
Abstract
Background
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition characterized by attention problems, excessive physical activity, and impulsivity. ADHD affects not only the patients but also their families. The development and use of technologies such as virtual reality (VR), augmented reality (AR), and mixed reality (MR) for ADHD has increased over recent years. However, little is known about their potential usefulness. This overview aimed to clarify the current knowledge about the use of these three innovative technologies for the diagnosis and treatment of children with ADHD.
Methods
This overview was conducted using the PubMed, Web of Science, and Scopus databases until January 24th, 2021. The following descriptive information was compiled from the identified studies: country, year of publication, sample size, study design, ADHD diagnosis methods, applied technology, hardware equipment, clinical target, and main findings.
Results
The initial database searches yielded 409 articles, but 103 were removed as duplicates. Eventually, 30 eligible studies remained for analysis, the majority of which were case-control (n = 22, 73%). Regarding the applied technology/hardware equipment, VR (n = 27; 90%), head-mounted displays (n = 19, 63%), VR-based continuous performance tests (VR-CPT) (n = 21, 70%) were most frequently used. Most studies (n = 21, 70%) used the DSM criteria for the diagnosis of childhood ADHD. They primarily evaluated the utility of these technologies in assessing ADHD symptoms (n = 10, 33%) and improving the ADHD diagnostic process (n = 7, 23%).
Conclusion
This comprehensive overview evaluated the studies on the use of VR, AR, and MR technologies for children with ADHD. These technologies seem to be promising tools for improving the diagnosis and management of ADHD in this population.
Similar content being viewed by others


Introduction
Attention deficit hyperactivity disorder (ADHD) is a prevalent mental disorder in children and adults [1] with its prevalence rate varying among different age groups [2]. ADHD affects approximately 4–12% of school-aged children worldwide [3, 4]. It is a syndrome characterized by a short attention span, impulsivity, and hyperactivity that often lead to multiple behavioral problems [5]. ADHD is classified into three categories of combined ADHD (highest prevalence), impulsive/hyperactive ADHD, and inattentive/distractible ADHD [6].
ADHD causes primary and secondary complications such as a lack of self-confidence, relationship maladjustment with friends, and incompatibility with social and academic environments [7, 8]. It is also associated with heavy healthcare costs since it increases the risk of major disorders such as depression, bipolar disorder, and anxiety in the patients [9]. ADHD can also contribute to hypertension, obesity, diabetes, asthma, migraine, epilepsy, and dyslipidemias [10]. Therefore, it is essential to properly diagnose the symptoms of this disorder and take effective measures to ameliorate the main symptoms and other clinical comorbidities [11].
Medication and cognitive-behavioral therapy (CBT) [12] are the primary treatment options for ADHD. Psychopharmacological treatment such as the prescription of methylphenidate is not always effective and may have serious side effects [13]. Low medication adherence is another common problem among children diagnosed with ADHD [14]. CBT involves targeted cognitive and behavioral therapeutic measures used for the treatment of multiple psychosocial disorders. In effective CBT, patients must have several sessions with a therapist who specializes in ADHD [15]. Other treatment options such as memory, speech, and family therapy are also effective in diminishing the adverse impact of ADHD symptoms on children [16, 17]. Unfortunately, these primary treatment options have potential limitations, such as medication side effects, lack of behavioral improvement, high costs, and major time commitments [18, 19]. In the treatment of children with ADHD, it is essential for the children to learn self-control and how to make and keep friends while developing a good sense of self-esteem [20].
Recently, technological advancement has enabled the use of mobile phone applications, telemedicine, computer/mobile games, continuous performance tests (CPT), virtual reality (VR), and augmented classroom simulators for ADHD diagnosis and treatment [21,22,23]. VR is a state-of-the-art, technologically advanced system that simulates three-dimensional (3D) environments in which an individual can become fully immersed and have a realistic experience [24,25,26].
Augmented reality (AR) is a subset of VR consisting of real-world features, digital information, and elements that enable users to interact with virtual objects and view the physical environment [27, 28]. VR transmits information from the physical environment to an entirely virtual world, whereas AR merges virtual objects into a real-world environment [29]. Consequently, VR allows users to feel psychologically immersed in a virtual environment, while AR provides an environment to let users interact with virtual objects in the real world [30]. Mixed reality (MR) falls somewhere between AR and VR as it is a mixture of actual and virtual reality whereby the user can observe the real world as in AR and observe realistic virtual objects as in VR [31, 32]. In other words, MR allows the users to interact with virtual elements within their real-world experience [33].
