
Abstract
Background
Parkinson’s disease (PD) is a progressive neurodegenerative disorder causing motor and non-motor symptoms that can affect independence, social adjustment and the quality of life (QoL) of both patients and caregivers. Studies designed to find diagnostic and/or progression biomarkers of PD are needed. We describe here the study protocol of COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015), an integral PD project based on four aspects/concepts: 1) PD as a global disease (motor and non-motor symptoms); 2) QoL and caregiver issues; 3) Biomarkers; 4) Disease progression.
Methods/design
Observational, descriptive, non-interventional, 5-year follow-up, national (Spain), multicenter (45 centers from 15 autonomous communities), evaluation study. Specific goals: (1) detailed study (clinical evaluations, serum biomarkers, genetic studies and neuroimaging) of a population of PD patients from different areas of Spain, (2) comparison with a control group and (3) follow-up for 5 years. COPPADIS-2015 has been specifically designed to assess 17 proposed objectives. Study population: approximately 800 non-dementia PD patients, 600 principal caregivers and 400 control subjects. Study evaluations: (1) baseline includes motor assessment (e.g., Unified Parkinson’s Disease Rating Scale part III), non-motor symptoms (e.g., Non-Motor Symptoms Scale), cognition (e.g., Parkinson’s Disease Cognitive Rating Scale), mood and neuropsychiatric symptoms (e.g., Neuropsychiatric Inventory), disability, QoL (e.g., 39-item Parkinson’s disease Quality of Life Questionnaire Summary-Index) and caregiver status (e.g., Zarit Caregiver Burden Inventory); (2) follow-up includes annual (patients) or biannual (caregivers and controls) evaluations. Serum biomarkers (S-100b protein, TNF-α, IL-1, IL-2, IL-6, vitamin B12, methylmalonic acid, homocysteine, uric acid, C-reactive protein, ferritin, iron) and brain MRI (volumetry, tractography and MTAi [Medial Temporal Atrophy Index]), at baseline and at the end of follow-up, and genetic studies (DNA and RNA) at baseline will be performed in a subgroup of subjects (300 PD patients and 100 control subjects). Study periods: (1) recruitment period, from November, 2015 to February, 2017 (basal assessment); (2) follow-up period, 5 years; (3) closing date of clinical follow-up, May, 2022. Funding: Public/Private.
Discussion
COPPADIS-2015 is a challenging initiative. This project will provide important information on the natural history of PD and the value of various biomarkers.
Similar content being viewed by others


Background
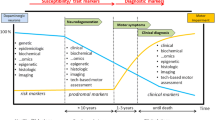
Parkinson’s disease (PD), the second most common neurodegenerative disease after Alzheimer’s disease, is a progressive neurodegenerative disorder causing motor and non-motor symptoms that result in disability, loss of patient autonomy and caregiver burden [1]. Understanding of PD has changed over recent years, with the disease currently considered to be a neurodegenerative disease involving a diversity of pathways and neurotransmitters that may explain, in part, the large range of symptoms that patients may have [2]. PD is not only a motor disease, as it also involves various non-motor symptoms that are important for different reasons. Non-motor symptoms are frequent and disabling, therefore, early identification and proper management of these symptoms is important [3]. Some non-motor symptoms (e.g., olfactory disorders, constipation or sleep disturbances) may precede motor symptoms, and could be useful as prodromal/preclinical markers of PD [4]. Others, such as dementia and psychosis, are more frequently develop during the late stages of the disease and sometimes difficult to manage. We need to know, in detail, the progression of non-motor symptoms and their relationship with motor changes over time. Reliable and well-validated biomarkers for PD to identify individuals “at risk” before motor symptoms develop, to accurately diagnose individuals at the threshold of clinical PD, and to monitor PD progression (motor and non-motor symptoms) throughout the course of the disease would dramatically accelerate research into both the cause and treatment of PD [5].
