
Abstract
Background
Uterine afterpains are among the most prevalent complaints after natural vaginal delivery. Non-pharmacological treatment modalities to relieve afterpains are an important care priority. This study was conducted to investigate the effect of foot reflexology in the fourth stage of labor on afterpains in multiparous women.
Methods
This single-blind, randomized, clinical trial recruited 80 eligible pregnant women presenting to Allameh Bohlool Hospital in Gonabad and 17-Shahrivar Hospital in Mashhad, Iran, in 2019. In the first and second hours postpartum, the reflexology group received 10 min of general massage and specific reflexology massage on each foot on the uterine, pituitary, and solar plexus points. The control group received 10 min of general massage, and then rotational massage on a neutral point on the lateral side of the heel. The pain was measured every hour up to 4 h postpartum using a visual analogue scale. The collected data were analyzed in SPSS-16 software at a significance level of P < 0.05.
Results
The median of the afterpain score in the first hour (P = 0.05) and second hour (P = 0.274) postpartum did not differ significantly between the two groups, but this score was lower in the reflexology group at the third hour (P < 0.001) and fourth hour (P < 0.001) postpartum. The mean total afterpain score in the 4 h postpartum was significantly lower in the reflexology group (P < 0.001).
Conclusion
The results revealed that foot reflexology in the fourth stage of labor has positive effects on relief from uterine afterpain. Reflexology is therefore recommended as a measure to reduce postpartum uterine afterpains.
Similar content being viewed by others

Background
Pregnancy, labor, and puerperium are associated with many changes in women’s body and can affect their health [1]. Uterine afterpains are reportedly the most prevalent postpartum pain (77%) in multiparous women [2]. Uterine afterpains usually last two to 4 days postpartum and resolve spontaneously. Factors affecting pain intensity include multiparity, uterine overdistention (multiple pregnancies, large fetus, polyhydramnios), breastfeeding, prolonged labor stages, analgesia during labor, maternal physical and mental disorders, history of dysmenorrhea, maternal weight, and cultural factors such as race, education and religion [3,4,5,6,7,8,9,10,11]. The severity of afterpains increases in multiparous women due to the increased sensitivity of their central nervous system and decreased uterine muscle tone following multiple deliveries or uterine overextension, while nulliparous women experience little or no afterpain because their uterus has high muscle tone and contracts well [3, 4, 12].
Afterpains can lead to maternal and neonatal complications including anxiety, sleep disturbances, emotional disorders, depression, inability to care for the baby and continue breastfeeding, delays in early breastfeeding, and reduced maternal ability to perform daily chores. James et al. (2008) reported pain in the early hours postpartum as one of the most important factors contributing to chronic postpartum pain and depression [13]. Furthermore, pain and stress increase adrenaline release and decrease oxytocin release, thus leading to the cessation of the oxytocin reflex and disrupting breast milk production in addition to causing discomfort for the mother [14].
The most common method used to relieve afterpains is the administration of oral analgesics such as acetaminophen and ibuprofen [15]. Nonetheless, some analgesics (e.g., mefenamic acid and ibuprofen) occasionally cause side effects such as nausea, vomiting, diarrhea, abdominal pain, bleeding, gastrointestinal obstruction or perforation, dizziness, drowsiness, seizures, acute renal failure, and interstitial nephritis [16, 17]. In the United States, the serious side effects of nonsteroidal anti-inflammatory drugs (NSAIDs) have resulted in 100,000 hospitalizations and more than 16,500 deaths [17]. Medication side effects have drawn attention to non-pharmacological pain management modalities, including reflexology. During breastfeeding, women are very much concerned about their drug intake, since some amount of any drug they take (about 1 %) enters the breast milk [18].
Reflexology is a branch of complementary medicine and an old and non-invasive method that involves massaging reflex points on the hand and legs. This method can reduce cortisol and adrenaline levels, increase the secretion of serotonin, endorphins and enkephalins, increase vasodilation in the peripheral arteries and improve blood flow, eliminate toxins, and boost the immune system by acting on the interstitial fluid and connective tissue throughout the body [19]. Reflexology generates electrochemical messages and thus stimulates certain nerve points, and this action is done to reduce stress and balance the body [20].
A systematic review study also showed that reflexology during different stages of labor reduces labor pain severity [21].