Several studies have indicated that VR and AR tools are remarkably effective in the promotion of general health, mental health treatment, and diagnosis [34, 35]. VR, AR, and MR have been integrated into the treatment of various mental disorders. For instance, a study by Smith et al. [36] demonstrated that VR could be used for the rehabilitation of patients with schizophrenia. Mclay et al. [37] reported the application of VR for the management of posttraumatic stress disorder (PTSD). Lee et al. [38] and Magrini et al. [39] also employed AR and Liu et al. [40] used MR to improve the symptoms of children with the autism spectrum disorder.
These technologies provide a virtual environment that allows individuals to experience various situations that may be difficult or even impossible to deal with in reality; as such, they are more effective and safer than traditional treatments [41]. In these environments, users can develop different skills and a greater understanding of their problems, which helps them to better control their behavior in similar real-world situations [42, 43].
VR, AR, and MR technologies are particularly effective with the design of attractive virtual environments that engage and increase users’ attention. Several studies have explored the use and effectiveness of VR, AR, and MR technologies in the treatment and diagnosis of children with ADHD [44,45,46]. This study aimed to compile and describe these studies.
Materials and methods
First, we searched for relevant articles on ADHD published until January 24th, 2021, and available on PubMed, Web of Science, and Scopus. The articles were retrieved using various keywords, including ((virtual reality) OR (augmented reality) OR (mixed reality)) AND ((attention deficit hyperactivity disorder) OR (ADHD)). The terms included in the search based on the PICO guideline are presented in Table 1.
Articles were selected in accordance with the PICO guidelines as follows: P-population (children and adolescents aged 4–18 years diagnosed with ADHD), I-intervention (using VR/AR/MR for ADHD diagnosis and management), C-comparison (VR/AR/MR intervention group vs. control group or groups before and after VR/AR/MR intervention), and O-outcome (the main outcomes of VR/AR/MR interventions).
The inclusion criteria were being written in English, with a focus on VR, AR, or MR in ADHD patients, and recruiting patients younger than 18 years. Publications were excluded if they reported no data on VR, AR, and MR outcomes, if they were unavailable in full text, and if they were reviews, abstracts, notes, protocols, letters, or editorials,
Quality assessment
Two independent reviewers (Saeideh Goharinejad and Samira Goharinejad) assessed the methodological quality of the studies based on the Joanna Briggs Institute (JBI) [47]. The JBI has different checklist items for each study design, i.e., case-control, cross-sectional, case studies, and randomized controlled trials. It also evaluates the extent to which a study addresses the potential biases in different aspects of research (e.g., sample size, study design, study procedure, confounding factors, and data analysis) [48].
Results
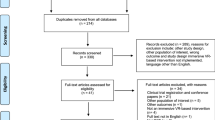
Initially, 409 articles were retrieved from the aforementioned databases. After eliminating 103 duplicates, 306 articles remained, the titles and abstracts of which were screened by two authors independently (Saeideh Goharinejad and Samira Goharinejad). Disagreements were resolved by consulting a third author (Sadrieh Hajsmaeel-Gohari). At this stage, 250 articles were also eliminated as they did not meet the inclusion criteria. Following that, the full texts of the remaining 56 articles were screened by two authors independently (Saeideh Goharinejad and Samira Goharinejad), and 26 articles were eliminated based on the exclusion criteria. Finally, 30 articles were selected for the final review (Fig. 1), and the same two authors independently compiled the descriptive data collected from these articles. This data included the first author’s name, year of publication, country of publication, sample size, study design, ADHD diagnosis methods, clinical target, type of applied hardware technology, type of applied VR, AR, or MR technology, and significant findings.

Flow Chart of Data Collection and Analysis
Twenty-five articles were published after 2010 (83%), 10 (33%) in 2020, four in 2018 and 2019 (13%), and three between 2009 and 2016 (10%) (Fig. 2). In terms of country, the most articles were published in Spain (n = 7; 23%), the United States (n = 4; 13%), and Israel, Korea, and China (all with n = 3; 10%) (Fig. 3).

Year of Publication

Frequency of Articles by Country
In total, 2378 participants were enrolled in the selected studies with ages ranging from 4 to 18 years. The majority of the participants were male (n = 1687; 73%), while two studies did not specify the gender of the participants. The number of the studied patients varied from case studies (n = 2; 7%) to larger samples of > 100 patients (n = 7; 23%) (Table 2).
Twenty-two studies (73%) were case-controls, three (10%) were cross-sectional, two (7%) were case studies, two (7%) were quasi-experimental, and one (3%) was a randomized controlled trial (Table 2).
As for the method of ADHD diagnosis, patients had been diagnosed based on the diagnostic criteria of different versions of the DSM (DSM5 and DSM-IV) in most of the studies (n = 21; 70%). Three studies (10%) did not mention the method of ADHD diagnosis. In the remaining studies, inclusion in the ADHD group was based on interviews with parents and children, parental confirmation, or psychiatrists’ and clinical centers’ diagnoses (Table 2).
