = 0.044). The prevalence of high emotional exhaustion was found in 33.1% (N = 38) of the participants, 45.7% (N = 58) had high depersonalization and 36.2% (N = 46) had low personal accomplishment (Table 1).
The ownership of research grant or scholarship had no association with EE, DP or low PA. The different categories of extracurricular activities didn’t have association with EE and low PA. Students with participation in community services had lower prevalence of high depersonalization (prevalence ratio (PR) 0.61, confidence interval 95% (CI 95%) 0.42–0.88) (Table 2). None of the characteristics of self-reported social support is associated with BS subscales (Table 2).
The burnout syndrome was defined as the presence of high emotional exhaustion and/or high depersonalization. The prevalence of BS does not differ among first and second year’s interns (PR 1.39 CI 95% 0.67–2.86). Neither household income, ownership of research grant, or scholarship was associated with overall BS prevalence. The involvement in extracurricular activities has no association with the overall BS prevalence, neither any subtype of self-related social support (Table 3).
Discussion
This study showed high prevalence of burnout syndrome among medical interns, affecting more than half of the participants (57.5%). The prevalence of high emotional exhaustion was 33.1% (N = 38), 45.7% (N = 58) of high depersonalization and 36.2% (N = 46) of low personal accomplishment. Students with participation in community services as an extracurricular activity had lower prevalence of high depersonalization (PR 0.61, CI 95% 0.42–0.88).
These results are consistent with some studies that found high prevalence of BS among medical students [28, 29]. Dyrbye et. al. evidenced that medical students were more likely to have burnout syndrome and depression than the general population [30]. A recent published meta-analysis including 24 studies and 17,431 medical students showed a prevalence of 44.2% (CI 95% 33.4–55.0%) of burnout syndrome, 40.8% of high EE (CI 95% 32.8–48.9%), 35.1% of high depersonalization (CI 95% 27.2–43.0%) and 27.4% of low PA (CI 95% 20.5–34.3%) [31].
The BS prevalence is similar to other Brazilian studies analysing the interns´ population, showing high levels of emotional exhaustion and depersonalization [14, 32]. The high prevalence of BS observed is concerning since it may also interfere with quality of patients´ care, especially with high depersonalization scores [33]. A recent study in Mexico published by Miranda-Ackerman et al. evaluated 176 interns and found prevalence of 43.1% of high EE, 53.9% of high DP and 34.6% of low PA [25].
There are several factors associated with the high prevalence of BS in internship. The internship has particular challenges compared to the early years as a medical undergraduate. Some are related to closer contact with patients´ suffering and deaths, what could cause students´ suffering and internal conflicts [34]. Another challenge is the organization of educational process for the workplace training, that is very different of the previous years of medical education. There are increase in responsibilities and demands to the students, greater hours in the workplace, increasing lack of sleep, frustration of working with time constrains, lack of ideal conditions to provide care, low motivated teams and eventually unprofessional attitudes, causing moral distress among students [35, 36].
In Brazilian medical education most of internship occurs within the Unified Health System (Sistema Único de Saúde), a public health system of primary, secondary and tertiary care services. Most Brazilian medical schools have partnerships with municipalities to work within these services. These arrangements introduce the opportunity to work with poverty and vulnerable groups, what could be an extra emotional challenge for students to cope with. Another factor associated with BS in health professionals are related to work organization. Management in health services with better work processes organization could influence on health professionals´ and medical students mental health [4].
There is a conceptual model of medical student well-being integrating the idea of coping reserve of each individual that includes negative and positive inputs. Dunn and colleagues suggested that negative inputs include stress, internal conflicts, time and energy demands. And positive inputs include psychosocial support, social and healthy activities, mentorship and intellectual stimulation. These inputs interact with personality traits and temperament factors, as resilience, changing the way that each individual perceive difficulties and demands [20].
