
Abstract
Background
In contrast to the well-described epidemiology and behavior of small cell lung carcinoma (SCLC), little is known about extrapulmonary small cell carcinoma (EPSCC).
Methods
Using data from the Surveillance, Epidemiology and End Results (SEER) Program (1992–2010), we calculated age-adjusted incidence rates (IRs), IR ratios (IRRs), annual percent change (APC), relative survival (RS), RS ratios (RSRs), and the respective 95% confidence intervals (95% CI) of SCLC and EPSCC according to primary site. We used the SEER historic stage variable that includes localized (confined to the organ of origin), regional (direct extension to adjacent organ/tissue or regional lymph nodes), and distant (discontinuous metastases) stages and combined localized and regional stages into “limited” stage.
Results
The incidence of SCLC (IR = 76.3/million person-years; n = 51,959) was 22-times that of EPSCC (IR = 3.5; n = 2,438). Of the EPSCC sites, urinary bladder, prostate, and uterine cervix had the highest incidence (IRs = 0.7-0.8); urinary bladder (IRR = 4.91) and stomach (IRR = 3.46) had the greatest male/female disparities. Distant-to-limited stage site-specific IRRs of EPSCC were significantly elevated for pancreas (IRR = 6.87; P < 0.05), stomach, colon/rectum, ovary, and prostate (IRRs = 1.62-2.42; P < 0.05) and significantly decreased for salivary glands, female breast, uterine cervix, and urinary bladder (IRRs = 0.32-0.46). During 1992–2010, significant changes in IRs were observed for EPSCC overall (APC = 1.58), small cell carcinoma of the urinary bladder (APC = 6.75), SCLC (APC = −2.74) and small cell carcinoma of unknown primary site (APC = −4.34). Three-year RS was significantly more favorable for patients with EPSCC than SCLC for both limited (RSR = 2.06; 95% CI 1.88, 2.26) and distant stages (RSR = 1.55; 95% CI 1.16, 2.07). Among limited stage small cell carcinoma, RS was most favorable for salivary glands, female breast, and uterine cervix (RS = 52-68%), whereas RS for nearly all sites with distant stage disease was <10%.
Conclusion
EPSCC comprises a heterogeneous group of diseases that appears, at least in part, etiologically distinct from SCLC and is associated with more favorable stage-specific patient survival.
Similar content being viewed by others


Background
In the broad spectrum of neuroendocrine tumors, small cell carcinomas comprise the less differentiated tumors associated with aggressive behavior [1]. Most of what is known regarding the epidemiology of small cell carcinoma is derived from studies of lung cancer. Indeed, of the major lung cancer types, cigarette smoking has been most strongly associated with small cell lung carcinoma (SCLC) [2,3]. Risk factors for extrapulmonary small cell carcinoma (EPSCC) are unknown. While population-based epidemiologic studies of neuroendocrine tumors have considered incidence according to anatomic site, most have excluded small cell histology, based on the assumption that these aggressive, highly fatal tumors are etiologically distinct from their well-differentiated counterparts [4-7]. Few studies of EPSCC have assessed incidence and patient survival by site [8,9], and although some studies have focused on selected sites [10-12], to our knowledge, none have been comprehensive in their inclusion of topography while describing site-specific incidence rates and patient survival. To gain insight into the etiology and behavior of small cell carcinoma, we comprehensively assessed SCLC and EPSCC incidence and patient survival using population-based data from the National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) Program.
Methods
We assessed incidence of small cell carcinoma based on cases diagnosed among residents of 13 cancer registry areas of the SEER (SEER-13) Program during 1992–2010. SEER-13 represents approximately 14% of the population of the U.S. and includes the states of Connecticut, Hawaii, Iowa, New Mexico, and Utah and the areas of Detroit, Michigan; San Francisco, Los Angeles, and San Jose-Monterey, California; Seattle-Puget Sound, Washington; Atlanta and rural Georgia; and the Alaska Native Tumor Registry. The SEER Program classifies histology and topography information according to the International Classification of Diseases for Oncology (ICD-O), and all cases have been recoded to the third edition of ICD-O (ICD-O-3) by the SEER Program [13].
