
Abstract
Background
Down syndrome (DS), a most frequently occurring genetic disorder, is associated with oral morphological abnormalities and higher incidence rates of oral diseases. Recent studies have analyzed the oral microbiome to elucidate their relationships with oral diseases and general health; however, reports on the oral microbiome in individuals with DS are scarce. This study aimed to characterize the oral microbiome in children with DS.
Methods
A total of 54 children aged 1–13 years were enrolled in this case-control study. Of these children, 27 had DS (Case: DS group) and 27 were age-matched healthy children (Control: ND group). Saliva in the oral cavity was collected with a swab, cultured, and tested for cariogenic and periodontopathic bacteria by quantitative polymerase chain reaction (qPCR) detection, and the salivary microbiome was analyzed using next-generation sequencing. The student’s t-test, Fisher’s exact test, Mann–Whitney U test, and permutational multivariate analysis of variance were used for statistical analysis.
Results
Results of culture and qPCR detection tests for cariogenic and periodontopathic bacteria showed no significant differences in the detected bacteria between the DS and ND groups, with the exception of a significantly higher detection rate of Candida albicans in children with DS with mixed dentition. A comparison of the salivary microbiomes by 16S sequencing showed no significant difference in α diversity; however, it showed a significant difference in β diversity. Children with DS had a higher relative abundance of Corynebacterium and Cardiobacterium, and lower relative abundance of TM7.
Conclusions
This study provided basic data on the salivary microbiome of children with DS and showed the microbiological markers peculiar to children with DS. However, further research to identify the relationship with oral diseases is warranted.
Similar content being viewed by others

Background
Down syndrome (DS), also known as trisomy 21, is the most common congenital genetic disorder as well as the most common cause of cognitive disorder in humans that affects approximately 12.6 in 10,000 births in the United States (2006–2010) [1], and 12.3 in 10,000 births in England (2013) [2]. The reported incidence in Japan is 22.6 per 10,000 births according to a 2016 survey, which is approximately twice as high as the incidence rates in Western nations [3]. Regarding dental traits, DS is characterized by abnormal shapes or number of teeth, such as congenitally missing, peg-shaped, conic teeth, or teeth with short roots [4,5,6]. Furthermore, it has been reported that subjects with DS develop periodontal diseases early and have a rapid progression, and conversely, they have fewer dental caries [7, 8].
Periodontal diseases and dental caries are both bacterial infections, and many previous microbiological studies using methods, such as culturing, polymerase chain reaction (PCR), and DNA–DNA hybridization, have reported differences between subjects with DS and healthy individuals in periodontal pathogens and Streptococcus mutans colonization in the oral cavity [9,10,11].
Recent studies have reported that dental caries and periodontal diseases are bacterial infections caused by S. mutans and the “red complex” as keystone pathogens and associated dysbiosis of the oral microbiome [12,13,14]. Furthermore, advances in 16S high-throughput sequencing have allowed for exhaustive analysis of the microbiome, which has also led to a wealth of new studies on the relationship between localized diseases and general health.
Studies of Down syndrome have also reported a comparisons of microbiomes found in the gut and oral rinse samples between adults with DS and non-DS controls have been reported [15, 16].
The oral cavity is almost sterile at birth. Different oral bacteria are known to colonize and continue to evolve depending on various factors, such as host and environmental factors, including vertical transmission. In particular, S. mutans infection that occurs between 19 and 31 months after birth, also known as the “window of infection,” is associated with the onset of dental caries [17].
Moreover, diversity of the oral microbiome is known to grow rapidly with tooth eruption, and it is reported that the microbiome on the dorsal surface of the tongue or in the subgingival plaque stabilizes in around 2 years [18, 19]. However, some other reports have documented that the oral microbiome continues to evolve after 2 years of age [20, 21], thereby leaving many unanswered questions. Colonization of strictly anaerobic gram-negative bacteria, which particularly have strong associations with periodontal disease, is believed to increase with age up until puberty.
Researching the characteristics of the oral microbiome from infancy to childhood is thus important for understanding the microbiome forming process in DS. This case-control study compared the differences in salivary microbiomes between children with and without Down syndrome by detecting the pathogenic microorganisms using culture and quantitative PCR methods and high-throughput sequencing.
Methods
Participants and ethical review
The participants of this case-control study were children with Down syndrome who lived in Tokyo and were recruited from the Lion Foundation for Dental Health Tokyo Dental Clinic. Twenty-seven children who met the inclusion criteria were included in the study as case group patients. The 27 age-matched healthy controls enrolled were recruited among 15 pupils of a nursery school in Tokyo and 138 students of an elementary school also in Tokyo. The enrolled participants were further divided into children in the primary dentition (PD) and mixed dentition (MD) to form four groups (Table 1).
