
Abstract
Background
Acute exacerbation (AE) of systemic autoimmune disease-related interstitial lung diseases (SAID-ILD) is less common than AE of idiopathic pulmonary fibrosis (IPF) and the details of AE-SAID-ILD have not been elucidated, but the prognosis is similarly devastating. This study was undertaken to determine the incidences of AE-ILD in each SAID and to elucidate the proportion of progressive fibrosing (PF)-ILD in AE-SAID-ILD.
Methods
We retrospectively analysed data for patients with SAID-ILD who were diagnosed and observed at our hospital between 1999 and 2020.
Results
Two hundred and thirty-two patients with SAID-ILD were enrolled, with a mean observation period of 100.2 months. AE-SAID-ILD was found in 25 patients (10.78%), mainly in patients with RA (17 patients, 68%) and elderly male patients with a smoking history. The overall incidence of AE-SAID-ILD was 1.29%/person-year, and the incidence for each SAID was as follows: RA 2.193, microscopic polyarteritis (MPA) 3.203, systemic sclerosis (SSc) 2.277, primary Sjögren syndrome 0.426, and polymyositis/dermatomyositis 0.222. The incidence of AE of RA/MPA/SSc-ILD was significantly higher than that of other AE-SAID-ILD (p < 0.001). Five of 25 patients (20%) fulfilled the criteria for PF-ILD. The 90-day survival rate was 48.0%, and a higher neutrophil count at AE (HR 13.27, 95%CI 2.447–246, p = 0.001) and early commencement of long-duration direct haemoperfusion with a polymyxin B-immobilised fibre column (HR 0.105, 95%CI 0.005–0.858, p = 0.035) were significant prognostic factors.
Conclusions
The incidence of AE-SAID-ILD was significantly higher in patients with RA, MPA, or SSc than in patients with other SAID. Furthermore, even in patients with AE-SAID-ILD, the proportion of PF-ILD just before AE was not high (20%).
Similar content being viewed by others

Introduction
Acute exacerbation (AE) of interstitial lung diseases (ILD) is a devastating condition that frequently occurs in patients with idiopathic pulmonary fibrosis (IPF), especially in its late stage [1,2,3,4,5]. AE-IPF accounts for 30%–40% of deaths in patients with IPF [6, 7], and is the most frequent cause of death in patients with IPF [7] or idiopathic interstitial pneumonia (IIPs) [8]. AE also occurs in other ILDs, such as idiopathic nonspecific interstitial pneumonia [9], unclassifiable IIP [10], connective tissue disease (CTD)-associated ILD [9, 11,12,13], and microscopic polyarteritis (MPA)-associated ILD [12].
Regarding systemic autoimmune diseases (SAID), including CTD and MPA, the presence of ILD has the significant impact on the long-term clinical course and the mortality [14, 15]. AE-ILD sometimes occurs during the clinical course in patients with SAID-ILD and makes the prognosis further worse than in those without AE-ILD [12, 14, 16, 17]. On admission of patients with AE-SAID-ILD, the exclusion of infectious diseases [18, 19] and drug-induced pneumonitis [20] is important to swiftly initiate proper treatments for saving patients with AE-SAID-ILD. AE-SAID-ILD is most common in patients with rheumatoid arthritis (RA) [11, 12], and was associated with decreased long-term survival of patients with RA during their clinical course [16, 17]. In addition, although the incidence of AE-ILD is relatively low in patients with SAID compared with IPF [9, 11], AE-SAID-ILD was associated with a poor prognosis after the onset of AE, similar to that of AE-IPF [12, 13]. However, little is known about the detailed incidence of AE-ILD in each SAID, or the proportion of progressive fibrosing (PF)-ILD associated with worsening ILD, even after treatment with corticosteroids and immunosuppressants [21]. Furthermore, no effective treatments for AE-SAID-ILD have yet been established. In the current study, we therefore retrospectively evaluated the incidences and clinical features of AE-SAID-ILD, as well as the prognostic factors, including treatments for AE-SAID-ILD. To the best of our knowledge, this is the first study to reveal the detailed incidence of AE-ILD for each SAID, the proportion of PF-ILD just before AE, and the possible therapeutic effect of direct haemoperfusion with a polymyxin B-immobilised fibre column (PMX-DHP) in patients with AE-SAID-ILD.
