
Abstract
Background
The progression of disc degeneration is generally believed to be associated with low back pain and/or degenerative lumbar diseases, especially in the elderly. The purpose of this study was to quantitatively evaluate changes in lumbar disc height using radiographic measurements and to investigate risk factors for development of disc height narrowing of the elderly.
Methods
From 1997 to 2007, 197 village inhabitants at least 65 years-old who participated in baseline examinations and more than four follow-up examinations conducted every second year were chosen as subjects for this study. Using lateral lumbar spine radiographs of each subject, L1-L2 to L5-S1 disc heights were measured. The subjects were divided into two groups according to the rate of change in disc height: mildly decreased (≤20 % decrease) and severely decreased (>20 % decrease). A stepwise multiple logistic regression analysis was used to select those factors significantly associated with disc height narrowing.
Results
Disc height at each intervertebral disc (IVD) level decreased gradually over ten years (p < 0.01, an average 5.8 % decrease of all disc levels). There was no significant difference in the rate of change in disc height among the IVD levels. Female gender, radiographic knee osteoarthritis and low back pain at baseline were associated with increased risk for disc height narrowing.
Conclusions
We conducted the first population-based cohort study of the elderly that quantitatively evaluated lumbar disc height using radiographic measurements. The risk factors identified in this study would contribute to a further understanding the pathology of disc degeneration.
Similar content being viewed by others


Background
With the advent of a populous aging society resulting from increasing life expectancy, the public health issues of the burden of disease and disability have gained prominence [1]. In particular, disability from musculoskeletal disorders in the aging population directly affects quality of life [2–5]. Degenerative disc diseases, or spondylosis of the lumbar spine, is a major factor affecting disability among the elderly [3, 6–8].
Lumbar degenerative disorders, such as spondylosis, lumbar canal stenosis and degenerative spondylolisthesis, are highly prevalent in the elderly [9]. It is generally thought that degenerative lumbar disorders occur during the progression of lumbar disc degeneration [10, 11]. Clinically, disc-space narrowing on lumbar radiographs is a common indicator for intervertebral disc (IVD) degeneration. To date, there are only a few epidemiologic population-based studies examining lumbar disc degeneration, especially in older populations [3, 9, 12, 13]. There are also only a few reports of longitudinal studies on the progression of lumbar disc degeneration [14–17]. In many epidemiologic studies, the extent of lumbar disc degeneration was semi-quantitatively evaluated using lumbar radiographs, but no study has been reported in which lumbar disc height was quantitatively evaluated.
The purposes of this population-based cohort study were to quantitatively evaluate the change and rate of progressive disc degeneration by radiographic measurements of lumbar disc height and to identify risk factors for the development of disc height narrowing in the elderly.
Methods
Participants
Data were analyzed from a population-based longitudinal prospective study of osteoporosis and knee osteoarthritis (OA) in a typical mountain village, Miyagawa, in the central Mie Prefecture of Japan [18–20]. A medical examination of village inhabitants at least 65 years-old had been conducted every second year since 1997. This study was conducted with approval of the Committee for the Ethics of Human Research of Mie University and all subjects provided written informed consent before enrollment in the study.
Clinical interview and physical examination
Subjects completed an interviewer-administrated questionnaire that included information on age, sex, work history, smoking history and medical history, including the presence of knee and/or low back pain. Histories of treatment for rheumatoid arthritis, osteoporosis, kidney and liver disorders, heart disease, hypertension, gout, thyroid disease, tuberculosis, and malignant tumors were recorded. Anthropometric measurements included body height, body weight, body mass index (BMI) and bone mineral density (BMD). The BMD of the forearm was measured using dual energy x-ray absorptiometry (DCS-600EX, Aloka, Tokyo). Anteroposterior radiographs of both knees were graded for radiographic knee OA using the Kellgren-Lawrence (KL) grading system. Definite radiographic knee OA was defined as KL grade 2 or higher. Vertebral compression fractures and calcification of the abdominal aorta were evaluated using lateral thoracic and lumbar radiographs. All radiographs were independently evaluated by three certified orthopedic surgeons who were blinded to the classification groups of this study.
