
Abstract
Background
High occupational burnout among general practitioners (GPs) is an important challenge to China’s efforts to strengthen its primary healthcare delivery; however, data to help understand this issue are unavailable. This study aimed to investigate the prevalence of burnout and associated factors among GPs.
Methods
A cross-sectional design was used to collect data from December 12, 2014, to March 10, 2015, with a self-administered structured questionnaire from 1015 GPs (response rate, 85.6%) in Hubei Province, Central China. Burnout was measured using a 22-item Maslach Burnout Inventory-Human Services Survey (MBI-HSS). MBI-HSS scores and frequency were analyzed by the three dimensions of emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA). Factors associated with burnout among GPs were estimated using a multiple linear regression model.
Results
Of the respondents, 2.46% had a high level of burnout in all three dimensions, 24.83% reported high levels of EE, 6.21% scored high on DP, and 33.99% were at high risk of PA. GPs who were unmarried, had lower levels of job satisfaction, and had been exposed to workplace violence experienced higher levels of burnout. Intriguingly, no statistically significant associations were found between burnout and the duration of GP practice, age, sex, income, practice setting, and professional level.
Conclusion
This is the first study of occupational burnout in Chinese general practice. Burnout is prevalent among GPs in Hubei, China. Interventions aimed at increasing job satisfaction, improving doctor-patient relationships and providing safer workplace environments may be promising strategies to reduce burnout among GPs in Hubei, China.
Similar content being viewed by others

Background
Burnout is a psychological syndrome that is a reaction to the accumulation and long-term negative effect of chronic work-related stress [1]. It is a syndrome characterized by feelings of overextension and the depletion of resources (emotional exhaustion), negative or callous responses to job responsibilities (depersonalization), and feelings of incompetence and a lack of achievement (decreased personal accomplishment) [2]. Burnout has been shown to exert an adverse effect on organizations (e.g., turnover, higher absenteeism, lack of job commitment, and job dissatisfaction), the mental and physical health of healthcare practitioners, and the quality of healthcare delivery [2,3,4,5,6,7]. Therefore, the primary prevention of occupational burnout should be considered as a public health priority worldwide.
Physicians are particularly vulnerable to experiencing burnout due to heavy workloads and high levels of work-related stresses [8]. A previous study found that physicians were significantly more likely than any other occupational group to experience symptoms of burnout [9]. Additionally, the degrees of burnout vary among medical specialties. General practitioners (GPs) have been found to have higher levels of burnout than physicians in other specialties [9,10,11]. Previous studies have mainly focused on burnout and its related factors among GPs in Western countries [10, 12,13,14,15,16,17,18,19,20,21]. GPs are the gatekeepers of the primary healthcare system. The efficiency, effectiveness and quality of a nation’s healthcare system is directly associated with the quality and quantity of its workforce, including GPs. In China, GPs work in Primary Health Institutions (PHIs), Township Health Centers (THCs), and Community Health Centers (CHCs), and mainly provide general medical services such as diagnosis, treatment and prevention of acute and chronic diseases. In addition, they provide referrals to secondary or tertiary hospitals. According to the 2014 Chinese Medical Doctors Association report, 66% of GPs worked more than 40 h per week [22]. These long working hours present a risk for GPs to develop burnout [4, 23,24,25].
Recently, shortages of primary healthcare workers and high GP turnover in China have been major issues. The establishment of a GP team is a key strategy to strengthen PHIs. A high level of burnout among Chinese GPs could lead to a reduction in their numbers of GPs and damage to their well-being, which could consequently affect the quality of health care. The above issues could result in serious repercussions on the country’s healthcare system. Few existing studies in China have focused on data on burnout among physicians, and to date, research has not distinguished between GPs or non-GPs [26]. This study aimed to assess the prevalence of burnout and its relevant predictors among GPs who work in PHIs in Hubei, China.
Methods
Study participants and settings
A cross-sectional study was conducted in Central China from December 2014 to March 2015. With a total of 12 independent variables included in the multivariable analysis model, to detect a 2% (effect size) difference between two subgroups (e.g., men vs. women or respondents with low job satisfaction vs. high job satisfaction) with 95% predictive power, the ideal sample size was 652 (computed by G-Power 3.1).