Children with standard trisomy 21 were selected for this study, and children who took antibiotics within 7 days were excluded; however, complications of DS were not listed in the exclusion criteria.
This study was approved by the ethics committee of the Japanese Society for Oral Health and was conducted according to their guidelines (Approval no.: 27-4, 27-9). This study was conducted from January 2016 to May 2017, and written informed consent was obtained from the parents of all participants.
Salivary collection and questionnaire survey
Saliva in the oral cavity was collected using SalivaBio Infant's Swab (SIS: Salimetrics, Carlsbad, CA). The SIS was then washed in 2 mL of sterilized saline solution (Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan) and collected, and the aliquot was centrifuged at 16,400 g for 3 min to obtain the bacterial pellet. Saliva was collected at least 1 h after tooth brushing, eating, or drinking. Before collection of saliva, the parents of the participants were asked to fill out a questionnaire in order to survey the oral hygiene habits of the participants. The oral cavity was inspected for the number of erupted teeth, but parameters such as the severity of plaque or gingival inflammation were not assessed.
DNA extraction
DNA was extracted from the bacterial pellet using nexttec™ 1-Step DNA Isolation Kit (nexttec Biotechnologie GmbH, Leverkusen, Germany) according to the manufacturer’s instructions, and stored at − 40 °C until it was used for quantitative PCR or next-generation sequencing analysis.
Quantification of cariogenic and periodontopathic bacteria
Cariogenic and periodontopathic bacteria (Streptococcus mutans, Streptococcus sobrinus, Prevotella intermedia, Tannerella forsythia, Treponema denticola, and Porphyromonas gingivalis) were measured by quantitative PCR. Premix Ex Taq™ Probe qPCR (Takara Biomedicals, Shiga, Japan) was used, and 1 μL of the template DNA was amplified in a 20-μL system containing the 200 nM probe and primer set [22, 23] (Additional file 1). The cariogenic and periodontopathic bacterial DNA samples used for creating the standard curve were extracted from S. mutans ATCC25175, S. sobrinus ATCC33478, P. intermedia ATCC25611, T. forsythia ATCC43037, T. denticola ATCC35405, and P. gingivalis ATCC33277.
Amplification in PCR with CFX Connect™Real-Time PCR Detection System (Bio-Rad Laboratories, Hercules, CA) was performed under the following conditions: initial denaturation at 95 °C for 30 s, followed by 40 cycles at 95 °C for 15 s, at 58 °C for 30 s, and at 72 °C for 30 s.
Results were analyzed with CFX Manager™ Ver.2.1 software (Bio-Rad Laboratories) and the bacterial count was calculated using the calibration curve created with type strains, wherein ≥ 2 × 102 cells/swab was considered positive.
Candida albicans was detected by culture. BD CHROMagar™ Candida medium plates (Becton, Dickinson and Company, Sparks, MD) by a smear of 200 µL of collected and serially diluted SIS, cultured for 3 days in an aerobic condition at 37 °C, and the colony forming units were calculated from the count of grown colonies to find the count of C. albicans per the total bacterial count.
16S sequencing
16S rRNA sequencing was performed using universal primers (27Fmod and 338R) [24, 25]. Specifically, Ex Taq polymerase (Takara Bio, Shiga, Japan) was used to amplify approximately 20 ng of template DNA with Veriti Thermal Cycler (Life Technologies Japan, Tokyo, Japan) under the following cycling conditions: initial denaturation at 96 °C for 2 min, followed by 25 cycles at 96 °C for 30 s, at 55 °C for 45 s, and at 72 °C for 1 min.
The PCR product was purified with AMPure XP magnetic purification beads (Beckman Coulter, CA, USA) and quantified with Quant-iT PicoGreen dsDNA Assay Kit (Life Technologies Japan). After quantification, mixed samples were prepared by pooling approximately equal amounts of each amplified DNA. Samples were sequenced using a MiSeq Reagent Kit V3 (300 × 2 cycles) and a MiSeq sequencer (Illumina, CA, USA), according to the manufacturer’s instructions.
