
Abstract
Introduction
To assess the ability of the Age-Adjusted Charlson Comorbidity Index (ACCI) to predict survival after radical gastrectomy in patients with gastric cancer (GC).
Method
Data from patients with GC who underwent radical gastrectomy from January 2008 to December 2012 in Fujian Medical University Union Hospital were retrospectively analyzed. Patients were categorized into either high ACCI group or low ACCI group based on the effect of ACCI on long-term GC prognosis. 1:1 propensity score matching (PSM) was used to reduce confounding bias. To further analyze the impact of ACCI on the long-term prognosis of patients after radical gastrectomy, a nomogram was built based on the Cox proportional hazards regression model.
Results
A total of 1476 patients were included in the analysis. After PSM, there was no statistically significant differences in tumor location, tumor size and tumor stage between low ACCI group (429 cases) and high ACCI group (429 cases) (all P > 0.05). Before and after PSM, the incidence of postoperative complications in high ACCI group was significantly higher than that in low ACCI group (P < 0.05). The 5-year overall survival rate (OS) in low ACCI group was significantly higher than that in high ACCI group. Multivariate analysis showed that ACCI was an independent risk factor for OS (P < 0.05). The Harrell’s C-statistics (C-index) of TNMA, a prognostic evaluation system combining ACCI and TNM staging system, was significantly higher than that of TNM staging system in both the modeling and validation groups (all P < 0.05).
Conclusions
ACCI was an independent risk factor for the long-term prognosis of GC patients after radical gastrectomy that could effectively improve the predictive efficacy of the TNM staging system for GC.
Similar content being viewed by others


Background
Although the incidence and mortality of GC showed a decreasing trend globally, [1], GC remains the fifth most common malignant tumor worldwide and the third leading cause of death (723,000 people die from GC, accounting for 8.8% of the world’s population) [2]. With the increase of population age and life expectancy, the proportion of elderly patients with gastric cancer also increases. Some studies showed that people over 70 years old account for more than 30% of patients with GC [3]. However, as the functional reserve of the human body tends to decline with age, elderly patients often have more comorbidities [4] and are more likely to have postoperative complications including death [5,6,7,8,9].
In 1994, Charlson et al. established a new scoring system, ACCI, to predict the incidence of complications during the perioperative period [10]. Recently, investigators have determined the predictive value of the ACCI on the long-term prognosis of patients with other malignant tumors (such as ovarian cancer, prostate cancer, pancreatic cancer, and colorectal cancer) [11,12,13,14,15]. Although the effect of the ACCI on the short-term prognosis of patients with GC has been reported in previous studies [16, 17], its predictive value on the long-term prognosis of patients with GC has not been reported. Therefore, the clinicopathological data of patients with radical gastrectomy from 2008 to 2012 were included in our study to evaluate the predictive value of the ACCI on the long-term prognosis of patients with GC.
Methods
Database
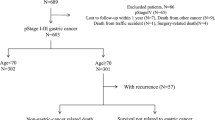
Data from patients with GC who underwent gastrectomy in the department of gastric surgery of the Affiliated Union Hospital of Fujian Medical University from January 2008 to December 2012 were collected and retrospectively analyzed. Patients who met the following criteria were included in this study: (1) pathologically diagnosed with gastric carcinoma before gastric surgery; (2) preoperative imaging examination (e.g., chest radiography, ultrasound examination, abdominal computed tomography) showed that the tumor had not invaded the surrounding organs, and there was no evidence of metastasis; and (3) patient underwent radical gastrectomy and proved to be an R0 excision after operation. Patients who had a previous history of gastric surgery or underwent neoadjuvant chemotherapy, or with gastric neuroendocrine tumor confirmed postoperatively were excluded. Thus, a total of 1476 patients were enrolled. The extend of gastrectomy and dissection of lymph nodes were performed according to the fourth edition of Japanese guidelines for the treatment of gastric cancer [18]. Tumor staging was based on the eighth cancer staging manual of American Joint Committee on Cancer (AJCC) [19].
