
Abstract
Purpose
To evaluate the efficacy and safety of transarterial chemoembolization (TACE) combined with camrelizumab (hereafter, TACE-camrelizumab) in the treatment of patients with recurrent hepatocellular carcinoma (R-HCC) after curative resection.
Patients and methods
R-HCC patients who underwent TACE plus camrelizumab or TACE-alone from January 2016 to August 2021 were retrospectively evaluated. Patients were assessed for tumor response, progression-free survival, survival rates and adverse events.
Results
Seventy-one patients were included in this study, including 20 patients in the TACE- camrelizumab group and 51 patients in the TACE-alone group. The objective response rate was 56.9% in the TACE-alone group and 40% in the TACE-camrelizumab group at 3 months (P = 0.201). The disease control rates were 84.3% in TACE-alone group and 80% in TACE-camrelizumab group at 3 months (P = 0.663). The progression-free survival (PFS) of the TACE-alone group was slightly longer than those of the TACE- camrelizumab group (9 months vs. 6 months). However, there were no statistically significant differences in the median PFS (P = 0.586). Similarly, there were no significant differences in the half-year and one-year survival rates (P = 0.304, P = 0.430). Multivariate analysis revealed that Neutrophil-to-lymphocyte ratio (NLR) was associated with PFS significantly. 75% patients developed at least one type of AEs related to camrelizumab in TACE-camrelizumab group, and no patients developed severe AEs.
Conclusion
Comparing with TACE-Alone, the efficacy of TACE-camrelizumab for patients with R-HCC was similar. Meanwhile, the results of this study also indicated that TACE is still a better choice for patients with R-HCC.
Similar content being viewed by others


Introduction
Hepatocellular carcinoma (HCC) is the fifth most common carcinoma and the second leading cause of cancer-related death [1]. Although the recommended first-line treatments for patients with early-stage HCC have the potential to cure patients, 70% of patients have tumor recurrence within five years and only less than 30% of HCC patients can benefit from curative therapies [2, 3]. There have been no established treatments for recurrent HCC, although repeated liver resection remains one of the most effective choices for recurrent HCC treatment in suitable patients. However, due to many factors such as the limited reserve of liver function in the residual liver, postoperative adhesions, and multifocal recurrent tumors, re-resection is only suitable for a small number of patients [4,5,6].
Compared to surgical resection, transarterial chemoembolization (TACE), which combines targeted chemotherapy with ischemic necrosis caused by arterial embolization, is a well-tolerated procedure with limited liver toxicity and can be employed for any type of HCC [5, 7]. Therefore, TACE is widely applicable and practical in patients with intrahepatic HCC recurrence [8,9,10]. Despite that, it is reported that TACE did not have a better survival benefit than liver resection [11, 12]. Based on this, the question of whether TACE combined with other drugs can achieve better efficacy needs to be answered urgently.
In recent years, anti-PD-1 antibodies, including nivolumab, pembrolizumab, and camrelizumab, have demonstrated promising anti-tumor effects as monotherapy for HCC [13,14,15,16]. One study reported last year that nivolumab improved overall survival and progression-free survival in the patients with post-operative recurrence of malignant pleural mesothelioma, and it suggested immune checkpoint inhibitors were helpful for the patients with R-HCC [17]. But the negative results of single-agent ICIs in HCC hinted to us that combined therapy may gain better survival benefits [18, 19]. Fortunately, these kind of immune checkpoint inhibitors (ICIs) that reverse immune exhaustion have been shown to be effective in combination with TACE in the treatment of intermediate and advanced HCC [20]. According to reports, the principle of the combination therapy is that TACE increases tumor-specific CD8 + T cell response by killing HCC cells and causing the release of tumor-associated antigens [21], and increases programmed death receptor 1 (PD-1) and programmed death ligand 1 (PD-L1) expression in HCC [22, 23]. Recently, camrelizumab was approved in China as a second-line treatment for unresectable HCC. It showed high receptor occupancy on circulating T lymphocytes, high affinity for PD-1, and the different binding epitope from that of nivolumab and pembrolizumab [24, 25].