Using SEER*Stat, version 8.1.2 (www.seer.cancer.gov), we calculated incidence rates (IRs), IR ratios (IRRs), and corresponding 95% confidence intervals (CIs) for all cases of microscopically confirmed small cell carcinoma (ICD-O-3 morphology codes 8041–8045) with malignant behavior (ICD-O-3 behavior code/3) according to primary site (topography codes specified in Table 1). Overall, 834 cases (1.5% of total) were not microscopically confirmed and were excluded from the study. Malignant tumor, small cell type (8002) was excluded due to being a nonspecific code and potentially including other malignancies characterized by small cells (e.g., malignant melanoma, lymphoma) [14]. All IRs were age-adjusted to the 2000 U.S. standard population and expressed per one million person-years (PY). IRs were assessed according to gender, age, calendar year, and stage. To allow a general overview of stage across primary sites, we used the SEER historic stage variable that includes localized (confined to the organ of origin), regional (direct extension to adjacent organ/tissue or regional lymph nodes), distant (discontinuous metastases), and unspecified stages. We combined localized and regional stages into the category of “limited” stage and maintained the distant stage variable as defined in SEER. Our “limited” and “distant” stage categories are intended to approximate the two-tier SCLC staging systems of the Veterans Administration Lung Study Group and the International Association for the Study of Lung Cancer [15].
Age-specific IRs (<15, 15–24, 25–34, 35–44, 45–54, 55–64, 65–74, 75+ years) were calculated and depicted on a log-linear scale as previously described [16]. Annual percent change (APC) in incidence was calculated using the weighted least squares method. We used the Joinpoint Regression Program (version 4.1.1.3) to assess the best fit for trend data and allowed up to 3 Joinpoints (http://surveillance.cancer.gov/joinpoint). Following the SEER Program convention, IRs are not presented for fewer than 16 cases [17].
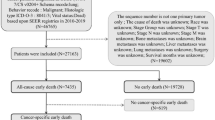
Relative survival (RS) for cases diagnosed during 1992–2010 and followed through 2011 was estimated using the actuarial method in the SEER*Stat Survival Session. RS is the ratio of the proportion of observed survivors in a cohort of patients to the proportion of expected survivors in a comparable cohort of the general population [18]. We estimated 3-year RS, RS ratios (RSRs), and 95% CIs overall, according to site, stage, gender, age, primary tumor size, and calendar year. To allow comparison with previously published studies describing 5-year survival, we calculated 5-year RS for SCLC and EPSCC (Additional file 1: Table S1 and Additional file 2: Table S2). We excluded individuals with second or later primary cancers (n = 9,848), cases diagnosed by death certificate or autopsy (n = 134), those with unknown age (n = 4), and those alive with unknown survival time (n = 6). In total, 45,747 cases were available for the survival analysis. Following SEER convention, RS rates based on fewer than 25 cases are not presented [17].
Results
Overall, 55,722 cases of small cell carcinoma were diagnosed among residents of SEER-13 during 1992–2010 (IR = 81.8/million PY). The incidence of SCLC (n = 51,959; IR = 76.3) was 22 times that of EPSCC (n = 2,438; IR = 3.5), accounting for 93% of cases of small cell carcinoma. Of the extrapulmonary sites, IRs were highest for urinary bladder, prostate, and uterine cervix (Table 1). Small cell carcinoma IR was 35% higher among men than women, with the greatest gender disparities noted for urinary bladder and stomach (male-to-female (M/F) IRR = 4.91 and 3.46, respectively).
