
Abstract
Background
Advances in genetics and genomics require that healthcare professionals manage and incorporate new technologies into the appropriate clinical practice. The aim of this study was to identify core competencies in genetics for non-geneticists, both physicians and non-physicians.
Methods
We performed a literature review by searching MEDLINE, SCOPUS, and ISI Web of Science databases to identify studies reporting competencies in genetics in terms of knowledge, attitudes and abilities for non-genetic healthcare professionals. Furthermore, we conducted a survey according to a modified Delphi method, involving genetics experts to evaluate the competencies to be included as items of the curricula.
Results
Three eligible documents were identified and 3 Delphi rounds were carried out to reach a consensus on the competencies to be incorporated in the curricula. With reference to the curriculum for physicians, 19 items were included in the knowledge domain, 3 in the attitudes and 10 in the abilities domain. We developed two different curricula for non-physicians: one specific for those working in genetic services (20 items in the knowledge domain, 3 in the attitudes and 12 in the abilities) and one for those not working in genetic services (10 items in the knowledge domain, 3 in the attitudes and 2 in the abilities).
Conclusions
We developed 3 curricula in genetics addressed to non-genetic healthcare professionals. They differ in the “knowledge” and “abilities”, while the “attitudes” are the same for all the healthcare professionals. Although some concerns about the generalizability of the findings could arise due to the Italian perspective, we envisage the curricula can be used for genetics educational programs in several contexts.
Similar content being viewed by others

Background
Over the last decades, new DNA sequencing technologies have been offered at increasingly reduced costs [1, 2]. This has led to a rapid spread of genetic tests utilization in the clinical practice [3]. The spread of this type of testing runs in parallel with an increasing inappropriateness that might be partly related to a lack of competencies of healthcare professionals that refer patients to genetic services [4,5,6]. Non-genetic healthcare providers themselves feel inadequately qualified to decide whether genetic testing is appropriate, to perform a genetic risk assessment and to interpret the genetic test results [7]. Khoury et al. highlighted to what extent the translation of genomics knowledge into clinical practice is a challenging phase of translational research [8]. Thus, the potential benefits of a genetic test can be affected by the lack of a proper education and training of non-genetic healthcare professionals [9].
In the Italian framework, different authors have reported the need to improve the genomic literacy of non-genetic healthcare workers [10,11,12] differentiating between physicians and non-physicians, since their careers are widely different in terms of educational programmes [13].
The predefinition of a set of core competencies is essential for the development of an educational programme [14]. A “competence” is made up of different aspects, including knowledge, relational attitudes and practical abilities [15, 16] and it is more complex than each single aspect as a standalone. In the educational context, the modifier “core” refers to that set of competencies that are identified as essential [17]. The definition of the core competencies for a certain professional category should be based on the assessment of educational needs, achievable through an appropriate reference to the existing evidence and through the involvement of an adequate group of experts [18, 19].
Our study was based on the hypothesis that a specific healthcare professional education is the first step for the appropriate implementation of genetics/genomics in clinical practice to guide decisions on prevention, diagnosis and treatment of patients. In this conceptual framework, our research aimed to identify the core competencies in genetics, developed in a curriculum-style structure, for both non-genetic physicians and non-physicians. As to the latter, we differentiated between healthcare professionals who work in genetic services and the others. An Italian perspective was adopted to develop these curricula. We targeted at those professionals operating in our healthcare system organization and excluded categories, like non-physician genetic counsellors, who do not operate in the Italian health system.
In order to achieve this goal, we performed a literature review to identify the potential competencies that may contribute to the core set. Afterwards, we conducted a survey according to a modified Delphi method, involving a group of genetics experts to evaluate the competencies to be included as items of the curricula.
Methods
Literature review
Search strategy and study selection
We searched the MEDLINE, SCOPUS and ISI Web of Science databases, including the following search terms: “genetics”, “genomics”, “health professional”, “healthcare professional”, “clinician”, “doctor”, “professional education”, “competence”, “continuing education”, “genetics curriculum”.