Radiographic measurements of the lumbar spine
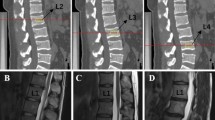
At each biannual examination, lateral lumbar spine radiographs of each subject were centered on the L3 vertebrae with the subjects in the left lateral recumbent position. The radiographs were digitalized using a scanner (ES-2200, EPSON, Tokyo, Japan). Anterior and posterior disc heights and IVD depth were measured as previously reported [21]. The criterion for positioning landmarks for measuring the discs was that the marks be on the extreme anterior and posterior margins of the vertebral end-plates. A trained observer assessed all lumbar radiographs from L1-L2 to L5-S1 discs using a custom software program in Microsoft Visual C++ with Microsoft Foundation Class programming environment (Microsoft Corp., Redmond, WA). Anterior disc height (Ha), posterior disc height (Hp), superior disc depth (Ds) and inferior disc depth (Di) were measured (Fig. 1). Disc height was expressed as the disc height index (DHI), based on the method of Farfan [22, 23] with modifications, calculated as: [(Ha + Hp)/(Ds + Di)] × 100. Within-observer reproducibility was assessed by test-retest analysis of 40 randomly selected radiographs from this study.

Disc height measurement. Ha: anterior disc height, Hp: posterior disc height, Ds: superior disc depth, Di: inferior disc depth. Disc height is expressed as the disc height index (DHI), which was calculated as: [(Ha + Hp)/(Ds + Di)] × 100
Classification of ∆DHI
The ∆DHI (%) was calculated as the rate of change in DHI compared to the baseline, [(DHI at follow ‐ up − DHI at baseline)/DHI at baseline] × 100. According to the value of ∆DHI (the rate of change in disc height) at the final examination, the subjects were divided into two groups: mildly decreased (MD) (∆DHI ≥ −20 %) and severely decreased (SD) (∆DHI ˂-20 %). Based on the classification of multilevel disc degeneration [24], the subjects with multilevel (more than two levels) SD were divided into contiguous SD (CSD) and skipped SD (SSD). Furthermore, the subjects with SSD were grouped into subtypes (I-V) dependent on the location of the severely decreased lumbar disc relative to the lumbar discs that were not severely decreased.
Statistical analysis
A two-way repeated measures analysis of variance was used to compare the IVD levels, assessed by ∆DHI, with times of examinations. Associations between ∆DHI and disc levels were analyzed using the chi-square test.
For a statistical analysis to identify the risk of progression of disc height narrowing that included severity of disc height narrowing at all lumbar disc levels, subjects were first divided into ordinal three groups according to the number of discs identified as severely decreased: Group A, no lumbar discs identified as severely decreased; Group B, one or two lumbar discs severely decreased; and Group C, three to five lumbar discs severely decreased. These three groups were then rearranged into two categories as follows: ‘group A and group B+ C’; or ‘group A + B and group C’. A stepwise polytomous logistic regression analysis using a cumulative logit model was subsequently performed to identify the risk factors among the three groups. Potential risk factors analyzed, including age, body weight, body height, BMI, presence of knee and/or low back pain, smoking, osteoporosis, radiographic knee OA and calcification of the abdominal aorta, treatment history of diabetes mellitus, kidney disorder, liver disorder, gout, hypertension, thyroid disorder, tuberculosis and osteoporosis, were assessed using the logistic regression model. Odds ratios were estimated between the two categories, ‘group A and group B + C’ and ‘group A + B and group C’ under the proportional odds assumption. A variance inflation factor (VIF) analysis was performed to evaluate the severity of multicollinearity. Data analyses were performed using SAS Version 9.0 (SAS Institute, North Carolina, USA).
Results
Characteristics of subjects
The population of this village was 4196 in 1997, including 1463 inhabitants who were 65 years-old or older. At baseline in 1997, 629 of these elderly inhabitants participated in this study. Over the ten years from 1997 to 2007, a possible total of six medical examinations were conducted. 197 inhabitants (62 males, 135 females, mean age: 70.1 years-old) who participated at baseline and had more than four subsequent examinations were chosen as subjects for this study. Of the 197 subjects, 154 (77.4 %) participated in the second examination (in 1999), 170 subjects (85.4 %) in the third (in 2001), 168 subjects (84.4 %) in the fourth (in 2003), 124 subjects (62.3 %) in the fifth (in 2005) and 103 subjects (51.6 %) in the sixth (in 2007). 36 subjects (18.3 %) were followed-up (until final examination) for 6 years, 60 subjects (30.4 %) for 8 years, and 101 subjects (51.3 %) for 10 years. The average follow-up period was 8.67 ± 1.53 years.