A stratified random sample design was used. According to the China Health Statistics Yearbook 2013 [27], there were 2325 PHIs in 17 prefecture-level cities of Hubei Province, and all of them were included in this study. According to the number of GPs and the scales of PHIs, we randomly selected 30% of the on-post GPs with at least 1 year of work experience from each sampled PHI. Among the 3752 eligible GPs, 1186 were randomly invited to participate in a training seminar on quality health care organized by the general practice training center of Hubei Province. After the training session, they were asked to complete a self-administered questionnaire. Overall, 1101 GPs participated in the survey. However, 86 questionnaires were excluded because of missing information on burnout (more than two items). Finally, 1015 eligible GPs were included in the analysis (response rate, 85.6%).
All respondents provided written informed consent, and the study was approved by the Ethics Committee of the Tongji Medical College Institutional Review Board, Huazhong University of Science and Technology (Wuhan, China).
Questionnaire design and content
The questionnaire was designed based on literature reviews, group discussions, and mock interviews. Furthermore, a pilot study was conducted in Wuhan’s CHCs to improve the questionnaire’s quality. The questionnaire comprised five sections: sociodemographic information, job satisfaction, burnout, workplace violence, and turnover intention. Given the purpose of this study, the data from sections 1, 2, 3 and 4 were included.
Measurements
Burnout was measured with a standardized scale that consisted of 22 items on a six-point Likert scale ranging from 0 (never) to 6 (every day). Burnout was assessed based on three subscales: emotional exhaustion (EE), depersonalization (DP), and personal achievement (PA) were measured with the 22-item Maslach Burnout Inventory (MBI-HSS) [28]. Higher scores on the EE and DP subscales were positively associated with higher levels of burnout, while PA was inversely associated with burnout.
In the analysis of the prevalence of burnout, we analyzed the subscales as categorical variables. The cut-off points for different categories (low, moderate, and high) of each subscale were defined in the study according to the MBI-HSS scoring guidelines [29]. GPs were categorized as having a high level of burnout if they scored high on EE and DP and low on PA. In this study, the Cronbach’s alpha coefficients for the MBI-HSS, EE, DP, and PA were 0.85, 0.91, 0.87 and 0.90, respectively, suggesting that the overall measurement was reliable.
We used the Chinese version of the Workplace Violence Scale developed by Wang et al. [30] consisting of 5 items on a four-point Likert scale ranging from 0 (never) to 3 (more than 3 times/year). Workplace violence included physical violence (physical and sexual assaults) and nonphysical violence (verbal abuse, threats, and sexual harassment). Workplace violence, as an independent variable of burnout, was recoded into yes (encountering one type of workplace violence) and no (not experiencing any type of workplace violence) for the statistical analyses.
Search strategy
We searched PubMed for similar studies that were conducted in the field between the 1990s and 2018 to compare the prevalence and scores of burnout among GPs in China and other countries.
Statistical analysis
Student’s t test and a one-way analysis of variance (ANOVA) were applied to examine the differences in burnout and its subscales among groups. Dependent variables (EE, DP, PA, and overall burnout) were treated as continuous variables. A multiple linear regression model was performed to estimate the predictors of GPs’ burnout and its three subscales. Predictive variables such as age (continuous), gender, marital status, education level, work tenure, average monthly income, contract status, professional level, managerial responsibility, practice setting, job satisfaction, and workplace violence were included in the multiple linear regression analysis. All statistical analyses were performed with Statistical Analysis System (SAS) version 9.2 (SAS Institute Inc., Cary, NC, USA). Statistical significance was accepted at the 5% level (P < 0.05).
Results
Table 1 shows the basic characteristics of the study respondents. Of the 1015 respondents, most were married (91.92%) and more than half were men. Half of respondents were 40 years or older, and 52.10% had a bachelor’s degree or above. Among the respondents, the mean time (standard deviation, SD) in the profession was 16.32 (7.90) years. More than half (55.47%) of the respondents worked in general practice settings in urban areas. In total, 62.2% of the respondents reported exposure to workplace violence in the preceding year.