Social support could have a protective effect for BS in medical students [16, 37]. Although this study found a difference of self-rated social support sought by women, which reported to rely more on family and partners than men, this not associated with BS. This study found high frequency of the behaviour of seeking social support, as 94.2% of students reported to rely on colleagues of the same rotation, 79.3% on family, 76.0% on friends within medical school (but different rotation), 74.2% on romantic partner and 68.6% on friends outside medical school. This could be explained by the questions used to evaluate social support or the lack of evaluation of quality or sufficiency of social support. Houpy et. al. evaluated medical interns and found that, after difficult clinical events, interns have the desire to talk about it in the same day (78.1%). Those who are comfortable to talk about stress and BS had higher resilience scores [38]. Despite the fact that some evidence shows that social support is an important coping mechanism against BS, there is no evidence in the data of present study that indicates the association of seeking social support and BS among the interns.
Being a medical undergraduate is emotionally challenging and one of the proposed buffers to mental suffering is healthy extracurricular activities, as music programs, theatre or physical activity [20]. The extracurricular activities can help or worsen the balance to maintain or achieve a better mental health status. This study observed high frequencies of participation in extracurricular activities related to medical students as 94.3% participated in academic programs, 85.1% in community programs and 47.9% in athletic activities. Individuals with participation in community services had lower prevalence of high depersonalization (PR 0.61, CI 95% 0.42–0.88). There is evidence that altruism is associated with happiness, better well-being and health, even longevity [39, 40]. Although we did not find studies with the exact same results in medical education, Dyrbye et. al. surveyed 4400 students from seven American medical schools and found that as mental health improves, students had more altruistic professional beliefs, as the desire to work with underserved populations [41]. Some possible explanations are that emotional exhaustion and fatigue related to BS could reduce the willingness to work in community services as an extracurricular activity, or the depersonalization could reduce the joy related to these activities. The students with BS could also perceive the workload as critical, reducing some extracurricular activities that are perceived as less important to entrance in residency programs. However, these possibilities are still underexplored in medical education literature.
Our study had some limitations. The response rate was lower than expected, although several studies had response rates similar to our study and lower than 70% [19, 24, 25]. The cross-sectional design had limitations to infer causality. It was not used a validated tool to analyse social support and it was not asked to the students in the present study if the social support were perceived as sufficient or not. The strengths of our study are the use of a validated questionnaire to evaluate BS and the population of interns in the initial approach. The focus on protective factors of BS and its subscales (social support and extracurricular activities) is recent in medical research. More studies with longitudinal design are needed to better understand the BS causality and its association with resilience training, medical schools ́ institutional social support programmes and educational climate.
Conclusions
The prevalence of burnout syndrome among Brazilian interns is high (57.5%). We found no association among BS and the behaviour of seeking social support among family, partners and other medical students. The prevalence ratio of high depersonalization was lower in interns that had community service extracurricular activity.
Availability of data and materials
The datasets generated during the current study are not publicly available due to the presence of individuals identification but are available from the corresponding author on reasonable request.
Abbreviations
- BS:
-
Burnout syndrome
- DP:
-
Depersonalization
- EE:
-
Emotional exhaustion
- ICD:
-
International Classification of Diseases
- MBI:
-
Maslach Burnout Inventory
- OR:
-
Odds Ratio
- PA :
-
Personal Accomplishment
- PR:
-
Prevalence Ratio
References
Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad Med. 2006;81(4):354–73..
Ishak W, Nikravesh R, Lederer S, Perry R, Ogunyemi D, Bernstein C. Burnout in medical students: a systematic review. Clin Teach. 2013;10(4):242–5.
Dyrbye LN, Shanafelt T. A narrative review on burnout experienced by medical students and residents. Med Educ. 2016;50:132–49.
Samra R. Brief history of burnout: we have much to learn from established countermeasures in aviation. BMJ. 2018;363:k5268. https://doi.org/10.1136/bmj.k5268.
Malasch C, Jackson SE, Leiter MP. Malasch burnout inventory manual. 3rd ed. Palo Alto: Consulting Psychologists Press; 1996.
Erschens R, Keifenheim KE, Heremann-Werner A, Loda T, Schwille-Kiuntke J, Bugaj TJ, et al. Professional burnout among medical students: systematic literature review and meta-analysis. Med Teach. 2018. https://doi.org/10.1080/0142159X.2018.1457213.