The results of anthropometric measurements are summarized in Table 1. Body height and weight were significantly higher in men than in women (p < 0.01), although there was no significant difference in BMI. Results of DHI at baseline are summarized in Table 2. At baseline, there were no significant differences in DHI for each disc level between men and women. Results of clinical interviews and interpretation of radiographs (knee OA and calcification of abdominal aorta) at baseline are summarized in Table 3. The percentage of smokers was significantly higher in men (p < 0.01). The prevalence of osteoporosis and radiographic knee OA was significantly higher in women (p < 0.01, p < 0.05, respectively).
Changes in disc height
The DHI at baseline (in 1997) was greatest at L5-S1, decreasing in sequence to L1-L2 (Table 2). The ∆DHI of each disc gradually decreased significantly (p < 0.0001) over the ten-year period (Fig. 2). An analysis of variance revealed no significant interaction between disc level and time-point (p = 0.63). The ∆DHI at each level had similar changes over ten years and did not differ significantly among the disc levels (p = 0.78). The overall average ∆DHI at the final examination (in 2007) was −5.8 ± 2.3 % (L1-L2: −3.2 ± 2.1 %, L2-L3: −6.5 ± 2.1 %, L3-L4: −8.4 ± 2.2 %, L4-L5: −7.3 ± 2.1 %, L5-S1: −3.7 ± 2.3 %). The within-observer reproducibility of DHI, assessed by the intraclass correlation coefficient [ICC], was 0.95.

Rate of change in disc height index (∆DHI). The ∆DHI shows a significant gradual decrease over the ten-year period (p < 0.0001) (Fig. 3). An analysis of variance revealed no significant disc level and time-point interactions (p = 0.63). The ∆DHI at each level shows similar changes over ten years that did not differ significantly among the disc levels (p = 0.78)
∆DHI classification
Comparing the ∆DHI classifications at each level, approximately 30 % of the subjects were in the SD group (L1-L2: 29 %, L2-L3: 29 %, L3-L4: 25 %, L4-L5: 26 %, L5-S1: 31 %) and 70 % were in the MD group (L1-L2: 71 %, L2-L3: 71 %, L3-L4: 75 %, L4-L5: 74 %, L5-S1: 69 %) (Fig. 3). There were no significant differences in the percentages of the SD group among the disc levels (p = 0.88).
The subjects were then sorted according to the number of discs identified as severely decreased (Fig. 4). Within the total number of subjects (n = 197), the number of subjects with no lumbar discs severely decreased was 30 % (n = 60); with one disc severely decreased was 25 % (n = 49); two discs 26 % (n = 52); three discs 11 % (n = 22); four discs 6 % (n = 11); and five discs 2 % (n = 3). The number of subjects with one or two discs severely decreased accounted for 55 % of the total.

Percentage of discs classified as severely and mildly decreased at each disc level by rate of change in disc height index (∆DHI). At each disc level, the severely decreased group was approximately 30% and the mildly decreased group was approximately 70%

Number of subjects with severely decreased disc height by disc level. The graph shows the number of subjects whose lumbar discs was identified as severely decreased at each level. The illustration below the graph is a representative image of the severely decreased degeneration pattern by number of subjects
Among the subjects with multilevel SD (45 % of the total subjects: n = 88), contiguous SD (CSD) was 47 % (n = 41) and skipped SD (SSD) was 53 % (n = 47). Among the subjects with SSD, type I was 60 % (n = 28), type II 13 % (n = 6), type III 11 % (n = 5), type IV 13 % (n = 6) and type V 4 % (n = 2).
Prediction of disc height narrowing
Results of the logistic regression analysis are summarized in Table 4. Increased risk for disc height narrowing was significantly associated with female gender (p = 0.0006), radiographic knee OA (p = 0.0197) and the presence of low back pain (p = 0.0253) at baseline. Other potential risk factors, including age, body height, body weight, BMI, smoking, knee pain, osteoporosis, radiographic calcification of abdominal aorta, work history, treatment history of diabetes mellitus, kidney disorder, liver disorder, gout, hypertension, thyroid disorder, tuberculosis and osteoporosis were not significantly associated with disc height narrowing.