The participants’ mean scores were 18.70 (SD = 12.06; range = 0–54) on the EE subscale, 3.89 (SD = 4.75; range = 0–30) on the DP subscale, and 34.44 (SD = 11.78; range = 0–48) on the PA subscale. This represents a pattern of moderate EE, low DP, and moderate PA. Higher mean scores of burnout were found among respondents who were male, married, and had experienced workplace violence.
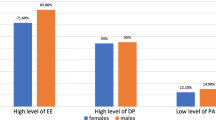
Table 2 shows the prevalence rate of burnout and its subscale among GPs. Among the GPs, 24.83% reported high levels of burnout on EE and 6.21% reported high levels on DP, and 33.99% exhibited reduced feelings of PA. In total, 35% of the respondents scored high for burnout in any dimension, 21% scored high for burnout in at least two dimensions, and 2.46% scored high for all three dimensions.
The factors associated with GPs’ burnout and the three subscales are presented in Table 3. GPs who were single/divorced-separated, who had a lower level of job satisfaction, and who had experienced workplace violence were more likely to report a higher risk of burnout.
A high professional level was positively associated with EE. Additionally, GPs who reported workplace violence had significantly higher EE scores than those without exposure to workplace violence. Being single, having a lower level of job satisfaction, and having a low professional title were associated with increased DP scores. GPs who experienced workplace violence had significantly higher DP scores than those who did not. In addition, we found that higher PA scores among GPs were associated with a higher level of job satisfaction.
Table 4 summarizes the comparisons between burnout scores and prevalence rates reported previously in some Western countries and the data from the present study.
Discussion
This is the first study to investigate the prevalence of burnout and related factors among GPs in Hubei, China. We found that 2.46% of GPs had a high level of burnout, with 24.83% scoring high for EE, 6.21% scoring high for DP, and 33.99% at a high risk of PA. Being single, having a lower level of job satisfaction, and experiencing workplace violence were significantly associated with a higher risk of burnout. Factors associated with a higher level of EE included a lower level of job satisfaction, a higher professional level, and experiences of workplace violence. Being single, having a lower level of job satisfaction, being at a lower professional level, and having experience of workplace violence were significantly associated with a higher level of DP. However, a lower level of job satisfaction was the only predictor of a higher level of PA.
Comparison with existing literature
Compared to Western countries, our study showed lower mean EE and DP scores and a higher mean PA score. Chinese GPs were also less often categorized as having a high risk of EE and DP. Specifically, our study found that 33.99% of GPs were at high risk of a reduced sense of PA. These differences may be partly attributable to the participants’ demographic factors (age, gender, professional level, and marital status), organizational factors (healthcare system, absence of work incentives (e.g., inadequate income), work time, and career progression), the type of questionnaire, and social support. Reduced PA may reflect reduced feelings of competence and productivity at work, which may lead to a higher risk of depression [2, 31]. Thus, improving the feeling of PA among Chinese GPs is a critical challenge faced by the government of China and calls for greater efforts from health policymakers and researchers.
In line with earlier studies, our findings showed that exposure to workplace violence was associated with a significantly higher risk of burnout in the areas of EE and DP [7, 32, 33]. Workplace violence is a key occupational hazard [34] which is faced by healthcare professionals worldwide and negatively affects healthcare workers’ mental health and general well-being. It has been associated with reduced job satisfaction, commitment and efficiency, poor quality of life, increased stress, sleep disruption, and occupational burnout, and even death [35,36,37,38,39]. Therefore, establishing an alarm and monitoring system and improving the relationship between patients and GPs are urgently needed to reduce violence in general practice.
We observed in the present study that GPs at higher professional levels were prone to higher risk of DP and EE. In China, the higher the GP’s professional level, the heavier his workload [22]. A highly intensive workload not only affects the health of GPs, but also affects the quality of health care [40]. Patients had high expectations of higher-ranking physicians. They preferred the services of GPs with many years of experience or with higher professional titles, even for minor illnesses or self-limited conditions [41, 42]. Thus, heavy workload increases work pressure on physicians, resulting in overwork. Long-term overwork could lead to the rushed, indifferent and disrespectful management of patients, which is a major constraint in the doctor-patient relationship [41]. The above issues could result in an increased likelihood of violence among GPs. In addition, workplace violence has been identified as an important predictor of occupational burnout [43,44,45,46], which is consistent with our findings. More importantly, we found that GPs at a higher professional level were more likely to experience workplace violence (61.8% vs. 38.2%, P < 0.0001).