Methods
Study design and subjects
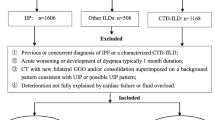
We retrospectively studied 232 patients with SAID-ILD, including CTD and MPA-related ILD, who were diagnosed and observed at our hospital between 1999 and 2020. The patients included 84 with RA, 51 with polymyositis/dermatomyositis (PM/DM), 28 with primary Sjögren syndrome (pSS), 17 with MPA, 16 with systemic sclerosis (SSc), nine with systemic lupus erythematosus (SLE), one with mixed connective tissue disease (MCTD), and 26 with several overlapping SAIDs (others). Patients with AE-SAID-ILD who had an acute, clinically significant respiratory deterioration characterized by new widespread alveolar abnormalities were selected. All patients met the modified diagnostic criteria for AE-SAID-ILD described by Collard et al. in 2016 [22]. Briefly, these included: 1) previous or concurrent diagnosis of ILD, 2) acute worsening or development of dyspnoea typically < 1 month in duration; 3) computed tomography (CT) with new bilateral ground-glass opacity and/or consolidation superimposed on background findings of ILD, and 4) deterioration not fully explained by cardiac failure or fluid overload. The study protocol was approved by the Ethics Committee of Hamamatsu University School of Medicine (approval number 18–085). All procedures in this study were performed in accordance with the study protocol and the 1964 Helsinki declaration as amended. The need for patient approval and informed consent was waived due to the retrospective nature of the study.
Data collection
Clinical, laboratory, physiological, and treatment data were obtained from medical records. The severity of ILD within 12 months before the AE event was assessed using the gender, age, and physiology (GAP) staging system [23] and the Japanese Respiratory Society (JRS) severity grades for ILD [24]. The former considers gender, age, and lung physiology variables, forced vital capacity (FVC) and diffusion lung capacity for carbon monoxide (DLCO) [23]. The latter consists of PaO2 at rest and minimum SpO2 during a 6-min walking test (6MWT) [24]. All blood samples were collected on the first or second day of admission before starting treatments for AE-ILD. Serum concentrations of S100A8 were measured by an enzyme-linked immunosorbent assay with the cooperation of Medical & Biological Laboratories (MBL, Nagoya, Japan; CircuLex™ S100A8/MRP8 ELISA Kit). The extent of lung opacity was measured in three high-resolution CT (HRCT) slices, as described previously [25]. The pattern of AE-ILD on HRCT was classified as 1) peripheral, 2) multifocal, or 3) diffuse, as reported by Akira et al. [26]. The HRCT findings were reviewed by two observers. The frequency of AE-SAID-ILD was calculated by dividing the number of patients with AE-SAID-ILD by the total number of patients with SAID-ILD and observation period (%/person-year).
Definition of PF-ILD
The patients were required to meet at least one of the following criteria for progression of ILD within the 24 months, despite standard treatment with an agent other than antifibrotic agents such as nintedanib or pirfenidone [21]: 1) a relative decline in the FVC of ≥ 10% of the predicted value, 2) a relative decline in FVC of 5% to < 10% of the predicted value and worsening of respiratory symptoms or an increased extent of fibrosis on HRCT, or 3) worsening of respiratory symptoms and an increased extent of fibrosis.
Statistical analysis
Statistical analysis was performed using JMP-13.1.0 (SAS Institute Inc., Cary, NC, USA) and EZR 1.41 (Saitama Medical Centre, Jichi Medical University, Saitama, Japan) [27]. The occurrence of AE-SAID-ILD was estimated considering death before AE as a competing event, and analysed using Gray's method. The relationships between SAIDs and AE-SAID-ILD occurrence were evaluated by Fine-Gray tests. Overall survival was estimated using Kaplan–Meier curves. The relationships between variables and mortality were evaluated by Cox proportional hazards regression analysis. All tests were two-sided and statistical significance was set at p < 0.05.
Results
Incidence of AE-ILD in patients with SAID
Twenty-five of the 232 patients (10.78%) with SAID-ILD had AE during the observation period (mean 100.2 months). The patient’s demographic, laboratory, physiologic, and radiologic data and treatments are shown in Table 1. The median age was 72 years, and males (17, 68%) and ex/current smokers (19, 76%) were predominant. Among the 25 patients with AE-SAID-ILD, the most common SAID was RA (17 patients, 68%) (Fig. 1), and other SAIDs included MPA (3 patients, 12%), SSc (2 patients, 8%), pSS (1 patient, 4%), DM (1 patient, 4%), and malignant RA + Sjögren syndrome (1 patient, 4%). The overall incidence of SAID-ILD was 1.29%/person-year, and the incidences of each SAID were as follows (Fig. 1B, Gray’s test, p = 0.023): RA, 2.193; MPA, 3.203; SSc, 2.277; pSS, 0.426; PM/DM, 0.222; SLE, 0; MCTD, 0; and several overlapping SAIDs (others), 0.481. The risks of AE were significantly higher in patients with RA-ILD and MPA-ILD compared with PM/DM-ILD (Fig. 1B, RA vs. PM/DM: Fine-Gray test, hazard ratio [HR] 11.35, 95% confidence interval (CI): 1.593–80.92; MPA vs. PM/DM: Fine-Gray test, HR 11.67, 95%CI: 1.365–99.81). The integrated incidence of AE of RA/MPA/SSc-ILD was significantly higher than that of other AE-CTD-ILD (Fig. 1C, Gray’s test, p < 0.001, Fine-Gray test; HR 8.324, 95%CI: 2.514–27.56).