Although numerous studies have reported the effect of reflexology on labor pain and post-cesarean section pain, an extensive review of literature up to the time of writing this paper yielded no studies regarding the effects of reflexology on the other stages of labor, including the fourth stage and the pain experienced after natural delivery. Since reflexology is a non-invasive modality that can be used along conventional therapies to reduce afterpains and mitigate the side effects of chemical medications, the present study was conducted to investigate the effect of foot reflexology performed in the fourth stage of labor on afterpains.
Methods
Trial design
The protocol of this randomized clinical trial was approved by the Ethics Committee of Gonabad University of Medical Sciences (IR.GMU.REC.1397.079). The study was also registered at the Iranian Registry of Clinical Trials on 4 February 2019 (IRCT20181214041962N1). The report of this clinical trial is based on the CONSORT 2010 checklist [22].
Participants and setting
Pregnant women referring to Allameh Bohlool Gonabadi Hospital in Gonabad and 17-Shahrivar Hospital in Mashhad, Iran, from February 2019 to July 2019, were enrolled for this study. The most important inclusion criteria were: Having no history of postpartum hemorrhage, gravida 2 or 3, gestational age of 37–42 weeks, no high-risk pregnancy, and no uterine overdistention. The exclusion criteria were: Unwillingness of the mother to continue participation, manual removal of the placenta and membranes, the need for additional treatments to control bleeding, and neonatal birth weight over 4 kg. The inclusion and exclusion criteria are fully described in the paper that reports the study protocol [23].
Sample size and randomization
The results reported by Yousefi et al. (2011) were used for determining the sample size required for comparing the two groups in G*Power software, version 3.1.9.2 [24], and t-tests were used for this purpose. In this study, the effect size d was 0.712, type I error was a maximum of 5%, and the test power was 80%, making the overall sample size 64 (32 per group). Taking into account a potential 20% sample loss, the final sample size reached 40 per group.
The researcher visited the select hospitals to carry out convenience sampling. The participants were then randomly allocated to the intervention and control groups by permuted blocks of four. To prevent selection bias, allocation to the groups was performed by an independent third person and the allocation sequence was concealed in sealed envelopes numbered from 1 to 80. Except for the senior researcher, the other investigators in the clinic were unaware of the size and sequence of the blocks. After the recruitment of the participants, the assigned envelopes were opened based on their order and the subjects were assigned to either the intervention group (A) or the control group (B) [23].
The sampling process was not concurrent in the two select hospitals, and it was first carried out at Allameh Bohlool Gonabadi Hospital and then continued in 17-Shahrivar Hospital.
Study instruments
Data were collected using several questionnaires, including a demographic and obstetric questionnaire, a labor checklist and the visual analogue scale (VAS) to assess the afterpain intensity.
The instruments are described in detail in the protocol article of this study [23]. The items in the demographic and obstetric questionnaire included the parturient and her husband’s age and education, weight, and obstetric history, i.e., gravidity, parity, postpartum bleeding, dysmenorrhea, gestational age, bleeding in pregnancy, and the position of the placenta.
The labor stage checklist included items such as vital signs in different labor stages, medications used to relieve labor pain or accelerate labor, the duration of each labor stage, neonatal weight, placental weight, and analgesics used in the fourth stage of labor.
VAS is a standard tool with a confirmed validity as per previous studies, including the one by Gallagher (2002) [25]. The reliability of VAS has also been confirmed in various studies, such as the one by Khalilian Muvahhed et al. (2012), which reported the equivalent forms reliability as r = 0.91 [26]. It ranges from 0 to 10, with a higher score indicating the more pain intensity.
Interventions and outcomes
Before sampling, the researcher’s skill in performing foot reflexology techniques based on the standard protocol was approved by a traditional Chinese medicine and acupuncture specialist after passing several training sessions. At the beginning of the study, the demographic and obstetric questionnaire was completed for the mother by asking questions from her and checking her hospital records. The researcher was present at the mother’s bedside during the second stage and monitored the entire second and third stages of labor and recorded the necessary information in the labor checklist. The participants were blinded to their group allocation (single-blind design). After the third stage of labor, the researcher started the intervention in the experimental group. The following measures were taken to ensure similar conditions were observed for the intervention in both arms; for instance, the room had to be private and a pillow was supposed to be placed under the foot to provide comfort. The same researcher (i.e., the first author) carried out the intervention in both arms. The reflexology group received 4 min of general massage on each foot, followed by 2 min of specific reflexology on each point of the uterus, pituitary, and solar plexus in the form of rotational pressures. Prior to this study, no research had been conducted on the afterpains of vaginal delivery. These points were selected for the reflexology because they have been effective in reducing maternal pain and anxiety during childbirth according to various studies [19]. In a study by Azizi et al., reflexology reduced cesarean section pain [24]. Reflexology was also performed in the second hour postpartum.