IRs of SCLC and EPSCC increased exponentially with advancing age among men and women, most rapidly for SCLC among both men and women and least rapidly for EPSCC among women (Figure 1). Significant gender differences in SCLC IRs were apparent beginning at ages 45–54 years (M/F IRR = 1.14; 95% CI 1.07, 1.20), peaking at the oldest age group (≥75 years; M/F IRR = 1.60; 95% CI 1.55, 1.65). In contrast, the M/F IRRs for EPSCC rose from a female excess through ages 45–54 years (M/F IRR = 0.77; 95% CI 0.60, 0.97) to a male excess starting at ages 55–64 years (M/F IRR = 1.38; 95% CI 1.14, 1.67) and increasing progressively until ≥75 years (IRR = 2.47; 95% CI 2.14, 2.85). Among EPSCC diagnosed prior to age 55 years, uterine cervix (n = 156) and ovary (n = 75) comprised 61% of 379 cases among women, whereas the urinary bladder (n = 37) and colon/rectum (n = 33) accounted for the largest proportion (39%) of the 179 cases among men.

Age-specific incidence rates of small cell lung carcinoma and extrapulmonary small cell carcinoma diagnosed in 13 cancer registry areas of the Surveillance, Epidemiology and End Results Program during 1992–2010 according to gender.
In contrast to SCLC where incidence of distant stage disease predominated over limited stage (distant/limited IRR = 2.32, 95% CI 2.28, 2.37), incidence of limited stage EPSCC was significantly higher than distant stage (distant/limited IRR = 0.89, 95% CI 0.82, 0.97) (Table 2). The distant/limited stage IRR was significantly elevated for small cell carcinoma of the stomach, colon/rectum, pancreas, ovary, and prostate, whereas IRRs were significantly decreased for salivary glands, female breast, uterine cervix, and urinary bladder.
Whereas the incidence of SCLC decreased during 1992–2010 (APC = −2.74; P < 0.05), the incidence of EPSCC increased significantly (APC = 1.58; P < 0.05), largely related to the marked rise in small cell carcinoma of the urinary bladder (APC = 6.75; P < 0.05) (Figure 2). Similar to SCLC, only the incidence of small cell carcinoma of unknown primary site decreased over this timeframe (APC = −4.34; P < 0.05). APC did not change significantly for any other site for which APC could be calculated. All trend data were best fitted with 0 joinpoints.

Annual percent change of small cell lung carcinoma and extrapulmonary small cell carcinoma diagnosed in 13 cancer registry areas of the Surveillance, Epidemiology and End Results Program during 1992–2010 according to site.
Among patients with limited stage disease, 3-year RS was significantly more favorable for patients with EPSCC than SCLC overall, among males and females <60 and ≥60 years, whites <60 years, whites and blacks ≥60 years, according to tumor size, and by calendar year period (Table 3). Among patients with distant stage small cell carcinoma, RS was poor but signifcantly better for EPSCC than for SCLC overall, among white males <60 years of age, for tumor size >7 cm, and for cases diagnosed 2001–2010. Compared to 1992–2000, survival during 2001–2010 increased significantly for limited (limited/distant RSR = 1.22, 95% CI 1.13, 1.31) and distant stage (limited/distant RSR = 1.26, 95% CI 1.09, 1.45) SCLC but not for limited (limited/distant RSR = 1.07, 95% CI 0.90, 1.27) or distant stage (limited/distant RSR = 1.22, 95% CI 0.68, 2.18) EPSCC. To allow comparison of RS by EPSCC sites, we used uterine cervix as the referent site, since there were sufficient cases to allow stable comparisons for both, limited and distant stage disease (Table 4). Compared to small cell carcinoma of the uterine cervix, 3-year RS was significantly less favorable for limited stage small cell carcinoma of the esophagus (RSR = 0.64, 95% CI 0.42, 0.98) and urinary bladder (RSR = 0.78, 95% CI 0.62, 0.99), whereas for distant stage disease, pancreas was associated with significantly less favorable survival (RSR = 0.19, 95% CI 0.04, 0.96).