Although the identification of a marker for diagnosis and for disease progression (preferably one that is non-invasive, affordable and accessible) is of utmost importance, concepts like quality of life (QoL) are also very important in chronic diseases, such as PD, for which a cure does not exist [6]. Improving patient QoL and identifying factors that lead to caregiver burden are very important aspects of the management of PD. In particular, the role of the principal caregiver in PD is very important because caregiver burden generates poor care and, in the long term, leads to patient institutionalization [7]. Specifically, identifying the changes experienced by PD patients and their caregivers in their QoL and degree of burden, respectively, over time, as well as factors that may predict these changes, in order to carry out a proper intervention, should be a priority. Well-designed, longitudinal prospective studies are key. Access to a population with a high proportion of patients who have been assessed comprehensively and rigorously, without screening bias, is highly valuable for both cross-sectional analysis and prospective follow-up. This is especially relevant for studying populations affected by a neurodegenerative disease, given that these patients are expected to develop different complications that we could identify and analyze.
Studies designed to identify PD diagnostic and/or progression biomarkers and to elucidate the natural progression of the disease are needed. We describe here the COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015) study protocol, an integral PD project based on four aspects/concepts: 1) PD as a global disease (motor and non-motor symptoms); 2) QoL and caregiver issues; 3) Biomarkers; 4) Disease progression.
Methods/design
Type of study
COPPADIS-2015 is a national, multicenter, epidemiological, descriptive, observational, non-interventional, longitudinal-prospective, 5-year follow-up study. COPPADIS-2015 has been classified by the AEMPS (Agencia Española del Medicamento y Productos Sanitarios) as a Post-authorization Prospective Follow-Up study.
The study will be conducted at different hospital sites in Spain. The essential requirement will be that the Principal Investigator participating at each site has experience and skills in the diagnosis and standard management of patients with PD in their daily clinical practice. As such, the participating site could be any establishment from a highly-specialized Movement Disorders Unit of a tertiary hospital to a general neurologist from a regional hospital with the aforementioned skills. More than one hundred researchers from 48 centers in Spain, from 15 autonomous communities, will participate in this project.
Specific goals
The aim COPPADIS-2015 is to: (1) study in detail (clinical evaluations, serum biomarkers, genetic studies and neuroimaging) a population of patients with PD representative of different areas of Spain; (2) compare it with a control group and (3) follow-up for 5 years. COPPADIS-2015 has been specifically designed to assess 17 proposed objectives (Table 1).
Study population
Non-dementia patients with idiopathic PD, caregivers (patient’s primary caregiver, if applicable) and controls will be assessed. We plan to include:
1) Approximately 800 patients with PD. Patients will be included if they have idiopathic PD according to the United Kingdom Parkinson’s Disease Society Brain Bank criteria [8], have no dementia criteria (Mini Mental State Examination [MMSE] ≥ 26) [9], are aged between 30 and 75 years, are participating voluntarily and have provided written informed consent. Patients will be excluded from the study if they: (1) are not capable of completing the questionnaires adequately; (2) have other disabling concomitant neurological disease (stroke, severe head trauma, neurodegenerative disease, etc.); (3) have other severe and disabling concomitant non-neurological disease (oncological, autoimmune, etc.); (4) have known chronic anemia and/or hyperuricemia; (5) are receiving active treatment with continuous infusion of levodopa and/or apomorphine and/or with deep brain stimulation; (6) they are participating in a clinical trial and/or other type of study that does not permit concomitant participation in another or (7) if long-term follow-up is not expected to be possible.
2) Approximately 600 caregivers (patient’s primary caregiver). A person who, without being a professional and/or receiving money in exchange for services, lives with the patient and is responsible for his/her care will be included as a primary caregiver [10]. He or she must voluntarily agree to participate and provide written informed consent.
3) Approximately 400 control subjects matched by age, sex and educational level. The control subject could be a family member (not the patient’s caregiver) or friend of the patient who would like to participate voluntarily. The same inclusion criteria (except PD diagnosis) and exclusion criteria as those for the patients will be applied.
Study design
The study will be carried out in two phases:
-
1)
Cross-sectional assessment (recruitment of patients with a baseline assessment over a period of 16 months, from November 2015 to February 2017). We have also considered the possibility, if necessary, of extending the recruitment period up to a maximum of 24 months in order to achieve the proposed target sample size.
-
2)
Prospective follow-up of the defined cohort of PD patients (COPPADIS) over 5 years.