World Health Organization. Available on: https://www.who.int/mental_health/evidence/burn-out/en/. Assessed 27 Jan 2020.
Dyrbye LN, Thomas MR, Huntington JL, Lawson KL, Novotny PJ, Sloan JA, Shanafelt TD. Personal life events and medical student burnout: a multicenter study. Acad Med. 2006;81(4):374–84.
Stewart SM, Lam TH, Betson CL, Wong CM, Wong AM. A prospective analysis of stress and academic performance in the first two years of medical school. Med Educ. 1999;33:243.
Spiegel DA, Smolen RC, Jonas CK. An examination of the relationships among interpersonal stress, morale and academic performance in male and female medical students. Soc Sci Med. 1986;23:1157–61.
Maslach C, Schaufeli WB, Leiter MP. Job Burnout. Annu Rev Psychol. 2001;52(1):397–422.
Brazeau CMLR, Schroeder R, Rovi S, Boyd L. Relationships between medical student burnout, empathy, and professional climate. Acad Med. 2010;85:S33–6.
Pacheco JP, Giacomin HT, Tam WW, Ribeiro TB, Arab C, Bezerra IM, Pinasco GC. Mental health problems among medical students in Brazil: a systematic review and meta-analysis. Rev Bras Psiq. 2017;39:369–78.
De Abreu Santos ATR, Grosseman S, De Oliva Costa EF, De Andrade TM. Burnout syndrome among internship medical students. Med Educ. 2011;45(11):1146.
Thompson G, McBride RB, Hosford CC, Halaas G. Resilience among medical students: the role of coping style and social support. Teach Learn Med. 2016;28(2):174–82.
Jenkins TM, Kim J, Hu C, Hickernell JC, Watanaskul S, Yoon JD. Stressing the journey: using life stories to study medical student wellbeing. Adv in Health Sci Educ. 2018. https://doi.org/10.1007/s10459-018-9827-0.
Babenko O, Mosewich A. In sport and now in medical school: examining Students ́ well-being and motivations for learning. Int J Med Educ. 2017;8:336–42.
Molero Jurado MM, Pérez-Fuentes MC, Linares JJG, Martin ABB. Burnout in health professionals according to their self-esteem, social support and empathy profile. Front Psychol. 2018;9:424. https://doi.org/10.3389/fpsyg.2018.00424.
Chang E, Eddins-Folensbee F, Coverdale J. Survey of the prevalence of burnout, stress, depression, and the use of supports by medical students at one school. Acad Psychiatry. 2012;36:177–82.
Dunn LB, Iglewicz A, Moutier C. A conceptual model of medical student well-being: promoting resilience and preventing burnout. Acad Psychiatry. 2008;32:44–53.
Erschens R, Loda T, Hermann-Werner A, Keifenheim KE, Stuber F, Nikendel C, et al. Behaviour-Based Functional and Dysfunctional Strategies of Medical Students to Cope with Burnout. Med Educ Online. 2018;23:1535738.
Fares J, Saadeddin Z, Al Tabosh H, Aridi H, El Mouhayyar C, Koleilat MK, Chaaya M, El Asmar K. Extracurricular activities associated with stress and burnout in preclinical medical students. J Epidemiol Global Health. 2016;6:177–85.
Almalki SA, Almojali AI, Alothman AS, Masuadi EM, Alaqeel MK. Burnout and its association with extracurricular activities among medical students in Saudi Arabia. Int J Med Educ. 2017;8:144–50.
Shadid A, Shadid AM, Shadid A, et al. Stress, burnout, and associated risk factors in medical students. Cureus. 2020;12(1):e6633. https://doi.org/10.7759/cureus.6633.
Miranda-Ackerman RC, Barbosa-Camacho FJ, Sander-Moller MJ, Buenorostro-Jimenez AD, Mares-Pais R, et al. Burnout syndrome prevalence during internship in public and private hospitals: a survey study in Mexico. Med Educ Online. 2019;24:1593785.
