
Abstract
Purpose of Review
Individuals with Down syndrome (DS) may be more susceptible to oral disorders as a result of a combination of genetic factors, immunological disturbances, anatomical anomalies, and probable difficulties in maintaining adequate oral hygiene. Within this context, we provide a comprehensive review of the most important relationships between oral health and Down syndrome.
Recent Findings
Recent investigations suggest that a diminished diversity in the oral microbiome could emerge as a critical factor affecting oral health in individuals with DS. Plausible anatomical and metabolic peculiarities inherent to DS, including alterations in salivary characteristics, the presence of obstructive sleep apnea, elevated end glycation product levels, and hypothyroidism, may exert a significant influence on the composition and dynamics of the oral microbiome. A comprehensive analysis of the evidence implies a reduced occurrence of caries in individuals with DS. Furthermore, a recent meta-analysis indicates that gingivitis (OR 1.93; 95% CI 1.09–3.41) and periodontitis (OR 3.93; 95% CI 1.81–8.53) are more frequent in people with DS and strongly associated. Oral function in DS is also affected resulting in speech, breathing and eating problems. These findings underscore the necessity to implement targeted educational and awareness programs, along with specific intervention protocols, for the younger generations of individuals with DS, their families, and caregivers.
Summary
Although trisomy 21 itself does not determine a specific cause of oral diseases in DS, common oral health conditions such as gingivitis, periodontitis, and caries remain a matter of concern. The nexus between insufficient plaque control, distinctive oral characteristics, and reluctance to engage in treatment persists as noteworthy determinants. The necessity for oral health professionals to exercise patience and commitment when addressing oral care for individuals with Down syndrome is crucial.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Down syndrome (DS) stands out as one of the most widespread chromosomal disorders. According to the World Health Organization, it has an estimated global incidence ranging from 1 in 1000 to 1 in 1100 live births [1, 2••]. While DS is connected with a variety of physical and cognitive issues, one component of health that is frequently overlooked is oral health. While individuals with DS do not have specific oral health pathologies, they frequently exhibit a spectrum of oral health issues that tend to manifest with increased severity compared to their non-syndromic counterparts. These issues encompass dental anomalies, delayed tooth eruption, and higher predisposition to both periodontal diseases and caries. Oral health is not only important for physical health, but it also affects quality of life [3•]. Additionally, they frequently struggle with communicating skills, making oral health issues particularly relevant. Hence, poor oral health can worsen these issues, resulting in social isolation and low self-esteem [4]. Research in this area not only enhances our understanding of the syndrome’s broader health implications but also aids in the development of inclusive and specialized dental care approaches for individuals with special needs. Here, we provide a comprehensive review of the most important relationships between oral health and DS.
Definition, Craniofacial, and Oral Features of Down Syndrome
Down syndrome (DS) stands out as the most prevalent autosomal aneuploidy found in surviving newborns. This genetic anomaly arises from the complete or partial triplication of chromosome 21 and manifests in three distinct karyotypes: complete trisomy 21, mosaicism, and translocation. In individuals with DS, there is an elevated number of copies of genes located on chromosome 21. Importantly, the genes implicated in DS exhibit normal characteristics, and their gene products remain unaffected. The genetic irregularity associated with DS results in an overexpression of genes on chromosome 21, leading to increased production of gene products in cells and tissues. This overexpression, in turn, contributes to the manifestation of phenotypic abnormalities [5, 6].
Various characteristics linked to the oral cavity have been documented in DS, although their occurrence is not universal among patients or across all age groups, displaying variations based on ethnic backgrounds. Reported alterations encompass structures such as the jaws, tongue, dental features, and muscular disorders (Table 1). These variations can impact occlusion, phonation, swallowing, and overall quality of life in diverse ways [7,8,9].
The tongue represents a distinctive feature in individuals with DS, as it may appear enlarged. However, contemporary understanding negates the notion of a genuinely enlarged tongue, characterizing it instead as a pseudo-macroglossia linked to diminished dimensions of the craniofacial bones. Notably, research has also indicated that individuals with DS may, in fact, exhibit a comparatively smaller tongue (2432 mm2) in contrast to a control group [8]. As age advances, there is a decline in both anterior and posterior tongue strength, impacting functions such as swallowing and phonation [10]. Additionally, individuals with DS exhibit a dry lingual surface attributed to the oral respiration they commonly experience [11, 12].
Esbensen (2016) reported that oral breathing and muscular hypotonia in association with sleep disorders, affecting structures such as the jaw and tongue in DS [13]. Individuals with DS may exhibit alterations in maxillary sizes, characterized by a reduction in the middle third of the face, leading to a skeletal class III tendency. Furthermore, hypodontia is also common which can influence the correct development of the jaws [14].
Dental agenesis is frequently reported in DS, often marked by the absence of three or more teeth. Among permanent teeth, the upper lateral incisor (27%), mandibular second premolar (21%), and upper second premolar (18%) exhibit the highest prevalence of agenesis [15]. Additionally, various associated findings have been reported, including malocclusions such as anterior open bite, temporomandibular joint alterations, bruxism, and delayed tooth eruption [16].