The control group received general massage on each foot for 4 min, followed by rotational pressures on a neutral point on the lateral side of the heel (placebo point) for 6 minutes. This step was repeated in the second hour postpartum. The VAS was marked by the participants at each time point of one, two, three and 4 h postpartum in both groups to check their afterpain intensity. Postpartum care was provided to both groups according to the national protocol. The use of NSAIDs, including mefenamic acid, in the third and fourth hours after delivery was also recorded.
Statistical analysis
SPSS-16 package was used for the statistical analysis of the data. Shapiro-Wilk’s test was used to check the normal distribution of the quantitative variables. The mean scores of the quantitative variables were compared using the independent-samples t-test and Mann-Whitney’s U-test. The qualitative and categorical variables were compared using the Chi-squared test. Friedman’s test was used to evaluate changes in the median score of postpartum pain separately in each group. To compare the postpartum pain scores at the different time points, since the two groups did not match in terms of mefenamic acid dosage in the third and fourth hours, the analysis of covariance (ANCOVA) was used to adjust the effect of mefenamic acid use as a confounder. The level of statistical significance was 0.05.
Results
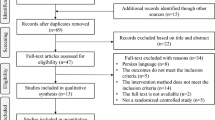
This study assessed the eligibility of 138 individuals and included 100 individuals in the study, who were allocated to the two groups (reflexology and control groups). During the study, 20 participants were excluded due to receiving misoprostol or extra oxytocin or showing lack of cooperation. Finally, 80 individuals (40 in the reflexology group and 40 in the control group) were evaluated (Fig. 1).

The flow chart of randomized clinical trials on the effect of foot reflexology in the fourth stage of labor on uterine afterpains
There was no statistically significant difference between the two groups in terms of demographic characteristics such as maternal age, husband’s age, maternal education, husband’s education, maternal occupation, husband’s occupation, maternal weight, and history of dysmenorrhea (Table 1).
The dose of mefenamic acid consumed at 4 h postpartum was not significantly different between two groups. Nonetheless, its dose used in the third hour and the total dose of mefenamic acid were significantly higher in the control group (Table 2).
The mean scores of afterpains were higher in the reflexology group than the control group in the first hour (P = 0.05) and second hour (P = 0.27) postpartum, but this difference was not statistically significant (Table 3). After adjustment for mefenamic acid usage, the mean scores of afterpains were significantly lower in the reflexology group at3 h (P < 0.001) and 4 h (P < 0.001) postpartum. Furthermore, the total mean score of afterpains throughout the 4 h postpartum was significantly lower in the reflexology group (P = 0.001) (Table 3). As an additional step of analysis, members of both groups who had not used any painkillers at all (n = 60) were also compared on the basis of their group, and the results were found to be the same in both groups (data not shown).
According to Friedman’s test, the median score of afterpains did not change significantly from the first to the fourth hours postpartum in the control group (P = 0.056); however, the median score of total afterpains decreased in the reflexology group from the first to fourth hours postpartum (P < 0.001) (Fig. 2).

Comparison of the mean postpartum pain in the foot reflexology and control groups
Discussion
Afterpains felt in the lower abdomen or lower back are one of the most prevalent complaints after labor [27]. NSAIDs are the most common treatment for afterpains [28]. In most studies, however, mefenamic acid has been compared to herbal pain killers to examine the possible side effects of this NSAID. Chananeh et al. (2018) reported that the combination of Nigella sativa and mefenamic acid is more effective in reducing afterpains than only mefenamic acid [2]. Abedian et al. (2016) also reported that Chamomile matricaria capsules are more effective in reducing afterpain than mefenamic acid [29]. Since mefenamic acid consumption was effective in reducing afterpain in the cited studies, this interfering variable was controlled in the present study using the ANCOVA.