Data processing
An analysis pipeline was used for processing the 16S rRNA gene V1–V2 region, as previously reported [26, 27]. Briefly, after multiplexed sequencing of the 16S amplicons, sequences were assigned to samples based on their barcode sequences. Reads with an average quality value < 25, inexact matches to both universal primers, and possible chimeric reads were eliminated. Among high-quality reads, 3,000 reads per sample were randomly chosen and used for the comparative microbiome analysis. We sorted selected reads with the average quality value and grouped them into operational taxonomic units (OTUs) using the UCLUST (v.5.2.32) algorithm with a 97% identity threshold [28]. Taxonomic assignments for each OTU were made by similarity searching against publicly available 16S database using the GLSEARCH program (v.36.3.8 g). The 16S database was constructed from three publicly available databases [29]: Ribosomal Database Project v.10.31, CORE (http://microbiome.osu.edu/ (31 January 2017, date last accessed)), and the reference genome sequence database obtained from the NCBI FTP site (ftp://ftp.ncbi.nih.gov/genbank/ (December 2011, date last accessed)). For assignment at the genus and species levels, sequence similarity thresholds of 96% and 97% were applied, respectively [28]. All high-quality 16S V1–V2 sequences were submitted to the DDBJ/EMBL/GenBank database (Accession number DRA012575).
Data analysis
The student’s t-test and Fisher’s exact test were used for the analysis of the results of the questionnaire survey and detection rates of the pathogenic bacteria. The Mann–Whitney U test was used for comparisons of diversity and ratios of component bacteria at the genus and species levels.
The principal coordinate analysis (PCoA) was used to visualize similarities/dissimilarities in microbiome structures from the UniFrac Distance [30]. A permutational multivariate analysis of variance (PERMANOVA) was conducted to compare overall microbiome structures.
Differences at p < 0.05 were considered statistically significant. All analyses were performed using R software program (v3.4.3).
Results
After excluding 2 individuals who met the exclusion criteria, the sample size of the DS group was 27 and that of the age-matched controls (ND) was 27, so these 54 individuals were ultimately enrolled in this study.
As shown in Table 1, the 27 participants comprised 12 participants in the PD group and 15 in the MD group, and DS-ND comparisons were made separately in the PD and MD groups. Children who received any antibiotics within the last 7 days were excluded from this study; however, complications of DS were not included in the exclusion criteria. In the PD and MD groups, 8/12 and 10/15 children, respectively, had complications related to DS; in both groups, the most common complication was heart disease, which affected 6/12 and 7/15 of children with PD and MD, respectively.
There were no differences in the participants’ characteristics with regards to age, sex, or the number of teeth. No significant differences were found in questionnaire survey results on oral hygiene in the PD group. The MD group had similar results, except for the percentage of children having “oral hygiene practiced by the parents,” which was significantly higher in the DS group (Table 1).
We collected the saliva samples of 27 children with DS and 27 age-matched children without DS and compared cariogenic and periodontopathic bacteria as well as the salivary microbiome. Salivary cariogenic and periodontopathic bacteria were detected by quantitative PCR. In the PD group, the detection rates of these pathogenic bacteria were low; S. mutans, P. intermedia, T. forsythia, and T. denticola were detected in only 1–2 children with DS, while none of the pathogenic bacteria were detected in the ND group. While detection rates of pathogenic bacteria in the MD group were higher than those in the PD group, S. sobrinus and P. gingivalis were not detected. There were no differences between the children with and without DS in terms of other detected pathogenic bacteria. However, among children with DS, the detection rate for C. albicans by culture was significantly higher in the MD group (Table 2).
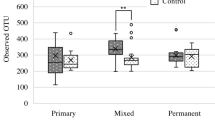
Salivary bacterial microbiomes were compared by high-throughput sequencing. No significant differences were observed between the children with DS and ND in the detected OTU count or Shannon’s diversity index in the PD or MD group (Fig. 1).

Salivary microbiome α diversity of children with and without DS. Panels a and b show the OTU counts of detected bacteria. Panels c and d are box plots of the Shannon index. Panels a and c compare the primary-dentition stage between children with DS and ND, while panels b and d compare mixed-dentition stage between children with DS and ND. The Mann–Whitney U test was performed for statistical analysis. p < 0.05 was considered statistically significant. DS: Down syndrome, ND: Non-Down syndrome, NS: Not Significant
Figure 2 displays the results of comparison of similarities/dissimilarities in salivary microbiome between children with DS and ND of the PCoA plot from the UniFrac Distance.

Principal coordinate analysis of microbiome structures in the saliva of children with and without DS. Panels a and c represent results based on Unweighted UniFrac Distance, while panels b and d show results based on Weighted UniFrac Distance. Panels a and b are the data in children with PD stage, and panels c and d are the data in children with MD stage. Samples of children with DS and ND are shown as red and blue dots, respectively. Statistical analyses were performed by permutational multivariate analysis of variance. DS: Down syndrome, ND: Non-Down syndrome, PD: primary dentition, MD: mixed dentition
Furthermore, PERMANOVA test showed significant differences in salivary microbiomes in the PD group in weighted and unweighted distances (p = 0.003, 0.032). Similarities in the microbiome in the MD group were more noticeable in unweighted and weighted distances (p < 0.001).