Discussion
The results of this population-based cohort study showed that the lumbar disc height of the village inhabitants gradually decreased over ten years and did not differ significantly among disc levels. The results of this study indicate that female gender, radiographic knee OA and the presence of low back pain are significantly associated with risk for development of lumbar disc height narrowing in the elderly.
A definition of intervertebral disc degeneration has not been uniformly applied, although it is well known that disc tissue shows progressive morphological, structural, histological, biochemical and functional changes with aging [25, 26]. In the early stage of degeneration, the water content of the hydrostatic nucleus pulposus, as shown by magnetic resonance imaging (MRI), decreases and microstructural changes within the disc tissues, such as clefts and tears, are often identified [27–29]. With progression, more severe morphological changes, such as anulus tears, disc prolapse and end-plate damage, are seen, with the formation of osteophytes [27]. In this advanced stage, disc height narrowing becomes evident on lumbar radiographs; this change is referred to as radiographic lumbar spondylosis [30], which has the potential to progress to such degenerative spinal diseases as lumbar spine canal stenosis [10, 11]. Therefore, although disc height narrowing is the most commonly used specific finding to indicate disc degeneration in the clinical setting, this change should be considered to represent an advanced stage of disc degeneration with significant structural changes.
In the study reported here, radiographic lumbar disc height was manually measured using a previously reported method of Farafan’s measurements [22, 23] with modifications. Amonoo-Kuofi [31] radiographically measured human IVD height on cross-sections and found that disc height increased until the fifth decade of life, after which there was an appreciable decline. To date, we are aware of no studies that report the quantitative assessment of disc height in a population-based longitudinal study of the elderly. The results of our study show a 5.8 % decrease in the disc height index of the lumbar spine over ten years with no significant differences in the rate of decrease among the disc levels.
The occurrence pattern of multilevel disc height narrowing has previously been evaluated based on the classification of multilevel disc degeneration [24, 32], which contains contiguous and skipped patterns. In our study, the percentage of subjects with multilevel severely degenerated (SD) discs was 45 % of all subjects. Among these, the percentage of subjects with skipped SD was 53 %; this percentage was much higher than that of subjects with degenerated discs in the Southern Chinese cohort study (21 %) as reported by Cheung and colleagues [24]. Different from this previous cross-sectional MRI-based study reported by Cheung and colleagues [24], our study evaluated the change in disc height by radiographic measurements in a longitudinal study (an average of 8.7 years follow-up). These differences could account for the large difference in the percentage of the subjects with skipped multilevel disc degeneration.
There have been a few longitudinal studies of risk factors associated with intervertebral disc degeneration. Elfering et al. [14] conducted a longitudinal MRI investigation of lumbar disc degeneration, and found that disc herniation, the lack of athletic activities, and night-shift work are significant risk factors for the development of lumbar disc degeneration. In a population-based longitudinal study of the progression of lumbar disc degeneration, Hassett et al. [15] reported that progression of disc space narrowing, semi-quantitatively assessed by lumbar radiography, was predicted by age, back pain, and radiographic hip and knee OA. Valdes et al. [17] reported a candidate gene association longitudinal study, and found that genes regulating inflammatory pathways [including matrix metalloproteinase-3 (MMP-3), tissue inhibitor of metalloproteinase 1 (TIMP-1), and cyclooxygenase-2 (COX-2)] were associated with radiographic progression of lumbar disc degeneration.
The results of our study showed that female gender is a risk factor for disc height narrowing in the elderly. This is in accordance with the findings of de Schepper et al. [33], who reported that the frequency of radiographic disc space narrowing was significantly higher in women than men in a cross-sectional cohort population aged 55 years and older. Muraki et al. [30] examined the incidence and risk factors for radiographic lumbar spondylosis assessed by Kellgren and Lawrence (K-L) grades [30], and found the incidence of disc space narrowing is higher in women. An MRI-based cohort study in the elderly by Wang et al. [34] also found female subjects had more severe disc degeneration. More recently, Wang et al. [35] reported that the prevalence and severity of disc space narrowing is higher in elderly women than in elderly men in a large population study. Recent evidence increasingly suggests that sex hormones influence the severity of disc degeneration [36]. Estrogens are known to have diverse physiological actions (e.g., on growth and proliferation) in several organs, including the intervertebral disc [37, 38], and estrogen deficiency is a factor contributing to accelerated disc degeneration [36, 39]. These studies, and ours, suggest the possibility that being a postmenopausal woman is one of the risk factors for progression of disc degeneration.