However, as far as we know, no studies have been reported on TACE combined with camrelizumab in R-HCC patients. Therefore, the objective of this study was to assess the efficacy and safety of TACE-camrelizumab verse TACE-alone in R-HCC patients.
Material and methods
Study design and patient selection
We reviewed the medical records of patients with recurrent HCC after curative resection who received treatment with TACE-camrelizumab or TACE-alone between January 2016 and August 2021 at Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. This retrospective study was approved by the institutional review board of the Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. Written informed consent for the patients’ data to be used for research purposes was obtained from all patients prior to treatment.
All of the patients included in this study met the inclusion criteria: (1) Adult patients whose diagnosis of HCC depended on the guidelines of the European Association for the Study of Liver and the American Association for the Study of Liver Disease [1]; (2) Patients were staged at BCLC-B or BCLC-C in accordance with the BCLC system; (3) Child–Pugh class A or B; (4) Eastern Cooperative Oncology Group (ECOG) performance status of 0–1. The exclusion criteria were: (1) Incomplete clinical information; (2) ECOG > 1; (3) Discontinuation of camrelizumab due to serious adverse events (AEs); (4) Loss to follow-up.
TACE procedure
TACE was performed by placing a 5-F catheter (Cook, Bloomington, Indiana, USA) or a 2.7-F microcatheter (Progreat, Terumo, Tokyo, Japan) into hepatic tumor feeding arteries. Initially, an emulsion of 2–20 mL lipiodol and 20–60 mg epirubicin was administered into the target vessels under fluoroscopic guidance. Next, gelatin sponge particles (350–710 μm, Alicon, Hangzhou, China) were administered into the tumor donor arteries. Embolization was operated under fluoroscopic guidance until the stasis of arteries flow was occurred. Finally, reexamination angiography of the hepatic artery was performed to validate the devascularization.
Camrelizumab administration
Patients were treated with camrelizumab within 2–3 weeks after TACE procedure. Camrelizumab was administered intravenously at a dose of 200 mg every 3 weeks. When serious adverse events (AEs) emerged, we reduced the dosage of drugs or interrupted it and symptomatic treatment such as glucocorticoids or immunosuppressant agents were administered, depending on the severity and the affected organs.
Assessment of clinical outcomes and follow-up
All patients were followed up until 31 July 2021. Patients were evaluated every 6–8 weeks with laboratory and abdominal contrast-enhanced CT or MR. Tumor response was evaluated based on Response Evaluation Criteria in Solid Tumors (RECIST 1.1) and Modified RECIST (mRECIST) [26]. However, for consistency, only assessments using mRECIST were summarized in the following section. Follow-up imaging examinations at 3 months were compared with pretreatment imaging to determine objective response rate (ORR) and disease control rate (DCR).
The primary endpoint was progress-free survival (PFS). The secondary endpoints were ORR and DCR. PFS was defined as the period between the date of the initial TACE after being diagnosed with R-HCC and the date of the diagnosis of tumor progression or patient death. The ORR was defined as the percentage of patients with a complete response (CR) or partial response (PR). DCR was defined as the percentage of patients with CR, PR or stable disease (SD). Adverse events attributed to TACE or camrelizumab treatment were recorded and assessed by The Common Terminology Criteria for Adverse Events Version 5.0. In addition, postembolization syndrome, such as fever, pain, nausea and vomiting, is not considered an AE in itself, but rather an expected outcome of embolization therapy [27].
Statistical analyses
All analyses were performed by using SPSS software, Version 24.0 (IBM, Armonk, New York). Discrete variables were represented by numbers with percentages and were calculated by Chi-square test, and continuous variables were presented as mean ± standard deviation and were calculated by Student’s t-test. Kaplan–Meier method and log-rank test were performed to evaluate the differences in PFS and survival rates between the two groups. The 95% confidence interval (CI) was calculated for median PFS and hazard ratio (HR). Log-rank test was used for univariate analysis, in which variables with P value less than 0.10 in univariate analysis were added to multivariate analysis. P < 0.05 indicated a statistically significance.