While DS does not exhibit specific oral features, certain oral and craniofacial aspects are altered in individuals with DS. Depending on the severity of these alterations, they can have substantial implications for their oral health. To guarantee whether adult and pediatric patients receive the right care, dentists and medical care professionals should be aware of recognizing these unique traits and modifying treatment plans accordingly.
The Oral Microbiota and Microbiome in Down Syndrome
The composition of the oral microbiota has been studied in individuals with DS. Cuenca et al. (2021) stratified diverse periodontal conditions, encompassing 62 cases of DS-periodontal health, 34 cases of DS-gingivitis, and 28 cases of DS-periodontitis and studied the subgingival microbiota using q-PCR and culture-based techniques. Tannerella forsythia was the most prevalent species across all groups (67.9% in DS-periodontitis, 47.0% in DS-gingivitis, and 48.8% in DS-periodontal health), exhibiting significantly higher percentages in DS-periodontitis compared to DS-gingivitis and DS-periodontal health. Furthermore, the frequency detection, counts, and proportions of Porphyromonas gingivalis, Prevotella intermedia, T. forsythia, and Eikenella corrodens exhibited a progressive increase, correlating with the deterioration of periodontal status [17]. A systematic review included 26 studies of which 24 focused on determining the bacterial microbiota in DS-periodontitis, while 2 others delved into the oral fungal and oral viral composition [18••]. These results suggest that the oral bacterial composition may be similar between DS and non-syndromic individuals with periodontitis. Nevertheless, a study in children with DS (5.5 years old) without periodontal breakdown found that the subgingival microbiota at their deciduous teeth harbored important periodontal pathogens (Aggregatibacter actinomycetemcomitans and T. forsythia) that would suggest close monitoring and preventive measures in DS patients.
The microbiome, which consists of the diverse community of microorganisms (bacteria, viruses, fungi, and more) residing in different niches such as the mouth, plays a crucial role in maintaining oral health and has broader implications for overall health. In the past decade, our understanding of the intestinal microbiome and its bidirectional interaction with the brain has significantly advanced. It is now recognized that the microbiota may exert influence on cognitive function, and conversely, cognitive function may impact the composition of the microbiota [19,20,21]. The microbiota-gut-brain axis assumes a pivotal role not only in the development of neurodegenerative diseases [22] but also in the context of DS, as alterations in the intestinal microbiome have been documented in individuals with this condition [20, 23]. A study identified a strong correlation between the prevalence of DS and the use of antibiotics, specifically tetracycline and beta-lactamase-resistant narrow-spectrum penicillin. This association was attributed to antibiotics that can act as disruptors of the human microbiome [24••]. Low diversity composition of gut microbiota has been found to be linked to cognitive impairment in DS. Furthermore, genera such as Blautia and Citrobacter demonstrated a negative correlation with cognitive scores [20]. In non-syndromic individuals, the development of the intestinal microbiota occurs postnatally through mother-child contact, facilitating the transmission of crucial species such as Bifidobacterium and Bacteroides [25]. In the case of DS patients, microbiota alterations have been identified even in the pregnant mother before birth. A pilot study indicated that pregnant women giving birth to infants with DS exhibited a distinct microbiome composition compared to the control group [23].
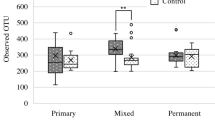
Willis et al. (2020) employed a comprehensive approach, utilizing 16S rRNA metabarcoding and high-throughput sequencing, along with culture and proteomics-based identification of fungi, to investigate the oral microbiome in individuals with DS in comparison to control samples. The initial observation revealed that DS individuals displayed lower salivary pH, and the microbiome exhibited reduced diversity. Specifically, individuals with DS demonstrated an elevated abundance of Kingella, Gemella, Cardiobacterium, Staphylococcus, Rothia, and Actinobacillus, coupled with a decreased abundance of Alloprevotella, Atopobium, and Candidatus saccharimonas. In the same study, the prevalence of fungi in individuals with DS was higher than controls (54% vs. 26%). Notably, Candida parapsilosis showed a significantly higher prevalence in DS (15.4% DS vs. 0.60% controls), as did Candida dubliniensis (15.4% DS vs. 1.51% controls), while the prevalence of Candida albicans was 30.8% in DS and 19% in controls [26]. In a recent case-control study [27], the salivary microbiome composition in children aged 1–13 years with DS was investigated using 16S DNA sequencing. The study found no statistically significant differences between the two groups in terms of diversity, except for a higher detection rate of Candida albicans in the mixed dentition of the DS group. Additionally, the DS group exhibited a high relative abundance of Corynebacterium and Cardiobacterium species with a low abundance of TM7. Furthermore, another study reported that Japanese children with DS do not exhibit red complex microorganisms (Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia) and that gingival inflammation impacts the diversity of the oral microbiome [28]. In contrast, once periodontitis is established, the subgingival microbiome of individuals with DS exhibits a higher abundance of Porphyromonas, Treponema, Tannerella, and Aggregatibacter, along with a lower abundance of genera such as Filifactor, Fretibacterium, and Desulfobulbus indicating a microbial profile similar to that observed in non-syndromic individuals with periodontitis [29].