Figure 3 displays the top 30 genera composing the salivary microbiome of children with DS and ND in the PD and MD stages. Significant differences between children with DS and ND were observed for four genera in the PD group; the relative abundance values of Gemella, Corynebacterium, and Cardiobacterium were significantly higher in DS, and that of TM7 was significantly lower in DS.

Bacteria composing salivary microbiomes in children with DS and ND (at the genus level). The mean abundance of the top 30 genera composing salivary microbiomes are compared between the group of children with DS and the ND group. The mean abundance (%) in a the PD stage and b the MD stage are presented. The Mann–Whitney U test was performed. Genera in red font were significantly more abundant in DS, and genera in blue font were significantly less abundant in DS (*p < 0.05, **p < 0.01). DS: Down syndrome, ND: Non-Down syndrome, PD: primary dentition, MD: mixed dentition
Among the top 30 genera, significant differences were observed for 14 genera in the MD group. In addition to genera Corynebacterium and Cardiobacterium mentioned above, eight total genera including Abiotrophia, Lautropia, and Capnocytophaga were also significantly more abundant in DS, whereas a total of six genera including Prevotella, Actinomyces, Veillonella, and TM7 mentioned above were significantly less abundant in children with DS in the MD stage.
Figures 4 and 5 present the bacterial species of which abundance was ≥ 0.3% and differed significantly between children with DS and ND (p < 0.05). Significant differences were observed for 13 bacterial species in the PD group and for 32 species in the MD group. Gemella haemolysans, Neisseria elongata, Rothia aeria, and Rothia dentocariosa were significantly more abundant in children with DS in both the PD and MD groups. Meanwhile, some Actinomyces sp. were less abundant in children with DS.

Species level of salivary microbiomes between children with DS and ND (PD stage). The mean abundance (± SD) of 13 species that showed ≥ 0.3% abundance and significant differences. p < 0.05% in the Mann–Whitney U test was considered statistically significant. DS: Down syndrome, ND: Non-Down syndrome, PD: primary dentition

Species level of salivary microbiomes between children with DS and ND (MD stage). The mean abundance (± SD) of 32 species that showed ≥ 0.3% abundance and significant differences. p < 0.05% in the Mann–Whitney U test was considered statistically significant. DS: Down syndrome, ND: Non-Down syndrome, MD: mixed dentition
Discussion
This study compared the salivary microbiomes of children with and without DS aged 1–13 years, which is considered the crucial period for microbiome formation.
Amano et al. and Sakellari et al. detected periodontopathic bacteria in 2- to 13-year-old and 8- to 28-year-old subjects with DS, respectively, using quantitative PCR and DNA–DNA hybridization, respectively. They reported that these bacteria were detected earlier in subjects with DS than in healthy subjects [9, 10]. With regards to cariogenic bacteria, Scalioni et al. [11] tested for S. mutans in the saliva of 3- to 12-year-old children with in situ hybridization, and reported lower detection rates of the species in children with DS than in healthy children.
This study collected the saliva of 27 children with DS and age-matched controls to test salivary cariogenic and periodontopathic bacteria in these samples using quantitative PCR, and found low detection rates of these pathogens in children with PD (aged 1–4 years), and no differences in detection rates between DS and ND in the MD stage (aged 6–12 years) (Table 2).
Studies to date have measured periodontopathic bacteria in the subgingival plaque, whereas this study tested them in saliva; this difference may explain why we did not observe a difference because of a lower detection rate of the red complex, which are composed of strictly anaerobic bacteria. Moreover, rates of colonization of cariogenic bacteria in children in Japan have recently decreased because of the increase in awareness of the importance of oral hygiene [31]; this may have played a role in the difference between the findings of this study and those of the previous studies.
The comparison of bacterial microbiome by 16S rRNA high-throughput sequencing did not reveal any difference between DS and ND in α diversity of the microbiomes in both PD and MD groups; however, a significant difference was observed in β diversity as shown on the PCoA plot (Figs. 1 and 2).
In both PD and MD groups, Corynebacterium and Cardiobacterium were dominant and TM7 was less abundant among the bacterial genera composing the microbiome in DS. Moreover, there were more genera with significant DS-ND differences in the MD stage than in the PD stage, suggesting that the DS-ND differences in salivary microbiomes may widen with age.