Breakdown of 25 patients with AE-SAID-ILD and incidence of each AE-SAID-ILD. A) Proportion of SAID among 25 patients with AE-SAID-ILD. B) Incidences of each SAID (Gray’s test, p = 0.023). C) Incidence of AE among patients with RA/MPA/SSc-ILD compared with other AE-CTD-ILD (Gray’s test, p < 0.001, Fine-Gray test; HR 8.324, 95%CI: 2.514–27.56). Abbreviations: AE-SAID-ILD: acute exacerbation of systemic autoimmune disease-related interstitial lung diseases, RA: rheumatoid arthritis, MPA: microscopic polyarteritis, SSc: systemic sclerosis, pSS: primary Sjögren syndrome, SS: secondary Sjögren syndrome, PM/DM: polymyositis/dermatomyositis, MRA: malignant RA, SLE: systemic lupus erythematosus, MCTD: mixed connective tissue disease, CTD: connective tissue disease, HR: hazard ratio
Physiological examination findings, laboratory data, HRCT findings, and treatments
The clinical data for all patients with AE-SAID-ILD, including physiological examination, laboratory data, HRCT findings, and treatments within 12 months before the onset of AE-ILD, are shown in Table 1. Twelve patients (48%) had a usual interstitial pneumonia pattern on HRCT. High proportions of patients with AE-SAID-ILD were Grade 1 according to the GAP and JRS staging systems (32% and 24%, respectively). Twenty patients (80%) with AE-SAID-ILD received immunosuppressive treatments including corticosteroids and/or immunosuppressants, one patient (4%) received an antifibrotic agent, and four patients (16%) received oxygen therapy before AE. There were no patients who underwent surgical lung biopsy, other surgical operation, or mechanical ventilation immediately before AE-SAID-ILD. Regarding laboratory data at AE, the median PaO2/FiO2 (P/F) ratio was 180. The peripheral white blood cell (WBC) and neutrophil counts increased at AE (11.6 and 10.7 × 103/μL, respectively). A diffuse pattern on HRCT at AE was the most frequent pattern (19, 76%) and the extent score on HRCT was 18.5/25. All of patients were treated with steroid-pulse therapy (methylprednisolone of 1,000 mg/day for 3 days) followed by a tapering dose of prednisolone. Thirteen patients (52%) received immunosuppressants, and eight (32%) received long-duration (mainly ≥ 12 h) PMX-DHP (Toray Medical Co., Ltd, Tokyo, Japan) [28, 29]. These treatments were commenced concomitantly with the antibiotics, as soon as possible after admission. There were no patients who underwent extracorporeal membrane oxygenation.
Proportion of patients who fulfilled the criteria of PF-ILD
Of the 25 patients with AE-SAID-ILD, five (20%) fulfilled the criteria for PF-ILD [21] within 12 months before AE (Fig. 2). Among these patients, ILD progressed slowly before AE-ILD, despite standard treatments other than antifibrotic agents such as nintedanib or pirfenidone.