While emerging research suggests differences in the oral microbiome between DS and non-syndromic individuals, the link between these findings and oral diseases requires additional investigation and ultimately will be essential for developing strategies to maintain oral health and potentially mitigate risks to overall health in individuals with DS. In addition, it appears plausible that specific anatomical and metabolic aspects of DS, such as changes in saliva characteristics, obstructive sleep apnea, increased end glycation products, and hypothyroidism, may influence the oral microbiome and hence create a susceptible environment for oral infections. These exploratory findings, when taken together, provide a glimpse into the specific oral microbiota in DS and allow for a greater knowledge of the oral health trends in this population.
Susceptibility to Periodontal Diseases
It is widely acknowledged that people with DS are more prone to periodontal diseases. In the seventies, Saxén et al. (1977) reported that the prevalence of bone loss (>5mm) in DS participants was 69% as compared to 20% in controls [30]. Other investigations found that clinical periodontal attachment loss is increased in people with DS; however, the difference is only about 0.6 mm when compared to controls [31,32,33]. A recent systematic review with meta-analysis revealed that the probing depth resulted in a mean difference of 0.40 mm (95% CI 0.09–0.70) between DS and non-syndromic people, which appears clinically insignificant. Hence, clinical periodontal findings do not support a clear association between DS and the severity of periodontal destruction. In contrast, the systematic review concluded that gingivitis (OR 1.93; 95% CI 1.09–3.41) and periodontitis (OR 3.93; 95% CI 1.81–8.53) were more frequent in people with DS and strongly associated [34••]. Furthermore, the prevalence of periodontitis in individuals with DS also rises with age and several studies have encompassed younger individuals (<15 years old), where a higher prevalence of gingivitis was observed [35, 36]. While the severity of periodontitis does not appear to be significantly elevated in individuals with DS, the increased frequency of periodontitis does lend support to the association between these two conditions. However, it is important to take into account factors such as variations in study designs and the utilization of partial periodontal indices, which may lead to an increased likelihood of overestimation.
Susceptibility of periodontitis has been studied from multiple perspectives. It has been recognized that inadequate oral hygiene plays a crucial role in predisposing individuals with DS to periodontitis [16, 37]. This susceptibility is attributed to factors such as cognitive disability, reduced manual dexterity, and a tendency to be uncooperative with treatment [38•, 39••]. Moreover, DS individuals often exhibit higher plaque indices compared to non-syndromic individuals, which can be exacerbated by dental abnormalities like peg-shaped teeth and dental crowding/malocclusion [40, 41]. Nevertheless, oral hygiene may be deemed satisfactory in individuals, typically children aged 10 years or younger, who receive assistance with toothbrushing from their parents or caregivers [42].
Other lines of research indicate that plaque is not the only issue and that the DS underlying systemic disorders may have a significant impact on susceptibility to periodontal diseases. Khocht et al. (2012) found that the percentage of monocytes actively involved in phagocytosis (whole blood samples) was significantly less in DS than that for controls and was associated with a slightly greater periodontal attachment loss (0.5 mm) [43]. Furthermore, studies have found increased oxidative burst activity in DS patients’ peripheral monocytes, granulocytes, and saliva, which may lead to inflammation of periodontal tissues and consequent loss of periodontal attachment [44, 45].
Research involving gingival biopsies and gingival crevicular fluid (GCF) from individuals with DS who have periodontitis suggests an alteration in immunoregulation. The findings indicate a more pronounced inflammatory cell infiltrate, which almost completely occupies the connective tissue, and an increased frequency of HLA Class II expression on both inflammatory cells and keratinocytes in the oral gingival epithelium. Additionally, there is an elevated CD4+/CD8+ T lymphocyte ratio, along with higher counts of CD4 T lymphocytes and monocytes/macrophages, indicative of a more active and destructive lesion. Analysis of GCF reveals elevated concentrations of cytokines associated with Th1, Th2, and Th17 responses, as well as increased levels of matrix metalloproteinases (MMP-2, MMP-8, and MMP-9) and prostaglandin E2 [46,47,48,49,50]. In recent years, genotyping and bioinformatic research have unveiled significant signaling pathways, such as the phosphatidylinositol 3-kinase (PI3K-Akt) pathway, which regulates cell proliferation and the inflammatory response. This pathway has also been found to be altered in individuals with DS who have periodontitis [51, 52].
In summary, research indicates that while gingivitis and periodontitis are considerable oral complications in DS patients, the underlying mechanisms are still debatable. However, the implementation of preventive measures, such as oral health programs for parents and caregivers, along with the early initiation of periodontal treatment and maintenance, has been shown to significantly enhance periodontal outcomes in individuals with DS [53••].
