
Abstract
Background
Hospital-acquired infections (HAIs) in intensive care units (ICUs) are among the avoidable morbidity and mortality causes. This study aimed at investigating the rate of ICU-acquired infections (ICU-AIs) in Iran.
Methods
For the purpose of this multi-center study, the rate of ICU-AIs calculated based on the data collected through Iranian nosocomial infections surveillance system and hospital information system. The data expanded based on 12 months of the year (13,632 records in terms of “hospital-ward-month”), and then, the last observation carried forward method was used to replace the missing data.
Results
The mean (standard deviation) age of 52,276 patients with HAIs in the ICUs was 47.37 (30.78) years. The overall rate of ICU-AIs was 96.61 per 1000 patients and 16.82 per 1000 patient-days in Iran’s hospitals. The three main HAIs in the general ICUs were ventilator-associated events (VAE), urinary tract infection (UTI), and pneumonia events & lower respiratory tract infection (PNEU & LRI) infections. The three main HAIs in the internal and surgical ICUs were VAE, UTI, and bloodstream infections/surgical site infections (BSI/SSI). The most prevalent HAIs were BSI, PNEU & LRI and eye, ear, nose, throat, or mouth (EENT) infections in the neonatal ICU and PNEU & LRI, VAE, and BSI in the PICU. Device, catheter, and ventilator-associated infections accounted for 60.96, 18.56, and 39.83% of ICU-AIs, respectively. The ventilator-associated infection rate was 26.29 per 1000 ventilator-days. Based on the Pabon Lasso model, the lowest rates of ICU-AIs (66.95 per 1000 patients and 15.19 patient-days) observed in zone III, the efficient area.
Conclusions
HAIs are common in the internal ICU wards. In fact, VAE and ventilator-related infections are more prevalent in Iran. HAIs in the ICUs leads to an increased risk of ICU-related mortality. Therefore, to reduce ICU-AIs, the specific and trained personnel must be responsible for the use of the devices (catheter use and ventilators), avoid over use of catheterization when possible, and remove catheters earlier.
Similar content being viewed by others

Introduction
Hospital-acquired infections (HAIs) in intensive care units (ICUs) are among the avoidable causes of morbidity and mortality, which also lead to increased hospital length of stay (LOS), associated costs, and multiple antibiotic resistance, especially in developing countries [1].
These infections are usually acquired after hospitalization and manifest 48 h after admission to the hospital HAIs define as a infections acquired after admission and occur within 48–72 h after admission to the hospital or up to 6 weeks after discharge [2]. In addition, HAIs by staff or newborn infections occurring during childbirth are also defined as HAIs [3].
Patients in ICUs are twice as likely to face a HAIs than patients in the general wards [4]. The global prevalence of ICU-acquired infections (ICU-AIs) is significantly high, i.e., around 51.4%; moreover, the prevalence of this type of infection is estimated to be 9 to 37% in Europe and the USA [5,6,7]. In addition, in Suetens et al. (2018), the prevalence of ICU-acquired infections was around 20.6% [8]. The most important types of ICU-AIs are ventilator-associated events/ respiratory infections/pneumonia (VAE/VAP), central line-associated bloodstream infections/ septicemia (CLABSI), and catheter-related urinary tract infection (CAUTI) [6]. Ventilator-associated pneumonia accounts for 15% of ICU-AIs [6]. In addition, according to the study by Braga et al. (2018), the most common ICU-acquired infections are VAP and BSIs (53 and 27.6%, respectively) [4].
Recent studies in Iran have shown that the prevalence of HAIs is 1.3 to 10% [9, 10]. Various factors such as the severity of the clinical condition, use of invasive procedures and the type of devices (endotracheal tubes, mechanical ventilation, surgery, central venous catheters, and urinary catheters) play an essential role in increasing the prevalence of HAIs [11, 12].
Hence, HAIs prevention is now a global priority, and the accurate recognition of the magnitude and incidence of HAIs at the national or supranational level using reliable data has become priority for adopting proper infection control measures and reducing the incidence of infection in hospitals, especially in ICU wards. Furthermore, many studies have been performed in Iran at the local and hospital level, but so far, there is no report on the rate of infection at the national level, taking into account all types of infections and by the hospital performance indicators in the ICU wards. Therefore, this study aimed at investigating the rate of ICU-AIs in Iran.