Expectedly, job satisfaction was identified as a significant predictor of burnout in this study. Previous studies have demonstrated that higher levels of burnout are associated with lower levels of job satisfaction [12, 19, 47]. This finding suggests that an improvement in job satisfaction could serve as an effective way to prevent or minimize burnout, and provides new insights for future studies on ways to improve the job satisfaction of GPs and indirectly address burnout problems.
Limitations
This study has several limitations. First, this study used a cross-sectional study design, which precluded the evaluation of the temporality and causality of the observed relationships. Second, data were collected from participants’ self-reports; thus, recall bias was unavoidable. Third, other potential predictors of burnout and the overall health of GPs (such as work schedules, work hours, work stress, sleep quality, job control, social support, other occupational health factors, self-reported health status, and mental health) were not captured in our questionnaire. Fourth, completing the questionnaire after following a seminar on the quality of health care may have introduced bias. Finally, this study was based on the data of a cross-sectional study conducted from December 2014 to March 2015. There is a seasonal trend in the work load of GPs that may have affected the results.
Implications for research and practice
Based on our findings, we suggest that, first, prospective studies are needed to investigate the association between the determined factors and burnout. Second, this study highlights the need for the investigation or implementation of interventions to improve GPs’ well-being or strategies to reduce work pressure on GPs in China’s primary healthcare settings. Third, a previous study [48] showed that new medical graduates are susceptible to burnout. Additional studies investigating the work demands, job satisfaction, burnout, and turnover intentions of new GPs could provide a valuable insight. Finally, investigating the potential impact of burnout on GPs’ work performance, the quality of patient care delivery, and family life would provide important insights.
Conclusions
In conclusion, burnout among GPs, especially single GPs, GPs with lower job satisfaction, and those with exposure to workplace violence, is prevalent in Hubei, China. In total, 25% of GPs suffered from high levels of EE, 6% suffered from high DP and 34% suffered from reduced PA.
Availability of data and materials
Data may be made available by contacting the corresponding author.
Change history
12 October 2022
A Correction to this paper has been published: https://doi.org/10.1186/s12889-022-14050-7
Abbreviations
- CHC:
-
Community health center
- CHS:
-
Community health service
- DP:
-
Depersonalization
- EE:
-
Emotional exhaustion
- GP:
-
General practitioner
- PA:
-
Personal achievement
- PHI:
-
Primary healthcare institution
- THC:
-
Township health center
References
Jin MU, Jeong SH, Kim EK, Choi YH, Song KB. Burnout and its related factors in Korean dentists. Int Dent J. 2015;65(1):22–31.
Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52(1):397–422.
Shirom A, Melamed S, Toker S, Berliner S, Shapira I. Burnout and health review: current knowledge and future research directions. Int Rev Ind Organ Psychol. 2005;20(1):269.
Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987–93.
Adriaenssens J, De Gucht V, Maes S. Determinants and prevalence of burnout in emergency nurses: a systematic review of 25 years of research. Int J Nurs Stud. 2015;52(2):649–61.
Turnipseed DL. An analysis of the influence of work environment variables and moderators on the burnout syndrome. J Appl Soc Psychol. 1994;24(9):782–800.
Hamdan M, Hamra AA. Burnout among workers in emergency Departments in Palestinian hospitals: prevalence and associated factors. BMC Health Serv Res. 2017;17(1):407.
Kumar S. Burnout and doctors: prevalence, prevention and intervention. Healthcare (Basel). 2016;4(3):37.
Shanafelt TD, Boone S, Tan L, Dyrbye LN, Sotile W, Satele D, West CP, Sloan J, Oreskovich MR. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172(18):1377–85.
Arigoni F, Bovier PA, Mermillod B, Waltz P, Sappino AP. Prevalence of burnout among Swiss cancer clinicians, paediatricians and general practitioners: who are most at risk? Support Care Cancer. 2009;17(1):75–81.
Twellaar M, Winants Y, Houkes I. How healthy are Dutch general practitioners? Self-reported (mental) health among Dutch general practitioners. Eur J Gen Pract. 2008;14(1):4–9.