The definition of ACCI
The ACCI, as defined by Charlson et al., is a combination of the age equivalence index and Charlson Comorbidity Index (CCI) [12]. For patients who over 40 years old, the cumulative score was 1 point for each additional 10 years of age (e.g.,1 point for those aged 50–59 years, 2 points for those aged 60–69 years, and so on), and the score for age is added to the CCI (e.g., 0,1,2,3) (Table 1). A completely resolved condition (i.e., a history of pneumonia) or a history of current inactive surgery (i.e., a history of cholecystectomy) is not considered as a comorbid disease [20].
Markers of systemic inflammation
Hematology and laboratory examinations were performed 1 week before surgery. Parameters including neutrophil count, lymphocyte count, platelet count, and albumin (Alb) levels were collected. NLR is defined as neutrophil count divided by lymphocyte count. PLR is defined as platelet count divided by lymphocyte count. LMR is defined as lymphocyte count divided by monocyte count. According to previous literature, cut-off values of NLR, PLR and LMR were defined as 4.0, 161.3 and 3.4 [21], respectively. Only 1017 patients with detailed preoperative registration of LMR, NLR and PLR in the whole group (1476 cases) were included in analysis.
Follow-up evaluation
Patients were followed up postoperatively using physical examination and laboratory tests, including tests for tumor markers (e.g., carcinoembryonic antigen [CEA] and CA19–9) every 3 months for the first 2 years, every 6 months for the next 3 years, and then annually. OS was defined as the time from surgery to the last follow-up or the date of death. Cancer-specific survival (CSS) refers to the time from surgery to the data of death from GC. Recurrence was diagnosed as an imaging manifestation or a biopsy of a suspicious lesion. Recurrence patterns were classified as local (anastomotic or gastric remnant), lymph node, peritoneum or hematogenous and unclear [22, 23]. Tumors involving the ovaries (Krukenberg’s tumor) were considered peritoneal [21].
Statistical analysis
The statistical analyses were performed using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). PMS was uesd to to reduce confounding bias [24,25,26,27]. A logistic regression model was chose for calculating the propensity scores and the following covariates: tumor size, tumor location and tumor stage. The 1:1 matching process was peformed by using the nearest neighbor matching method, under a 0.2 caliper [28]. The optimal cutoff point of the ACCI was obtained through X-tile (Version 3.6.1, Yale University) [29, 30]. Categorical data was presented as proportions and analyzed with the Chi-square test or Fisher’s exact test. Survival rate was calculated with the Kaplan-Meier method, and the differences were compared by log-rank tests. The Cox proportional hazards model was used to assess differences in survival. Variables with a p value of < 0.05 on univariate analysis were then included in a multivariate Cox stepwise regression analysis. Data of whole cohort (1476 cases) were randomly divided into modeling group (70%) and validation group (30%) [31, 32]. A nomogram was established based on the Cox proportional hazards regression model for calculating risk score of independent prognosis factors to further evaluate predictive value of ACCI by R software version 3.4.3 (http://www.r-project.org/) with the survival, rms, and survivalROC package [33, 34]. The differences of predictive ability on survival were compared by the C-index.
Results
The distribution and cut-off of the ACCI
The ACCI in the whole cohort ranged from 0 to 8, with a median of 2.00. The optimal cutoff value of the ACCI determined by the X-tile program, based on OS, was 3.00 (X2 = 37.30, P < 0.05, Additional file 4: Figure S1 A and B). Thus, patients were categorized into two groups (ACCI category): a low ACCI group (ACCI = 0–2; 1047 cases, 70.9%), and a high ACCI group (ACCI = 3–8; 429 cases, 29.1%). As is shown in Additional file 1: Table S1, low ACCI group included patients who were younger than 70 years old without comorbidity or with low CCI (CCI < 3). Those who were older than 70 years old were all included in high ACCI group. With the increase in age, the proportion of patients with comorbidities is also increased.