Discussion
This is among the first population-based studies to describe distinct differences in incidence patterns between SCLC and EPSCC, suggesting etiologic differences, with the most convincing evidence arising from opposing temporal trends across sites. With the decrease in SCLC attributed to declining cigarette smoking, our findings raise the possibility that tobacco may have a less important role in the etiology of EPSCC overall, and also in small cell carcinoma of the bladder. Etiologic heterogeneity is also suggested by site-specific differences in incidence of EPSCC by gender, possibly reflecting varying environmental exposures and/or inherent susceptibility. Differences in stage at presentation of site-specific EPSCC may be due to distinct disease biology, since sites for which screening is available did not all present with less advanced disease (e.g., prostate), although diagnostic challenges could also affect stage at presentation. RS differences by site also suggest distinct biologic behavior and/or responsiveness to therapy.
Our findings differ from a 1970–2004 population-based study of 1,618 cases of EPSCC from South East England where EPSCC predominated among women (male:female case ratio of 1:1.3, comparable to a case ratio of 0.77) [9], in contrast to our case ratio of 1.09. In South East England, small cell carcinoma of the esophagus comprised the majority of EPSCC (18%), followed by stomach (6%) and prostate (6%). Among our 2,438 cases of EPSCC, the largest fractions were of the urinary bladder (22%), uterine cervix (11%), and colon/rectum (10%). While these findings may reflect differences in study design, calendar years of study, histologic entities included, or population characteristics, they also support potential differences in exposures or susceptibility between individuals in the U.S. and South East England. A literature review including more than 130 reports of gastrointestinal small cell carcinoma during 1970–2003 also identified esophagus as the most commonly reported primary site, accounting for 53% (n = 290/544 cases) of gastrointestinal small cell carcinomas [19]. While tobacco and alcohol use were found to be prevalent among patients in these series, an association with these or other putative risk factors has not been identified [19,20]. The differences in frequency of site-specific EPSCC across studies may reflect various factors, including time periods of study, accuracy of cancer reporting to cancer registries, varying extent of screening, distinct exposures among populations, diverse population characteristics (e.g., race/ethnicity), access to health care, and publication bias.
Among EPSCC, we report the highest incidence for the urinary bladder, a site that may clinically manifest early with hematuria or urinary symptoms, as supported by the more than triple number of cases diagnosed with limited stage than distant stage disease. The IRs were next highest for prostate and uterine cervix, both sites for which some form of cancer screening was available during the entire study period. For EPSCC of the cervix and female breast, there were more than twice as many cases with limited than distant stage, as would be expected in screen-detected cancers. However, there were 62% more distant than limited stage cases for the prostate, confirming findings in a prior SEER-based study (1973–2003) [21]. In combination, these findings raise the possibility that small cell carcinoma of the prostate may be associated with more aggressive biology than other sites for which screening is similarly available. However, alternate explanations, including a delay in diagnosis due to urinary symptoms being attributed to other causes, a missed finding of co-existing small cell carcinoma with adenocarcinoma of the prostate, or absence of elevation in prostate-specific antigen [22] could also account for the predominance of distant stage disease.
Incidence rates for SCLC and nearly all evaluable site-specific EPSCC were higher among males than females. This gender disparity in incidence has been similarly described for many other cancers [23]. While we noted a female predominance of EPSCC prior to age 55 years, this was driven by sex-specific cancer sites (uterine cervix, ovary). An early-onset incidence pattern has been described for cervical [24] and ovarian cancers [25], and whether human papillomavirus and hormonal factors, respectively, are risk factors for small cell carcinoma of these sites remains to be determined.