Results
Study population and patient characteristics
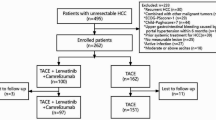
A total of 353 R-HCC patients underwent a treatment of either TACE- camrelizumab or TACE-alone in the study. 282 patients were excluded from the study and 71 patients were finally included in this analysis: 20 patients were treated with TACE-camrelizumab and 51 patients were treated with TACE-alone (Fig. 1). The baseline characteristics of the 71 patients were listed in Table 1. There was no significant difference in baseline characteristics between the two groups. The median follow-up period was 12 months (range, 4–55 months) in the TACE-alone group and 9 months (range, 5–15 months) in the TACE-camrelizumab group. In the TACE-alone group, 35 patients (68.6%) died at the end of follow-up, and in the TACE-camrelizumab group, 5 patients (25.0%) died.

Flow chart shows the screening procedure for recurrent HCC patients with treated with TACE-camrelizumab or TACE-alone. HCC = hepatocellular carcinoma, R-HCC = recurrent hepatocellular carcinoma, TACE = transarterial chemoembolization, TAI = transcatheter arterial infusion, RFA = radiofrequency ablation
Tumor response
The response of the tumor was determined by the abdominal contrast-enhanced CT or MR imaging. In the TACE–camrelizumab group, 1 patient (5%) achieved complete response, 7 patients (35%) achieved partial response, and 8 patients (40%) achieved stable disease. Therefore, the objective response rate and disease control rate were 40% and 80%, respectively. In the TACE–alone group, 18 patients (35.3%) achieved complete response, 11 patients (21.6%) achieved PR, and 14 patients (27.5%) achieved SD. Therefore, the objective response rate and disease control rate were 56.9% and 84.3%, respectively. The chi-square test indicated that there was no significant difference in objective response rate (P = 0.201) and disease control rate (P = 0.663) between the two groups.
Progression-free survival and survival rates
The median PFS was 6 months (95%CI: 3.5, 8.6 months) in the TACE- camrelizumab group, and 9 months (95%CI: 3.0, 15.0 months) in the TACE-alone groups. No statistically significant difference was found between the two groups in the median PFS (P = 0.586) (Fig. 2A). In the patients at the stage of BCLC-C, the median PFS was 6 months (95%CI: 2.6, 9.4 months) in the TACE- camrelizumab group, and 8 months (95%CI: 4.6, 11.4 months) in the TACE- alone group with no significant difference (P = 0.862) (Fig. 2B). Univariate analysis indicated that BCLC stage, tumor number and Neutrophil-to-lymphocyte ratio (NLR) were associated with PFS (Table 2). Among these factors, multivariate analysis indicated that NLR was a prognostic factor for PFS (Table 3). The half-year survival rate was 95.0% in the TACE–camrelizumab group, and 86.3% in the TACE–alone group with no significant difference (P = 0.304). The one-year survival rate was estimated at 60.7% and 49.0% in the TACE–camrelizumab group and TACE–alone group, respectively (P = 0.430). In the patients at the stage of BCLC-C, the half-year survival rate was 94.4% in the TACE-camrelizumab group, and 83.8% in the TACE-alone group with no significant difference (P = 0.264). The one-year survival rate was 65.0% in the TACE- camrelizumab group, and 40.5% in the TACE–alone group with no significant difference (P = 0.177).

A Kaplan–Meier curves of cumulative PFS in recurrent HCC patients treated with TACE-camrelizumab or TACE-alone. HCC = hepatocellular carcinoma, PFS = progression-free survival. B Kaplan–Meier curves of cumulative PFS in recurrent HCC patients treated with TACE-camrelizumab or TACE-alone at the stage of BCLC-C. HCC = hepatocellular carcinoma, PFS = progression-free survival. BCLC = Barcelona Clinic Liver Cancer
Adverse events
In the TACE-camrelizumab group, 9 patients (45%) developed fever (n = 7), abdominal pain (n = 4), nausea and vomiting (n = 4) within one week after TACE, and in the TACE-alone group, 16 patients (31.4%) developed fever (n = 11), abdominal pain (n = 8), nausea and vomiting (n = 6) within one week after TACE. After symptomatic treatment during hospitalization, the symptoms of all patients were alleviated or eliminated.