In agreement with the study results of Hasset [15], the results of our study showed that radiographic OA is a risk factor associated with disc height narrowing. Cross-sectional studies have suggested a relationship between disc degeneration and generalized OA [40, 41]. Biochemically, it is well known that the components and metabolism of the extracellular matrix of intervertebral discs and articular cartilage share common characteristics. Recent advances in genetic studies suggest that certain genetic polymorphisms may be relevant to development of degenerative musculoskeletal disorders, such as OA and disc degeneration (see review [42]). It has recently been suggested that genetic polymorphisms associated with knee OA [e.g., in asporin [43, 44] and growth differentiation factor 5 [45, 46]] may also be related to disc degeneration [47].
Hassett et al. [15] found that having back pain at baseline had a significant association with the progression of disc height narrowing. We also found a significant association of back pain with progressive disc height narrowing. Although the pathogenesis of back pain in the elderly is not fully understood, lumbar spondylotic changes, including disc height narrowing [30] and spinal alignment changes with lumbar spondylosis [48], are thought to have an effect on low back pain. The results of our risk factor analysis suggest that the existence of low back pain furthered the progression of lumbar spondylotic changes, including disc height narrowing in the elderly.
In our study of an older population, BMI had no association with disc height narrowing. However, the effect of being overweight on disc degeneration is controversial. In two extensive population-based longitudinal studies [14, 15], no significant relationship between high BMI and disc degeneration was identified. On the other hand, in a cross-sectional MRI-based study of adolescents and young adults, Samarzis et al. [49] reported that juvenile disc degeneration was strongly associated with being overweight. Liuke et al. [50] also reported an association between being overweight and lumbar disc degeneration in a population-based MRI study in middle-aged men, and provided evidence that a BMI above 25 kg/m2 increased the risk of disc degeneration, with a greater effect at younger ages than in middle age. This suggests that high BMI is strongly associated with disc degeneration, especially in the young. Therefore, it may be appropriate to interpret our finding that BMI has no association with development of disc height narrowing in the elderly with caution.
Although the mechanism of disc degeneration remains largely unknown, it is generally believed that progression of disc degeneration is attributable to degradation of IVD tissues by environmental factors, such as mechanical stimuli and injury, and/or intrinsic factors, such as compromise of local nutrition to the disc, the aberrant expression of cytokines and cell death, under the influence of heredity and genetic factors [25, 42, 51–53]. Our study focused on the progression of radiographic disc height narrowing in commonly seen degenerative lumbar diseases in an elderly population at least 65-years-old. The results of our study indicate that, under the influence of heredity and genetic factors [42, 51, 53], gender and/or local factors associated with aging may play a role in disc height narrowing, which is representative of the progression of degenerative structural changes in IVD tissues.
This study has several limitations. First, the subjects of this study were limited to a minimum age of 65 years-old. Therefore, the risk factors identified in this study cannot be regarded as those for the general population. Second, the follow-up period was not the same for all subjects, ranging from 6–10 years, thus possibly introducing heterogeneity into the analysis of DHI data.
Conclusions
The lumbar disc height of the elderly inhabitants of a mountain village gradually decreased over time, and the rate of change in disc height did not differ significantly among disc levels. A risk factor analysis using a multivariate logistic regression model showed that female gender, radiographic knee OA and having low back pain are significantly associated with development of lumbar disc height narrowing in the elderly. The progression of disc degeneration is one of the underlying pathologies of the degenerative lumbar diseases commonly seen in an elderly population. More comprehensive epidemiologic research evidence on disc degeneration would contribute not only to understanding its pathology, but would also provide clues for a prophylactic approach and future treatment of the diseases associated with disc degeneration.
References
Guralnik JM, Fried LP, Salive ME. Disability as a public health outcome in the aging population. Annu Rev Public Health. 1996;17:25–46.
Ayis S, Dieppe P. The natural history of disability and its determinants in adults with lower limb musculoskeletal pain. J Rheumatol. 2009;36(3):583–91.
Muraki S, Akune T, Oka H, En-Yo Y, Yoshida M, Saika A et al. Health-related quality of life in subjects with low back pain and knee pain in a population-based cohort study of Japanese men: the research on osteoarthritis against disability study. Spine. 2011;36(16):1312-9. doi:10.1097/BRS.0b013e3181fa60d1.