Willis et al. [16] collected the oral rinse samples from individuals with DS aged 7–55 years for a comparison of the microbiome with healthy controls, and reported that the genera Kingella, Staphylococcus, Gemella, Cardiobacterium, Rothia, and Actinobacillus were more abundant, and Alloprevotella, Atopobium, Candidatus, and Saccharimonas were less abundant in DS.
The results of this study also showed higher abundance of Cardiobacterium in children with DS in both the PD and MD groups, suggesting that the dominance of Cardiobacterium is a characteristic of the oral microbiome of DS from a very early stage.
At birth, the oral cavity is practically sterile, while bacterial flora develops under the influence of factors and events, such as mode of delivery, breast or bottle feeding, eruption of tooth, introduction of solids, and oral hygiene status [32, 33]. Among them, the oral hygiene status is one of the major factors of dental caries and onset of periodontal diseases as well as microbiome formation [34].
There are several limitations to this study related to insufficient data collection. First, we could not obtain clinical indices, such as the Oral Hygiene Index and the Gingival Index, and we were unable to study the relationships with the degree of dental plaque accumulation or gingival inflammation. However, the results of the questionnaire survey showed no major differences in the number of teeth or oral hygiene habits (Table 1), suggesting that the differences in the oral microbiome between children with and without DS are primarily due to differences in their oral environments, including salivary properties.
Many characteristics of the saliva of individuals with DS have been reported, including low secretion, increased oxidative stress, increased secretory IgA, and abnormality of inorganic salts [35,36,37,38,39], and all these factors are likely to affect the salivary microbiome [40, 41].
Effects of decreased salivary secretion on the oral microbiome have been discussed in the context of Sjögren’s syndrome and side effects of radiotherapy and drug therapies [42,43,44]. Such studies have commonly reported higher detection rates of Lactobacilli and C. albicans; however, the present study showed a low detection rate of Lactobacilli and no significant difference between children with DS and ND group. In DS group, the observed high detection rate of C. albicans was consistent with the findings of the previous studies.
Overexpression of the superoxide dismutase gene encoded on chromosome 21 has been reported to cause overproduction of hydrogen peroxide and associated hydroxy radicals in subjects with DS than in healthy individuals [45], and accordingly, oxidative stress marker levels in their saliva have been reported to be higher compared to those in healthy individuals [35, 36]. Furthermore, hydrogen peroxide produced by some bacterial species in the genus Streptococcus in the oral cavity are known to affect the surrounding microbiome, and hydrogen peroxide produced by S. sanguinis inhibits S. mutans colonization [46, 47]. Such increased oxidative stress in the saliva may indeed have an effect on the microbiome.
Among the bacterial species found at significantly higher abundance in children with DS in both PD and MD groups, Neisseria elongate, Rothia aeria, and Rothia dentocariosa are catalase-positive bacteria, except Gemella haemolysans [48]. These bacteria are known to show resistance to high oxidative stress environments and may be a factor of dysbiosis in the salivary microbiome of the group of children with DS. Moreover, the aforementioned C. albicans also has a catalase gene, which may similarly explain their higher abundance in the DS group.
Dental plaque is formed through cell to cell interactions between bacteria from initial colonizers to the late colonizers in the oral cavity [49], and dental plaque adapted to the environment are known to develop in the supragingival and subgingival plaque [50, 51].
Khocht et al. [52] studied 40 bacterial species in the subgingival plaque of adults with DS using checkerboard DNA–DNA hybridization. They reported that Streptococcus sp. (i.e., S. oralis, S. mitis, and S. gordonii), which are initial colonizers, were more abundant in adults with DS than in healthy individuals. S. sanguinis, an initial colonizer, was also significantly more abundant in our participants with DS in the MD stage. These Streptococcus bacteria are known to be particularly important in the initial stage of dental plaque formation, and their differences in saliva are thus likely to influence the constituents in subsequent dental plaque formation.
Xiao et al. [53] analyzed supragingival dental plaque in adult patients with dental caries using 16S pyrosequencing and have reported the characteristic presence of Cardiobacterium and Corynebacterium bacteria in participants without dental caries. Janem et al. [54] studied the salivary microbiome of obese children with and without type 2 diabetes and have shown that Lautropia, Corynebacterium, and Cardiobacterium bacteria were detected in association with gingivitis.
In this study, the genera Corynebacterium and Cardiobacterium were dominant in the saliva of children with DS in the PD and MD stages, and the genus Lautropia was dominant in children with DS in the MD stage. The observed differences in salivary microbiomes, including the aforementioned differences in Streptococcus sp. affect the composition of plaque bacteria and may be associated with the onset of dental caries or periodontal diseases.