AEs related to camrelizumab are shown in Table 4. During the follow-up period, 15 (75%) patients developed at least one type of AEs after treatment with camrelizumab, and no patients developed severe AEs (more than grade 3). In addition, 1 patient (5%) developed pneumonitis, and the symptom was improved by glucocorticoids and interruption of camrelizumab. No treatment-related deaths occurred in this study.
Discussion
Because of the high risk of tumor recurrence after liver resection, it is urgent to find an effective treatment for the recurrence that can be used repeatedly and is suitable for patients with limited reserve of liver function. TACE is usually used in this kind of patients, but TACE alone cannot replace repeated liver resection. However, TACE increases tumor-specific CD8 + T cell response and programmed death receptor 1 (PD-1) and programmed death ligand 1 (PD-L1) expression, which provides an impetus for the exploration of immunotherapy after TACE [28]. In this study, we found that the efficacy of TACE-camrelizumab and TACE-alone is similar for R-HCC patients, with no significant statistical differences in PFS, objective response rate and disease control rate between the two groups. Previous study reported that NLR was useful prognostic factors in predicting outcomes in patients with HCC who underwent live resection, and multivariate analysis in our study found similar result, which suggested that inflammation played an important role in R-HCC [29, 30].
The median PFS in patients treated with TACE alone was 9 months (95%CI: 3.0, 15.0 months), longer than 6 months reported for TACE-camrelizumab. According to the previous research and our hypothesis, the addition of ICIs was helpful for patients who underwent TACE treatment in patients with primary HCC [23], but our study reports negative results both in PFS and survival rates. Similar negative results were reported in the study that evaluated the efficacy of TACE plus sorafenib [31], and one possible reason for this is the timing of sorafenib administration. More than half of the patients underwent sorafenib treatment 9 weeks after TACE, and yet the production of VEGF by triggering ischemic conditions might just exist for a short time [32], which reminded us that the condition of high expression of PD-1 and the increasing tumor-specific CD8 + T cell response in the tumor microenvironment might disappear soon. Another study comparing TACE plus sorafenib with TACE achieved positive results at median PFS (25.2 vs 13.5 months, P = 0.006). Besides the new criteria for progression, another possible factor of the positive results was that sorafenib was given 2–3 weeks before initial TACE was performed [33]. In this retrospective study, patients were treated with camrelizumab within 2–3 weeks after TACE procedure. It is possible that shrinking the interval between TACE and camrelizumab or giving the camrelizumab prior to TACE procedure after evaluating the condition of patients carefully can bring more survival benefits.
Some studies demonstrated the efficacy of transarterial embolization combined with ICIs in the treatment of primary HCC [20, 34]. However, recently, a study indicated that different immune therapy strategies should be considered for the treatment of primary HCC and recurrent HCC due to the significant differences in tumor microenvironments between the two groups [35]. According to the report, CD8 + T cells in recurrent tumors overexpressed KLRB1 (CD161) and displayed an innate-like low cytotoxic state, with low clonal expansion, unlike the classical exhausted state observed in primary HCC. Meanwhile, by compromising antigen presentation in DC cells and recruiting innate-like CD161 + CD8 + T cells, recurrent malignant cells could enhance immune evasion capacities and reduced cellular proliferation. As a result, the efficacy of ICIs was reduced in patients with R-HCC and normal in patients with primary HCC.
In the TACE-camrelizumab group, 70% of patients developed at least one type of AEs after treatment with camrelizumab, and all of the AEs were grade 1 or 2. These AEs were significantly improved after symptomatic treatment. Similar to the previous study, reactive cutaneous capillary endothelial proliferation (RCCEP) is the most common adverse event related to the camrelizumab, but RCCEPs were clinically controllable and self-limiting [24]. Overall, the treatment method of TACE–camrelizumab for R-HCC patients was safe and tolerable.