Proportion of patients with AE-SAID-ILD who fulfilled the criteria for PF-ILD within 12 months before AE. Abbreviations: PF-ILD: progressive fibrosing interstitial lung disease, AE-SAID-ILD: acute exacerbation of systemic autoimmune disease-related interstitial lung diseases
Mortality rate and prognostic factors in all patients with AE-SAID-ILD
Fifteen of the 25 patients died of respiratory failure, one died of lung cancer, one died of lower intestine bleeding, and one died of multiple cerebral embolisms during the whole observation period. The survival curves within 90 days after the onset of AE are shown in Fig. 3. Thirteen patients died within 90 days, and the 90-day survival rate after the onset of AE was 48% in patients with AE-SAID-ILD (Fig. 3A). Eleven of the 13 patients (84.6%) died of respiratory failure, one died of lower intestine bleeding, and one died of multiple cerebral embolisms within 90 days (Supplementary Fig. 1). Patient survival was not affected by the presence of PF-ILD (Fig. 3B, log-rank p = 0.316). Patients with the GAP stage 1 or JRS severity stage 1 before AE had significantly better survival (Fig. 3C, p = 0.030 and 3D, p = 0.039, respectively). Furthermore, a higher peripheral blood WBC count at AE (Fig. 3E, p = 0.006), and especially a higher neutrophil count (Fig. 3F, p = 0.002), were associated with significantly worse survival. However, survival was not related to serum S100A8, which is produced by activated neutrophils (p = 0.239, data not shown). Regarding treatments at AE, all of patients received steroid-pulse therapy followed by a tapering dose of prednisolone. The addition of immunosuppressants, mainly intravenous cyclophosphamide, did not improve survival (Fig. 3G, p = 0.968). In addition, treatment with PMX-DHP overall at AE did not significantly improve survival (p = 0.629, data not shown); however, commencement of PMX-DHP within 3 days after admission significantly improved the 90-day survival (Fig. 3H, p = 0.022).

Kaplan–Meier survival curves in patients with AE-SAID-ILD. A) Ninety-day survival rate in patients with AE-SAID-ILD. B) Ninety-day survival was unaffected by the presence of PF-ILD (log-rank p = 0.316). Ninety-day survival according to C) GAP stage (p = 0.030) and D) JRS severity stage (p = 0.039) within 12 months before AE. Ninety-day survival in relation to E) peripheral WBC count (p = 0.006) and F) neutrophil count (p = 0.002). All patients received steroid-pulse therapy followed by a tapering dose of prednisolone. Ninety-day survival in relation to addition of G) immunosuppressants, mainly intravenous cyclophosphamide (p = 0.968) and H) PMX-DHP within 3 days after admission (p = 0.022). Abbreviations: AE-SAID-ILD: acute exacerbation of systemic autoimmune disease-related interstitial lung diseases, PF-ILD: progressive fibrosing interstitial lung disease, GAP: gender, age, and physiology, JRS: Japanese Respiratory Society, PMX-DHP: direct haemoperfusion with a polymyxin B-immobilised fibre column
We also evaluated prognostic factors using Cox proportional hazards models. The results of univariate Cox proportional hazards models of mortality in AE-SAID-ILD are shown in Table 2. JRS severity grade before AE (3/4 vs. 1/2, HR 10.97, p = 0.016) and peripheral blood WBC and neutrophil counts at AE (high vs. low based on median value, HR 6.350, p = 0.005 and HR 13.27, 95%CI 2.447–246, p = 0.001, p = 0.001, respectively) were significant prognostic factors. Serum S100A8 level at AE was not a significant factor (high vs. low, p = 0.239). Regarding treatments, the addition of immunosuppressants to corticosteroids was not a significant factor (p = 0.968), and although the treatment with PMX-DHP overall was not significant, commencement of treatment with long-duration PMX-DHP within 3 days after admission was a significant prognostic factor (HR 0.105, 95%CI 0.005–0.858, p = 0.035). Furthermore, serum lactate dehydrogenase 2 days after starting treatments for AE was a significant prognostic factor (HR 1.005, p = 0.006). Multivariate Cox proportional hazards models were not carried out due to a lack of statistical power.
Discussion
In the present study, we retrospectively evaluated 232 patients with SAID-ILD, including CTD- and MPA-related ILD, of whom 25 had AE-SAID-ILD. Among these 25 patients, RA was the most common baseline disease (68%), and the frequency of AE was significantly higher among patients with RA/MPA/SSc-ILD compared with other AE-SAID-ILD. The proportion of patients fulfilling the criteria for PF-ILD was 20%, and the 90-day survival rate was as low as 48.0%. Furthermore, more-severe ILD before AE, a higher neutrophil count at AE, and early commencement (within 3 days after admission) of long-duration PMX-DHP were significant prognostic factors. To the best of our knowledge, this study provides the first detailed evidence for the incidence of each AE-SAID-ILD and the proportion of PF-ILD in patients with AE-SAID-ILD.
Most of the 25 patients with AE-SAID-ILD were elderly males with an ex/current smoking history, in contrast to patients with common CTDs who tend to be young, females with a no-smoking history. Although the total reported incidence of AE-CTD-ILD or AE-SAID-ILD is lower than that of AE-IPF [9, 11,12,13], the incidences of each AE-SAID-ILD remain unclear because of their rarity. Furthermore, even among patients with IIPs, the incidence of AE-ILD was significantly lower among patients who met the criteria for interstitial pneumonia with autoimmune features (IPAF) compared with those without IPAF [8]. Autoimmune features may thus prevent exacerbation of ILD in both SAID and IPAF. In the present study, the incidence of AE of RA/MPA/SSc-ILD was significantly higher than that of other AE-SAID-ILD. Regarding the disease stage at which AE-ILD occurs, we previously reported that patients with AE-SAID-ILD had a significantly higher %FVC before AE compared with AE-IPF patients [12], suggesting that AE-SAID-ILD appears suddenly even in its earlier stage compared with patients with AE-IPF, although the mechanism remains unclear.