Clinicopathologic characteristics of the study population
The clinicopathologic characteristics of the whole cohort (1476 cases) and patients after PSM (858 cases) are shown in Table 2. High ACCI group and low ACCI group had significant differences in preoperative abdominal surgery history, ASA grade, tumor size, tumor location, pathological stages and histologic type (all P < 0.05), as well as in age (P < 0.001) and comorbidity (P < 0.001). After PSM, the difference in tumor size, tumor location and tumor stage between the two groups was not statistically significant. Before and after PSM, the incidence of postoperative complications in the high ACCI group was significantly higher than that in low ACCI group (P < 0.05). In addition, we also found significant differences in the distribution of NLR, LMR and PLR between the two groups, which may indicate the correlation between ACCI and systemic inflammation (P < 0.05, Additional file 2: Table S2).
Influence of ACCI level on the prognosis of patients
The median follow-up time of 858 matched patients was 48 months. There were significant differences in OS between high ACCI group and low ACCI group respectively (1-year OS: 82.7% vs 81.6%, 3-year OS: 62.4% vs 57.2%, 5-year OS: 56.4% vs 47.5%, all P < 0.05, Fig. 1). Although the difference of CSS between low and high ACCI groups were not reached statistic significant, the CSS curve in low ACCI group was still better than high ACCI group. Further stratified analysis showed that ACCI had a significant impact on the OS and CSS in patients with stage I and II. But in patients with stage III, significant difference only observed in OS between different groups, but not in CSS (Fig. 2). The types of tumor recurrence and metastasis observed during the follow-up period were shown in Additional file 3: Table S3. There were no statistically significant differences in the recurrence rate and the patterns of recurrence between patients of two groups with high ACCI and low ACCI (P > 0.05). However, high ACCI group still showed a trend of higher recurrence rate.

Kaplan-Meier overall survival (a) and cancer specific survival (b) for the Age-adjusted Charlson Comorbidity Index

Kaplan-Meier (KM) curves comparing the OS of patients with low ACCI and high ACCI. (a) American Joint Committee on Cancer, 8th edition (AJCC) stage I, (b) AJCC stage II, and (c) AJCC stage III. (d-f) KM curves comparing the CSS of patients with low ACCI and high ACCI at: (d) AJCC stage I, (e) AJCC stage II, and (f) AJCC stage III
Analysis of prognostic factors for OS and CSS
On univariate analysis, factors associated with 5-year OS included the ACCI, preoperative BMI, operative approach, tumor location, tumor size, TNM stage, histologic type and postoperative adjuvant chemotherapy (all P < 0.05, Table 3). Further multivariate analysis suggested that ACCI, tumor location, and TNM stage remained independent risk factors for OS (Table 4, all P < 0.05). While ACCI was not an independent prognostic factor for CSS (P > 0.05, Table 4).
Predictive value of the ACCI on long-term prognosis
In order to further assess the predictive value of the ACCI on survival after radical gastrectomy in patients with GC, we combined the ACCI and TNM stage, developing a new predictive system (TNMA). A nomogram was developed to predict the 5-year OS, which was based on the independent prognostic factors identified by multivariate analyses (Fig. 3a). And statistically significant difference in C-index between TNMA and TNM staging system was observed (0.720 vs 0.708, P = 0.022). In validation group, C-index of TNMA for OS prediction was also significantly higher than that in the TNM staging system (0.777 vs 0.742, P < 0.001). It suggested that the new TNMA prediction system could better predict the long-term survival of GC patients than TNM stage.

Nomogram plots and calibration curves based on ACCI and AJCC stage (a, b, c)
Discussion
With the aging of the population, the proportion of elderly patients with gastric cancer is gradually increasing. Meanwhile, the functional reserve of the human body tends to decline with age, which makes the incidence of complications increase [4]. Studies have shown that the screening strategy, treatment regimen and prognosis of patients with gastrointestinal tumors could be greatly affect by comorbidities [17]. The CCI was originally developed to predict the prognosis of patients with comorbidity in longitudinal studies [13]. It has been used in multiple studies to stratify the prognosis of patients and allow a more individualized treatment strategy. The ACCI is a simple scoring system further combining the two related factors of age and comorbidity. The previous study was mainly used to predict the occurrence of perioperative complications. Recently, studies has reported that ACCI also has predictive value on the long-term prognosis of patients with many malignant tumors including ovarian cancer, prostate cancer and lung cance [12, 13, 35]. However, the predictive value of ACCI on the long-term prognosis of patients with GC has not been reported. Therefore, in this large-scale study, we included patients with GC who underwent gastrectomy by a unified team to investigate the impact of ACCI on the long-term prognosis of GC patients.