Lung cancer incidence rates among males and females have correlated with prior prevalence of tobacco use, in particular for SCLC and squamous cell carcinoma [26-28], thereby supporting the hypothesis that small cell carcinomas may share risk factors with non-small cell carcinomas occurring at the same site. Our study extends previous SEER-based reports [26,29], and we describe a continued decline in incidence of SCLC through 2010. In contrast to the significant decline in incidence during 1992–2010 observed for SCLC, a smoking-related cancer, the overall incidence of EPSCC increased. A rise in incidence was most notable for small cell carcinoma of the urinary bladder, despite cigarette smoking being an established risk factor for both lung and urinary bladder cancers. The increase in small cell carcinoma of the urinary bladder suggests a role for risk factor(s) other than tobacco, including occupational exposures. This finding is further supported by the decrease in incidence of papillary, squamous, and adenocarcinomas of the bladder since the early 1990s in the U.S., in contrast to the rise in small cell carcinoma previously described [30]. Therefore, the opposing trends of bladder cancer by histologic subtype makes early detection an unlikely explanation for the rising incidence of small cell carcinoma of the urinary bladder, as a similar direction in trend would be expected across histologic subtypes.
Consistent with some [8,9], but not all [31] prior reports, we found that RS was significantly more favorable for EPSCC than SCLC. In the U.S. and England, small cell carcinoma of female breast is associated with among the most favorable survival [8,9]. We also found survival for limited stage small cell carcinoma of salivary gland to be favorable, although based on few cases. Younger age and smaller tumor size were also associated with more favorable survival among limited stage SCLC and EPSCC. These findings are in agreement with a SEER-based study of EPSCC (1973–2006) where age ≥50 years, tumor size ≥5 cm, regional stage, and distant stage were identified as predictors of survival in multivariate analysis [8]. While several population-based studies [8,9,32] and single institution studies [31,33-41] have evaluated survival of EPSCC, comparison between studies is difficult due to varying measures of survival calculated, in addition to the extent to which staging and treatment information is considered; access to medical care is available; and distinct characteristics (e.g., race/ethnicity, socioeconomic status) are reflected in study populations. Additionally, with site-specific variation in survival of EPSCC, the entities included within the category of EPSCC across studies are likely to influence overall survival estimates.
A modest improvement in survival of SCLC has been reported since the 1970s and 1980s [42,43], and we observed a slight, but statistically significant, improvement in limited and extensive stage SCLC RS and a nonsignificant improvement in EPSCC RS subsequent to the 1990s. Despite statistical associations, clinically, the minimal change in survival over time likely reflects the lack of new therapies available for SCLC, with platinum agents remaining the mainstay of therapy since the 1980s [43]. Although the optimal treatment for EPSCC is unknown, it is often managed like SCLC [31], and while identification of new agents in the future may affect survival of both SCLC and EPSCC, variable response by site of disease might be expected based on historically reported differences in site-specific survival.
The strength of our population-based study includes the large size which allowed evaluation of incidence and patient survival by site. Despite its large size, we did not have sufficient cases of EPSCC to assess age-specific IRs, temporal trends, or RS for every specified site. Pathology was not centrally reviewed, so we cannot exclude the possibility of misclassification of other histologic entities characterized by small cells [14], including well differentiated neuroendocrine tumors. Our survival analyses did not include information on prognostic indicators such as performance status, lactate dehydrogenase, or weight loss because this information is not collected by the SEER Program. Additionally, we did not consider treatment or response to treatment in our survival analyses because treatment data (surgery, radiation) are limited to the first course of therapy, and information on chemotherapy, the mainstay of treatment for small cell carcinoma, is not publicly available. Lastly, our staging dichotomy (limited vs. distant stage) may have resulted in misclassification by stage, thereby yielding conservative RS estimates for limited stage disease and optimistic RS estimates for distant stage disease.
Conclusions
In summary, distinct incidence patterns suggest that there are etiologic differences between SCLC and EPSCC. Opposing temporal trends for SCLC and EPSCC since the 1990s support a less important role for cigarette smoking in EPSCC overall than in SCLC. Gender disparities in incidence of site-specific EPSCC further implicate distinct exposures and/or inherent susceptibility differences by site. Disease biology of EPSCC also appears to differ by primary site, as demonstrated by some screen-detectable cancer sites presenting predominantly with limited stage disease (e.g., uterine cervix, female breast) in contrast to other sites where distant stage disease predominated (e.g., prostate). Lastly, while a survival advantage was evident for limited stage EPSCC compared to SCLC, the advantage was less pronounced for distant stage small cell carcinoma which was associated with dismal survival across nearly all sites. The generally poor survival associated with small cell carcinoma underscores the importance of understanding disease etiology, identifying prevention/screening modalities, considering new treatment approaches, and ensuring that older patients and racially/ethnically diverse populations are included in clinical trials of new agents.