Our study had limitations. First, our study was retrospective, and the sample size in the two treatment groups was relatively small, therefore, it was difficult to make strong conclusions about these results. Second, our study was conducted in a single center. Finally, due to the relatively short period of follow-up time, this study did not achieve median OS. Therefore, it is necessary that prospective multicenter clinical trials be conducted in the future to validate our findings.
Conclusion
In summary, this study is the first one to report the efficacy and safety of the TACE combined with camrelizumab in the treatment of R-HCC patients, and the results indicated that this combination therapy had a similar effect on R-HCC patients compared with TACE-alone, which reminded us that TACE was still a better choice for patients with R-HCC. At the same time, the treatment of TACE combined with camrelizumab had an acceptable safety profile, with no occurrence of severe AEs. Although this study did not demonstrate the superiority of TACE-camrelizumab over TACE-Alone, the results can definitely serve as an important reference for other research.
Availability of data and materials
The data analysed during this study are avaliable from the electrical medical database of Union Hospital, Tongji Medical college, Huazhong University of Science and Technology. Please contact the author Chuansheng Zheng (hqzcsxh@sina.com) upon reasonable requests.
Abbreviations
- AFP:
-
Alpha-fetoprotein
- BCLC:
-
Barcelona Clinic Liver Cancer
- CR:
-
Complete response
- CT:
-
Computed tomography
- EASL:
-
European Association for the Study of the Liver
- R-HCC:
-
Recurrent hepatocellular carcinoma
- MR:
-
Magnetic resonance
- RECIST:
-
Response Evaluation Criteria in Solid Tumors
- OS:
-
Overall survival
- PD:
-
Progressive disease
- PFS:
-
Progressionfree survival
- PR:
-
Partial response
- SD:
-
Stable disease
- TACE:
-
Transarterial chemoembolization
- RCCEP:
-
Reactive cutaneous capillary endothelial proliferation
- AEs:
-
Adverse events
References
EASL Clinical Practice Guidelines. Management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236.
Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology (Baltimore, MD). 2003;37(2):429–42.
Maluccio M, Covey A. Recent progress in understanding, diagnosing, and treating hepatocellular carcinoma. CA cancer j clin. 2012;62(6):394–9.
Jeon MY, Kim HS, Lim TS, Han DH, Kim BK, Park JY, et al. Refractoriness to transarterial chemoembolization in patients with recurrent hepatocellular carcinoma after curative resection. PloS one. 2019;14(4):e0214613.
Koh PS, Chan AC, Cheung TT, Chok KS, Dai WC, Poon RT, et al. Efficacy of radiofrequency ablation compared with transarterial chemoembolization for the treatment of recurrent hepatocellular carcinoma: a comparative survival analysis. HPB (Oxford). 2016;18(1):72–8.
Liu Y, Ren Y, Ge S, Xiong B, Zhou G, Feng G, et al. Transarterial Chemoembolization in Treatment-Naïve and Recurrent Hepatocellular Carcinoma: A Propensity-Matched Outcome and Risk Signature Analysis. Frontiers in oncology. 2021;11:662408.
Shim JH, Kim KM, Lee YJ, Ko GY, Yoon HK, Sung KB, et al. Complete necrosis after transarterial chemoembolization could predict prolonged survival in patients with recurrent intrahepatic hepatocellular carcinoma after curative resection. Ann Surg Oncol. 2010;17(3):869–77.
Kim DS, Lim TS, Jeon MY, Kim BK, Park JY, Kim DY, et al. Transarterial Chemoembolization in Treatment-Naïve and Recurrent Hepatocellular Carcinoma: A Propensity-Matched Outcome Analysis. Dig Dis Sci. 2019;64(12):3660–8.