Methods
Data sources
Iranian nosocomial infections surveillance (INIS)
The national nosocomial infections surveillance, using the definitions provided by the national hospital-acquired infections surveillance system (NNIS), registers the different type of infections, including: ventilator-associated events (VAE), catheter-associated urinary tract infections (CAUTI), surgical site infections (SSI), central line-associated bloodstream infections (CLABSI), pneumonia events & lower respiratory tract infection (PNEU & LRI), infection in bone and joint (BJ), central nervous system (CNS), chorionic villus sampling (CVS), eye, ear, nose, throat or mouth (EENT), gastrointestinal system (GI), reproductive system (REPR), and skin and soft tissue (SST). INIS collects data from about 863 hospitals. It records different variables on HAIs in addition to indicators for each ward and hospital including province, university, affiliated organization, age, gender, type of HAIs, number of hospitalizations, patient-day, number of deaths, number of surgeries, date of infection, and devices used (different types of catheters and ventilator) [13]. In general, INIS data covers more than 85% of Iranian hospitals. The lowest coverage is related to army hospitals, which is 71.87%. INIS data cover 80.23, 85.16%, and more than 85% of private hospitals, governmental hospitals and those managed by other organizations, respectively.
Hospital statistics and information system (AVAB)
We also extracted performance indicators, including the average LOS, occupancy rate, and bed turnover from AVAB, a system for monitoring and evaluation of different hospitals which facilitate decision policy making. This system registers the hospital characteristics including province, university, accreditation degree, affiliated organization, type of specialty, activity status, ward type, personnel-to-bed ratio, death to bedridden ratio, doctor-to-bed ratio, nurse-to-bed ratio, number of death, number of surgery and performance indicators including the average hospital length of stay, bed occupancy and bed turnover in about 1007 hospitals in Iran in 2018 [13].
Expanded data and missing data imputation
In this multi-center study, INIS and AVAB used to collect data (including 12,586 records in terms of “hospital-ward-month”) on patients with HAIs from 662 hospitals in 2018. The data expanded based on 12 months of the year (13,632 records in terms of “hospital-ward-month”), and then, the last observation carried forward (LOCF) method used to replace the missing data. In LOCF imputation, first, the data on each variable in each hospital ward sorted in terms of months, and the last observation replaced through the forward method; then, the data on the same variable sorted in a reverse order of months. Then, the previous observation replaced for the missing values through the backward method. Finally, the missing value is replace with the average values obtained in the two steps of forward and backward methods. The hospitals with no data on the number of infections and hospitalizations (in none of the months under the study) were excluded.
Linkage of data sources
In order to link different data sources, we first aggregated the INIS data by summing up the number of patients, number of hospitalizations, and patient-days in each hospital and by the type of ward and the month of diagnosis. In addition, AVAB data was collected as an aggregate data including different variables for each hospital. Then, the two data sources were linked together using a unique code based on the initials of the name of each hospital and the name of the University of Medical Sciences to which the following hospital belonged, using the merge command and as one-to-one key variables by Stata software. Finally, the rate of ICU-AIs calculated using 10,836 records obtained from 579 hospitals.
The national standard for hospital performance indicators
Hospital performance indicators were categorized based on the standards of the Ministry of Health and Medical Education (MOHME) of Iran as follows:
Indicators | Desirable | Moderate | Undesirable |
|---|---|---|---|
Average LOS (day) | < 3.5 | 3.5–4 | > 4 |
Bed occupancy rate (%) | > 70 | 60–70 | < 60 |
Bed turnover rate | > 24 | 17–24 | < 17 |
Death to bedridden ratio (%) | < 2 | 2–3 | > 3 |
Pabon Lasso model is another indicator of hospital performance. Two indices can be used to calculate this model; bed turnover (BTO) and bed occupancy rate (BOR). In this study, the national average of BTO (134.24) and BOR (62.73) was used to plot the Pabon Lasso graphical chart. The plotted Pabon Lasso graph distinguish four zones (zone I, II, III, and IV), where zone I is the inefficient area; hospitals with low BTO and low BOR indicating a surplus of hospital beds relative to the existing demand, zone II is hospitals with high BTO and low BOR (unnecessary hospitalizations, and oversupply of beds), zone III is the efficient area; hospitals with high BTO and high BOR, and zone IV is hospitals with low BTO and high BOR.