In the previous manuscripts about the ACCI for the prediction of long-term prognosis of patients with malignant tumors, the selection of the optimal ACCI cut-off was quite different. Dias-Santos et al. obtained the cut-off point based on the ROC curve and quartile method [15], while Kahl et al. directly quoted similar studies in the literature for the cut-off [12]. In our study, the X-tile program and observed long-term survival of the study patients were used to obtain the ACCI cut-off value. This software, developed by Robert Camp et al. from Yale University in 2004, is a new method for obtaining the optimal cut-off. The cut-point selection is complicated by time-dependent assessment of the outcome in the X-tile program [30]. Compared with the ROC curve method for obtaining the optimal cutoff, which was merely based on the outcome, the use of the X-tile program is more appropriate. Thus, we obtained the best cut-off value of the ACCI at 3.00 and divided the whole cohort into a low-ACCI group (ACCI = 0–2) and high-ACCI group (ACCI = 3–8).
Since Virchow first established a link between cancer and inflammation in the nineteenth century, an increasing number of studies have shown that inflammatory markers is also plays an important role in tumor progression and metastasis [36]. It has been shown that preoperative inflammatory makers, including LMR, NLR and PLR, are closely related to the prognosis of various tumors [37,38,39]. Therefore, we included 1017 patients with detailed preoperative registration of LMR, NLR and PLR in the whole group for analysis, and found statistical differences in the distribution of inflammatory markers between low ACCI group and high ACCI group, which may indicate the correlation between ACCI and systemic inflammation.
Similar to most previous studies, the incidence of postoperative complications in our study was significantly higher in patients with a high ACCI [9, 12, 13], indicating that the ACCI had a significant effect on the short-term outcome of patients. In the prognostic analysis, the 5-year OS in high ACCI group were significantly worse than that in low ACCI group. Further stratified analysis showed that ACCI had a significant impact on the OS and CSS in patients with stage I and II. But in patients with stage III, significant difference only observed in OS between different groups. Although the CSS of low ACCI group is better than high ACCI group, the difference is not statistically significant. It also showed that there were no statistically significant difference in the recurrence rate and the patterns of recurrence between patients of two groups with high ACCI and low ACCI. However, high ACCI group still showed a trend of higher recurrence rate. This result may be affected to some extent due to not counting into the population with unclear site of recurrence. In the univariate analysis, ACCI and age were statistically significant prognostic factors for gastric cancer patients. On multivariate analysis, the ACCI was also an independent prognostic factor for gastric cancer patients, while age and CCI were not independent prognostic factors. This result demonstrated that ACCI, as a comprehensive indicator with age and comorbidity, provides a better prognostic assessment for patients. Although the effect of age and comorbidity should be assessed separately in a univariate, bivariate or multivariate analysis. The index is designed to be a simple, crude combined risk assessment for clinicians to use [10]. However, it is worth considering that, a stratified analysis showed that among patients without adjuvant chemotherapy, difference of 5-year OS between low ACCI group and high ACCI group was statistically significant. However, among patients received adjuvant chemotherapy, there was no statistically significant difference in survival between the two groups. These results might partly contribute to that the patients with a high degree of ACCI were more likely in poor physical condition than low ACCI patients. They may resist a more intensive treatment, which may affect the efficacy of treatment. This partly reflects the impact of ACCI on the treatment choices of patients after operation and their long-term prognosis. In addition, previous studies have shown that postoperative complications affect the long-term prognosis of patients [40, 41], while Liu et al. found that complications are unrelated to the long-term prognosis of gastric cancer patients [42], which is similar to our study. The relationship between postoperative complications and prognosis of gastric cancer patients is still controversial. Further analysis is needed on whether postoperative complications affect long-term prognosis.