Susceptibility to Caries
Studies on the association between DS and caries have produced contrasting results. However, a recent systematic review determined that the incidence of caries in children and adolescents with DS was lower compared to control groups (49.9% vs. 63.4%) [54•]. But the certainty of this evidence is low since factors such as the type of affected dentition, caries index used, age, and geographic location significantly affect the results. Moreover, analyzed studies have low certainty of evidence and present issues such as small sample sizes, absence of a suitable control group, broad age ranges among participants, and even a deficiency in statistical analysis [54•, 55, 56]. These findings highlight the difficulty in controlling all pertinent variables that could potentially influence the results, making it challenging to draw definitive conclusions.
Possible explanations for the observed low incidence of caries in individuals with DS include the presence of diastemas, delayed tooth eruption and simpler tooth morphology, featuring fewer evident pits, and fissures. Some DS individuals also experience bruxism which smoothens the occlusal surfaces leading to enhanced self-cleaning and less biofilm retentive surfaces [57, 58]. Additionally, some studies suggest that individuals with DS exhibit elevated levels of salivary immunoglobulin A (sIgA), which inhibits the adhesion of bacteria responsible for dental caries to the tooth surface. This mechanism not only neutralizes extracellular enzymes involved in the caries process but also plays a crucial role in minimizing caries-related factors in individuals with DS [59]. In addition, research suggests that DS children exhibit reduced genotypic diversity and lower counts of Streptococcus mutans, resulting in decreased acidogenicity [60]. But despite the presence of observable traits seemingly associated with a lower incidence of caries, some studies imply that individuals with DS might still be more susceptible to dental caries. In terms of oral health, DS patients are thought to be at a disadvantage when compared to non-syndromic individuals. As a result, an early program of preventative measures is suggested that focuses on dental cleanliness, anti-plaque agents, and oral hygiene instructions not only for DS patients but also that include parents and caregivers [61].
The literature highlights that caries is a multifactorial disease that can be influenced by socioeconomic disparities. Therefore, considering these variables is crucial when comparing DS individuals with non-syndromic individuals. Differences in diet and oral hygiene standards among these groups can also contribute to variations in caries experiences [62]. The significance of oral hygiene appears to be pivotal in preventing dental caries in children with DS. An increase in disease experience is observed in the DS group when brushing occurs less than twice a day. This suggests that home care and health behaviors play a crucial role in determining disease experience [58]. Although the pooled evidence suggests a lower caries incidence in DS individuals, this finding should not undermine the importance of preventive oral health programs for special care patients and caregivers.
Oral Function in Down Syndrome
It is crucial to emphasize the scarcity of scientific literature dedicated to the study of oral complications in adults with DS and to avoid generalizing findings obtained from adolescent and pediatric populations [63]. Recognized risks include the heightened likelihood of developing multiple clinical comorbidities that necessitate continuous medical care, such as congenital heart disease, thyroid dysfunction, obstructive sleep apnea, dysphagia, chronic respiratory infections, and gastroesophageal reflux disease [16, 63]. Moreover, specific anatomical characteristics of DS can complicate optimal oral function [64]. For instance, an ogival palate coupled with reduced mandibular development may contribute to lingual protrusion and macroglossia, impede lip occlusion, and elevate the risk of anterior open bite and swallowing problems. Labial and lingual hypotonia, hindering proper sucking, saliva, and food bolus management, has also been reported [63]. Dental agenesis, supernumerary teeth, delayed dentition eruption, bruxism, and type III malocclusion are common dentition features; labial and tongue fissures may lead to secondary oral infections; all these features may directly affect healthy oral function in DS individuals [64•, 65].
A protruding tongue can lead to issues with speech and oral function, potentially moving posteriorly into the pharynx (glossoptosis), thereby contributing to obstructive sleep apnea. The repercussions of sleep disruption caused by sleep apnea are highly significant, particularly in terms of neurocognitive and cardiovascular effects. This, in turn, can result in a diminished life expectancy and quality of life within this population [66]. Early interventions in the oral cavity that influence jaw growth and tongue position may play a crucial role in mitigating the severity of sleep apnea.
Pharyngeal hypotonicity, where weakened muscle strength increases the risk of aspiration before and after swallowing, even leading to death by choking, is a significant concern [63]. Altered sensory perception causing intolerance to certain foods is also reported in DS individuals. These orofacial alterations may generate feeding and swallowing difficulties due to intermaxillary discrepancy hindering the stabilization of the mandible and hyoid bone, as well as poor control and mobilization of the food bolus [63], which can lead to serious health problems, favoring constipation, dysfunctional eating habits, obesity, and adversely impacting the quality of life.
These findings underscore the necessity to implement targeted educational and awareness programs, along with specific intervention protocols, for the younger generations of individuals with DS, their families, and caregivers. Emphasizing the significance of early interventions to maintain oral health is crucial, given that disease manifest in childhood and persist throughout life. These interventions should aim to compensate for difficulties in oral functions to the extent permitted by the anatomical characteristics unique to individuals with DS. Practical guidance for oral care, both for individuals with DS and their caregivers, is available in the recommendations provided by The National Institute of Dental and Craniofacial Research. (https://www.nidcr.nih.gov/sites/default/files/2017-09/practical-oral-care-down-syndrome.pdf; https://www.nidcr.nih.gov/sites/default/files/2017-09/dental-care-every-day-caregiver.pdf).