Odding E, Valkenburg HA, Stam HJ, Hofman A. Assessing joint pain complaints and locomotor disability in the Rotterdam study: effect of population selection and assessment mode. Arch Phys Med Rehabil. 2000;81(2):189–93.
Odding E, Valkenburg HA, Stam HJ, Hofman A. Determinants of locomotor disability in people aged 55 years and over: the Rotterdam Study. Eur J Epidemiol. 2001;17(11):1033–41.
Huang KY, Lin RM, Lee YL, Li JD. Factors affecting disability and physical function in degenerative lumbar spondylolisthesis of L4-5: evaluation with axially loaded MRI. Eur Spine J. 2009;18(12):1851–7.
Robertson PA, Plank LD. Prospective cohort analysis of disability reduction with lumbar spinal fusion surgery in community practice. J Spinal Disord Tech. 2008;21(4):235–40.
Sigmundsson FG, Kang XP, Jonsson B, Stromqvist B. Correlation between disability and MRI findings in lumbar spinal stenosis: a prospective study of 109 patients operated on by decompression. Acta orthopaedica. 2011;82(2):204-10. doi:10.3109/17453674.2011.566150.
Muraki S, Oka H, Akune T, Mabuchi A, En-Yo Y, Yoshida M, et al. Prevalence of radiographic lumbar spondylosis and its association with low back pain in elderly subjects of population-based cohorts: the ROAD study. Ann Rheum Dis. 2009;68(9):1401–6.
Szpalski M, Gunzburg R. Lumbar spinal stenosis in the elderly: an overview. Eur Spine J. 2003;12 Suppl 2:S170–5. doi:10.1007/s00586-003-0612-1.
Yong-Hing K, Kirkaldy-Willis WH. The pathophysiology of degenerative disease of the lumbar spine. Orthop Clin North Am. 1983;14(3):491–504.
Yoshimura N, Dennison E, Wilman C, Hashimoto T, Cooper C. Epidemiology of chronic disc degeneration and osteoarthritis of the lumbar spine in Britain and Japan: a comparative study. J Rheumatol. 2000;27(2):429–33.
Yoshimura N, Muraki S, Oka H, Mabuchi A, En-Yo Y, Yoshida M, et al. Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: the research on osteoarthritis/osteoporosis against disability study. J Bone Miner Metab. 2009;27(5):620–8.
Elfering A, Semmer N, Birkhofer D, Zanetti M, Hodler J, Boos N. Risk factors for lumbar disc degeneration: a 5-year prospective MRI study in asymptomatic individuals. Spine. 2002;27(2):125–34.
Hassett G, Hart DJ, Manek NJ, Doyle DV, Spector TD. Risk factors for progression of lumbar spine disc degeneration: the Chingford Study. Arthritis Rheum. 2003;48(11):3112–7.
Symmons DP, van Hemert AM, Vandenbroucke JP, Valkenburg HA. A longitudinal study of back pain and radiological changes in the lumbar spines of middle aged women. II. Radiographic findings. Ann Rheum Dis. 1991;50(3):162–6.
Valdes AM, Hassett G, Hart DJ, Spector TD. Radiographic progression of lumbar spine disc degeneration is influenced by variation at inflammatory genes: a candidate SNP association study in the Chingford cohort. Spine. 2005;30(21):2445–51.
Ikeda Y, Sudo A, Yamada T, Uchida A. Mortality after vertebral fractures in a Japanese population. J Orthop Surg (Hong Kong). 2010;18(2):148-52.
Nishimura A, Hasegawa M, Kato K, Yamada T, Uchida A, Sudo A. Risk factors for the incidence and progression of radiographic osteoarthritis of the knee among Japanese. Int Orthop. 2011;35(6):839-43. doi:10.1007/s00264-010-1073-x.
Sudo A, Miyamoto N, Horikawa K, Urawa M, Yamakawa T, Yamada T, et al. Prevalence and risk factors for knee osteoarthritis in elderly Japanese men and women. J Orthop Sci. 2008;13(5):413–8.
Tibrewal SB, Pearcy MJ. Lumbar intervertebral disc heights in normal subjects and patients with disc herniation. Spine. 1985;10(5):452–4.
Dabbs VM, Dabbs LG. Correlation between disc height narrowing and low-back pain. Spine. 1990;15(12):1366–9.