Study assessments
The Principal Investigator will make the decision on the patient’s inclusion. Extensive information on sociodemographic aspects, factors related to PD, comorbidity and treatment will be collected. Patient baseline evaluations will include motor assessment (Hoenh & Yahr [11], Unified Parkinson’s Disease Rating Scale [UPDRS] part III and part IV [12], Freezing of Gait Questionnaire [FOGQ] [13]), non-motor symptoms (Non-Motor Symptoms Scale [NMSS] [14], Parkinson’s Disease Sleep Scale [PDSS] [15], Visual Analog Scale-Pain [VAS-Pain] [16], Visual Analog Fatigue Scale [VAFS] [17]), cognition (MMSE [18], Parkinson’s Disease Cognitive Rating Scale [PD-CRS] [19], completing a simple 16-piece puzzle [20]), mood and neuropsychiatric symptoms (Beck Depression Inventory-II [BDI-II] [21], Neuropsychiatric Inventory [NPI] [22], Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale [QUIP-RS] [23]), disability (Schwab & England Activities of Daily Living Scale [ADLS] [24]) and QoL (39-item Parkinson’s disease Quality of Life Questionnaire Summary Index [PDQ-39SI] [25], PQ-10 [26], European Health Interview Survey-Quality of Life 8 item index [EUROHIS-QOL 8 item-index] [27]). Caregiver baseline evaluation includes the degree of burden (Zarit Caregiver Burden Inventory [ZCBI] [28], Caregiver Strain Index [CSI] [29]), mood (BDI-II) and QoL (PQ-10, EUROHIS-QOL 8 item-index). The same evaluation as for the patients, except for the motor assessment, will be performed in control subjects at baseline.
In a subgroup of 400 consecutive non-selected subjects (300 PD patients and 100 controls) willing to participate voluntarily and without any contraindications (e.g., magnetic resonance imaging [MRI]), complementary tests will be performed as follows:
-
1)
Blood sample collection for the determination of different molecular biomarkers: S-100b protein, tumor necrosis factor (TNF)-ɑ, interleukin (IL)-1, IL-2, IL-6, vitamin B12, methylmalonic acid, homocysteine, uric acid, C-reactive protein, ferritin and iron. The analysis will be conducted at a common laboratory: REFERENCE LABORATORY (www.reference-laboratory.es). The extraction of the sample will be carried out no longer than 3 months after the first clinical assessment.
-
2)
Blood sample collection for genetic studies on lymphocyte DNA and RNA with 4 fundamental objectives: (1) expression profile studies; (2) exome sequencing (SNCA, LRRK2, FBXO7, PINKI, PRKN, DJ1, HTRA2, UCHLI, ATPI3A2, VPS35, PLA2G6, GIGYF2, EIF4G1, GBA); (3) analysis of genes considered relevant according to the state of the art; (4) candidate gene association studies in order to determine if the pathological variations are present more frequently in subjects with PD (with respect to the control group).
-
3)
Neuroimaging study: T1 3D MRI of the head using standardized protocols that include frontal and/or coronal slices in T1 sequence at 1.5 T or above without intravenous contrast. Volumetric (spoiled gradient recalled sequence; TR 8,5 ms, TE 4 ms, flip angle 8°, FOV 240 × 240 mm2, thickness 1 mm, matrix 288 × 288, voxel size 0.84 mm3) and tractography (echo-planar imaging; TR 9.500 ms, TE 73 ms, FOV 224, thickness 2 mm, matrix 128 × 128, b-factors of zero and 700 s/mm2) studies will be performed. Also, the Medial Temporal Atrophy Index (MTAi) [30] will be calculated. The MRI study will be performed no longer than 6 months after the first clinical assessment.
Figure 1 shows baseline study assessments. Table 2 shows data regarding centers, number of patients that they have estimated to recruit and distribution of patients selected for the complementary studies according to the different centers.