These findings suggest that the distinct characteristics of the salivary microbiome in subjects with DS from that in healthy individuals may be attributable to several factors; however, we were not able to measure the amount of salivary secretion or oxidative stress status in this study. Moreover, complications of DS or history of antibiotic administration within 1 week of specimen sampling can also affect the salivary microbiome [55], thus these factors should also be analyzed in future studies to get a better understanding of the dysbiosis of the salivary microbiome in DS. Furthermore, associations between the development of dental caries, periodontal diseases, and bacteria constituting dental plaque in the affected sites in subjects with DS should also be analyzed.
Conclusions
In conclusion, qPCR and high-throughput sequencing provided basic data on the salivary microbiome in DS and revealed dysbiosis in the salivary microbiome in children with DS when compared with that in children without DS.
Availability of data and materials
The reported nucleotide sequence data are available in the DDBJ Sequenced Read Archive under the accession numbers DRA012575.
Abbreviations
- DS:
-
Down syndrome
- MD:
-
Mixed dentition
- ND:
-
Non-Down syndrome
- OUT:
-
Operational taxonomic unit
- PCoA:
-
Principal coordinate analysis
- PCR:
-
Polymerase chain reaction
- PD:
-
Primary dentition
- PERMANOVA:
-
Permutational multivariate analysis of variance
References
de Graaf G, Buckley F, Skotko BG. Estimates of the live births, natural losses, and elective terminations with Down syndrome in the United States. Am J Med Genet A. 2015;167A:756–67.
Doidge JC, Morris JK, Harron KL, Stevens S, Gilbert R. Prevalence of Down’s syndrome in England, 1998–2013: comparison of linked surveillance data and electronic health records. Int J Popul Data Sci. 2020;5:1157.
Sasaki A, Sago H. Equipoise of recent estimated Down syndrome live births in Japan. Am J Med Genet A. 2019;179:1815–9.
Hennequin M, Faulks D, Veyrune JL, Bourdiol P. Significance of oral health in persons with Down syndrome: a literature review. Dev Med Child Neurol. 1999;41:275–83.
Descamps I, Marks LA. Oral Health in children with Down syndrome: parents’ views on dental care in Flanders (Belgium). Eur J Paediatr Dent. 2015;16:143–8.
Shukla D, Bablani D, Chowdhry A, Thapar R, Gupta P, Mishra S. Dentofacial and cranial changes in down syndrome. Osong Public Health Res Perspect. 2014;5:339–44.
Cichon P, Crawford L, Grimm WD. Early-onset periodontitis associated with Down’s syndrome–a clinical interventional study. Ann Periodontol. 1998;3:370–80.
Deps TD, Angelo GL, Martins CC, Paiva SM, Pordeus IA, Borges-Oliveira AC. Association between dental caries and Down syndrome: a systematic review and meta-analysis. PLoS ONE. 2015;10:e0127484.
Amano A, Kishima T, Kimura S, Takiguchi M, Ooshima T, Hamada S, Morisaki I. Periodontopathic bacteria in children with Down syndrome. J Periodontol. 2000;71:249–55.
Sakellari D, Arapostathis KN, Konstantinidis A. Periodontal conditions and subgingival microflora in Down syndrome patients. A case-control study. J Clin Periodontol. 2005;32:684–90.
Scalioni F, Carrada C, Machado F, Devito K, Ribeiro LC, Cesar D, Ribeiro R. Salivary density of Streptococcus mutans and Streptococcus sobrinus and dental caries in children and adolescents with Down syndrome. J Appl Oral Sci. 2017;25:250–7.
Marsh PD. In sickness and in health-what does the oral microbiome mean to us? An ecological perspective. Adv Dent Res. 2018;29:60–5.
Kilian M, Chapple IL, Hannig M, et al. The oral microbiome–an update for oral healthcare professionals. Br Dent J. 2016;221:657–66.
Lamont RJ, Koo H, Hajishengallis G. The oral microbiota: dynamic communities and host interactions. Nat Rev Microbiol. 2018;16:745–59.
Biagi E, Candela M, Centanni M, et al. Gut microbiome in Down syndrome. PLoS ONE. 2014;9:e112023.
Willis JR, Iraola-Guzmán S, Saus E, Ksiezopolska E, Cozzuto L, Bejarano LA, et al. Oral microbiome in down syndrome and its implications on oral health. J Oral Microbiol. 2020;13:1865690.
Caufield PW, Cutter GR, Dasanayake AP. Initial acquisition of mutans streptococci by infants: evidence for a discrete window of infectivity. J Dent Res. 1993;72:37–45.