Tung-Ping Poon R, Fan ST, Wong J. Risk factors, prevention, and management of postoperative recurrence after resection of hepatocellular carcinoma. Ann Surg. 2000;232(1):10–24.
Poon RT, Fan ST, Lo CM, Liu CL, Wong J. Intrahepatic recurrence after curative resection of hepatocellular carcinoma: long-term results of treatment and prognostic factors. Ann Surg. 1999;229(2):216–22.
Midorikawa Y, Takayama T, Moriguchi M, Yagi R, Yamagishi S, Nakayama H, et al. Liver Resection Versus Embolization for Recurrent Hepatocellular Carcinoma. World J Surg. 2020;44(1):232–40.
Kim HS, Yi NJ, Kim JM, Joh JW, Lee KW, Suh KS. Clinical impact of the treatment modality on small, solitary, recurrent intrahepatic hepatocellular carcinomas after primary liver resection. Annals of surgical treatment and research. 2021;101(2):85–92.
Zhu XD, Sun HC. Emerging agents and regimens for hepatocellular carcinoma. J Hematol Oncol. 2019;12(1):110.
El-Khoueiry AB, Sangro B, Yau T, Crocenzi TS, Kudo M, Hsu C, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet (London, England). 2017;389(10088):2492–502.
Kudo M, Lim HY, Cheng AL, Chao Y, Yau T, Ogasawara S, et al. Pembrolizumab as Second-Line Therapy for Advanced Hepatocellular Carcinoma: A Subgroup Analysis of Asian Patients in the Phase 3 KEYNOTE-240 Trial. Liver cancer. 2021;10(3):275–84.
Q in SK, Ren ZG, Meng ZQ, Chen ZD, Chai XL, Xiong JP, et al. LBA27A randomized multicentered phase II study to evaluate SHR-1210 (PD-1 antibody) in subjects with advanced hepatocellular carcinoma (HCC) who failed or intolerable to prior systemic treatment. 2018;29(suppl_8):viii719–viii720.
Nakamura A, Kondo N, Nakamichi T, Kuroda A, Hashimoto M, Matsumoto S, et al. Initial evaluation of nivolumab in patients with post-operative recurrence of malignant pleural mesothelioma. Jpn J Clin Oncol. 2020;50(8):920–5.
Finn RS, Ryoo BY, Merle P, Kudo M, Bouattour M, Lim HY, et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2020;38(3):193–202.
Yau T, Park JW, Finn RS, Cheng AL, Mathurin P, Edeline J, et al. LBA38_PR - CheckMate 459: A randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann Oncol. 2019;30:v874–5.
Zhan C, Ruohoniemi D, Shanbhogue KP, Wei J, Welling TH, Gu P, et al. Safety of Combined Yttrium-90 Radioembolization and Immune Checkpoint Inhibitor Immunotherapy for Hepatocellular Carcinoma. Journal of vascular and interventional radiology : JVIR. 2020;31(1):25–34.
Flecken T, Schmidt N, Hild S, Gostick E, Drognitz O, Zeiser R, et al. Immunodominance and functional alterations of tumor-associated antigen-specific CD8+ T-cell responses in hepatocellular carcinoma. Hepatology (Baltimore, MD). 2014;59(4):1415–26.
Montasser A, Beaufrère A, Cauchy F, Bouattour M, Soubrane O, Albuquerque M, et al. Transarterial chemoembolisation enhances programmed death-1 and programmed death-ligand 1 expression in hepatocellular carcinoma. Histopathology. 2021;79(1):36–46.
Chao J, Zhu Q, Chen D, An X, Liu A, Zhou F, et al. Case Report: Transarterial Chemoembolization in Combination With Tislelizumab Downstages Unresectable Hepatocellular Carcinoma Followed by Radical Salvage Resection. Frontiers in oncology. 2021;11:667555.
Qin S, Ren Z, Meng Z, Chen Z, Chai X, Xiong J, et al. Camrelizumab in patients with previously treated advanced hepatocellular carcinoma: a multicentre, open-label, parallel-group, randomised, phase 2 trial. Lancet Oncol. 2020;21(4):571–80.