Dyrbye LN, West CP, Shanafelt TD. Defining burnout as a dichotomous variable. J Gen Intern Med. 2009;24(3):440.
Thomas NK. Resident Burnout. JAMA. 2004;292:2880–9.
Dyrbye LN, Thomas MR, Massie FS, Power DV, Eacker A, Harper W, Durning S, Moutier C, Szydlo DW, Novotny PJ, Sloan JA, Shanafelt TD. Burnout and suicidal ideation among U.S. medical students. Ann Intern Med. 2008;149(5):334–41.
Parr JM, Pinto N, Hanson M, Meehan A, Moore PT. Medical graduates, tertiary hospitals, and burnout: a longitudinal cohort study. Ochsner J. 2016;16(1):22–6.
Dyrbye LN, West CP, Satele D, Boone S, Tan L, Sloan J, Shanafelt TD. Burnout among US medical students, residents, and early career physicians relative to the general US population. Acad Med. 2014;89(3):443–51.
Frajerman A, Morvan Y, Krebs MO, Gorwood P, Chaumette B. Burnout in medical students before residency. European Psychiatry. 2019;55:36–42.
Costa EF, Santos SA, Santos AT, Melo EV, Andrade TM. Burnout syndrome and associated factors among medical students: A cross-sectional study. Clinics. 2012;67(6):573–80.
Chen KY, Yang CH, Lien CH, Chiou HY, Lin MR, Chang HR, Chiu WT. Burnout, job satisfaction, and medical malpractice among physicians. Int J Med Sci. 2013;10(11):1471–8.
Marion R. The intern blues: the timeless classic about the making of a doctor. Perennial; 2001.
Monrouxe LV, Rees CE, Dennis I, Wells SE. Professionalism dilemmas, moral distress and the healthcare student: Insights from two online UK-wide questionnaire studies. BMJ Open. 2015;5:e007518. https://doi.org/10.1136/bmjopen-2014-007518.
Berger JT. Moral distress in medical education and training. J Gen Intern Med. 2013;29(2):395–8. https://doi.org/10.1007/s11606-013-2665-0.
Kim B, Jee S, Lee J, An S, Lee SM. Relationships between social support and student burnout: a meta-analytic approach. Stress Health. 2017:1–8. https://doi.org/10.1002/smi.2771.
Houpy JC, Lee WW, Woodruff JN, Pincavage AT. Medical students resilience and stressful clinical events during clinical training. Med Educ Online. 2017;22:1320187.
Post SG. Altruism, happiness, and health: It’s good to be good. Int J of Behav Med. 2005;12(2):66–77.
Borgonovi F. Doing well by doing good. The relationship between formal volunteering and self-reported health and happiness. Soc Sci Med. 2008;66:2321–34.
Dyrbye LN, Harper W, Moutier C, Durning SJ, Power DV, Massie S, Eacker A, Thomas MR, Salete D, Sloan JA, Shanafelt TD. A multi-institutional study exploring the impact of positive mental health on medical students´ professionalism in an era of high burnout. Acad Med. 2012;87(8):1024–31.
Acknowledgements
None.
Funding
MCPF and IPG had research grant for junior research investigation internship (PIBIC - CNPq).
DBL and AS had no funding.
Author information
Authors and Affiliations
Contributions
MCPF participated of data analysis and writing the manuscript. IPG analysed and interpreted the data and contributed to writing the final manuscript. AS participated in study design, data collection and data analysis. DBL participated in study design, data analysis and interpretation, and manuscript review. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was submitted to the Ethics Board of Irmandade da Santa Casa de São Paulo and approved. The study protocol was approved under number CAAE 31151315.5.0000.5479 in March, 2015. All participants that were invited and agreed to participate in the research, signed the informed written consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fontana, M.C.P., Generoso, I.P., Sizilio, A. et al. Burnout syndrome, extracurricular activities and social support among Brazilian internship medical students: a cross-sectional analysis. BMC Med Educ 20, 81 (2020). https://doi.org/10.1186/s12909-020-01998-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-020-01998-6