In terms of PF-ILD, the term progressive pulmonary fibrosis (PPF) was also recently proposed in international guideline [30] and PF-ILD/PPF are attracting attention. While most IPF patients show slow disease progression and IPF is the most representative disease of PF-ILD [31], PF-ILD accounts for 24%-31% in patients with CTD-ILD [32, 33]. However, the proportion of PF-ILD in the current study was not particularly high (20%), even in patients with AE-SAID-ILD. These results suggest that PF-ILD may not be strongly related to the occurrence of AE-SAID-ILD.
AE-SAID-ILD is deemed to be related to high levels of inflammation. Patients with AE-SAID-ILD accordingly had higher neutrophil counts and higher C-reactive protein at AE compared with patients with AE-IPF. This high inflammatory status mimic infectious diseases, leading to a delay in the appropriate treatments for AE-ILD [12]. The peripheral blood neutrophil count and CRP were apparently high at AE in the current study; however, the addition of immunosuppressants, mainly intravenous cyclophosphamide, to corticosteroid-pulse therapy did not improve the poor prognosis. The addition of cyclophosphamide to corticosteroids also failed to improve the prognosis in patients with AE-IPF [34, 35]. Novel treatments, other than immunosuppressants, are therefore warranted for the treatments of AE-ILD. In the pathogenesis of AE-IPF, neutrophils infiltrate the alveolar wall and play a role in the progression of diffuse alveolar damage, especially in the very early phase of AE-IPF [22, 36]. Treatment with long-duration PMX-DHP was previously shown to remove activated neutrophils [37] and improve survival in patients with AE-IPF [28, 29, 38] or AE-unclassifiable IIP [10]. In the current study, early commencement (within 3 days after admission) of long-duration PMX-DHP also significantly improved survival. Long-duration PMX-DHP thus seems to be a novel therapeutic option for AE-SAID-ILD. In addition, antifibrotic agents, such as nintedanib and pirfenidone, may also be novel treatments for AE-ILD, given that baseline antifibrotic therapy decreased the incidence of AE-IPF [39, 40], and improved survival after the onset of AE-IPF [34, 40]. These new treatments may improve the currently poor prognosis of patients with AE-ILD better than immunosuppressants.
This study had several limitations. First, the number of patients with AE-SAID-ILD was small because of the rarity of the condition. Second, the data were collected retrospectively. Finally, the treatments for AE-SAID-ILD varied, and notably, only one patient in the study received an antifibrotic agent before AE-SAID-ILD. A larger prospective study is therefore needed to assess the precise effects of treatments on AE-SAID-ILD.
In conclusion, we retrospectively evaluated 232 patients with SAID-ILD for a long period, and found 25 patients with AE-SAID-ILD. AE was significantly more common among patients with RA/MPA/SSc-ILD compared with other AE-SAID-ILD. The proportion of patients fulfilling the criteria for PF-ILD was 20%. More-severe ILD before AE, a higher neutrophil count at AE, and early commencement (within 3 days after admission) of long-duration PMX-DHP were significant prognostic factors. These findings imply that more attention should be paid to AE-ILD in patients with RA, MPA, or SSc, and the removal of activated neutrophils may be a promising treatment for improving respiratory condition in patients with AE-SAID-ILD. This information should aid the management of patients with AE-SAID-ILD. However, further prospective studies are needed to identify effective treatments, such as PMX-DHP and antifibrotic agents, to improve the currently poor survival of patients with AE-SAID-ILD.
Availability of data and materials
The data underlying this article cannot be shared publicly due to the protection of privacy in individuals that participated in the study. The data will be shared on reasonable request to the corresponding author.