Soler JK, Yaman H, Esteva M, Dobbs F, Asenova RS, Katic M, Ozvacic Z, Desgranges JP, Moreau A, Lionis C, et al. Burnout in European family doctors: the EGPRN study. Fam Pract. 2008;25(4):245–65.
Orton P, Orton C, Pereira Gray D. Depersonalised doctors: a cross-sectional study of 564 doctors, 760 consultations and 1876 patient reports in UK general practice. BMJ Open. 2012;2:e000274.
Lee FJ, Stewart M, Brown JB. Stress, burnout, and strategies for reducing them What’s the situation among Canadian family physicians? Can Fam Physician. 2008;54(2):234–5.
O’Dea B, O’Connor P, Lydon S, Murphy AW. Prevalence of burnout among Irish general practitioners: a cross-sectional study. Ir J Med Sci. 2017;186(2):447–53.
Goehring C, Bouvier GM, Künzi B, Bovier P. Psychosocial and professional characteristics of burnout in Swiss primary care practitioners: a cross-sectional survey. Swiss Med Wkly. 2005;135(7–8):101–8.
Cathebras P, Begon A, Laporte S, Bois C, Truchot D. Burn out among French general practitioners. Presse Med. 2004;33(22):1569–74.
Grassi L, Magnani K. Psychiatric morbidity and burnout in the medical profession: an Italian study of general practitioners and hospital physicians. Psychother Psychosom. 2000;69(6):329–34.
Thommasen HV, Lavanchy M, Connelly I, Berkowitz J, Grzybowski S. Mental health, job satisfaction, and intention to relocate - opinions of physicians in rural British Columbia. Can Fam Physician. 2001;47:737–44.
Yaman H, Soler JK. The job related burnout questionnaire. A multinational pilot study. Aust J Gen Pract. 2002;31(11):1055–6.
Kirwan M, Armstrong D. Investigation of burnout in a sample of British general practitioners. Br J Gen Pract. 1995;45(394):259–60.
Chinese Medical Doctor Association. The fifth research reports of Chinese physician practice status 2014. http://www.cmda.net/zlwqgzdt/596.jhtml
McCormack HM, MacIntyre TE, O'Shea D, Herring MP, Campbell MJ. The prevalence and cause(s) of burnout among applied psychologists: a systematic review. Front Psychol. 2018;9:1897.
Wu H, Liu L, Wang Y, Gao F, Zhao X, Wang L. Factors associated with burnout among Chinese hospital doctors: a cross-sectional study. BMC Public Health. 2013;13:786.
Wang ZH, Xie ZY, Dai JM, Zhang LQ, Huang YB, Chen B. Physician burnout and its associated factors: a cross-sectional study in Shanghai. J Occup Health. 2014;56(1):73–83.
Lo D, Wu F, Chan M, Chu R, Li D. A systematic review of burnout among doctors in China: a cultural perspective. Asia Pac Fam Med. 2018;17:3.
National Health and Family Planning Commission of the People's Republic of China. China Statistical Yearbook of Health 2013. Available from http://www.moh.gov.cn.
Maslach C, Jackson SE. The measurement of experienced burnout. J Organ Behav. 1981;2(2):99–113.
Maslach C, Jackson SE, Leiter MP. Maslach burnout inventory. 3rd ed. Menlo Park: Mind Garden Inc.; 1996.
Wang PX, Wang MZ, Hu GX, Wang ZM. Study on the relationship between workplace violence and work ability among health care professionals in Shangqiu City. Wei Sheng Yan Jiu. 2006;35(4):472–4.
Maslach C, Goldberg J. Prevention of burnout: new perspectives. Appl Prev Psychol. 1998;7(1):63–74.
Erdur B, Ergin A, Yuksel A, Turkcuer I, Ayrik C, Boz B. Assessment of the relation of violence and burnout among physicians working in the emergency departments in Turkey. Ulus Travma Acil Cer. 2015;21(3):175–81.
Alameddine M, Kazzi A, El-Jardali F, Dimassi H, Maalouf S. Occupational violence at Lebanese emergency departments: prevalence, characteristics and associated factors. J Occup Health. 2011;53(6):455–64.
Nowrouzi B, Nguyen C, Casole J, Nowrouzi-Kia B. Occupational stress: a comprehensive review of the top 50 annual and lifetime cited articles. Workplace Health Saf. 2017;65(5):197–209.