The search was limited to English or Italian written articles published from January 1st, 2007 to January 1st, 2018. We selected the year 2007 as the starting point of the search period because the Italian Task Force on Public Health Genomics was launched at the end of 2016, thereby underlying the importance of genetics and genomics education in the Italian context.
We performed an extensive cross-check of the references from the original studies using a snowball approach to find additional studies. Two investigators (AT and MBM) screened the records (titles and abstracts) that were taken into account for a full-text analysis in case they fulfilled the inclusion criteria. Any disagreements were resolved through discussion and review by a supervisor researcher (SB). The review was drafted in accordance with the PRISMA guidelines [20].
Inclusion and exclusion criteria
The inclusion criteria required that the articles reported: 1) set of competencies in genetics for graduated healthcare professionals; 2) set of competencies according to the three domains of theoretical knowledge, relational attitudes and practical abilities; 3) description of the methodology used to identify the competencies. Articles that reported curricula for categories of healthcare professionals that are not currently present in Italy, such as non-physician genetic counsellors, were excluded.
Data extraction
Qualitative data extraction was performed by two investigators (AT and MBM) who collected the following information from each article: name of the scientific society, publication year, country (if any) to which the article was referred, target professionals. We collected the competencies reported in the retrieved studies according to the three domains of theoretical knowledge, relational attitudes and practical abilities. We did not perform the quality assessment of the selected studies, since inclusion criteria were strict enough to avoid inclusion of low-quality reports.
Delphi process
We used a Delphi method to process the results from the literature review and select the competencies to include in the curricula. This method was originally developed in the 1950s by the Rand Corporation and mainly implemented by Dalkey and Helmer in 1963. It is a social science technique used in qualitative research to consult experts on a specific topic thanks to serial rounds of questionnaires. After the elaboration of data resulting in each round, a new set of questions is generated, and a new group report is created. This process is performed until a consensus is reached [21].
This approach has frequently been adopted in healthcare research and education to identify the competencies that professionals should acquire on the basis of experts’ judgement [19, 22, 23].
We adopted a modified Delphi process: we provided a base of competencies retrieved from the literature instead of asking the experts to propose them. In the first round, however, experts could propose new competencies. Thirty-seven healthcare professional experts of the Italian Network for Public Health Genomics (GENISAP) were involved in the Delphi process [24]. The GENISAP is a network created to connect Italian professionals with great knowledge and experience in the field of genetics and genomics. Invitations were sent via e-mail, with the description of the study and the assurance of anonymity of their participation in the study. Disclosure of conflicts of interest was requested to the participants. In order to increase the response rate, between the rounds a reminder was sent to the participants by e-mail.
The questionnaire was divided into three sections. The first section reported demographic information: age, gender, professional qualification, years of work experience in genetics, teaching experience in genetics. In the second section, participants were asked to approve or disapprove of the organization of the competencies into the three domains of knowledge, attitudes and abilities. The third section included all the specific items that had to be evaluated by the participants. Each item could be voted in the survey to be included in the curriculum for physicians, in the curriculum for non-physicians and/or in the curriculum dedicated to non-physicians working in genetic services.
In the first round the participants were asked to assess each item as “important”, “should be modified”, or “not important”. In an additional dedicated section, modifications or integrations of the items could be proposed. If at least 70% of the participants rated the item as “important”, the item would automatically be included in the curriculum. In the same way, if at least 70% of participants considered an item “not important”, it was automatically excluded. In the remaining cases, items were proposed again to be voted in the second round, along with the modifications proposed by the participants. Two authors (AT and MBM) evaluated all modifications suggested and integrated them into the items. In the second round, the original and the modified items were reported aligned for comparison and participants could vote “yes” or “no” for the inclusion of the modified items in the curricula. As in the first round, the threshold for inclusion was 70%.