An accurate staging system is essential for the prognosis of patients and the choice of treatment strategy options. The TNM staging system released by the AJCC is one of the most commonly used staging systems in the world. However, this system mainly focuses on the tumor condition, and personal factors are not included to make a more individualized evaluation. In this study, the combination of the ACCI and TNM stage (TNMA) was used to further evaluate the predictive value of the ACCI on prognosis in patients with GC. The results showed that C-index of TNMA on predicting OS of patients with GC was significantly higher than that in TNM staging system both in the modeling group and the validation group. Therefore, in adding the ACCI personal factors to the TNM staging system, the prediction of survival in patients with GC will be more accurate, and guidance will be enhanced for later treatment strategies. However, this study is a single-center study and lack of external validation, which should be validated by a multicenter prospective study.
Conclusions
In conclusion, ACCI was an independent risk factor for the long-term prognosis of patients after radical gastrectomy. Moreover, ACCI could effectively improve the predictive efficacy of the TNM staging system for the prognosis of patients with GC. It provided a simple and effective tool for preoperative evaluation.
Abbreviations
- ACCI:
-
Age-Adjusted Charlson Comorbidity Index
- AJCC:
-
American Joint Committee on Cancer
- Alb:
-
albumin
- ASA:
-
American Society of Anesthesiologists
- BMI:
-
body mass index
- CCI:
-
Charlson Comorbidity Index
- CEA:
-
carcinoembryonic antigen
- C-index:
-
the Harrell’s C-statistics
- CSS:
-
cancer-specific survival
- GC:
-
gastric cancer
- LMR:
-
lymphocyte count divided by monocyte count
- NLR:
-
neutrophil count divided by lymphocyte count
- OS:
-
overall survival
- PLR:
-
platelet count divided by lymphocyte count
- PSM:
-
propensity score matching
- TNMA:
-
a predictive system combining the ACCI and TNM stage
References
Matsuzaka M, et al. The decreasing burden of gastric cancer in Japan. Tohoku J Exp Med. 2007;212:207–19.
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90.
Oohara T, Johjima Y, Yamamoto O, et al. Gastric cancer in patients above 70 years of age. World J Surg. 1984;8:315–20.
Extermann M, Overcash J, Lyman GH, Parr J, Balducci L. Comorbidity and functional status are independent in older cancer patients. J Clin Oncol. 1998;16:1582–7.
Hamilton TD, et al. The impact of advanced age on short-term outcomes following gastric cancer resection: an ACS-NSQIP analysis. Gastric Cancer. 2017;21(4):710–9 Epub ahead of print.
Akeshita H, Ichikawa D, Komatsu S, Kubota T, Okamoto K, Shiozaki A, Fujiwara H, Otsuji E. Surgical outcomes of gastrectomy for elderly patients with gastric cancer. World J Surg. 2013;37:2891.
Huang CM, et al. A scoring system to predict the risk of postoperative complications after laparoscopic gastrectomy for gastric cancer based on a large-scale retrospective study. Medicine (Baltimore). 2015;94:e812.
Lee KG, et al. Risk factors associated with complication following gastrectomy for gastric cancer: retrospective analysis of prospectively collected data based on the Clavien-Dindo system. J Gastrointest Surg. 2014;18(7):1269–77.
Hsu JT, et al. Standard radical gastrectomy in octogenarians and nonagenarians with gastric cancer: are short-term surgical results and long-term survival substantial? J Gastrointest Surg. 2012;16(4):728–37.
Charlson M, et al. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–51.
Robbins JR, et al. Impact of age-adjusted Charlson comorbidity score on outcomes for patients with early-stage endometrial cancer. Gynecol Oncol. 2013;131(3):593–7.
Kahl A, du Bois A, Harter P, Prader S, Schneider S, Heitz F, Traut A, et al. Prognostic value of the age-adjusted Charlson comorbidity index (ACCI) on short- and long-term outcome in patients with advanced primary epithelial ovarian Cancer. Ann Surg Oncol. 2017;24(12):3692–9.