Data analysis
Mean, and median (standard deviation and interquartile range) used to describe age and hospitalization length until infection and hospital LOS. The rates of HAIs also calculated as follows:
Rate per patient and patient-days
By each variable, the rate per patient calculated by dividing the total number of patients with ICU-AIs over the total number of hospitalizations, multiplied by 1000. In addition, the rate per patient-days calculated by dividing the total number of patients with ICU-AIs over the total number of patient-days, multiplied by 1000.
Rate per device-days
The rate per device-days by each infection type, calculated by dividing the ICU-AIs over the total device-days, multiplied by 1000. For SSIs, the SSIs were divided by the all surgeries in each hospital. The device-associated infections rate was calculated by dividing the ICU-AIs related to ventilator and catheters over the total device-days, multiplied by 1000 [13]. Data were analyzed using Stata software (version 14).
All procedures performed in the study were approved by the ethical committee of the National Institute for Medical Research Development and all methods were carried out in accordance with relevant guidelines and regulations.
Results
The mean age of the 52,276 patients with HAIs was 47.37 (SD = 30.78) years. The median of hospitalization-infection length and hospital LOS in the patients were 8.28 (IQR = 12.8) days and 21 (IQR = 62.67) days, respectively. Based on the data collected from the 579 hospitals in Iran, the overall rate of ICU-AIs was 96.61 per 1000 patients and 16.82 per 1000 patient-days.
HAIs rate by ward type and type of infection
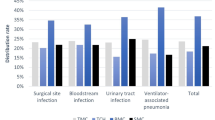
The highest rate of ICU-AIs per 1000 patients and patient-days observed in internal and general ICUs, and the rate of infection in these two wards was higher than the average of national rate (Fig. 1). The most common ICU-AIs were VAE (38.59%; 37.25 per 1000 patients, and 6.49 per 1000 patient-days), UTI (19.76%; 19.09 per 1000 patients, and 3.32 per 1000 patient-days), PNEU & LRI (15.21%; 14.69 per 1000 patients, and 2.55 per 1000 patient-days), and BSI (13.23%; 12.78 per 1000 patients, and 2.22 per 1000 patient-days), respectively (Fig. 2). The three main HAIs in the general ICUs were VAE, UTI, and PNEU & LRI infections. The three main HAIs in the internal and surgical ICUs were VAE, UTI, and BSI/SSI infections. In addition, the most prevalent HAIs were BSI, PNEU & LRI, and EENT infections in the NICU and PNEU & LRI, VAE, and BSI infections in the PICU (Fig. 3).

ICU-acquired infections rate per 1000 patients and 1000 patient-days by type of ICU in Iran hospitals-2018

ICU-acquired infections rate per 1000 patients and 1000 patient-days by type of infection in Iran hospitals-2018

Frequency of main ICU-acquired infections by type of ICU in Iran hospitals-2018
HAIs rate by device-days and device-associated infections
Concerning device-days, the rate of VAE and PNEU & LRI infections was 35.52 per 1000 device-days, and the rate of SSI was 23 per 1000 surgeries (Table 1). Device, catheter, and ventilator-associated infections accounted for 60.96, 18.56, and 39.83% of ICU-AIs. The device-associated infections in ICUs were 7 per 1000 device-days, and the ventilator-associated infections rate was 26.29 per 1000 ventilator-days. The most common catheter-associated infections were umbilical and urinary tract infections (5.87 and 4.93 per 1000 device-days, respectively). The main catheter-associated infections in the internal, general, and pediatric ICUs were urinary and temporary central venous catheter-related infections. However, the main catheter-associated infections in the surgical and neonatal ICUs were urinary and umbilical catheter-related infections (Fig. 4). In addition, the rate of ventilator-associated infections in the internal, surgical, general, pediatric, and neonatal ICUs were 30.41, 28.5, 27.39, 21.56, and 11.7 per 1000 ventilator-days, respectively.