Moreover, in the first round, participants could propose additional items, which were voted in the second round with the same system as the first round. In case of non-consensus, items were modified as suggested by the participants and voted again in the third round. In the third round the participants could vote “yes” or “no” for the inclusion of the modified items into the curricula, with a 70% consensus threshold. Since a consensus was reached among respondents, the third round was the last one. At the end of the survey, results were returned to the participants.
Fig. 1 reports the Delphi process steps along with a graphic illustration of the consensus definition.

Flowchart of the steps of the Delphi process
Results
Literature review
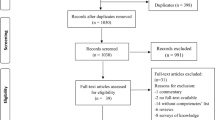
After removing duplicates, we identified a total of 4417 articles of which 4284 were excluded after title and abstract screening because not related to the research topic. The remaining 133 articles were assessed for eligibility and 131 were excluded because they did not meet the inclusion criteria. Figure 2 reports the flowchart of the bibliographic search strategy and the results.

Flowchart of the bibliographic strategy and results
Table 1 describes the main characteristics of the two studies selected through the literature review [17, 25] and of the document retrieved as a result of the snowball search [26]. These were the “Core Competencies in Genetics for Health Professionals in Europe” published by the European Society of Human Genetics (ESHG) [17], the “Core Competencies in Genetics for Health Professionals” published by the National Coalition for Health Professional Education in Genetics (NCHPEG) [25], and the “Learning outcomes in genetics and genomics for specialty trainees in non-genetic specialties” published by the UK National Health Service National Genetics and Genomics Education Centre (UK NHS NGGEC) [26].
The individual competencies from each of the three studies were unified into a single report and divided into the aforementioned three domains. The total number of the competencies was 33, of which 19 items for “knowledge”, 3 for “attitudes” and 11 for “abilities”. All these items were proposed for evaluation in the Delphi survey.
Delphi process
A total of 23 GENISAP members (62.2% out of 37 invited) participated in the first round, 21 (56.8%) in the second round and 12 (32.4%) in the third one. The participants of the first round, with a median age of 57 years (range 28–67), were 65.2% females and included 34.8% of geneticists, 34.8% of biologists, 17.4% of non-geneticist physicians and 13% of other healthcare professional categories. Most of the participants (78.3%) had a previous teaching experience in genetics. No disclosed conflicts of interest were reported by the experts. Figure 3 describes the results of the Delphi process.

Flowchart of the results of the Delphi process
The division into three domains (knowledge, attitudes and abilities) of the curricula structure was approved by 95.7% of the participants.
As to the curriculum for non-geneticist physicians, 30 out of the 33 items proposed were included after the first round. For the remaining 3, some modifications were proposed to be voted in the second round, after which only one was included. During the first round the participants proposed 3 new items, of which only one was included after the second round. Lastly, a total of 32 items were included in the curriculum for non-geneticist physicians: 19 concerning knowledge, 3 concerning attitudes and 10 concerning abilities (Table 2).
As to the curriculum for non-physicians, after the second round, the 33 items proposed were all considered applicable to non-physicians working in genetic services, while just 14 were considered applicable to those not working in genetic services. The 3 new items proposed by the participants were all included into the curriculum for non-physicians working in genetic services after the second round. After the third round, only one new item was modified and included in the curriculum for those not working in genetic services.
In conclusion, we had 15 items (10 of which on knowledge, 3 on attitudes and 2 on abilities) included in the curriculum for non-physician health professionals not working in genetic services, and 36 items included for non-physicians working in genetic services (21 knowledge, 3 attitudes and 12 abilities). Tables 3 and 4 report the complete curriculum for each of the two categories, respectively.
Discussion
The aim of our study was to elaborate three curricula containing essential competencies in genetics and genomics, targeted at health professionals not specialized in genetics, a key group still unaddressed as this area of knowledge and practice has been rapidly evolving. To achieve this goal, we performed a literature review in order to identify relevant competencies. Once identified, their inclusion in the three curricula was assessed through a Delphi survey involving Italian experts in the field of genetics and genomics, as participants. We used this procedure for the selection of the items, thanks to the advantages it offers: the anonymity of the Delphi survey prevents the participants from influencing each other; the controlled feedback on the group’s opinion allows the participants to modify the items and propose new ones during the subsequent rounds [21, 22, 27].