Lee JY, Kang HW, Rha KH, et al. Age-adjusted Charlson comorbidity index is a signifcant prognostic factor for long-term survival of patients with high-risk prostate cancer after radical prostatectomy: a Bayesian model averaging approach. J Cancer Res Clin Oncol. 2016;142(4):849–58.
Wu CC, et al. Age-adjusted Charlson comorbidity index scores as predictor of survival in colorectal cancer patients who underwent surgical resection and chemoradiation. Medicine (Baltimore). 2015;94(2):e431.
Dias-Santos D, et al. The Charlson age comorbidity index predicts early mortality after surgery for pancreatic cancer. Surgery. 2015;157(5):881–7.
Park HA, et al. Impact of age and comorbidity on the short-term surgical outcome after laparoscopy-assisted distal Gastrectomy for adenocarcinoma. Am Surg. 2013;79(1):40–8.
Tian Y, et al. Age-adjusted Charlson comorbidity index score as predictor of survival of patients with digestive system cancer who have undergone surgical resection. Oncotarget. 2017;8(45):79453–61.
Japanese Gastric Cancer AssociationJapanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017;20:1):1–19.
Ajani JA, In H, Sano T, et al. Stomach. In: Amin MB, editor. AJCC Cancer staging manual. 8th ed. New York: Springer-Verlag; 2016.
Charlson ME, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
Lin J-X, Lin J-P, et al. Prognostic importance of the preoperative modified systemic inflammation score for patients with gastric cancer. Gastric Cancer. 2018. https://doi.org/10.1007/s10120-018-0854-6. [Epub ahead of print].
Lu J, et al. CRP/prealbumin, a novel inflammatory index for predicting recurrence after radical resection in gastric cancer patients: post hoc analysis of a randomized phase III trial. Gastric Cancer. 2018. https://doi.org/10.1007/s10120-018-0892-0. [Epub ahead of print].
Jin LX, Moses LE, et al. Factors associated with recurrence and survival in lymph node-negative gastric adenocarcinoma: a 7-institution study of the US gastric Cancer collaborative. Ann Surg. 2015;262(6):999–1005.
Little RJ, Rubin DB. Causal effects in clinical and epidemiological studies via potential outcomes: concepts and analytical approaches. Annu Rev Public Health. 2000;21:121–45.
Kokudo T, et al. Survival benefit of liver resection for hepatocellular carcinoma associated with portal vein invasion. J Hepatol. 2016;65(5):938–43.
Fan G, et al. Different risk profiles for the postsurgical prognosis of gastric Cancer patients with different blood types: the FIESTA study. J Cancer. 2018;9(16):2885–94.
Ghinolfi D, et al. Use of elderly donors in liver transplantation: a paired-match analysis at a single Center. Ann Surg. 2018;268(2):325–31.
Huang SM, et al. Optimal timing for postsurgical adjuvant therapy in patients with gastric Cancer: a propensity score matching study. J Cancer. 2019;10(2):332–40.
Shang-Guan XC, et al. Preoperative lymph node size is helpful to predict the prognosis of patients with stage III gastric cancer after radical resection. Surg Oncol. 2018 Mar;27(1):54–60.
Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10(21):7252–9.
Attiyeh MA, et al. Development and validation of a multi-institutional preoperative Nomogram for predicting grade of dysplasia in Intraductal papillary mucinous neoplasms (IPMNs) of the pancreas: a report from the pancreatic surgery consortium. Ann Surg. 2018;267(1):157–63.
Petros FG, et al. Preoperative multiplex nomogram for prediction of high-risk nonorgan-confined upper-tract urothelial carcinoma. Urol Oncol. 2018;7(4):292.e1–9.
Lei Z, et al. Nomogram for preoperative estimation of microvascular invasion risk in hepatitis B virus-related hepatocellular carcinoma within the Milan criteria. JAMA Surg. 2016;151(4):356–63.
Deng QL, et al. Development and validation of a Nomogram for predicting survival in patients with advanced pancreatic ductal adenocarcinoma. Sci Rep. 2017;7(1):11524.