Abbreviations
- APC:
-
Annual percent change
- CI:
-
Confidence interval
- EPSCC:
-
Extrapulmonary small cell carcinoma
- ICD-O:
-
International Classification of Diseases for Oncology
- ICD-O-3:
-
Third edition of ICD-O
- IR:
-
Incidence rate
- IRR:
-
Incidence rate ratio
- M/F:
-
Male-to-female
- PY:
-
Person-years
- RS:
-
Relative survival
- RSR:
-
Relative survival ratio
- SCLC:
-
Small cell lung carcinoma
- SEER:
-
Surveillance, Epidemiology and End Results
- SEER-13:
-
13 cancer registry areas of the SEER Program
References
Bertino EM, Confer PD, Colonna JE, Ross P, Otterson GA. Pulmonary neuroendocrine/carcinoid tumors: a review article. Cancer. 2009;115(19):4434–41.
Kenfield SA, Wei EK, Stampfer MJ, Rosner BA, Colditz GA. Comparison of aspects of smoking among the four histological types of lung cancer. Tob Control. 2008;17(3):198–204.
Lubin JH, Blot WJ. Assessment of lung cancer risk factors by histologic category. J Natl Cancer Inst. 1984;73(2):383–9.
Crocetti E, Paci E. Malignant carcinoids in the USA, SEER 1992–1999. An epidemiological study with 6830 cases. Eur J Cancer Prev. 2003;12(3):191–4.
Hauso O, Gustafsson BI, Kidd M, Waldum HL, Drozdov I, Chan AK, et al. Neuroendocrine tumor epidemiology: contrasting Norway and North America. Cancer. 2008;113(10):2655–64.
Lawrence B, Gustafsson BI, Chan A, Svejda B, Kidd M, Modlin IM. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol Metab Clin N Am. 2011;40(1):1–18. vii.
Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008;26(18):3063–72.
Grossman RA, Pedroso FE, Byrne MM, Koniaris LG, Misra S. Does surgery or radiation therapy impact survival for patients with extrapulmonary small cell cancers? J Surg Oncol. 2011;104(6):604–12.
Wong YN, Jack RH, Mak V, Henrik M, Davies EA. The epidemiology and survival of extrapulmonary small cell carcinoma in South East England, 1970–2004. BMC Cancer. 2009;9:209.
Chen J, Macdonald OK, Gaffney DK. Incidence, mortality, and prognostic factors of small cell carcinoma of the cervix. Obstet Gynecol. 2008;111(6):1394–402.
Koay EJ, Teh BS, Paulino AC, Butler EB. A Surveillance, Epidemiology, and end results analysis of small cell carcinoma of the bladder: epidemiology, prognostic variables, and treatment trends. Cancer. 2011;117(23):5325–33.
van der Aa MA, Helmerhorst TJ, Siesling S, Riemersma S, Coebergh JW. Vaginal and (uncommon) cervical cancers in the Netherlands, 1989–2003. Int J Gynecol Cancer. 2010;20(4):638–45.
Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin L, Parkin DM, et al. International Classification of Diseases for Oncology, 3rd edn. Geneva (Switzerland): World Health Organization; 2000.
Quinn AM, Blackhall F, Wilson G, Danson S, Clamp A, Ashcroft L, et al. Extrapulmonary small cell carcinoma: a clinicopathological study with identification of potential diagnostic mimics. Histopathology. 2012;61(3):454–64.