Markham A, Keam SJ. Camrelizumab: First Global Approval. Drugs. 2019;79(12):1355–61.
Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60.
Gaba RC, Lokken RP, Hickey RM, Lipnik AJ, Lewandowski RJ, Salem R, et al. Quality Improvement Guidelines for Transarterial Chemoembolization and Embolization of Hepatic Malignancy. Journal of vascular and interventional radiology : JVIR. 2017;28(9):1210-23.e3.
Hur S, Shin JH, Lee IJ, et al. Early Experience in the Management of Postoperative Lymphatic Leakage Using Lipiodol Lymphangiography and Adjunctive Glue Embolization. J Vasc Interv Radiol. 2016;27:1177–86 Journal of vascular and interventional radiology JVIR 2016 27(10) 1627.
Zhang LX, Wei ZJ, Xu AM, Zang JH. Can the neutrophil-lymphocyte ratio and platelet-lymphocyte ratio be beneficial in predicting lymph node metastasis and promising prognostic markers of gastric cancer patients? Tumor maker retrospective study. International journal of surgery (London, England). 2018;56:320–7.
Wang D, Bai N, Hu X, OuYang XW, Yao L, Tao Y, et al. Preoperative inflammatory markers of NLR and PLR as indicators of poor prognosis in resectable HCC. PeerJ. 2019;7:e7132.
Kudo M, Imanaka K, Chida N, Nakachi K, Tak WY, Takayama T, et al. Phase III study of sorafenib after transarterial chemoembolisation in Japanese and Korean patients with unresectable hepatocellular carcinoma. Eur j cancer. 2011;47(14):2117–27.
Kudo M, Arizumi T. Transarterial Chemoembolization in Combination with a Molecular Targeted Agent: Lessons Learned from Negative Trials (Post-TACE, BRISK-TA, SPACE, ORIENTAL, and TACE-2). Oncology. 2017;93(Suppl 1):127–34.
Kudo M, Ueshima K, Ikeda M, Torimura T, Tanabe N, Aikata H, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–501.
Marinelli B, Cedillo M, Pasik SD, Charles D, Murthy S, Patel RS, et al. Safety and Efficacy of Locoregional Treatment during Immunotherapy with Nivolumab for Hepatocellular Carcinoma: A Retrospective Study of 41 Interventions in 29 Patients. Journal of vascular and interventional radiology : JVIR. 2020;31(11):1729-38.e1.
Sun Y, Wu L, Zhong Y, Zhou K, Hou Y, Wang Z, et al. Single-cell landscape of the ecosystem in early-relapse hepatocellular carcinoma. Cell. 2021;184(2):404-21.e16.
Acknowledgements
We thank to all the medical workers in our department for their assistance with the study.
Funding
This work was supported by grant from National Nature Science Foundation of China (No. 81601580 and No.81873919), Fundamental Research Funds for the Central Universities (2021yjsCXCY101).
Author information
Authors and Affiliations
Contributions
Y.s. G., Y.q. R., L. C. and T.S. collected the patients’ data, Y.s. G. drafted the manuscript. W.h. Z. revised the manuscript. Y.q. R., B. S. and L.c. Z. analyzed and interpreted the data. F.X. and C.s.Z. made substantial contributions to the conception and design of the work. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by institutional review board of the Union Hospital, Tongji Medical college, Huazhong University of Science and Technology (UHCT-IEC-SOP-016–03-01) and has been conducted in accordance with the ethical standards, according to the Declaration of Helsinki, and according to national and international guidelines. Written informed consent was obtained from all patients prior to treatment and from legal guardians of dead patients.
Consent for publication
Not applicable.
Competing interests
The author reports no conflicts of interest in this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guo, Y., Ren, Y., Chen, L. et al. Transarterial chemoembolization combined with camrelizumab for recurrent hepatocellular carcinoma. BMC Cancer 22, 270 (2022). https://doi.org/10.1186/s12885-022-09325-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-09325-6