With respect to hardware, most of the studies utilized a head-mounted display (HMD) (n = 19; 63%), while others used different 3D glasses, computers, headsets, motion sensors, and robots (Table 2). In terms of the applied technologies, from the 30 studies (n = 27; 90%) utilizing VR, two studies used AR (n = 2; 7%) and only one study employed MR (n = 1; 3%). Notably, these studies used a VR classroom continuous performance test (VR-CPT) (n = 21; 70.0%), a VR classroom (VRC) environment (n = 3; 10%), games (n = 2; 7%), web-based VR (n = 3; 10%), and an AR robot (n = 1; 3%) (Table 2).
The clinical objective of 10 studies (33%) was to evaluate the utility of these technologies in assessing ADHD symptoms, while seven studies (23%) focused on improving the ADHD diagnostic process (Fig. 4). In the current review, we found several studies that employed various types of VR, AR, and MR technologies, such as VR-CPT, VRC, web-based AR, and MR games, for the management of ADHD symptoms (n = 12; 40.0%). These studies included improving concentration (n = 8; 27%) by cognitive therapy [44, 62, 76], eye contact training games [46], memory training [57], and controlling a robot’s movements [45], These studies also focused on the use of VR technologies to improve academic achievement [54, 77], and in improving reading and spelling skills of children with ADHD [73]. In addition, some researchers attempted to assess the effects of medication (n = 2; 6%) [68, 72] and memory capacity (n = 1; 3.%) using these technologies [72] (Fig. 4).

Clinical Target
Significant findings
Most of the reviewed studies (n = 28; 93%) reported that using VR/AR/MR tools helped meet at least one of the clinical objectives of the study. Six of the seven studies (86%) regarding the efficacy of VR/AR/MR technologies in diagnosing ADHD found these technologies to be helpful. Similarly, eight of the nine studies (83%) assessing the ability of these technologies to manage ADHD symptoms found they were beneficial. Using VRC technology, Blume [54] found no difference between proximal and distant seat location on learning outcomes. Tosto [73] reported that training with and without AR had the same outcomes in terms of improving the spelling and reading skills of children with ADHD.
Quality of evidence
Additional file 1 contains the critical appraisal of the reviewed studies. Overall, most of the studies (n = 28; 93%) had a fair quality, and only two studies (7%) implied low/moderate quality. On the other hand, most of the studies (n = 24; 80%), especially case-control and cross-sectional studies, had limitations such as not evaluating the confounding factors and strategies to manage these factors.
Discussion
Recently, VR, AR, and MR technologies have become increasingly accessible to medical researchers seeking to improve diagnostic, therapeutic, and preventive measures for patients with mental disorders [78, 79]. In particular, there has been a growing interest in the use of these technologies for the diagnosis and management of children with ADHD. We conducted a systematic search of the literature focusing on this topic.
According to our findings, VR-, AR-, and MR-based tools can be developed to improve the diagnosis and treatment of children with ADHD. Most of the reviewed studies (90%) revolved around the use of VR. Since MR technology is still in the developmental stages, most of the studies concerning its use are generally descriptive and published in lower-ranking academic journals as opposed to the studies concerning VR and AR [80]. Overall, VR appears to be a more promising technology than AR and MR for clinical purposes. On the other hand, AR and MR integrate virtual and real-world components that might prove helpful in the assessment and management of ADHD and, therefore, further investigations are warranted.
In total, 21 of the reviewed articles (70.0%) focused on the use of VR-CPT, with the first study published in 2007. In contrast, the studies regarding the application of AR and MR for this population have mostly been published in 2020. VR has been incorporated in some neuropsychological tests. Notably, VR-CPT is the most widely used non-traditional tool to diagnose and manage the symptoms of ADHD [52, 69]. In particular, this technology offers better ecological validity since patients’ sustained attention is evaluated in more realistic settings [52, 68].
Given the subjectivity of ADHD interviews and ADHD behavior rating scales, additional and more objective assessment of childhood ADHD has been recommended [81]. Unfortunately, multiple studies concerning the improvement of the ADHD diagnostic process in children have found inconsistent results when it comes to employing both objective and subjective measures [82,83,84]. It is, however, encouraging that according to some studies, compared to traditional CPT instrumentation, VR-CPT has superior efficiency and greater validity for ADHD diagnosis in children [58, 67, 85].
Several studies have concluded that VR-CPT technology is more efficient than traditional CPT in the treatment of children with ADHD [45, 55, 57]. This is partly because VR-CPT evokes more enjoyment in children [69]. VR-CPT technology could reportedly improve concentration for a longer period by training the patient to pay less attention to distractions [49]. Behavior therapy, which encompasses cognitive therapy and social skills training, is also reportedly effective in the rehabilitation of children with ADHD [42]. VR-enhanced behavior therapy might further ameliorate ADHD behavioral symptoms, while also enhancing treatment adherence and motivation in the patients [71]. Several studies have indicated that VR, AR, and MR technologies could incorporate effective instructional strategies to help children with ADHD learn to better manage their symptoms [86, 87]. VR-, AR-, and MR-based applications could also help these patients learn daily life skills and other helpful behaviors, while also improving their concentration and memory [88].