Micke P, Faldum A, Metz T, Beeh KM, Bittinger F, Hengstler JG, et al. Staging small cell lung cancer: Veterans Administration lung study group versus International Association for the Study of Lung Cancer--what limits limited disease? Lung cancer (Amsterdam, Netherlands). 2002;37(3)):271–6.
Devesa SS, Donaldson J, Fears T. Graphical presentation of trends in rates. Am J Epidemiol. 1995;141(4):300–4.
Howlader N, Noone AM, Krapcho M, Garshell J, Neyman N, Altekruse SF, et al. SEER Cancer Statistics Review, 1975–2010. Bethesda: National Cancer Institute; 2013.
Ries LAG, Young Jr JL, Keel GE, Eisner MP, Lin YD, Horner M-J. SEER Survival Monograph: Cancer Survival Among Adults: U.S. SEER Program, 1988–2001, Patient and Tumor Characteristics. In: National Cancer Institute, SEER Program. 2007.
Brenner B, Tang LH, Klimstra DS, Kelsen DP. Small-cell carcinomas of the gastrointestinal tract: a review. J Clin Oncol. 2004;22(13):2730–9.
Casas F, Ferrer F, Farrus B, Casals J, Biete A. Primary small cell carcinoma of the esophagus: a review of the literature with emphasis on therapy and prognosis. Cancer. 1997;80(8):1366–72.
Deorah S, Rao MB, Raman R, Gaitonde K, Donovan JF. Survival of patients with small cell carcinoma of the prostate during 1973–2003: a population-based study. BJU Int. 2011;109(6):824–30.
Sella A, Konichezky M, Flex D, Sulkes A, Baniel J. Low PSA metastatic androgen- independent prostate cancer. Eur Urol. 2000;38(3):250–4.
Cook MB, Dawsey SM, Freedman ND, Inskip PD, Wichner SM, Quraishi SM, et al. Sex disparities in cancer incidence by period and age. Cancer Epidemiol Biomarkers Prev. 2009;18(4):1174–82.
Kurdgelashvili G, Dores GM, Srour SA, Chaturvedi A, Huycke MM, Devesa SS: Incidence of potentially HPV-related neoplasms in the United States, 1978–2007. Cancer 2013:In press.
Goodman MT, Shvetsov YB. Incidence of ovarian, peritoneal, and fallopian tube carcinomas in the United States, 1995–2004. Cancer Epidemiol Biomarkers Prev. 2009;18(1):132–9.
Travis WD, Lubin J, Ries L, Devesa S. United States lung carcinoma incidence trends: declining for most histologic types among males, increasing among females. Cancer. 1996;77(12):2464–70.
Jemal A, Travis WD, Tarone RE, Travis L, Devesa SS. Lung cancer rates convergence in young men and women in the United States: analysis by birth cohort and histologic type. Int J Cancer. 2003;105(1):101–7.
Devesa SS, Bray F, Vizcaino AP, Parkin DM. International lung cancer trends by histologic type: male:female differences diminishing and adenocarcinoma rates rising. Int J Cancer. 2005;117(2):294–9.
Riaz SP, Luchtenborg M, Coupland VH, Spicer J, Peake MD, Moller H. Trends in incidence of small cell lung cancer and all lung cancer. Lung cancer (Amsterdam, Netherlands). 2012;75(3):280–4.
Zhang Y, Zhu C, Curado MP, Zheng T, Boyle P. Changing patterns of bladder cancer in the USA: evidence of heterogeneous disease. BJU Int. 2011;109(1):52–6.
Terashima T, Morizane C, Hiraoka N, Tsuda H, Tamura T, Shimada Y, et al. Comparison of chemotherapeutic treatment outcomes of advanced extrapulmonary neuroendocrine carcinomas and advanced small-cell lung carcinoma. Neuroendocrinology. 2012;96(4):324–32.
Haider K, Shahid RK, Finch D, Sami A, Ahmad I, Yadav S, et al. Extrapulmonary small cell cancer: a Canadian province’s experience. Cancer. 2006;107(9):2262–9.