Farfan H. Mechanical disorder of the low back. Philadelphia: Lea and Febiger; 1973.
Cheung KM, Samartzis D, Karppinen J, Luk KD. Are “patterns” of lumbar disc degeneration associated with low back pain?: new insights based on skipped level disc pathology. Spine. 2012;37(7):E430–8. doi:10.1097/BRS.0b013e3182304dfc.
Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006;31(18):2151–61.
Urban JP, Roberts S. Degeneration of the intervertebral disc. Arthritis Res Ther. 2003;5(3):120–30.
Boos N, Weissbach S, Rohrbach H, Weiler C, Spratt KF, Nerlich AG. Classification of age-related changes in lumbar intervertebral discs: 2002 Volvo Award in basic science. Spine. 2002;27(23):2631–44.
Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine. 2001;26(17):1873–8.
Vernon-Roberts B, Moore RJ, Fraser RD. The natural history of age-related disc degeneration: the pathology and sequelae of tears. Spine. 2007;32(25):2797–804.
Muraki S, Akune T, Oka H, Ishimoto Y, Nagata K, Yoshida M et al. Incidence and risk factors for radiographic lumbar spondylosis and lower back pain in Japanese men and women: the ROAD study. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society. 2012;20(7):712-8. doi:10.1016/j.joca.2012.03.009.
Amonoo-Kuofi HS. Morphometric changes in the heights and anteroposterior diameters of the lumbar intervertebral discs with age. J Anat. 1991;175:159–68.
Cheung KM, Samartzis D, Karppinen J, Mok FP, Ho DW, Fong DY, et al. Intervertebral disc degeneration: new insights based on “skipped” level disc pathology. Arthritis Rheum. 2010;62(8):2392–400. doi:10.1002/art.27523.
de Schepper EI, Damen J, van Meurs JB, Ginai AZ, Popham M, Hofman A et al. The association between lumbar disc degeneration and low back pain: the influence of age, gender, and individual radiographic features. Spine. 2010;35(5):531-6. doi:10.1097/BRS.0b013e3181aa5b33.
Wang YX, Griffith JF, Ma HT, Kwok AW, Leung JC, Yeung DK et al. Relationship between gender, bone mineral density, and disc degeneration in the lumbar spine: a study in elderly subjects using an eight-level MRI-based disc degeneration grading system. Osteoporos Int. 2011;22(1):91-6. doi:10.1007/s00198-010-1200-y.
Wang YX, Griffith JF, Zeng XJ, Deng M, Kwok AW, Leung JC, et al. Prevalence and sex difference of lumbar disc space narrowing in elderly chinese men and women: osteoporotic fractures in men (Hong Kong) and osteoporotic fractures in women (Hong Kong) studies. Arthritis Rheum. 2013;65(4):1004–10. doi:10.1002/art.37857.
Wang YX, Griffith JF. Effect of menopause on lumbar disk degeneration: potential etiology. Radiology. 2010;257(2):318-20. doi:10.1148/radiol.10100775.
Gruber CJ, Tschugguel W, Schneeberger C, Huber JC. Production and actions of estrogens. N Engl J Med. 2002;346(5):340–52.
Gruber HE, Yamaguchi D, Ingram J, Leslie K, Huang W, Miller TA, et al. Expression and localization of estrogen receptor-beta in annulus cells of the human intervertebral disc and the mitogenic effect of 17-beta-estradiol in vitro. BMC Musculoskelet Disord. 2002;3:4.
Deng M, Griffith JF, Zhu XM, Poon WS, Ahuja AT, Wang YX. Effect of ovariectomy on contrast agent diffusion into lumbar intervertebral disc: a dynamic contrast-enhanced MRI study in female rats. Magn Reson Imaging. 2012;30(5):683-8. doi:10.1016/j.mri.2012.01.001.
Bijkerk C, Houwing-Duistermaat JJ, Valkenburg HA, Meulenbelt I, Hofman A, Breedveld FC, et al. Heritabilities of radiologic osteoarthritis in peripheral joints and of disc degeneration of the spine. Arthritis Rheum. 1999;42(8):1729–35.
de Schepper EI, Damen J, van Meurs JB, Ginai AZ, Popham M, Hofman A, et al. The association between lumbar disc degeneration and low back pain: the influence of age, gender, and individual radiographic features. Spine. 2010;35(5):531–6. doi:10.1097/BRS.0b013e3181aa5b33.