Conclusions
Although trisomy 21 itself does not determine a specific cause of oral diseases in Down syndrome, common oral health conditions such as gingivitis, periodontitis, and caries remain a matter of concern. The nexus between insufficient plaque control, distinctive oral characteristics, and reluctance to engage in treatment persists as noteworthy determinants. This underscores the necessity for oral health professionals to exercise patience and commitment when addressing oral care for individuals with Down syndrome.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Thomas J. Down syndrome: facts, statistics, and you [Internet]. Healthline Med. 2019; [cited 2023 Sept 28]. Available from: https://www.healthline.com/health/down-syndrome/down-syndrome-facts#Demographics.
•• Abukhaled Y, Hatab K, Awadhalla M, Hamdan H. Understanding the genetic mechanisms and cognitive impairments in Down syndrome: towards a holistic approach. J Neurol. 2023; https://doi.org/10.1007/s00415-023-11890-0. This article explains in detail the most important genetic mechanisms involved in the development of intellectual disabilities in Down syndrome.
• Risner-Bauman A, Robbins MR. Patient with a history of Down syndrome presents for periodic examination and cleaning. Dent Clin North Am. 2023 Oct;67(4):569–71. https://doi.org/10.1016/j.cden.2023.05.003. This article reviews the most important aspect of treating Down syndrome patients during periodic examinations.
Neitzel I. Narrative abilities in individuals with Down syndrome: single case-profiles. Front Psychol. 2023;14:1116567. https://doi.org/10.3389/fpsyg.2023.1116567.
Plaiasu V. Down syndrome - genetics and cardiogenetics. Maedica (Bucur). 2017;12(3):208–13.
Sperling K, Scherb H, Neitzel H. Population monitoring of trisomy 21: problems and approaches. Mol Cytogenet. 2023;16(1):6. https://doi.org/10.1186/s13039-023-006371.
Marques LS, Alcântara CE, Pereira LJ, Ramos-Jorge ML. Down syndrome: a risk factor for malocclusion severity? Braz Oral Res. 2015;29:44. https://doi.org/10.1590/1807-3107BOR-2015.vol29.0044.
Kaczorowska N, Kaczorowski K, Laskowska J, Mikulewicz M. Down syndrome as a cause of abnormalities in the craniofacial region: a systematic literature review. Adv Clin Exp Med. 2019;28(11):1587–92. https://doi.org/10.17219/acem/112785.
Takizawa H, Takahashi M, Maki K. Three-dimensional assessment of craniofacial features in patients with Down syndrome during the mixed dentition period: a case-control study. Cleft Palate Craniofac J. 2022;59(2):177–84. https://doi.org/10.1177/1055665621998181.
Javed F, Akram Z, Barillas AP, Kellesarian SV, Ahmed HB, Khan J, Almas K. Outcome of orthodontic palatal plate therapy for orofacial dysfunction in children with Down syndrome: a systematic review. Orthod Craniofac Res. 2018;21(1):20–6. https://doi.org/10.1111/ocr.12211.
Ghaith B, Al Halabi M, Khamis AH, Kowash M. Oral health status among children with Down syndrome in Dubai, United Arab Emirates. J Int Soc Prev Community Dent. 2019;9(3):232–9. https://doi.org/10.4103/jispcd.JISPCD_396_18.
Farpour HR, Moosavi SA, Mohammadian Z, Farpour S. Comparing the tongue and lip strength and endurance of children with Down syndrome with their typical peers using IOPI. Dysphagia. 2022;37(4):966–72. https://doi.org/10.1007/s00455-021-10359-4.
Esbensen AJ. Sleep problems and associated comorbidities among adults with Down syndrome. J Intellect Disabil Res. 2016;60(1):68–79. https://doi.org/10.1111/jir.12236.
van Marrewijk DJ, van Stiphout MA, Reuland-Bosma W, Bronkhorst EM, Ongkosuwito EM. The relationship between craniofacial development and hypodontia in patients with Down syndrome. Eur J Orthod. 2016;38(2):178–83. https://doi.org/10.1093/ejo/cjv054.
Palaska PK, Antonarakis GS. Prevalence and patterns of permanent tooth agenesis in individuals with Down syndrome: a meta-analysis. Eur J Oral Sci. 2016;124(4):317–28. https://doi.org/10.1111/eos.12282.
Goud EVSS, Gulati S, Agrawal A, Pani P, Nishant K, Pattnaik SJ, Gupta S. Implications of Down’s syndrome on oral health status in patients: a prevalence-based study. J Family Med Prim Care. 2021;10(11):4247–52. https://doi.org/10.4103/jfmpc.jfmpc_885_21.
Cuenca M, Marín MJ, Nóvoa L, O Connor A, Sanchez MC, Blanco J, Limeres J, Sanz M, Diz P, Herrera D. Periodontal condition and subgingival microbiota characterization in subjects with Down syndrome. Appl Sci. 2021;11(2):778. https://doi.org/10.3390/app11020778.