Complementary medicine used for the treatment of afterpains includes a variety of anti-inflammatory and pain-relieving herbs, such as dill and Nigella sativa, or acupressure and acupuncture, which affect the body’s energy channels. Since no study was found on the effect of foot reflexology in the fourth stage of labor on afterpains in our review of literature, the results of the present study are discussed against and compared with the findings of the most relevant articles on the effect of complementary medicine, such as acupressure or acupuncture, on afterpains and the use of foot reflexology in the treatment of pain. This result is consistent with the present findings. The similarity of the results of the two studies can be attributed to the fact that the mechanisms of pain are somewhat similar in labor and afterpains. Ghasemali et al. (2014), Mathew et al. (2016) and Jenabi et al. (2011) reported positive effects for foot reflexology on pain relief in the first stage of labor [30,31,32]. First, the instruments used and the types of intervention given in the cited studies are similar to those in the present study; second, the mechanism of pain in labor and postpartum pain are somewhat similar; the similarity in the results obtained in the studies can thus be justified.
Mokhtari et al. (2010), Abbaspoor et al. (2014), and Razmjo et al. (2012) reported a reduction in pain after cesarean section using foot reflexology [24, 33, 34]. Their results are consistent with the present findings too. Although part of the pain after cesarean section is related to the incision site, the pain experienced after c-section and vaginal delivery afterpains is generally similar in nature and caused by uterine contractions. Therefore, the pain relief mechanism in the cited studies appears to be similar to that in the present study and is based on foot reflexology massage, which stimulates and activates the neural pathways and the subtle energy pathways associated with the sole and can reduce pain intensity in patients. During massage, blood circulation is improved and the transmission of pain signals through the sensory nerves is inhibited, and pain relief is thus achieved by the release of endorphins and enkephalins [35].
Soltani et al. (2017) used acupressure but found that it did not reduce afterpains in the first and second hours postpartum [36]. This failure to reduce afterpains in the first hour postpartum is consistent with the present study, but the failure observed in the second hour postpartum is not. This difference can be attributed to the place and time of the intervention and also to the fact that the time of pain intensity measurement and participants’ gravidity and parity differ in the two studies; in Soltani’s study, the pain intensity of women with a parity of five or less was measured in one and 2 h postpartum, but in the present study, the severity of pain was measured in women with a parity of two or three up to 4 h postpartum.
In the study by Bakhtyari Nia et al. (2019), the participants were given 10 min of massage on each foot (general foot massage, followed by the application of pressure on the pituitary points, the solar plexus points, the inner arch of the foot and the uterine point) and the severity of postoperative pain was measured in them immediately, 30, 60, 120 min and 6 h after the intervention. In their study, the afterpain experienced in the intervention group was reduced compared to the control group on all the measurement occasions [37]. In the present study, afterpain was measured one, two, three and 4 h after the intervention, and a reduction was noticed in it only at three and 4 h postpartum in the reflexology group. Bakhtyari Nia’s results are consistent with the present findings.
The limitations of the present study include the failure to confirm the accuracy of participants’ statements due to ethical constraints and the influence of personal and genetic characteristics on the pain tolerance. The massage was given by a researcher trained by a complementary medicine specialist. Another limitation was the impossibility of blinding the professionals who performed the reflexology massage.
The strengths of this study include its RCT design, the significance of the subject matter, which has been neglected in literature for the most part, and the use of complementary therapies in the puerperium.
Conclusion
The results of the present study showed that foot reflexology in the fourth stage of labor has positive effects on and can relieve afterpains. Therefore, it is recommended that foot reflexology be used in clinics for postpartum care as a modality without side effects to improve midwifery services.
Availability of data and materials
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Abbreviations
- RCT:
-
Randomized controlled trial
- VAS:
-
Visual analogue scale
- IRCT:
-
Iranian Registry of Clinical Trials
References
Zanardo V, Parotto M, Manghina V, Giliberti L, Volpe F, Severino L, Straface G. Pain and stress after vaginal delivery: characteristics at hospital discharge and associations with parity. J Obstet Gynaecol. 2020;40(6):808–12. https://doi.org/10.1080/01443615.2019.1672140.