Asmis TR, et al. Age and comorbidity as independent prognostic factors in the treatment of non small-cell lung cancer: a review of National Cancer Institute of Canada clinical trials group trials. J Clin Oncol. 2008;26(1):54–9.
Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet. 2001;357:539–45.
McMillan DC. The systemic inflammation-based Glasgow prognostic score:a decade of experience in patients with cancer. Cancer Treat Rev. 2013;39:534–40.
Grenader T, et al. Derived neutrophil lymphocyte ratio may predict benefit from cisplatin in the advanced biliary cancer: the ABC-02 and BT-22 studies. Ann Oncol. 2015;26(9):1910–6.
Kim EY, Lee JW, Yoo HM, Park CH, Song KY. The platelet-to-lymphocyte ratio versus neutrophil-to lymphocyte ratio: which is better as a prognostic factor in gastric Cancer? Ann Surg Oncol. 2015;22(13):4363–70.
Tokunaga M, Tanizawa Y, Bando E, et al. Poor survival rate in patients with postoperative intra-abdominal infectious complications following curative gastrectomy for gastric cancer. Ann Surg Oncol. 2013;20:1575–83.
Kubota T, Hiki N, Sano T, et al. Prognostic significance of complications after curative surgery for gastric cancer. Ann Surg Oncol. 2014;21:891–8.
Liu X, Zhang D, Lin E, et al. Preoperative controlling nutritional status (CONUT) score as a predictor of long-term outcome after curative resection followed by adjuvant chemotherapy in stage II-III gastric Cancer. BMC Cancer. 2018;18(1):699.
Acknowledgements
The authors thank all the medical staff who contributed to the maintenance of the medical record database.
Funding
This study was supported by the Scientific and technological innovation joint capital projects of Fujian Province (2016Y9031); Construction Project of Fujian Province Minimally Invasive Medical Center (No. [2017]171); The second batch of special support funds for Fujian Province innovation and entrepreneurship talents (2016B013). The funding body had no role in the study design, data collection and analysis, or preparation of manuscript.
Availability of data and materials
The dataset analyzed for this study is available from the corresponding author upon reasonable request.
Author information
Authors and Affiliations
Contributions
YQH, JXL, CMH, PL and CHZ, conceived of the study, analyzed the data, and drafted the manuscript; RHT, JLL, JWX, ZNH and JBW helped revise the manuscript critically for important intellectual content; JL, QYC, LLC, and ML helped collect data and design the study. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study obtained approval from the Independent Ethics Committee of Fujian Medical University Union Hospital to identify patients diagnosed with gastric cancer in our center. Written informed consent was provided by the patients for their information and specimens to be stored in the hospital database and used in research. Patient records were anonymized and de-identified before analysis.
Consent for publication
Written consent was given by the patients and their relatives to use their information in a research study and publish it.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Table S1. Distribution of ACCI score according to age and comorbidity. (PDF 78 kb)
Additional file 2:
Table S2. Association of immune function and ACCI (N = 1017). (PDF 66 kb)
Additional file 3:
Table S3. Distribution of site of recurrence between different ACCI groups. (PDF 66 kb)
Additional file 4:
Figure S1. X-tile analysis of survival data reveals a continuous distribution based on the Age-Adjusted Charlson Comorbidity Index (ACCI) (A) X-tile plots for the ACCI constructed according to patients enrolled in this study. The plots show the X2 log-rank values with groups divided into 2 based on 1 cutoff points. The brightest pixel represents the maximum X2 log-rank value (37.298) generated by the cutoff value (3.00) as marked by the black spot. (B) The distribution of the number of patients related to ACCI. The ACCI ranged from 0.00 to 8.00 with a median of 2.00. (C) Survival curve of patients according to the ACCI. (PDF 196 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lin, JX., Huang, YQ., Xie, JW. et al. Age-adjusted Charlson Comorbidity Index (ACCI) is a significant factor for predicting survival after radical gastrectomy in patients with gastric cancer. BMC Surg 19, 53 (2019). https://doi.org/10.1186/s12893-019-0513-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-019-0513-9