We compared the strengths and limitations of our method for identifying core competencies to those published in the literature [14, 19, 28, 29].
The approach chosen to develop these curricula was strengthened through the involvement of participants with a wide range of specialties: geneticists, biologists and physicians as most represented categories. The multidisciplinary composition of the panel was selected with the aim of limiting the risk of a “curriculum overload”, that means avoiding that the contents of the curriculum may be too many or too much specialized [28].
The structure of the curricula (divided into three domains of knowledge, attitudes and abilities) is consistent with other similar studies found in the international literature [14, 19, 29].
The Delphi process was chosen as the best methodology to assess the content of the curricula, similarly to analogous studies with the same aim [19, 29]. The response rate in the first round of our procedure (62.2%) was comparable with other studies that used similar invitation methods (e-mail, post) [19].
While similar studies used a “classical” Delphi methodology [19, 29], we adopted a “modified” Delphi methodology, since the contents of the survey were identified through a literature review. Another considerable difference consists in the target of the curricula: while many studies focused on a specific professional group (mainly on general practitioners) [19, 29], we addressed all healthcare professionals, differentiating the competencies for physicians and for the other healthcare professionals, with a specific distinction for those who work in genetic services. Thanks to this approach, these curricula can be easily incorporated in the post-graduate educational programmes of each professional category. The content of the “knowledge” domain may be taught as frontal or distance teaching lessons; the “abilities” might be transferred through problem-based clinical cases to be solved; the “attitudes” may be part of the ethics teaching contents.
It is remarkable that the three curricula widely differ in the “knowledge” and the “abilities”, while the “attitudes” are the same for every healthcare professional. In particular, physicians and non-physicians who work in genetic services are requested to have the same competencies, while the knowledge and abilities required for non-physicians not working in genetics services should be less detailed. On the other hand, items referring to attitudes were rated as “important” for all the healthcare professionals by the vast majority of participants in the first round, thus suggesting that the relational competencies are considered essential, without distinction as to the professional category.
The main limitation of our study concerns the generalizability of the findings, as we adopted an Italian health system perspective. This led to strict inclusion criteria for the review, excluding papers specifically referred to professional categories not operating in Italy, like non-physician genetic counsellors. These criteria were selected because the validation of the curricula had to be performed by members of the Italian Network for Public Health Genomics. Despite this limitation, we envisage that the outcome of our work, namely the curricula, may be adapted to any professional categories. A limitation may also be found in reaching a consensus during the Delphi process: while in the first round the response rate was 62.2%, in the third round it decreased to 32.4%. Another limitation concerns the selection of the survey participants: even if a multi-professional and multidisciplinary group was involved, only experts in genetics participated in the Delphi process. Lack of different perspectives could be addressed in the future by submitting the curricula to a wider target group for further validation and by involving non-experts in genetics and patient representatives.
Conclusions
We identified the contents of three curricula in genetics for non-genetic health professionals, differentiating those who work and who do not work in genetic services. These curricula are intended as an exhaustive and ready-to-use material for post-graduate courses about genetics/genomics. The implementation of these competencies in an educational programme is made feasible thanks to the structure of the curricula divided into the three mentioned domains.
The relevance of our results is related to the urgent need for improving the genetics/genomics literacy of healthcare professionals who are not specialized in genetics, as a possible response to the mainstream spread of this kind of knowledge and practice [30].
Abbreviations
- ESHG:
-
European Society of Human Genetics
- GENISAP:
-
Italian Network for Public Health Genomics
- NCHPEG:
-
National Coalition for Health Professional Education in Genetics
- UK NHS NGGEC:
-
UK National Health Service National Genetics and Genomics Education Centre
References
Ropers H. On the future of genetic risk assessment. J Community Genet. 2012;3(3):229–36. https://doi.org/10.1007/s12687-012-0092-2.