VR-based treatments may also have additional advantages over traditional interventions [89]. For instance, they offer a safe environment for patients and therapists and allow therapists to follow up and evaluate patients’ behavioral changes. Based on the objectives of an intervention, it is possible to modify VR-based treatments for single- or multiple-user applications. In addition, VR-based treatment options could be self-directed or carried out under a therapist’s supervision. Further research in this regard should examine the success of VR, AR, and MR technologies in the rehabilitation therapies conducted at the homes of children with ADHD as well as in clinical settings.
Based on the findings, cost-efficient HMDs are the most frequently used hardware with VR, AR, and MR technologies [90]. Compared to the traditional visualization technology, HMD has more potentials to improve the attention, general behavior, and learning ability of children with ADHD [91, 92].
Besides the merits of the reviewed studies, some of them mentioned limitations as well. First of all, the sample size of patients with ADHD in studies must be expanded to draw more accurate conclusions about the effectiveness of these technologies [50, 51, 58]. Furthermore, studies suggested that it is better to recruit two groups in such interventions to compare and acquire more reliable results [52]. Moreover, the nature of the main treatment (e.g., the time of receiving the medication and its dosage) should be taken into account since they may alter the outcome of intervention [49, 62]. Therefore, future investigations can address these limitations and, thus, improve the quality of research.
Limitations of the study
As the search strategy was mainly focused on the titles and abstracts of relevant articles, some relevant studies may have been missed. In addition, it was not possible to access the full text of six articles, and they were excluded from the study. Potentially relevant non-English articles were excluded as well.
Conclusion
According to the results of the reviewed studies, VR and AR technologies could be used as effective assessment tools to better assess ADHD symptoms and to improve the diagnosis of ADHD in children. Ample evidence also suggests that VR technology could augment traditional treatment options, thereby promoting their effectiveness in the management of ADHD symptoms.
Availability of data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
References
Vitola ES, Bau CH, Salum GA, Horta BL, Quevedo L, Barros FC, et al. Exploring DSM-5 ADHD criteria beyond young adulthood: phenomenology, psychometric properties and prevalence in a large three-decade birth cohort. Psychol Med. 2017;47(4):744–54.
Bachmann CJ, Philipsen A, Hoffmann F. ADHD in Germany: trends in diagnosis and pharmacotherapy: a country-wide analysis of health insurance data on attention-deficit/hyperactivity disorder (ADHD) in children, adolescents and adults from 2009–2014. Dtsch Arztebl Int. 2017;114(9):141.
Polanczyk G, Rohde LA. Epidemiology of attention-deficit/hyperactivity disorder across the lifespan. Curr Opin Psychiatry. 2007;20(4):386–92.
Polanczyk G, De Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatr. 2007;164(6):942–8.
Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159–65.
Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics. 2015;135(4):e994–1001.
Beauchaine TP, Zisner AR, Sauder CL. Trait impulsivity and the externalizing Spectrum. Annu Rev Clin Psychol. 2017;13:343–68.
Harpin VA. The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Arch Dis Child. 2005;90(Suppl 1):i2–7.
Katzman MA, Bilkey TS, Chokka PR, Fallu A, Klassen LJ. Adult ADHD and comorbid disorders: clinical implications of a dimensional approach. BMC Psychiatry. 2017;17(1):302.
Nigg JT. Attention-deficit/hyperactivity disorder and adverse health outcomes. Clin Psychol Rev. 2013;33(2):215–28.
Dias TG, Kieling C, Graeff-Martins AS, Moriyama TS, Rohde LA, Polanczyk GV. Developments and challenges in the diagnosis and treatment of ADHD. Rev Bras Psiquiatr (Sao Paulo, Brazil : 1999). 2013;35(Suppl 1):S40–50.
Evans SW, Owens JS, Bunford N. Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. J Clin Child Adolesc Psychol. 2014;43(4):527–51.
Inglis SK, Carucci S, Garas P, Häge A, Banaschewski T, Buitelaar JK, et al. Prospective observational study protocol to investigate long-term adverse effects of methylphenidate in children and adolescents with ADHD: the attention deficit hyperactivity disorder drugs use chronic effects (ADDUCE) study. BMJ Open. 2016;6(4):e010433.
Sitholey P, Agarwal V, Chamoli S. A preliminary study of factors affecting adherence to medication in clinic children with attention-deficit/hyperactivity disorder. Indian J Psychiatry. 2011;53(1):41–4.
Solanto MV. Cognitive-behavioral therapy for adult ADHD: targeting executive dysfunction. New York: Guilford Press; 2011.