Device-associated infections rate per 1000 device-days by type of ICU in Iran hospitals-2018
HAIs rate by hospital type and affiliation
The rate of ICU-AIs in educational hospitals was higher than in non-educational hospitals (115.45 and 18.42 per 1000 patients and patient-days vs. 79.96 and 14.94 per 1000 patients and patient-days, respectively). The highest rate of ICU-AIs per 1000 patient-days by hospital affiliation observed in semi-government hospitals (19.22 per 1000 patient-days) (Additional file 1: Appendix 1).
HAIs rate by hospital performance indicators
Considering performance indicators including average LOS, bed occupancy, bed turnover, and death to bedridden ratio, the rates of ICU-AIs per 1000 patients were higher in hospitals with an undesirable condition (Fig. 5). In addition, the rates of ICU-AIs per 1000 patient-days by all performance indicators in hospitals with the undesirable condition were higher than the national average rate (Additional file 1: Appendix 2). On the other hand, based on the results of the Pabon Lasso model, the lowest patients per 1000 and patient-days of ICU-AIs were observed in zone III (66.95 and 15.19, respectively) where there were high bed turnover and high bed occupancy rate/efficient (Fig. 6).

ICU-acquired infections rate per 1000 patients by hospital performance indicators in Iran hospitals-2018

ICU-acquired infections rate per 1000 patients and 1000 patient-days by Pabon Lasso in Iran hospitals-2018
HAIs rate by provinces of Iran
Considering the geographic distribution of ICU-AIs, the highest rates of ICU-AIs per 1000 patients observed in Zanjan, Qazvin, Bushehr, and Hormozgan provinces. Also, the rate of HAIs in 16 provinces was higher than the national average rate. Moreover, the highest rates of ICU-AIs per 1000 patient-days observed in Bushehr, Qazvin, South Khorasan, Hormozgan provinces, and the rate of ICU-AIs 19 provinces were higher than the national average rate. The lowest rates of HAIs per 1000 patient-days observed in Sistan and Baluchestan, Kohgiluyeh & Boyer-Ahmad, and Kerman provinces (Additional file 1: Appendix 3).
Discussion
In the present study, the overall rate of ICU-AIs was 96.61 per 1000 patients and 16.82 per 1000 patient-days (5.03 infections per 1000 patient-days), which were different from the rates observed in Korea (2.76 infections per 1000 patient-days), Japan (2.76 infections per 1000 patient-days), and other countries [4, 14, 15].
In addition, the most common ICU-AIs in this study were VAE (38.59%), UTI (19.76%), PNEU & LRI (15.21%), and BSI (13.23%), respectively. However, in studies by Suetens et al. (2018) and Bianco et al. (2018) in Europe, UTIs accounted for about 20% of all HAIs in the ICUs [8, 16]. Furthermore, in report by Despotovic et al. (2020), UTIs accounted for larger than a third of HAIs observed in adults admitted to ICUs [12]. Nevertheless, in study by Braga et al. (2018) in Brazil, the most common ICU-AIs were pneumonia and BSIs (53 and 27.6%, respectively) that are consistent with our results [4]. Studies in India and China have shown that VAP/VAE in intensive care units were 9.4 and 20.8 cases per 1000 ventilator-days, respectively [17, 18].
All invasive devices are associated with an increased risk of ICU-AIs. In this study, device-, catheter-, and ventilator-associated infections accounted for 60.96, 18.56, and 39.83% of ICU-AIs, respectively, though other studies have reported lower rates [19, 20]. In developing countries, the rates of VAP, BSI, and UTI infections have been reported to be 22.9, 11.3, and 9.8 per 1000 device-days, respectively [21], which are higher than the rates observed in our study.
For the purpose of this study, we had access to only one year of national data and therefore we were not able to investigate trends. Although, the current data is the most available registered data which represent the national situation in Iran, its coverage is about 87.5%. It was not possible to compare not covered hospitals with the included ones according to performance indicators. A random selection of all included hospitals provide a national view of ICU-AI in Iran. Third, the diagnosis of HAIs in countries like Iran is suffering from false negative reports and missing data. Therefore, in this study, we limited our studies to ICU-AIs data which is supposed to be more reliable. The missing data in our analyses managed properly. The present study was the first comprehensive and national study conducted on the rate of ICU-AIs, using both patient-days and device-days, which provide more accurate picture of ICU-AIs.