Brennan SM, Gregory DL, Stillie A, Herschtal A, Mac Manus M, Ball DL. Should extrapulmonary small cell cancer be managed like small cell lung cancer? Cancer. 2010;116(4):888–95.
Chalermchai T, Suwanrusme H, Chantranuwat P, Voravud N, Sriuranpong V. Retrospective review of extra-pulmonary small cell carcinoma at King Chulalongkorn memorial hospital cases during 1998–2005. Asia Pac J Clin Oncol. 2010;6(2):111–5.
Cicin I, Karagol H, Uzunoglu S, Uygun K, Usta U, Kocak Z, et al. Extrapulmonary small-cell carcinoma compared with small-cell lung carcinoma: a retrospective single-center study. Cancer. 2007;110(5):1068–76.
Fruh M, Kacsir B, Ess S, Cerny T, Rodriguez R, Plasswilm L. Extrapulmonary small cell carcinoma: An indication for prophylactic cranial irradiation? A single center experience. Strahlenther Onkol. 2011;187(9):561–7.
Galanis E, Frytak S, Lloyd RV. Extrapulmonary small cell carcinoma. Cancer. 1997;79(9):1729–36.
Kim KO, Lee HY, Chun SH, Shin SJ, Kim MK, Lee KH, et al. Clinical overview of extrapulmonary small cell carcinoma. J Korean Med Sci. 2006;21(5):833–7.
Lee SS, Lee JL, Ryu MH, Chang HM, Kim TW, Kim WK, et al. Extrapulmonary small cell carcinoma: single center experience with 61 patients. Acta oncologica (Stockholm, Sweden). 2007;46(6):846–51.
Ochsenreither S, Marnitz-Schultze S, Schneider A, Koehler C, Daum S, Loddenkemper C, et al. Extrapulmonary small cell carcinoma (EPSCC): 10 years’ multi-disciplinary experience at Charite. Anticancer Res. 2009;29(8):3411–5.
Soto DE, Eisbruch A. Limited-stage extrapulmonary small cell carcinoma: outcomes after modern chemotherapy and radiotherapy. Cancer journal (Sudbury, Mass. 2007;13(4):243–6.
Govindan R, Page N, Morgensztern D, Read W, Tierney R, Vlahiotis A, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24(28):4539–44.
van Meerbeeck JP, Fennell DA, De Ruysscher DK. Small-cell lung cancer. Lancet. 2011;378(9804):1741–55.
Acknowledgements
The authors would like to thank David P. Check of the Division of Cancer Epidemiology and Genetics, National Cancer Institute for his expert assistance with the figures and the reviewers of our manuscript for their insightful suggestions. This work was supported by the Oklahoma City Veterans Affairs Health Care System, Oklahoma City, OK and the Intramural Research Program of the National Cancer Institute, National Institutes of Health, Department of Health and Human Services, Bethesda, MD. The Department of Veterans Affairs and the Intramural Research Program of the National Cancer Institute had no role in the design, data analysis, interpretation of data, manuscript writing, or submission process of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors have no competing interests to declare.
Authors’ contributions
All authors participated in the conception and design of the study and data interpretation. GMD performed the analysis and drafted the manuscript. All authors critically reviewed the manuscript for important intellectual content, and approved the final manuscript.
Additional files
Additional file 1: Table S1.
Stage-specific five-year relative survival of patients with small cell lung carcinoma and extrapulmonary small cell carcinoma diagnosed in SEER-13 according to gender, age, calendar year, and site, 1992-2010*.
Additional file 2: Table S2.
Stage-specific five-year relative survival of patients with extrapulmonary small cell carcinoma diagnosed in SEER-13 according to site, 1992-2010*.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Dores, G.M., Qubaiah, O., Mody, A. et al. A population-based study of incidence and patient survival of small cell carcinoma in the United States, 1992–2010. BMC Cancer 15, 185 (2015). https://doi.org/10.1186/s12885-015-1188-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-015-1188-y