Kageyama S, Asakawa M, Takeshita T, et al. Transition of bacterial diversity and composition in tongue microbiota during the first two years of life. mSphere. 2019;4:e00187-19.
Li F, Tao D, Feng X, Wong MCM, Lu H. Establishment and development of oral microflora in 12–24 month-old toddlers monitored by high-throughput sequencing. Front Cell Infect Microbiol. 2018;8:422.
Dzidic M, Collado MC, Abrahamsson T, Artacho A, Stensson M, Jenmalm MC, et al. Oral microbiome development during childhood: an ecological succession influenced by postnatal factors and associated with tooth decay. ISME J. 2018;12:2292–306.
Crielaard W, Zaura E, Schuller AA, Huse SM, Montijn RC, Keijser BJ. Exploring the oral microbiota of children at various developmental stages of their dentition in the relation to their oral health. BMC Med Genomics. 2011;4:22.
Yoshida A, Suzuki N, Nakano Y, Kawada M, Oho T, Koga T. Development of a 5′ nuclease-based real-time PCR assay for quantitative detection of cariogenic dental pathogens Streptococcus mutans and Streptococcus sobrinus. J Clin Microbiol. 2003;41:4438–41.
Kuboniwa M, Amano A, Kimura KR, et al. Quantitative detection of periodontal pathogens using real-time polymerase chain reaction with TaqMan probes. Oral Microbiol Immunol. 2004;19:168–76.
Jo R, Yama K, Aita Y, et al. Comparison of oral microbiome profiles in 18-month-old infants and their parents. Sci Rep. 2021;11:861.
Kim SW, Suda W, Kim S, et al. Robustness of gut microbiota of healthy adults in response to probiotic intervention revealed by high-throughput pyrosequencing. DNA Res. 2013;20:241–53.
Said HS, Suda W, Nakagome S, Chinen H, Oshima K, Kim S, et al. Dysbiosis of salivary microbiota in inflammatory bowel disease and its association with oral immunological biomarkers. DNA Res. 2014;21:15–25.
Iwasawa K, Suda W, Tsunoda T, Oikawa-Kawamoto M, Umetsu S, Takayasu L, et al. Dysbiosis of the salivary microbiota in pediatric-onset primary sclerosing cholangitis and its potential as a biomarker. Sci Rep. 2018;8:5480.
Urushiyama D, Suda W, Ohnishi E, Araki R, Kiyoshima C, Kurakazu M, et al. Microbiome profile of the amniotic fluid as a predictive biomarker of perinatal outcome. Sci Rep. 2017;7:12171.
Takayasu L, Suda W, Takanashi K, Iioka E, Kurokawa R, Shindo C, et al. Circadian oscillations of microbial and functional composition in the human salivary microbiome. DNA Res. 2017;24:261–70.
Lozupone C, Lladser ME, Knights D, Stombaugh J, Knight R. UniFrac: an effective distance metric for microbial community comparison. ISME J. 2011;5:169–72.
Seki M, Yamashita Y. Decreasing caries prevalence in Japanese preschool children is accompanied with a reduction in mutans streptococci infection. Int Dent J. 2005;55:100–4.
Xiao J, Fiscella KA, Gill SR. Oral microbiome: possible harbinger for children’s health. Int J Oral Sci. 2020;12:12.
Gomez A, Nelson KE. The oral microbiome of children: development, disease, and implications beyond oral health. Microb Ecol. 2017;73:492–503.
Mashima I, Theodorea CF, Thaweboon B, Thaweboon S, Scannapieco FA, Nakazawa F. Exploring the salivary microbiome of children stratified by the oral hygiene index. PLoS ONE. 2017;12:e0185274.
Domingues NB, Mariusso MR, Tanaka MH, Scarel-Caminaga RM, Mayer MPA, Brighenti FL, et al. Reduced salivary flow rate and high levels of oxidative stress in whole saliva of children with Down syndrome. Spec Care Dent. 2017;37:269–76.
Komatsu T, Duckyoung Y, Ito A, Kurosawa K, Maehata Y, Kubodera T, et al. Increased oxidative stress biomarkers in the saliva of Down syndrome patients. Arch Oral Biol. 2013;58:1246–50.
Siqueira WL, Siqueira MF, Mustacchi Z, de Oliveira E, Nicolau J. Salivary parameters in infants aged 12 to 60 months with Down syndrome. Spec Care Dent. 2007;27:202–5.
Hashizume LN, Schwertner C, Moreira MJS, Coitinho AS, Faccini LS. Salivary secretory IgA concentration and dental caries in children with Down syndrome. Spec Care Dent. 2017;37:115–9.