Wu SY, Lin SW, Li HY, Chai WL, Zhang QH, Wu YH, Zhu W. A study on workplace violence and its effect on quality of life among medical professionals in China. Arch Environ Occup H. 2014;69(2):81–8.
Roche M, Diers D, Duffield C, Catling-Paull C. Violence toward nurses, the work environment, and patient outcomes. J Nurs Scholarsh. 2010;42(1):13–22.
Camerino D, Estryn-Behar M, Conway PM, van Der Heijden BIJM, Hasselhorn HM. Work-related factors and violence among nursing staff in the European NEXT study: a longitudinal cohort study. Int J Nurs Stud. 2008;45(1):35–50.
Isaksson U, Graneheim UH, Richter J, Eisemann M, Astrom S. Exposure to violence in relation to personality traits, coping abilities, and burnout among caregivers in nursing homes: a case-control study. Scand J Caring Sci. 2008;22(4):551–9.
Yang BX, Stone TE, Petrini MA, Morris DL. Incidence, type, related factors, and effect of workplace violence on mental health nurses: a cross-sectional survey. Arch Psychiatr Nurs. 2018;32(1):31–8.
Wada K, Arimatsu M, Yoshikawa T, Oda S, Taniguchi H, Higashi T, Aizawa Y. Factors on working conditions and prolonged fatigue among physicians in Japan. Int Arch Occup Environ Health. 2008;82(1):59–66.
Hesketh T, Wu D, Mao L, Ma N. Violence against doctors in China. BMJ. 2012;345:e5730.
Jiao M, Ning N, Li Y, Gao L, Cui Y, Sun H, Kang Z, Liang L, Wu Q, Hao Y. Workplace violence against nurses in Chinese hospitals: a cross-sectional survey. BMJ Open. 2015;5(3):e006719.
Pihl-Thingvad J, Elklit A, Brandt LPA, Andersen LL. Workplace violence and development of burnout symptoms: a prospective cohort study on 1823 social educators. Int Arch Occup Environ Health. 2019;92(6):843.
Chen S, Lin S, Ruan Q, Li H, Wu S. Workplace violence and its effect on burnout and turnover attempt among Chinese medical staff. Arch Environ Occup Health. 2016;71(6):330–7.
Deniz T, Saygun M, Eroglu O, Ulger H, Azapoglu B. Effect of exposure to violence on the development of burnoutsyndrome in ambulance staff. Turk J Med Sci. 2016;46(2):296–302.
Kim H, Kim JS, Choe K, Kwak Y, Song JS. Mediating effects of workplace violence on the relationships between emotional labour and burnout among clinical nurses. J Adv Nurs. 2018;74(10):2331–9.
Linzer M, Visser MRM, Oort FJ, Smets EMA, McMurray JE, de Haes HCJM. Predicting and preventing physician burnout: results from the United States and the Netherlands. Am J Med. 2001;111(2):170–5.
Weidner AKH, Phillips RL Jr, Fang B, Peterson LE. Burnout and scope of practice in new family physicians. Ann Fam Med. 2018;16(3):200–5.
Acknowledgements
We thank the general practitioners who participated in this research.
Funding
This study was supported by the National Social Science Foundation of China (18ZDA085) and the Young Scientists Fund of National Natural Science Foundation of China (71804049). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
YG and ZXL conceived and designed the study. YDY, CW, JXL, TTY, SH, HBX, and YYC participated in the acquisition of data. YG analyzed the data. HJ, LQL, and PQF gave advice on methodology. YG wrote the draft of the paper. All authors contributed to writing, reviewing or revising the paper and read and approved the final manuscript. ZXL is the guarantors of this work and has full access to all the data in the study and takes responsibility for its integrity and the accuracy of the data analysis. All authors read and approved the final manuscript
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Tongji Medical College Institutional Review Board, Huazhong University of Science and Technology, Wuhan, China. Informed consent was obtained from all survey participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Gan, Y., Jiang, H., Li, L. et al. Prevalence of burnout and associated factors among general practitioners in Hubei, China: a cross-sectional study. BMC Public Health 19, 1607 (2019). https://doi.org/10.1186/s12889-019-7755-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-019-7755-4