Chananeh M, Janati Ataei P, Dolatian M, Mojab F, Nasiri M. Effects of the combination of nigella sativa and mefenamic acid and mefenamic acid alone on the severity of postpartum pain in multiparous women: a double-blind clinical trial. Iran J Obstet Gynecol Infertil. 2018;21(4):62–71.
Williams JW, Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe JS. Williams obstetrics. 15, editor. Golban: IRAN; 2018.
Holdcroft A, Snidvongs S, Cason A, Doré CJ, Berkley KJ. Pain and uterine contractions during breast feeding in the immediate post-partum period increase with parity. Pain. 2003;104(3):589–96.
Yerby M. Pain in childbearing: key issues in management: Elsevier health sciences; 2000.
Taffazoli M, Khadem AM. Assessment of factors affecting afterpain in multiparous women delivered in Mashhad 17-Shahrivar hospital, Mashhad, Iran. J Midwife Reprod Health. 2014;2(1):60–5.
Jangsten E, Bergh I, Mattsson LÅ, Hellström AL, Berg M. Afterpains: a comparison between active and expectant management of the third stage of labor. Birth. 2011;38(4):294–301.
Russell R, Reynolds F. Back pain, pregnancy, and childbirth. BMJ. 1997;314(7087):1062.
Jangsten E, Strand R, de Freitas ED, Hellström AL, Johansson A, Bergström S. Women’s Perceptions of Pain and Discomfort after Childbirth in Angola. Afr J Reprod Health. 2005;9(3):148–58.
Fang X, Huan Y, Tao Y, Song Y, Du W, Liu Z, et al. Incidence, severity, and determinants of uterine contraction pain after vaginal delivery: a prospective observational study. Int J Obstet Anesth. 2021;46:102961.
Fahey JO. Best practices in management of postpartum pain. J Perinat Neonatal Nurs. 2017;31(2):126–36.
Betts D. Postnatal acupuncture. J Chinese Med. 2005;77:5–1542.
Eisenach JC, Pan PH, Smiley R, Lavand’homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94.
Lewallen LP, Dick MJ, Wall Y, Zickefoose KT, Hannah SH, Flowers J, et al. Toward a clinically useful method of predicting early breast-feeding attrition. Appl Nurs Res. 2006;19(3):144–8.
Batten M, Stevenson E, Zimmermann D, Isaacs C. Implementation of a hydrotherapy protocol to improve postpartum pain management. J Midwif Women’s Health. 2017;62(2):210–4.
Shadipour M, Simbar M, Salamzadeh J, Nasire N. A comparative study on the effects of Menstrogol and Mefenamic acid on postpartum after-pain. Iran South Med J. 2014;16(6):401–9.
Ebrahim Zadeh MA, Gholami K, Gharanjik U, Javadian P. S.M. evaluation of drug interactions of non-stteroidal anti-inflamatory drugs (NSAIDs) in sari insured prescriptions during 1999-2001. Razi J Med Sci. 2003;10(36):489–95.
Vahidi AA, Eranmanesh E. Breastfeeding and medications. J Kerman Univ Med Sci. 2011;18(2):194–201.
Akköz Çevik S, Incedal İ. The effect of reflexology on labor pain, anxiety, labor duration, and birth satisfaction in primiparous pregnant women: a randomized controlled trial. Health Care Women Int. 2020:1–16.
Bagheri L, Ghiasi A, Ahmadnia E. Effect of reflexology on the length of labor: a systematic review and Meta- analysis of clinical trials. Iran J Obstet Gynecol Infertil. 2018;21(1):105–14.
Sharifi N, Bahri N. The effect of foot reflexology on the severity of labor pain: a systematic review study. Iran J Obstet Gynecol Infertil. 2019;22(9):85–93.
Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332.
Sharifi N, Bahri N, Talasaz FH, Azizi H, Nezami H. The effect of foot reflexology in the fourth stage of labor on postpartum hemorrhage and after pain: a randomized controlled trial protocol. Adv Integr Med. 2020.
Razmjoo N, Yousefi F, Esmaeeli H, Azizi H, Lotfalizadeh M. Effect of foot reflexology on pain and anxiety in women following elective cesarean section. Iran J Obstet Gynecol Infertil. 2012;15(1):8–16.
Gallagher EJ, Bijur PE, Latimer C, Silver W. Reliability and validity of a visual analog scale for acute abdominal pain in the ED. Am J Emerg Med. 2002;20(4):287–90.