Conclusions
The results showed that HAIs are common in the internal ICU wards, while VAE and ventilator-related infections are more prevalent in Iranian hospitals. Therefore, to reduce ICU-AIs, the specific and trained personnel must be responsible for the use of the devices (catheter use and ventilators), avoid catheterization when possible, and remove catheters earlier. Regular training programs, using standard based on infection control guidelines, must be considered for all personnel involved in providing health care for admitted patients.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AVAB:
-
Hospital statistics and information system
- CAUTI:
-
Catheter-related urinary tract infection
- CLABSI:
-
Central line-associated bloodstream infections / septicemia
- HAIs:
-
Hospital-acquired infections
- ICU-AIs:
-
ICU-acquired infections
- ICUs:
-
Intensive care units
- INIS:
-
Iranian Nosocomial Infections Surveillance
- IQR:
-
Interquartile range
- MOHME:
-
Ministry of Health and Medical Education
- NNIS:
-
National hospital-acquired infections surveillance system
- LOCF:
-
Last observation carried forward
- LOS:
-
Length of stay
- VAE/VAP:
-
Ventilator-associated events / respiratory infections / pneumonia
References
Askarian M, Mahmoudi H, Assadian O. Incidence of nosocomial infections in a big University affiliated Hospital in Shiraz, Iran: a six-month experience. Int J Prev Med. 2013;4:366–72.
Bereket W, Hemalatha K, Getenet B, Wondossen T, Solomon A, Zeynudin A, et al. Update on bacterial nosocomial infections. Euro Rev Med Pharmacolo Sci. 2012;16:1039–44.
Iacovelli V, Gaziev G, Topazio L, Bove P, Vespasiani G, Finazzi AE. Nosocomial urinary tract infections: a review. Urologia. 2014;81(4):222–7. https://doi.org/10.5301/uro.5000092.
Braga I, Campos P, Gontijo-Filho P, Ribas R. Multi-hospital point prevalence study of healthcare-associated infections in 28 adult intensive care units in Brazil. J Hosp Infect. 2018;99(3):318–24. https://doi.org/10.1016/j.jhin.2018.03.003.
Trubiano JA, Padiglione AA. Nosocomial infections in the intensive care unit. Anaesth Intensive Care Med. 2015;16(12):598–602. https://doi.org/10.1016/j.mpaic.2015.09.010.
Edwardson S, Cairns C. Nosocomial infections in the ICU. Anaesth Intensive Care Med. 2019;20(1):14–8. https://doi.org/10.1016/j.mpaic.2018.11.004.
Prevention ECfD, Control. Point prevalence survey of healthcare associated infections and antimicrobial use in European acute care hospitals. ECDPC: Stockholm; 2013.
Suetens C, Latour K, Kärki T, Ricchizzi E, Kinross P, Moro ML, et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: results from two European point prevalence surveys, 2016 to 2017. Eurosurveillance. 2018;23(46):1800516.
Askarian M, Yadollahi M, Assadian O. Point prevalence and risk factors of hospital acquired infections in a cluster of university affiliated hospitals in shiraz. Iran J Infect Public Health. 2012;5(2):169–76. https://doi.org/10.1016/j.jiph.2011.12.004.
Rajabi M, Esmaeili Abdar M, Rafiei H, Aflatoonia MR, Esmaeili AZ. Nosocomial infections and epidemiology of antibiotic resistance in teaching hospitals in south east of Iran. Global J Health Sci. 2016;8(2):190–7.
Brunner L, Smeltzer S. Brunner & Suddarth’s textbook of medical-surgical nursing. 12th ed. Philadelphia: WoltersKluwer/Lippincott Williams & Wilkins, c; 2010.