•• Contaldo M, Lucchese A, Romano A, Della Vella F, Di Stasio D, Serpico R, Petruzzi M. Oral microbiota features in subjects with Down syndrome and periodontal diseases: a systematic review. Int J Mol Sci. 2021;22(17):9251. https://doi.org/10.3390/ijms22179251. An updated systematic review that provides objective evidence of the association of Down syndrome and the oral microbiota
Cryan JF, O’Riordan KJ, Sandhu K, Peterson V, Dinan TG. The gut microbiome in neurological disorders. Lancet Neurol. 2020;19:179–94. https://doi.org/10.1016/S1474-4422(19)30356-4.
Ren S, Wang X, Qin J, Mu Q, Ye S, Zhang Y, Yu W, Guo J. Altered gut microbiota correlates with cognitive impairment in Chinese children with Down syndrome. Eur Child Adolesc Psychiatry. 2022;31(1):189–202. https://doi.org/10.1007/s00787-021-01799-2.
Mayer EA, Nance K, Chen S. The Gut-Brain Axis. Annu Rev Med. 2022 Jan;27(73):439–53. https://doi.org/10.1146/annurev-med-042320-014032.
Sorboni SG, Moghaddam HS, Jafarzadeh-Esfehani R, Soleimanpour S. A Comprehensive review on the role of the gut microbiome in human neurological disorders. Clin Microbiol Rev. 2022;35(1):e0033820. https://doi.org/10.1128/CMR.00338-20.
Hursitoglu M, Kural A, Kuras S, Akdeniz E, Sezer S, Caypinar SS, Kazezoglu C, Yaprak B, Karandere F, Guven HZ. Maternal gut microbiota in pregnancies resulting in down syndrome newborns - a pilot study. Acta Clin Croat. 2021;60(4):722–30. https://doi.org/10.20471/acc.2021.60.04.20.
•• Ternák G, Márovics G, Sümegi K, Bánfai Z, Büki G, Magyari L, Szabó A, Melegh B. Down-syndrome-related maternal dysbiosis might be triggered by certain classes of antibiotics: a new insight into the possible pathomechanisms. Antibiotics (Basel). 2023;12(6):1029. https://doi.org/10.3390/antibiotics12061029. This study discusses and provides insights on recent plausible mechanisms in which antibiotics cause dysbiosis in pregnant mothers and its association with Down syndrome.
Browne HP, Shao Y, Lawley TD. Mother-infant transmission of human microbiota. Curr Opin Microbiol. 2022;69:102173. https://doi.org/10.1016/j.mib.2022.102173.
Willis JR, Iraola-Guzmán S, Saus E, Ksiezopolska E, Cozzuto L, Bejarano LA, Andreu-Somavilla N, Alloza-Trabado M, Puig-Sola A, Blanco A, Broglio E, Carolis C, Hecht J, Ponomarenko J, Gabaldón T. Oral microbiome in down syndrome and its implications on oral health. J Oral Microbiol. 2020;13(1):1865690. https://doi.org/10.1080/20002297.2020.1865690.
Morishima S, Takeda K, Greenan S, Maki Y. Salivary microbiome in children with Down syndrome: a case-control study. BMC Oral Health. 2022;22(1):438. https://doi.org/10.1186/s12903-022-02480-z.
Mitsuhata C, Kado N, Hamada M, Nomura R, Kozai K. Characterization of the unique oral microbiome of children with Down syndrome. Sci Rep. 2022;12(1):14150. https://doi.org/10.1038/s41598-022-18409-z.
Nóvoa Garrido L, Sánchez MD, Blanco Carrión J, Limeres Posse J, Cuenca M, Marín MJ, Sanz M, Herrera D, Diz Dios P. The subgingival microbiome in patients with Down syndrome and periodontitis. J Clin Med. 2020;9(8):2482. https://doi.org/10.3390/jcm9082482.
Saxén L, Aula S, Westermarck T. Periodontal disease associated with Down’s syndrome: an orthopantomographic evaluation. J Periodontol. 1977;48(6):337–40. https://doi.org/10.1902/jop.1977.48.6.337.
López-Pérez R, Borges-Yáñez SA, Jiménez-García G, Maupomé G. Oral hygiene, gingivitis, and periodontitis in persons with Down syndrome. Spec Care Dentist. 2002;22(6):214–20. https://doi.org/10.1111/j.1754-4505.2002.tb00274.x.
Zigmond M, Stabholz A, Shapira J, Bachrach G, Chaushu G, Becker A, Yefenof E, Merrick J, Chaushu S. The outcome of a preventive dental care programme on the prevalence of localized aggressive periodontitis in Down’s syndrome individuals. J Intellect Disabil Res. 2006;50(Pt 7):492–500. https://doi.org/10.1111/j.1365-2788.2006.00794.x.
Khocht A, Janal M, Turner B. Periodontal health in Down syndrome: contributions of mental disability, personal, and professional dental care. Spec Care Dentist. 2010;30(3):118–23. https://doi.org/10.1111/j.1754-4505.2010.00134.x.