De Meyer H, Beckers T, Tripp G, van der Oord S. Reinforcement contingency learning in children with ADHD: Back to the basics of behavior therapy. J Abnorm Child Psychol. 2019;47(12):1889–902.
Dobrakowski P, Łebecka G. Individualized Neurofeedback training may help achieve long-term improvement of working memory in children with ADHD. Clin EEG Neurosci. 2020;51(2):94–101.
Pozzi M, Carnovale C, Peeters G, Gentili M, Antoniazzi S, Radice S, et al. Adverse drug events related to mood and emotion in paediatric patients treated for ADHD: a meta-analysis. J Affect Disord. 2018;238:161–78.
Zhao X, Page TF, Altszuler AR, Pelham WE 3rd, Kipp H, Gnagy EM, et al. Family burden of raising a child with ADHD. J Abnorm Child Psychol. 2019;47(8):1327–38.
Barba MC, Covino A, De Luca V, De Paolis LT, D’Errico G, Di Bitonto P, et al. BRAVO: a gaming environment for the treatment of ADHD. International Conference on Augmented Reality, Virtual Reality and Computer Graphics. Cham: Springer; 2019. p. 394–407.
Naslund JA, Aschbrenner KA, Araya R, Marsch LA, Unützer J, Patel V, et al. Digital technology for treating and preventing mental disorders in low-income and middle-income countries: a narrative review of the literature. Lancet Psychiatry. 2017;4(6):486–500.
Powell L, Parker J, Harpin V. What is the level of evidence for the use of currently available technologies in facilitating the self-management of difficulties associated with ADHD in children and young people? A systematic review. Eur Child Adolesc Psychiatry. 2018;27(11):1391–412.
Spencer T, Noyes E, Biederman J. Telemedicine in the management of ADHD: literature review of telemedicine in ADHD. J Atten Disord. 2020;24(1):3–9.
Zhou N-N, Deng Y-L. Virtual reality: a state-of-the-art survey. Int J Autom Comput. 2009;6(4):319–25.
Radianti J, Majchrzak TA, Fromm J, Wohlgenannt I. A systematic review of immersive virtual reality applications for higher education: design elements, lessons learned, and research agenda. Comput Educ. 2020;147:103778.
Kyaw BM, Saxena N, Posadzki P, Vseteckova J, Nikolaou CK, George PP, et al. Virtual reality for health professions education: systematic review and Meta-analysis by the digital health education collaboration. J Med Internet Res. 2019;21(1):e12959.
Kaplan AD, Cruit J, Endsley M, Beers SM, Sawyer BD, Hancock PA. The effects of virtual reality, augmented reality, and mixed reality as training enhancement methods: a Meta-analysis. Hum Factors. 2021;63(4):706–26.
Muñoz-Saavedra L, Miró-Amarante L, Domínguez-Morales M. Augmented and virtual reality evolution and future tendency. Appl Sci. 2020;10(1):322.
Jung TH, tom Dieck MC. Augmented reality, virtual reality and 3D printing for the co-creation of value for the visitor experience at cultural heritage places. J Place Manag Dev. 2017;10(2):140–51.
Ferguson C, Davidson PM, Scott PJ, Jackson D, Hickman LD. Augmented reality, virtual reality and gaming: an integral part of nursing. Contemp Nurse. 2015;51(1):1–4.
Mann S, Furness T, Yuan Y, Iorio J, Wang ZJA: All reality: virtual, augmented, mixed (X), Mediated (X, Y), and Multimediated Reality Comput Sci ArXiv 2018, abs/1804.08386.
Mann S, Furness T, Yuan Y, Iorio J, ZJapa W. All reality: virtual, augmented, mixed (x), mediated (x, y), and multimediated reality; 2018.
Speicher M, Hall BD, Nebeling M. What is mixed reality? In: Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems: 2019; 2019. p. 1–15.
Wilson CJ, Soranzo A. The use of virtual reality in psychology: a case study in visual perception. Comput Math Methods Med. 2015;2015:151702.
Freeman D, Reeve S, Robinson A, Ehlers A, Clark D, Spanlang B, et al. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol Med. 2017;47(14):2393–400.
Smith MJ, Fleming MF, Wright MA, Roberts AG, Humm LB, Olsen D, et al. Virtual reality job interview training and 6-month employment outcomes for individuals with schizophrenia seeking employment. Schizophr Res. 2015;166(1–3):86–91.
McLay R, Ram V, Murphy J, Spira J, Wood DP, Wiederhold MD, et al. Effect of virtual reality PTSD treatment on mood and neurocognitive outcomes. Cyberpsychol Behav Soc Netw. 2014;17(7):439–46.