Despotovic A, Milosevic B, Milosevic I, Mitrovic N, Cirkovic A, Jovanovic S, et al. Hospital-acquired infections in the adult intensive care unit—epidemiology, antimicrobial resistance patterns, and risk factors for acquisition and mortality. Am J Infect Control. 2020;48(10):1211–5. https://doi.org/10.1016/j.ajic.2020.01.009.
Izadi N, Eshrati B, Etemad K, Mehrabi Y, Hashemi-Nazari S-S. Rate of the incidence of hospital-acquired infections (HAIs) in Iran based on the data of the national nosocomial infections surveillance. New Microbes New Infect. 2020;100768.
Chiang CH, Pan SC, Yang TS, Matsuda K, Kim HB, Choi YH, et al. Healthcare-associated infections in intensive care units in Taiwan, South Korea, and Japan: recent trends based on national surveillance reports. Antimicrob Resist Infect Control. 2018;7(1):129. https://doi.org/10.1186/s13756-018-0422-1.
Ling ML, Apisarnthanarak A, Madriaga G. The burden of healthcare-associated infections in Southeast Asia: a systematic literature review and meta-analysis. Clin Infect Dis. 2015;60(11):1690–9. https://doi.org/10.1093/cid/civ095.
Bianco S, Buzzelli M, Schettini R. Multiscale fully convolutional network for image saliency. J Electron Imag. 2018;27(5):051221.
Mehta Y, Jaggi N, Rosenthal VD, Kavathekar M, Sakle A, Munshi N, et al. Device-associated infection rates in 20 cities of India, data summary for 2004-2013: findings of the international nosocomial infection control consortium. Infect Control Hosp Epidemiol. 2016;37(2):172–81. https://doi.org/10.1017/ice.2015.276.
Tao L, Hu B, Rosenthal VD, Gao X, He L. Device-associated infection rates in 398 intensive care units in Shanghai, China: international nosocomial infection control consortium (INICC) findings. IJID. 2011;15(11):e774–80. https://doi.org/10.1016/j.ijid.2011.06.009.
Centers for Disease Control and Prevention, USA. National Healthcare Safety Network Reports. Available at: https://www.cdc.gov/nhsn/datastat/index.html. Accessed 14 Apr 2020.
European Centre for Disease Prevention and Control. Healthcare-associated infections acquired in intensive care units - Annual Epidemiological Report for 2015. Available at: https://ecdc.europa.eu/en/publications-data/healthcare-associated-infections-acquired-intensive-care-units-annual. Accessed 30 Apr 2020.
Allegranzi B, Nejad SB, Combescure C, Graafmans W, Attar H, Donaldson L, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377(9761):228–41. https://doi.org/10.1016/S0140-6736(10)61458-4.
Acknowledgments
This paper was extracted from an epidemiology graduate thesis. We would like to express our thanks to all the staff of the Iranian nosocomial infections surveillance hospital and statistics and information system department of the ministry of health, Iran, as well as to all individuals helping us in completing this research project.
Funding
This study was supported by National Institute for Medical Research Development Grant No 988979. The funding agency did not play any role in the planning, conduct, and reporting or in the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
N. I: Contribution to study concept and design, acquisition, analysis and interpretation of data, drafting of the manuscript. B. E: Contribution to study concept and design, acquisition, analysis, and interpretation of data. Y. M: Contribution to analysis and interpretation of data. K. E: Contribution to the drafting of the manuscript. SS. HN: Contribution to study concept and design, acquisition, analysis and interpretation of data, drafting of the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in the study were approved by the ethical committee of the National Institute for Medical Research Development. Also informed consent was obtained from all participants. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable. The manuscript does not contain patient identifiable data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix 1.
ICU-acquired infections rate per 1000 patients and 1000 patient-days by hospital affiliation in Iran hospitals-2018. Appendix 2. ICU-acquired infections rate per 1000 patient-days by hospital performance indicators in Iran hospitals-2018. Appendix 3. ICU-acquired infections rate per 1000 patients and 1000 patient-days by the province in Iran hospitals-2018.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Izadi, N., Eshrati, B., Mehrabi, Y. et al. The national rate of intensive care units-acquired infections, one-year retrospective study in Iran. BMC Public Health 21, 609 (2021). https://doi.org/10.1186/s12889-021-10639-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-021-10639-6