Azhari S, Khalilian Muvahhed H, Tara F, Esmaeli H. Comparison the effect of sitting and kneeling positions during the second stage of labor on pain and duration of second stage of labor in nulliparous women. Iran J Obstet Gynecol Infertil. 2013;15(38):7–16.
Eshkevari L, Trout KK, Damore J. Management of postpartum pain. J Midwife Women’s Health. 2013;58(6):622–31.
Pourmaleky S, Najar S, Montazery S, Haghighizadeh MH. Comparison between the effects of Zintoma (ginger) and Mefenamic acid on after pain during postpartum in multiparous women. Iran J Obstet Gynecol Infertil. 2013;16(79):18–25.
Abedian Z, Rezvani Fard M, Asili J, Esmaeili H, Dadgar S. Comparison of the effect of chamomile Matricaria and Mefenamic acid capsules on postpartum hemorrhage in women with postpartum pain. Iran J Obstet Gynecol Infertil. 2016;19(14):1–8.
Mathew AM, Francis F. Effectiveness of Foot Reflexology in Reduction of Labour Pain among Mothers in Labour Admitted at PSG. Int J Nurs Educ. 2016;8(3).
Hajighasemali S, Amir Ali Akbari S, Akbarzadeh A, Heshmat R. Comparison between effect acupuncture on SP6 point and reflexology on the severity of first-stage labor pain. Pars Jahrom Univ Med Sci. 2014;12(4):17–22.
Jenabi E, Hajiloo Mohajeran M, Torkamani M. The effect of reflexology on relieving the labor pain. Iran J Obstet Gynecol Infertil. 2012;14(8):34–8.
Mokhtari NJ, Sirati NM, Sadeghi SM, Ghanbari Z, Babatabar DH, Mahmoudi H. Comparison of impact of foot reflexology massage and Bensone relaxation on severity of pain after cesarean section: a randomized trial; 2010.
Abbaspoor Z, Akbari M, Najar S. Effect of foot and hand massage in post–cesarean section pain control: a randomized control trial. Pain Manage Nurs. 2014;15(1):132–6.
Watson S. The effects of massage: an holistic approach to care. Nurs Stand. 1997;11(47):45–7.
Soltani M, Azhari S, Khorsand Vakilzadeh A, Tara F, Mazloum SR. The effect of acupressure on uterine tone and pain after delivery. Iran J Obstet Gynecol Infertil. 2017;20(9):91–100.
Nia GB, Montazeri S, Afshari P, Haghighizadeh MH. Foot reflexology effect on postpartum pain-a randomized clinical trial. J Evol Med Dent Sci. 2019;8(39):2976–82.
Acknowledgements
The present study was extracted from an approved master’s thesis in midwifery at Gonabad University of Medical Sciences, funded by the Research and Technology Deputy of the university (Grant number: A1016741). We express our gratitude to the Research Deputy of Gonabad University of Medical Sciences for their financial support.
Funding
This research was funded by the research council of Gonabad University of Medical Sciences (grant number: A1016741). The funding body did not have any role in the study design, data analysis, manuscript preparation and submission.
Author information
Authors and Affiliations
Contributions
NSh, NB, FH, HA and HN contributed to the conception or design of the research protocol. NSh and NB formulated and revised the research protocol critically for important intellectual content. HN reviewed the statistical methods and sample size calculations. HN and HT analyzed the data. NSh, NB, FH, HA, HN, and HT reviewed the drafts and approved the final version of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants provided written informed consent for participating in the study. The trial received its ethical approval by the Regional Committee on Ethics in Medical Research at Gonabad University of Medical Sciences on 3 December 2018 (Approval ID: IR.GMU.REC.1397.079). All the experimental protocols involving human subjects in this research were in accordance with the national/institutional guidelines. This study was also registered at the Iranian Registry of Clinical Trials on 4 February 2019 (IRCT20181214041962N1). Participants’ information was collected in a personal file and kept in a locked office with limited access.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sharifi, N., Bahri, N., Hadizadeh-Talasaz, F. et al. A randomized clinical trial on the effect of foot reflexology performed in the fourth stage of labor on uterine afterpain . BMC Pregnancy Childbirth 22, 57 (2022). https://doi.org/10.1186/s12884-022-04376-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-022-04376-w