Lee IJ, Chen C-H, Wang C-P, Chung C-H. Augmented reality plus concept map technique to teach children with ASD to use social cues when meeting and greeting. Asia Pac Educ Res. 2018;27(3):227–43.
Magrini M, Curzio O, Carboni A, Moroni D, Salvetti O, Melani A. Augmented interaction Systems for Supporting Autistic Children. Evolution of a multichannel expressive tool: the SEMI project feasibility study. Appl Sci. 2019;9(15):3081.
Liu J, Bian Y, Yuan Y, Xi Y, Geng W, Jin X, et al. Designing and deploying a mixed-reality aquarium for cognitive training of young children with autism spectrum disorder. SCIENCE CHINA Inf Sci. 2020;64(5):154101.
Gongsook P. Time simulator in virtual reality for children with attention deficit hyperactivity disorder. In: International Conference on Entertainment Computing: 2012: Springer; 2012. p. 490–3.
Yeh SC, Tsai CF, Fan YC, Liu PC, Rizzo A. An innovative ADHD assessment system using virtual reality. In: 2012 IEEE-EMBS Conference on Biomedical Engineering and Sciences, IECBES 2012, vol. 2012; 2012. p. 78–83.
Baragash RS, Al-Samarraie H, Moody L, Zaqout F. Augmented reality and functional skills acquisition among individuals with special needs: a Meta-analysis of group design studies. J Spec Educ Technol. 2020;35(3):382–97.
Bioulac S, Micoulaud-Franchi JA, Maire J, Bouvard MP, Rizzo AA, Sagaspe P, et al. Virtual remediation versus methylphenidate to improve distractibility in children with ADHD: a controlled randomized clinical trial study. J Atten Disord. 2020;24(2):326–35.
Arpaia P, Duraccio L, Moccaldi N, Rossi S. Wearable brain-computer Interface instrumentation for robot-based rehabilitation by augmented reality. IEEE Trans Instrum Meas. 2020;69(9):6362–71.
Kim S, Ryu J, Choi Y, Kang Y, Li H, Kim K. Eye-contact game using mixed reality for the treatment of children with attention deficit hyperactivity disorder. IEEE Access. 2020;8:45996–6006.
The Joanna Briggs Institute: Critical Appraisal Tools [https://jbi.global/critical-appraisal-tools].
Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Healthc. 2015;13(3):147–53.
Adams R, Finn P, Moes E, Flannery K, Rizzo A. Distractibility in attention/deficit/hyperactivity disorder (ADHD): the virtual reality classroom. Child Neuropsychol. 2009;15(2):120–35.
Areces D, Rodriguez C, Garcia T, Cueli M, Gonzalez-Castro P. Efficacy of a continuous performance test based on virtual reality in the diagnosis of ADHD and its clinical presentations. J Atten Disord. 2018;22(11):1081–91.
Areces D, Dockrell J, Garcia T, Gonzalez-Castro P, Rodriguez C. Analysis of cognitive and attentional profiles in children with and without ADHD using an innovative virtual reality tool. PLoS One. 2018;13(8):1–18.
Areces D, Rodríguez C, García T, Cueli M. Is an ADHD observation-scale based on DSM criteria able to predict performance in a virtual reality continuous performance test? Appl Sci (Switzerland). 2020;10(7).
Bioulac S, Lallemand S, Rizzo A, Philip P, Fabrigoule C, Bouvard MP. Impact of time on task on ADHD patient's performances in a virtual classroom. Eur J Paediatr Neurol. 2012;16(5):514–21.
Blume F, Göllner R, Moeller K, Dresler T, Ehlis AC, Gawrilow C. Do students learn better when seated close to the teacher? A virtual classroom study considering individual levels of inattention and hyperactivity-impulsivity. Learn Instr. 2019;61:138–47.
Cho BH, Ku J, Jang D, Lee J, Oh M, Kim H, et al. Clinical test for attention enhancement system. Stud Health Technol Inform. 2002;85:89–95.
Clancy TA, Rucklidge JJ, Owen D. Road-crossing safety in virtual reality: a comparison of adolescents with and without ADHD. J Clin Child Adolesc Psychol. 2006;35(2):203–15.
Coleman B, Marion S, Rizzo A, Turnbull J, Nolty A. Virtual reality assessment of classroom - related attention: an ecologically relevant approach to evaluating the effectiveness of working memory training. Front Psychol. 2019;10:1851.
Díaz-Orueta U, Garcia-López C, Crespo-Eguílaz N, Sánchez-Carpintero R, Climent G, Narbona J. AULA virtual reality test as an attention measure: convergent validity with Conners continuous performance test. Child Neuropsychol. 2014;20(3):328–42.
Eom H, Kim KK, Lee S, Hong YJ, Heo J, Kim JJ, et al. Development of virtual reality continuous performance test utilizing social cues for children and adolescents with attention-deficit/hyperactivity disorder. Cyberpsychol Behav Soc Netw. 2019;22(3):198–204.