Wetterstrand KA. DNA sequencing costs: data. National Human Genome Research Institute (NHGRI) 2017. http://www.genome.gov/sequencingcostsdata. Accessed 22 Jan 2018.
GeneTests online Database Genetestsorg. 2017. http://www.genetests.org. Accessed 22 Jan 2018.
Marzuillo C, De Vito C, Boccia S, et al. Knowledge, attitudes and behavior of physicians regarding predictive genetic tests for breast and colorectal cancer. Prev Med. 2013;57(5):477–82. https://doi.org/10.1016/j.ypmed.2013.06.022.
Kotzer K, Riley J, Conta J, Anderson C, Schahl K, Goodenberger M. Genetic testing utilization and the role of the laboratory genetic counselor. Clin Chim Acta. 2014;427:193–5. https://doi.org/10.1016/j.cca.2013.09.033.
Wakefield E, Keller H, Mianzo H, Nagaraj CB, Tawde S, Ulm E. Reduction of health care costs and improved appropriateness of incoming test orders: the impact of genetic counselor review in an academic genetic testing laboratory. J Genet Couns. 2018:1–7. https://doi.org/10.1007/s10897-018-0226-8.
Mikat-Stevens NA, Larson IA, Tarini BA. Primary-care providers’ perceived barriers to integration of genetics services: a systematic review of the literature. Genet Med. 2015;17:169–76.
Khoury M, Gwinn M, Yoon P, Dowling N, Moore C, Bradley L. The continuum of translation research in genomic medicine: how can we accelerate the appropriate integration of human genome discoveries into health care and disease prevention? Genet Med. 2007;9(10):665–74. https://doi.org/10.1097/gim.0b013e31815699d0.
Kohane I. Ten things we have to do to achieve precision medicine. Science. 2015;349(6243):37–8. https://doi.org/10.1126/science.aab1328.
Mazzucco W, Ricciardi W, Boccia S. Addressing the gap between genetics knowledge and clinical practice: a pilot study to implement genetics education among physicians in Italy. Ital J Public Health. 2012. https://doi.org/10.2427/8673.
Boccia S. Why is personalized medicine relevant to public health? Eur J Pub Health. 2014;24(3):349–50. https://doi.org/10.1093/eurpub/cku030.
Michelazzo M, Pastorino R, Mazzucco W, Boccia S. Distance learning training in genetics and genomics testing for Italian health professionals: results of a pre and posttest evaluation. Epidemiol Biostat Public Health. 2015. https://doi.org/10.2427/11516.
Battista R, Blancquaert I, Laberge A, van Schendel N, Leduc N. Genetics in health care: an overview of current and emerging models. Public Health Genomics. 2012;15(1):34–45. https://doi.org/10.1159/000328846.
Guttmacher A, Porteous M, McInerney J. Educating health-care professionals about genetics and genomics. Nat Rev Genet. 2007;8(2):151–7. https://doi.org/10.1038/nrg2007.
Cobatrice Collaboration. Bion JF, Barrett H. development of core competencies for an international training programme in intensive care medicine. Intensive Care Med. 2006;32(9):1371–83. https://doi.org/10.1007/s00134-006-0215-5.
Collaborative CIH. A national Interprofessional competency framework. Cihcca. 2010; http://www.cihc.ca/files/CIHC_IPCompetencies_Feb1210.pdf. Accessed 22 Jan 2018.
Skirton H, Lewis C, Kent A, Coviello D. Genetic education and the challenge of genomic medicine: development of core competences to support preparation of health professionals in Europe. Eur J Hum Genet. 2010;18(9):972–7. https://doi.org/10.1038/ejhg.2010.64.
Jenkins J, Blitzer M, Boehm K, et al. Recommendations of core competencies in genetics essential for all health professionals. Genet Med. 2001;3(2):155–9. https://doi.org/10.1097/00125817-200103000-00011.