Davidovich E, Aframian DJ, Shapira J, Peretz B. A comparison of the sialochemistry, oral pH, and oral health status of Down syndrome children to healthy children. Int J Paediatr Dent. 2010;20:235–41.
Lynge Pedersen AM, Belstrøm D. The role of natural salivary defences in maintaining a healthy oral microbiota. J Dent. 2019;80:S3–12.
Marsh PD, Do T, Beighton D, Devine DA. Influence of saliva on the oral microbiota. Periodontol. 2000;2016(70):80–92.
Medeiros CCG, Dos Anjos Borges LG, Cherubini K, Salum FG, Medina da Silva R, de Figueiredo MAZ. Oral yeast colonization in patients with primary and secondary Sjögren’s syndrome. Oral Dis. 2018;24:1367–78.
Arrifin A, Heidari E, Burke M, Fenlon MR, Banerjee A. The effect of radiotherapy for treatment of head and neck cancer on oral flora and saliva. Oral Health Prev Dent. 2018;16:425–9.
Nonzee V, Manopatanakul S, Khovidhunkit SO. Xerostomia, hyposalivation and oral microbiota in patients using antihypertensive medications. J Med Assoc Thai. 2012;95:96–104.
Sinet PM. Metabolism of oxygen derivatives in Down’s syndrome. Ann N Y Acad Sci. 1982;396:83–94.
Giacaman RA, Torres S, Gómez Y, Muñoz-Sandoval C, Kreth J. Correlation of Streptococcus mutans and Streptococcus sanguinis colonization and ex vivo hydrogen peroxide production in carious lesion-free and high caries adults. Arch Oral Biol. 2015;60:154–9.
Herrero ER, Slomka V, Bernaerts K, Boon N, Hernandez-Sanabria E, Passoni BB, et al. Antimicrobial effects of commensal oral species are regulated by environmental factors. J Dent. 2016;47:23–33.
Neisseria TT, Rothia BA, Kathryn AB, Guido F. Corynebacterium. In: Bergey’s manual of systematics of Archaea and bacteria. 2015. http://onlinelibrary.wiley.com/book/https://doi.org/10.1002/9781118960608. Accessed 20 Jan 2021.
Kolenbrander PE, London J. Adhere today, here tomorrow: oral bacterial adherence. J Bacteriol. 1993;175:3247–52.
Haffajee AD, Socransky SS, Patel MR, Song X. Microbial complexes in supragingival plaque. Oral Microbiol Immunol. 2008;23:196–205.
Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL Jr. Microbial complexes in subgingival plaque. J Clin Periodontol. 1998;25:134–44.
Khocht A, Yaskell T, Janal M, Turner BF, Rams TE, Haffajee AD, et al. Subgingival microbiota in adult Down syndrome periodontitis. J Periodont Res. 2012;47:500–7.
Xiao C, Ran S, Huang Z, Liang J. Bacterial diversity and community structure of supragingival plaques in adults with Dental Health or caries revealed by 16S pyrosequencing. Front Microbiol. 2016;7:1145.
Janem WF, Scannapieco FA, Sabharwal A, et al. Salivary inflammatory markers and microbiome in normoglycemic lean and obese children compared to obese children with type 2 diabetes. PLoS ONE. 2017;12:e0172647.
Zaura E, Brandt BW, de Mattos MJT, et al. Same Exposure but two radically different responses to antibiotics: resilience of the salivary microbiome versus long-term microbial shifts in feces. MBio. 2015;6:e01693-15.
Acknowledgements
We would like to thank Ryutaro Jo, Kazuma Yama, Hisashi Kawasaki, Yuto Aita, and Takuya Inokuchi for their assistance in Illumina Miseq sequencing.
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Contributions
Conceived and designed the experiments: SM, KT, SG, and YM. Collection of clinical samples: KT, SG, and YM. Performed experiments: SM and KT. Analyzed the data: SM. Wrote the manuscript: SM. Revised the manuscript: SG, and YM. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of the Japanese Society for Oral Health and was conducted according to their guidelines (Approval no.: 27-4, 27-9). Written informed consent was obtained from the parents of all participants.
Consent for publication
Written informed consent was obtained from the parents of all participants for the publication of this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Sequences of primers and probes used in the quantitative PCR assays.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Morishima, S., Takeda, K., Greenan, S. et al. Salivary microbiome in children with Down syndrome: a case-control study. BMC Oral Health 22, 438 (2022). https://doi.org/10.1186/s12903-022-02480-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-022-02480-z