Fang Y, Han D, Luo H. A virtual reality application for assessment for attention deficit hyperactivity disorder in school-aged children. Neuropsychiatr Dis Treat. 2019;15:1517–23.
Gutiérrez-Maldonado J, Letosa-Porta A, Rus-Calafell M, Penaloza-Salazar C. The assessment of attention deficit hyperactivity disorder in children using continous performance tasks in virtual environments. Anu Psicol. 2009;40(2):211–22.
Hong N, Kim JJ, Kwon JH, Eom H, Kim E. Effect of distractors on sustained attention and hyperactivity in youth with attention deficit hyperactivity disorder using a Mobile virtual reality school program. J Atten Disord. 2021.
Mangalmurti A, Kistler WD, Quarrie B, Sharp W, Persky S, Shaw P. Using virtual reality to define the mechanisms linking symptoms with cognitive deficits in attention deficit hyperactivity disorder. Sci Rep. 2020;10(1):1–9.
Mühlberger A, Jekel K, Probst T, Schecklmann M, Conzelmann A, Andreatta M, et al. The influence of methylphenidate on hyperactivity and attention deficits in children with ADHD: a virtual classroom test. J Atten Disord. 2020;24(2):277–89.
Neguț A, Jurma AM, David D. Virtual-reality-based attention assessment of ADHD: ClinicaVR: classroom-CPT versus a traditional continuous performance test. Child Neuropsychol. 2017;23(6):692–712.
Ou YK, Wang YL, Chang HC, Yen SY, Zheng YH, Lee BO. Development of virtual reality rehabilitation games for children with attention-deficit hyperactivity disorder. J Ambient Intell Humaniz Comput. 2020;11(11):5713–20.
Parsons TD, Bowerly T, Buckwalter JG, Rizzo AA. A controlled clinical comparison of attention performance in children with ADHD in a virtual reality classroom compared to standard neuropsychological methods. Child Neuropsychol. 2007;13(4):363–81.
Pollak Y, Shomaly HB, Weiss PL, Rizzo AA, Gross-Tsur V. Methylphenidate effect in children with ADHD can be measured by an ecologically valid continuous performance test embedded in virtual reality. CNS Spectr. 2010;15(2):125–30.
Pollak Y, Weiss PL, Rizzo AA, Weizer M, Shriki L, Shalev RS, et al. The utility of a continuous performance test embedded in virtual reality in measuring ADHD-related deficits. J Dev Behav Pediatr. 2009;30(1):2–6.
Rodríguez C, Areces D, García T, Cueli M, González-Castro P. Comparison between two continuous performance tests for identifying ADHD: traditional vs. virtual reality. Int J Clin Health Psychol. 2018;18(3):254–63.
Shema-Shiratzky S, Brozgol M, Cornejo-Thumm P, Geva-Dayan K, Rotstein M, Leitner Y, et al. Virtual reality training to enhance behavior and cognitive function among children with attention-deficit/hyperactivity disorder: brief report. Dev Neurorehabil. 2019;22(6):431–6.
Tabrizi M, Manshaee G, Ghamarani A, Rasti J. Comparison of the effectiveness of virtual reality with medication on the memory of attention deficit hyperactivity disorder students. Int Arch Health Sci. 2020;7(1):37–42.
Tosto C, Hasegawa T, Chiazzese G, Treacy R, Merlo G, Chifari A, et al. "AHA - ADHD AUGMENTED" - PARTICIPANTS' CHARACTERISTICS. In: Chova LG, Martinez AL, Torres IC, editors. Edulearn19: 11th International Conference on Education and New Learning Technologies. edn; 2019. p. 5637–45.
Yeh SC, Lin SY, Wu EHK, Zhang KF, Xiu X, Rizzo A, et al. A virtual-reality system integrated with Neuro-behavior sensing for attention-deficit/hyperactivity disorder intelligent assessment. IEEE Trans Neural Syst Rehabil Eng. 2020;28(9):1899–907.
Zulueta A, Díaz-Orueta U, Crespo-Eguilaz N, Torrano F. Virtual reality-based assessment and rating scales in ADHD diagnosis. Psicol Educativa. 2019;25(1):13–22.
Cho BH, Lee JM, Ku JH, Jang DP, Kim JS, Kim IY, et al. Attention enhancement system using virtual reality and EEG biofeedback. In: Loftin B, Chen JX, Rizzo S, Goebel M, Hirose M, editors. Ieee virtual reality 2002, Proceedings. edn; 2002. p. 156–63.
Tosto C, Hasegawa T, Mangina E, Chifari A, Treacy R, Merlo G, et al. Exploring the effect of an augmented reality literacy programme for reading and spelling difficulties for children diagnosed with ADHD. Virtual Reality. 2020;25:879–94.
van Genderen ME, Vlake JH. Virtual healthcare; use of virtual, augmented and mixed reality. Ned Tijdschr Geneeskd. 2018;162:D3229.