Abbreviations
- AE:
-
Acute exacerbation
- CTD-ILD:
-
Connective tissue disease-related interstitial lung disease
- CRP:
-
C-reactive protein
- DLCO :
-
Diffusion lung capacity for carbon monoxide
- FVC:
-
Forced vital capacity
- GAP:
-
Gender, age, and physiology
- HRCT:
-
High-resolution computed tomography
- JRS:
-
Japanese Respiratory Society
- KL-6:
-
Krebs von den Lungen-6
- LDH:
-
Lactate dehydrogenase
- MPA:
-
Microscopic polyarteritis
- Neut:
-
Neutrophils
- P/F:
-
PaO2/FiO2
- PF-ILD:
-
Progressive fibrotic interstitial lung disease
- PM/DM:
-
Polymyositis/dermatomyositis
- PMX-DHP:
-
Direct haemoperfusion with a polymyxin B-immobilised fibre column
- pSS:
-
Primary Sjögren syndrome 0.426
- RA:
-
Rheumatoid arthritis
- SAID:
-
Systemic autoimmune disease
- SP-D:
-
Surfactant protein D
- SSc:
-
Systemic sclerosis
- UIP:
-
Usual interstitial pneumonia
- WBC:
-
White blood cells
References
Kim DS, Park JH, Park BK, Lee JS, Nicholson AG, Colby T. Acute exacerbation of idiopathic pulmonary fibrosis: frequency and clinical features. Eur Respir J. 2006;27(1):143–50.
Song JW, Hong SB, Lim CM, Koh Y, Kim DS. Acute exacerbation of idiopathic pulmonary fibrosis: incidence, risk factors and outcome. Eur Respir J. 2011;37(2):356–63.
Collard HR, Moore BB, Flaherty KR, Brown KK, Kaner RJ, King TE Jr, Lasky JA, Loyd JE, Noth I, Olman MA, et al. Acute exacerbations of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2007;176(7):636–43.
Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, Colby TV, Cordier JF, Flaherty KR, Lasky JA, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183(6):788–824.
Kakugawa T, Sakamoto N, Sato S, Yura H, Harada T, Nakashima S, Hara A, Oda K, Ishimoto H, Yatera K, et al. Risk factors for an acute exacerbation of idiopathic pulmonary fibrosis. Respir Res. 2016;17(1):79.
Ley B, Collard HR, King TE Jr. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431–40.
Natsuizaka M, Chiba H, Kuronuma K, Otsuka M, Kudo K, Mori M, Bando M, Sugiyama Y, Takahashi H. Epidemiologic survey of Japanese patients with idiopathic pulmonary fibrosis and investigation of ethnic differences. Am J Respir Crit Care Med. 2014;190(7):773–9.
Enomoto N, Homma S, Inase N, Kondoh Y, Saraya T, Takizawa H, et al. Prospective nationwide multicentre cohort study of the clinical significance of autoimmune features in idiopathic interstitial pneumonias. Thorax. 2022;77:143–153.
Park IN, Kim DS, Shim TS, Lim CM, Lee SD, Koh Y, Kim WS, Kim WD, Jang SJ, Colby TV. Acute exacerbation of interstitial pneumonia other than idiopathic pulmonary fibrosis. Chest. 2007;132(1):214–20.
Enomoto N, Naoi H, Aono Y, Katsumata M, Horiike Y, Yasui H, Karayama M, Hozumi H, Suzuki Y, Furuhashi K, et al. Acute exacerbation of unclassifiable idiopathic interstitial pneumonia: comparison with idiopathic pulmonary fibrosis. Ther Adv Respir Dis. 2020;14:1753466620935774.
Suda T, Kaida Y, Nakamura Y, Enomoto N, Fujisawa T, Imokawa S, Hashizume H, Naito T, Hashimoto D, Takehara Y, et al. Acute exacerbation of interstitial pneumonia associated with collagen vascular diseases. Respir Med. 2009;103(6):846–53.
Enomoto N, Oyama Y, Enomoto Y, Yasui H, Karayama M, Kono M, Hozumi H, Suzuki Y, Furuhashi K, Fujisawa T, et al. Differences in clinical features of acute exacerbation between connective tissue disease-associated interstitial pneumonia and idiopathic pulmonary fibrosis. Chron Respir Dis. 2019;16:1479972318809476.
Suzuki A, Kondoh Y, Brown KK, Johkoh T, Kataoka K, Fukuoka J, Kimura T, Matsuda T, Yokoyama T, Fukihara J, et al. Acute exacerbations of fibrotic interstitial lung diseases. Respirology. 2020;25(5):525–34.
Akiyama M, Kaneko Y. Pathogenesis, clinical features, and treatment strategy for rheumatoid arthritis-associated interstitial lung disease. Autoimmun Rev. 2022;21(5):103056.
Ruaro B, Baratella E, Confalonieri P, Wade B, Marrocchio C, Geri P, Busca A, Pozzan R, Andrisano AG, Cova MA, et al. High-Resolution Computed Tomography: Lights and Shadows in Improving Care for SSc-ILD Patients. Diagnostics (Basel). 2021;11(11):1960.