•• Rondón-Avalo S, Rodríguez-Medina C, Botero JE. Association of Down syndrome with periodontal diseases: systematic review and meta-analysis. Spec Care Dentist. 2023; https://doi.org/10.1111/scd.12892. A recent and updated systematic review that provides objective evidence of the association of Down syndrome and periodontal diseases.
van de Wiel B, van Loon M, Reuland W, Bruers J. Periodontal disease in Down's syndrome patients. A retrospective study. Spec Care Dentist. 2018;38(5):299–306. https://doi.org/10.1111/scd.12314.
Chandra HS, Johnson JS, Sagar L, Naveen M, Ziauddin S, Britto F, Havaldar KS, Shalini H. A Comparative evaluation of physical parameters of saliva and correlation with periodontal condition in Down syndrome children and healthy controls. J Contemp Dent Pract. 2023;24(6):372–80. https://doi.org/10.5005/jp-journals-10024-3481.
Sandeepa NC, Al Hagbani SA, Alhammad FA, Al Shahrani AS, Al Asmari SE. Oral health status of Down’s syndrome patients in Aseer. Saudi Arabia. J Pharm Bioallied Sci. 2021;13(Suppl 1):S656–9. https://doi.org/10.4103/jpbs.JPBS_593_20.
• Holzapfel SD, Ringenbach SD, Mulvey GM, Sandoval-Menendez AM, Cook MR, Ganger RO, Bennett K. Improvements in manual dexterity relate to improvements in cognitive planning after assisted cycling therapy (ACT) in adolescents with down syndrome. Res Dev Disabil. 2015;45-46:261–70. https://doi.org/10.1016/j.ridd.2015.08.003. This study shows how exercising can improve manual dexterity in patients with Down syndrome and this may improve oral hygiene.
•• Padia N, Bose M, Parab S. Determinants of hand function in children and adolescent with Down syndrome-a scoping review. J Hand Ther. 2022; https://doi.org/10.1016/j.jht.2022.07.010. A recent and updated systematic review that shows how hand functions are altered in Down syndrome.
Cheng RH, Leung WK, Corbet EF, King NM. Oral health status of adults with Down syndrome in Hong Kong. Spec Care Dentist. 2007;27(4):134–8. https://doi.org/10.1111/j.1754-4505.2007.tb00335.x.
Scott AM, Reed WM, Ajwani S, Parmenter TR. Panoramic radiographs and dental patients with Down syndrome: a scoping review. Spec Care Dentist. 2023;43(2):199–220. https://doi.org/10.1111/scd.12762.
Oredugba FA. Oral health condition and treatment needs of a group of Nigerian individuals with Down syndrome. Downs Syndr Res Pract. 2007;12(1):72–6. https://doi.org/10.3104/reports.2022.
Khocht A, Russell B, Cannon JG, Turner B, Janal M. Phagocytic cell activity and periodontitis in Down syndrome. Oral Dis. 2012;18(4):346–52. https://doi.org/10.1111/j.1601-0825.2011.01877.x.
Komatsu T, Duckyoung Y, Ito A, Kurosawa K, Maehata Y, Kubodera T, Ikeda M, Lee MC. Increased oxidative stress biomarkers in the saliva of Down syndrome patients. Arch Oral Biol. 2013;58(9):1246–50. https://doi.org/10.1016/j.archoralbio.2013.03.017.
Khocht A, Russell B, Cannon JG, Turner B, Janal M. Oxidative burst intensity of peripheral phagocytic cells and periodontitis in Down syndrome. J Periodontal Res. 2014;49(1):29–35. https://doi.org/10.1111/jre.12075.
Søhoel PD, Johannessen AC, Kristoffersen T, Haugstvedt Y, Nilsen R. In situ characterization of mononuclear cells in marginal periodontitis of patients with Down’s syndrome. Acta Odontol Scand. 1992;50(3):141–9. https://doi.org/10.3109/00016359209012757.
Søhoel DC, Johannessen AC, Kristoffersen T, Nilsen R. Expression of HLA class II antigens in marginal periodontitis of patients with Down’s syndrome. Eur J Oral Sci. 1995;103(4):207–13. https://doi.org/10.1111/j.1600-0722.1995.tb00161.x.
Tsilingaridis G, Yucel-Lindberg T, Modéer T. Enhanced levels of prostaglandin E2, leukotriene B4, and matrix metalloproteinase-9 in gingival crevicular fluid from patients with Down syndrome. Acta Odontol Scand. 2003;61(3):154–8. https://doi.org/10.1080/00016350310002270.
Yamazaki-Kubota T, Miyamoto M, Sano Y, Kusumoto M, Yonezu T, Sugita K, Okuda K, Yakushiji M, Ishihara K. Analysis of matrix metalloproteinase (MMP-8 and MMP-2) activity in gingival crevicular fluid from children with Down’s syndrome. J Periodontal Res. 2010;45(2):170–6. https://doi.org/10.1111/j.1600-0765.2009.01214.x.
Tsilingaridis G, Yucel-Lindberg T, Modéer T. T-helper-related cytokines in gingival crevicular fluid from adolescents with Down syndrome. Clin Oral Investig. 2012;16(1):267–73. https://doi.org/10.1007/s00784-010-0495-6.