Burke S, Martyn M, Stone A, Bennett C, Thomas H, Farndon P. Developing a curriculum statement based on clinical practice: genetics in primary care. Br J Gen Prac. 2009;59(559):99–103. https://doi.org/10.3399/bjgp09x395094.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–12. https://doi.org/10.1016/j.jclinepi.2009.06.005.
Dalkey N, Helmer O. An experimental application of the Delphi method to the use of experts. Manag Sci. 1963;9:458–67.
Hsu C, Sandford B. The Delphi technique: making sense of consensus. Pract Assess Res Eval 2017;12(10). http://pareonline.net/getvn.asp?v=12&n=10. Accessed 22 Jan 2018.
Jünger S, Payne SA, Brine J, Radbruch L, Brearley SG. Guidance on conducting and REporting DElphi studies (CREDES) in palliative care: recommendations based on a methodological systematic review. Palliat Med. 2017;31(8):684–706. https://doi.org/10.1177/0269216317690685.
Boccia S, Ricciardi W. Challenges for the Italian public health genomics task force. Ital J Public Health. 2006;3:113–4.
Carroll JC, Rideout AL, Wilson BJ, et al. Genetics education for primary-care providers: improving attitudes knowledge and confidence. Can Fam Physician. 2009;55:e92–9.
NHS National Genetics and Genomics Education Centre. Learning outcomes in genetics and genomics for specialty trainees in non-genetic specialties. 2015. http://www.geneticseducation.nhs.uk. Accessed 22 Jan 2018.
Hentges K, Hosokawa M. Delphi: group participation in needs assessment and curriculum development. J Sch Health. 1980;50(8):447–50. https://doi.org/10.1111/j.1746-1561.1980.tb03126.x.
Midlöv P, Höglund P, Eriksson T, Diehl A, Edgren G. Developing a competency-based curriculum in basic and clinical pharmacology - a Delphi study among physicians. Basic Clin Pharmacol Toxicol. 2015;117(6):413–20. https://doi.org/10.1111/bcpt.12436.
Houwink E, Henneman L, Westerneng M, et al. Prioritization of future genetics education for general practitioners: a Delphi study. Genet Med. 2012;14(3):323–9. https://doi.org/10.1038/gim.2011.15.
Ricciardi W, Boccia S. New challenges of public health: bringing the future of personalised healthcare into focus. Eur J Pub Health. 2017;27(4):36–9. https://doi.org/10.1093/eurpub/ckx164.
Acknowledgements
We would like to thank the GENISAP group for taking part to the Delphi process.
Funding
This work is supported by the Personalized Prevention of Chronic DIsesase (PRECeDI) project (Marie Skłodowska-Curie Research and Innovation Staff Exchange – RISE, Contract number: 645740) and by the Italian Center for Disease Control (Centro Nazionale per il Controllo delle Malattie CCM) of the Italian Ministry of Health within the project titled “Provide tools for innovation of the healthcare system based on the use of genomic knowledge and on personalized medicine” (Project reference n. (CUP): J52F16000300001). The role of the funding bodies regards the publication of the manuscript.
Availability of data and materials
All data generated or analysed during this study are included in this published article. Additional information is available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
SB conceived the study and AT, MBM participated in its design. AT and MBM identified the studies through a search of online databases and performed the data extraction from the papers. SB, AF, WR supervised AT and MBM. SB, WR, AF, AT, MBM critically discussed and interpreted the results of the review. SB, AT and MBM conceived and performed the Delphi survey. SB, WR, AF, AT, MBM critically discussed and interpreted the results of the Delphi rounds and built the final curricula. All authors drafted and critically reviewed this manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Tognetto, A., Michelazzo, M.B., Ricciardi, W. et al. Core competencies in genetics for healthcare professionals: results from a literature review and a Delphi method. BMC Med Educ 19, 19 (2019). https://doi.org/10.1186/s12909-019-1456-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-019-1456-7