Hozumi H, Nakamura Y, Johkoh T, Sumikawa H, Colby TV, Kono M, Hashimoto D, Enomoto N, Fujisawa T, Inui N, et al. Acute exacerbation in rheumatoid arthritis-associated interstitial lung disease: a retrospective case control study. BMJ Open. 2013;3(9):e003132.
Qiu M, Jiang J, Nian X, Wang Y, Yu P, Song J, Zou S. Factors associated with mortality in rheumatoid arthritis-associated interstitial lung disease: a systematic review and meta-analysis. Respir Res. 2021;22(1):264.
Orlandi M, Landini N, Sambataro G, Nardi C, Tofani L, Bruni C, Bellando-Randone S, Blagojevic J, Melchiorre D, Hughes M, et al. The role of chest CT in deciphering interstitial lung involvement: systemic sclerosis versus COVID-19. Rheumatology (Oxford). 2022;61(4):1600–9.
Tsuji H, Nakashima R, Hosono Y, Imura Y, Yagita M, Yoshifuji H, Hirata S, Nojima T, Sugiyama E, Hatta K, et al. Multicenter prospective study of the efficacy and safety of combined immunosuppressive therapy with high-dose glucocorticoid, tacrolimus, and cyclophosphamide in interstitial lung diseases accompanied by anti-melanoma differentiation-associated gene 5-positive dermatomyositis. Arthritis Rheumatol. 2020;72(3):488–98.
Sawada T, Inokuma S, Sato T, Otsuka T, Saeki Y, Takeuchi T, Matsuda T, Takemura T, Sagawa A. Study Committee for Leflunomide-induced Lung Injury JCoR: Leflunomide-induced interstitial lung disease: prevalence and risk factors in Japanese patients with rheumatoid arthritis. Rheumatology (Oxford). 2009;48(9):1069–72.
Flaherty KR, Wells AU, Cottin V, Devaraj A, Walsh SLF, Inoue Y, Richeldi L, Kolb M, Tetzlaff K, Stowasser S, et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N Engl J Med. 2019;381(18):1718–27.
Collard HR, Ryerson CJ, Corte TJ, Jenkins G, Kondoh Y, Lederer DJ, Lee JS, Maher TM, Wells AU, Antoniou KM, et al. Acute exacerbation of idiopathic pulmonary fibrosis. an international working group report. Am J Respir Crit Care Med. 2016;194(3):265–75.
Ley B, Ryerson CJ, Vittinghoff E, Ryu JH, Tomassetti S, Lee JS, Poletti V, Buccioli M, Elicker BM, Jones KD, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156(10):684–91.
Homma S, Sugino K, Sakamoto S. Usefulness of a disease severity staging classification system for IPF in Japan: 20 years of experience from empirical evidence to randomized control trial enrollment. Respir Investig. 2015;53(1):7–12.
Enomoto N, Suda T, Kono M, Kaida Y, Hashimoto D, Fujisawa T, Inui N, Nakamura Y, Imokawa S, Funai K, et al. Amount of elastic fibers predicts prognosis of idiopathic pulmonary fibrosis. Respir Med. 2013;107(10):1608–16.
Akira M, Kozuka T, Yamamoto S, Sakatani M. Computed tomography findings in acute exacerbation of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2008;178(4):372–8.
Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48(3):452–8.
Enomoto N, Mikamo M, Oyama Y, Kono M, Hashimoto D, Fujisawa T, Inui N, Nakamura Y, Yasuda H, Kato A, et al. Treatment of acute exacerbation of idiopathic pulmonary fibrosis with direct hemoperfusion using a polymyxin B-immobilized fiber column improves survival. BMC Pulm Med. 2015;15:15.
Enomoto N, Suda T, Uto T, Kato M, Kaida Y, Ozawa Y, Miyazaki H, Kuroishi S, Hashimoto D, Naito T, et al. Possible therapeutic effect of direct haemoperfusion with a polymyxin B immobilized fibre column (PMX-DHP) on pulmonary oxygenation in acute exacerbations of interstitial pneumonia. Respirology. 2008;13(3):452–60.
Raghu G, Remy-Jardin M, Richeldi L, Thomson CC, Inoue Y, Johkoh T, Kreuter M, Lynch DA, Maher TM, Martinez FJ, et al. Idiopathic pulmonary fibrosis (an Update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2022;205(9):e18–47.
Kolb M, Vasakova M. The natural history of progressive fibrosing interstitial lung diseases. Respir Res. 2019;20(1):57.