Ikegawa S. The genetics of common degenerative skeletal disorders: osteoarthritis and degenerative disc disease. Annu Rev Genomics Hum Genet. 2013;14:245–56. doi:10.1146/annurev-genom-091212-153427.
Kizawa H, Kou I, Iida A, Sudo A, Miyamoto Y, Fukuda A, et al. An aspartic acid repeat polymorphism in asporin inhibits chondrogenesis and increases susceptibility to osteoarthritis. Nat Genet. 2005;37(2):138–44. doi:10.1038/ng1496.
Song YQ, Cheung KM, Ho DW, Poon SC, Chiba K, Kawaguchi Y, et al. Association of the asporin D14 allele with lumbar-disc degeneration in Asians. Am J Hum Genet. 2008;82(3):744–7. doi:10.1016/j.ajhg.2007.12.017.
Chapman K, Takahashi A, Meulenbelt I, Watson C, Rodriguez-Lopez J, Egli R, et al. A meta-analysis of European and Asian cohorts reveals a global role of a functional SNP in the 5′ UTR of GDF5 with osteoarthritis susceptibility. Hum Mol Genet. 2008;17(10):1497–504. doi:10.1093/hmg/ddn038.
Williams FM, Popham M, Hart DJ, de Schepper E, Bierma-Zeinstra S, Hofman A, et al. GDF5 single-nucleotide polymorphism rs143383 is associated with lumbar disc degeneration in Northern European women. Arthritis Rheum. 2011;63(3):708–12. doi:10.1002/art.30169.
Loughlin J. Knee osteoarthritis, lumbar-disc degeneration and developmental dysplasia of the hip--an emerging genetic overlap. Arthritis Res Ther. 2011;13(2):108. doi:10.1186/ar3291.
Takemitsu Y, Harada Y, Iwahara T, Miyamoto M, Miyatake Y. Lumbar degenerative kyphosis. Clinical, radiological and epidemiological studies. Spine. 1988;13(11):1317–26.
Samartzis D, Karppinen J, Mok F, Fong DY, Luk KD, Cheung KM. A population-based study of juvenile disc degeneration and its association with overweight and obesity, low back pain, and diminished functional status. J Bone Joint Surg. 2011;93(7):662-70. doi:10.2106/JBJS.I.01568.
Liuke M, Solovieva S, Lamminen A, Luoma K, Leino-Arjas P, Luukkonen R, et al. Disc degeneration of the lumbar spine in relation to overweight. Int J Obes (Lond). 2005;29(8):903–8.
Battie MC, Videman T. Lumbar disc degeneration: epidemiology and genetics. J Bone Joint Surg. 2006;88 Suppl 2:3–9. doi:10.2106/JBJS.E.01313.
Sambrook PN, MacGregor AJ, Spector TD. Genetic influences on cervical and lumbar disc degeneration: a magnetic resonance imaging study in twins. Arthritis Rheum. 1999;42(2):366–72.
Videman T, Battie MC, Ripatti S, Gill K, Manninen H, Kaprio J. Determinants of the progression in lumbar degeneration: a 5-year follow-up study of adult male monozygotic twins. Spine. 2006;31(6):671–8. doi:10.1097/01.brs.0000202558.86309.ea.
Acknowledgements
This study was sponsored by grants from the Ministry of Education, Culture, Sports, Science and Technology (Japan). The authors would like to thank Drs. Akihiko Matsumine, Masahiro Hasegawa, Hiroki Wakabayashi, Kunihiro Asanuma, Masaya Tsujii, Shinichi Miyazaki, Takao Matsubara, Tomoki Nakamura and Tosiro Yamaguchi for participation in the medical examinations.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KA conceived of this study and participated in the study design, and performed data acquisition, analysis and interpretation, and drafted the manuscript. TY participated in the interpretation of data, performed statistical analyses, and critically revised the manuscript. NI developed and programmed the image analysis software, participated in the interpretation of data, and helped to draft the manuscript. AN directed the medical examinations, performed data acquisition, and critically revised the manuscript. AS contributed to the study design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Akeda, K., Yamada, T., Inoue, N. et al. Risk factors for lumbar intervertebral disc height narrowing: a population-based longitudinal study in the elderly. BMC Musculoskelet Disord 16, 344 (2015). https://doi.org/10.1186/s12891-015-0798-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-015-0798-5