Cipresso P, Giglioli IAC, Raya MA, Riva G. The past, present, and future of virtual and augmented reality research: a network and cluster analysis of the literature. Front Psychol. 2018;9:2086.
McMillan K, Flood K, Glaeser RJACM, Ecosystems F. Virtual reality, augmented reality, mixed reality, and the marine conservation movement. Wiley Online Libr. 2017;27:162–8.
Emser TS, Johnston BA, Steele JD, Kooij S, Thorell L, Christiansen HJB, et al. Assessing ADHD symptoms in children and adults: evaluating the role of objective measures. Behav Brain Funct. 2018;14(1):1–14.
Corkum P, Tannock R, Moldofsky H, Hogg-Johnson S, Humphries TJS. Actigraphy and parental ratings of sleep in children with attention-deficit/hyperactivity disorder (ADHD). Sleep. 2001;24(3):303–12.
Manor I, Meidad S, Zalsman G, Zemishlany Z, Tyano S, Weizman AJCp, development h. Objective versus subjective assessment of methylphenidate response. Child Psychiatry Hum Dev. 2008;39(3):273–82.
Choi J, Yoon I-Y, Kim H-W, Chung S, Yoo HJJJoCSM. Differences between objective and subjective sleep measures in children with attention deficit hyperactivity disorder. J Clin Sleep Med. 2010;6(6):589–95.
Shriki L, Weizer M, Pollak Y, Weiss PL, Rizzo AA, Gross-Tsur V. The utility of a continuous performance test embedded in virtual reality in measuring the effectiveness of MPH treatment in boys with ADHD. Harefuah. 2010;149(1):18–23 63.
Thomopoulos SC, Kanellos T, Doulgerakis A, Georgiou E, Bessa M. REEFocus: a VR/AR mixed reality digital game system for non-medication treatment of ADHD and remote monitoring with data privacy and security by design: the FocusLocus approach. In: Smart biomedical and physiological sensor technology XVI, Baltimore, Maryland, United States, 2019, Proceedings Volume 11020.
Kanellos T, Doulgerakis A, Georgiou E, Bessa M, Thomopoulos SCA, Vatakis A, Navarra J. FocusLocus : ADHD management achievement and social inclusion. Smart biomedical And Physiological sensor Technology XV, Greece, 2018, Proceeding Volume 106620E.
Avila-Pesantez D, Rivera LA, Vaca-Cardenas L, Aguayo S, Zuñiga L. Towards the improvement of ADHD children through augmented reality serious games: preliminary results. Proceedings of the 2018 IEEE Global Engineering Education Conference (EDUCON). 18–20 April 2018; Santa Cruz de Tenerife, Canary Islands, Spain. Piscataway: Institute of Electrical and Electronics Engineers; 2018. pp. 843–8.
Bashiri A, Ghazisaeedi M, Shahmorasdi L. The opportunities of virtual reality in the rehabilitation of children with attention deficit hyperactivity disorder: a literature review. Korean J Pediatr. 2017;60(11):337–43.
Grassini S, Laumann KJFIP. Are modern head-mounted displays sexist? A systematic review on gender differences in HMD-mediated virtual reality. Front Psychol. 2020;11:1604.
Grassini S, Laumann K, Rasmussen Skogstad M. The use of virtual reality alone does not promote training performance (but sense of presence does). Front Psychol. 2020;11:1743.
Fonseca D, Navarro I, de Renteria I, Moreira F, Ferrer Á, de Reina O. Assessment of wearable virtual reality Technology for Visiting World Heritage Buildings: an educational approach. J Educ Comput Res. 2018;56(6):940–73.
Acknowledgments
Hereby, we extend our gratitude to the Institute of Futures Studies in Health of Kerman University of Medical Sciences, Iran for providing the research environment.
Funding
None.
Author information
Authors and Affiliations
Contributions
Saeideh Goharinejad, Sadrieh Hajesmaeel-Gohari, and Kambiz Bahaadinbeigy proposed and developed the concept and design of the study. Saeideh Goharinejad and Samira Goharinejad selected and evaluated the collected articles and carried out data compilation. Saeideh Goharinejad, Sadrieh Hajesmaeel-Gohari, and Kambiz Bahaadinbeigy contributed to the drafting of the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
None declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Goharinejad, S., Goharinejad, S., Hajesmaeel-Gohari, S. et al. The usefulness of virtual, augmented, and mixed reality technologies in the diagnosis and treatment of attention deficit hyperactivity disorder in children: an overview of relevant studies. BMC Psychiatry 22, 4 (2022). https://doi.org/10.1186/s12888-021-03632-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-021-03632-1