Wijsenbeek M, Kreuter M, Olson A, Fischer A, Bendstrup E, Wells CD, Denton CP, Mounir B, Zouad-Lejour L, Quaresma M, et al. Progressive fibrosing interstitial lung diseases: current practice in diagnosis and management. Curr Med Res Opin. 2019;35(11):2015–24.
Kwon BS, Choe J, Chae EJ, Hwang HS, Kim YG, Song JW. Progressive fibrosing interstitial lung disease: prevalence and clinical outcome. Respir Res. 2021;22(1):282.
Naccache JM, Jouneau S, Didier M, Borie R, Cachanado M, Bourdin A, et al. Cyclophosphamide added to glucocorticoids in acute exacerbation of idiopathic pulmonary fibrosis (EXAFIP): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. 2022;10(1):26–34.
Hozumi H, Hasegawa H, Miyashita K, Yasui H, Suzuki Y, Kono M, Karayama M, Furuhashi K, Hashimoto D, Enomoto N, et al. Efficacy of corticosteroid and intravenous cyclophosphamide in acute exacerbation of idiopathic pulmonary fibrosis: A propensity score-matched analysis. Respirology. 2019;24(8):792–8.
Tanaka K, Enomoto N, Hozumi H, Isayama T, Naoi H, Aono Y, Katsumata M, Yasui H, Karayama M, Suzuki Y, et al. Serum S100A8 and S100A9 as prognostic biomarkers in acute exacerbation of idiopathic pulmonary fibrosis. Respir Investig. 2021;59(6):827–36.
Abe S, Seo Y, Hayashi H, Matsuda K, Usuki J, Azuma A, Kudoh S, Gemma A. Neutrophil adsorption by polymyxin B-immobilized fiber column for acute exacerbation in patients with interstitial pneumonia: a pilot study. Blood Purif. 2010;29(4):321–6.
Abe S, Azuma A, Mukae H, Ogura T, Taniguchi H, Bando M, Sugiyama Y. Polymyxin B-immobilized fiber column (PMX) treatment for idiopathic pulmonary fibrosis with acute exacerbation: a multicenter retrospective analysis. Intern Med. 2012;51(12):1487–91.
Richeldi L, du Bois RM, Raghu G, Azuma A, Brown KK, Costabel U, Cottin V, Flaherty KR, Hansell DM, Inoue Y, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2071–82.
Kang J, Han M, Song JW. Antifibrotic treatment improves clinical outcomes in patients with idiopathic pulmonary fibrosis: a propensity score matching analysis. Sci Rep. 2020;10(1):15620.
Acknowledgements
This study was assisted by the Study Group on Diffuse Lung Disease and the Scientific Research/Research on Intractable Diseases in the Ministry of Health, Labour and Welfare of Japan. We thank Susan Furness, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
This research was not funded.
Author information
Authors and Affiliations
Contributions
Conception and design: NE. Administrative support: TS. Provision of patients: NE, HN, YM, YT, AF, YA, MK, HY, MK, HH, YS, KF, TF, NI, YN. Collection and assembly of data: NE, HN, YM, TI, YT, AF, YA, KM, MK, HY, MK, HH, YS, KF, TF, NI, YN. Data analysis and interpretation: NE, HN, YM, TI, YT, AF, YA, MK, HY, KM, MK, HH, YS, KF, TF, NI, YN. Manuscript writing: NE, YN, TS. Final approval of manuscript: NE, HN, YM, TI, YT, AF, YA, MK, HY, KM, MK, HH, YS, KF, TF, NI, YN, TS. Guarantor of the paper: TS.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the ethics committee of Hamamatsu University School of Medicine (approval number 18–085). All procedures in this study were performed in accordance with the study protocol and the 1964 Helsinki declaration as amended.
The need for informed consent was waived by the ethics committee of Hamamatsu University School of Medicine, because of the retrospective nature of the study.
Consent for publication
Not applicable.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file1: Supplementary Fig. 1.
Causes of death within 90 days after the onset of AE-SAID-ILD. Thirteen patients died within 90 days. Eleven of the 13 patients (84.6%) died of respiratory failure, one died of lower intestine bleeding, and the other died of multiple cerebral embolisms within 90 days. Abbreviations: AE-SAID-ILD: acute exacerbation of systemic autoimmune disease-related interstitial lung diseases.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Enomoto, N., Naoi, H., Mochizuka, Y. et al. Frequency, proportion of PF-ILD, and prognostic factors in patients with acute exacerbation of ILD related to systemic autoimmune diseases. BMC Pulm Med 22, 387 (2022). https://doi.org/10.1186/s12890-022-02197-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-022-02197-3