Fernández M, de Coo A, Quintela I, García E, Diniz-Freitas M, Limeres J, Diz P, Blanco J, Carracedo Á, Cruz R. Genetic susceptibility to periodontal disease in Down syndrome: a case-control study. Int J Mol Sci. 2021;22(12):6274. https://doi.org/10.3390/ijms22126274.
Chen Y, Yu X, Kong J. Identification of neuropeptides as potential crosstalks linking Down syndrome and periodontitis revealed by transcriptomic analyses. Dis Markers. 2021;2021:7331821. https://doi.org/10.1155/2021/7331821.
•• Ferreira R, Michel RC, Greghi SL, Resende ML, Sant'Ana AC, Damante CA, Zangrando MS. Prevention and periodontal treatment in Down syndrome patients: a systematic review. PLoS One. 2016;11(6):e0158339. https://doi.org/10.1371/journal.pone.0158339. This systematic review shows the importance of periodontal care for individuals with DS.
• Martins M, Mascarenhas P, Evangelista JG, Barahona I, Tavares V. The incidence of dental caries in children with Down syndrome: a systematic review and meta-analysis. Dent J (Basel). 2022;10(11):205. https://doi.org/10.3390/dj10110205. This systematic review shows a lower incidence of caries in children with DS.
Moreira MJ, Schwertner C, Jardim JJ, Hashizume LN. Dental caries in individuals with Down syndrome: a systematic review. Int J Paediatr Dent. 2016;26(1):3–12. https://doi.org/10.1111/ipd.12212.
Silva MCPMD, Lyra MCA, Almeida HCR, Alencar Filho AV, Heimer MV, Rosenblatt A. Caries experience in children and adolescents with Down syndrome: a systematic review and meta-analysis. Arch Oral Biol. 2020;115:104715. https://doi.org/10.1016/j.archoralbio.2020.104715.
Areias CM, Sampaio-Maia B, Guimaraes H, Melo P, Andrade D. Caries in Portuguese children with Down syndrome. Clinics (Sao Paulo). 2011;66(7):1183–6. https://doi.org/10.1590/s1807-59322011000700010.
Discepolo K, Herzog C, Anderson NK, Chandwani N. Comparison of contributing risk factors for primary tooth caries in Down syndrome and non-special health needs children. Pediatr Dent. 2022;44(5):355–62.
Hamid H, Adanir N, Asiri FYI, Abid K, Zafar MS, Khurshid Z. Salivary IgA as a useful biomarker for dental caries in Down’s syndrome patients: a systematic review and meta-analysis. Eur J Dent. 2020;14(4):665–71. https://doi.org/10.1055/s-0040-1716443.
Moreira MJS, Klaus NM, Dall'Onder AP, Grando D, Parolo CCF, Faccini LS, Hashizume LN. Genotypic diversity and acidogenicity of Streptococcus mutans in Down syndrome children. Spec Care Dentist. 2019;39(6):578–86. https://doi.org/10.1111/scd.12420.
Cornejo LS, Zak GA, Dorronsoro de Cattoni ST, Calamari SE, Azcurra AI, Battellino LJ. Bucodental health condition in patients with Down syndrome of Cordoba City, Argentina. Acta Odontol Latinoam. 1996;9(2):65–79.
Moreira MJ, Schwertner C, Grando D, Faccini LS, Hashizume LN. Oral health status and salivary levels of mutans streptococci in children with Down syndrome. Pediatr Dent. 2015;37(4):355–60.
Cañizares-Prado S, Molina-López J, Moya MT, Planells E. Oral function and eating habit problems in people with Down syndrome. Int J Environ Res Public Health. 2022;19(5):2616. https://doi.org/10.3390/ijerph19052616.
• Kaczorowska N, Kaczorowski K, Laskowska J, Mikulewicz M. Down syndrome as a cause of abnormalities in the craniofacial region: a systematic literature review. Adv Clin Exp Med. 2019;28(11):1587–92. https://doi.org/10.17219/acem/112785. Readers can further review other oral abnormalities in Down syndrome.
Luconi E, Togni L, Mascitti M, Tesei A, Nori A, Barlattani A, Procaccini M, Santarelli A. Bruxism in children and adolescents with Down Syndrome: a comprehensive review. Medicina (Kaunas). 2021;57(3):224. https://doi.org/10.3390/medicina57030224.
Nguyen DT, Bricout VA, Tran HT, Pham VH, Duong-Quy S. Sleep apnea in people with Down syndrome: causes and effects of physical activity? Front Neurol. 2023;14:1123624. https://doi.org/10.3389/fneur.2023.1123624.
Funding
Open Access funding provided by Colombia Consortium
Author information
Authors and Affiliations
Contributions
JB, CR, SA, CLS, and AC wrote the main manuscript text, and JB and SA prepared Table 1. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This is not applicable to a review article. No human photographs were included.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Botero, J.E., Rodríguez-Medina, C., Amaya-Sanchez, S. et al. A Comprehensive Review of the Relationship Between Oral Health and Down Syndrome. Curr Oral Health Rep 11, 15–22 (2024). https://doi.org/10.1007/s40496-024-00363-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40496-024-00363-6