Recruitment period, from November 2015 to February 2017 (baseline assessment of each participating subject). 1, patient inclusion process and motor assessment by the Principal Investigator (neurologist who is an expert in movement disorders and Parkinson’s disease); 2a, non-motor assessment by the Principal Investigator, specialized nurse, psychologist or fellow with adequate training; 2b, caregiver assessment; 2c, control assessment. *Only patients with motor fluctuations (UPDRS-IV) will be assessed during the OFF-medication (first thing in the morning without taking medication in the 12 previous hours) and during the ON-medication state; the rest will only be assessed during the OFF-medication state. Blood samples from the baseline assessment will be stored for the purpose of being able to test other future markers not currently included in the project
During the 5 years of follow-up, annual evaluations (PD patients) or evaluations at 24, 48 and 60 months (caregivers and controls) will be performed. Figure 2 shows assessments during the follow-up phase in each group. The subjects who undergo complementary tests at baseline will repeat the head MRI study (preferably at the same site and with the same machine) and determination of molecular markers (S-100b, TNF-ɑ, IL-1, IL-2, IL-6, vitamin B12, methylmalonic acid, homocysteine, uric acid, C-reactive protein, ferritin and iron; same laboratory, REFERENCE LABORATORY) at 60 months. Table 3 shows the working plan summary.

Follow-up of the cohort of patients (a), caregivers (b) and controls (c). At the end of follow-up, the patients (n = 300) and controls (n = 100) who underwent complementary tests at baseline will undergo repeat testing (molecular markers and imaging study). ADLS, Schwab & England Activities of Daily Living Scale; BDI, Beck Depression Inventory; CSI, Caregiver Strain Index; FOGQ, Freezing of Gait Questionnaire; HY, Hoenh & Yahr; NMSS, Non-Motor Symptoms Scale; NPI, Neuropsychiatric Inventory; PD-CRS, Parkinson’s Disease Cognitive Rating Scale; PDQ-39SI, 39-item Parkinson’s disease Quality of Life Questionnaire Summary Index; QUIP-RS, Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale; PDSS, Parkinson’s Disease Sleep Scale; UPDRS, Unified Parkinson’s Disease Rating Scale; VAFS, Visual Analog Fatigue Scale; VAS-Pain, Visual Analog Scale-Pain; ZCBI, Zarit Caregiver Burden Inventory
Data collection and statistical analysis
Data will be collected using an electronic Case Report Form (e-CRF) and will be transferred to a statistical package for subsequent analysis. The company responsible for study monitoring is Alphabioresearch (www.alphabioresearch.com).
We calculated the sample size, taking into account a maximum estimated loss to follow-up of 10 % of patients per year, and that between 15 % and 20 % of the sites involved in a multicenter study are estimated to leave the study for different reasons [31]. A minimum of 280 patients at the end of follow-up would be sufficient to include up to 27 predictive variables in the multiple regression analyses with a power of 0.8 and a confidence interval of 95 % [32]. The pertinent analysis (descriptive studies, univariate studies, binary logistic regression, multiple linear regression, etc.) will be performed based on the type of objective. In addition, given de complexity of potential analysis including a diversity of variables from different origin and measurement properties, advanced statistical methodology (data mining, artificial intelligence techniques, etc.) will be applied as needed. One of the authors (PMM) will coordinate these aspects.
Ethical considerations
The project will be conducted in accordance with the standards for Good Clinical Practice, the fundamental ethical principles established in the Declaration of Helsinki and the Oviedo Convention, as well as the requirements established in Spanish legislation in the research field. Approval of the Ethics Committee at each center was obtained.
Study timetable
-
1)
Pre-start-up procedures: until October 2015.
-
2)
First assessment (cross-sectional assessment): November 2015 to February 2017.
-
3)
Database review: March–June 2017.
-
4)
Statistical analysis: second half of 2017.
-
5)
Reporting and publication of papers (objectives 1 to 12 of the cross-sectional assessment and other subanalyses): years 2017 to 2019.
-
6)
Objectives of the prospective follow-up of the cohort: from 2018 onwards.
Future possibilities of the project
-
1)
To perform other evaluations and/or complementary studies during follow-up; for example, electromyographic studies to determine the frequency of polyneuropathy in PD patients compared with controls and also to identify related risk factors (clinical, biomarkers, etc.); other studies (optical coherence tomography, electroencephalogram, salivary secretion and/or cerebrospinal fluid analysis, skin biopsy, etc.).
-
2)
To continue follow-up of the subjects (patients, caregivers and controls) over time (10, 15, 20 years, etc.).
-
3)
To create a COPPADIS Brain Bank. We have designed a working group with the participation of members of different biobanks in Spain with the aim of create a Brain Donation Program for COPPADIS PD patients.
Discussion
The described project, COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015), is an ambitious initiative that will provide important information regarding the natural history of PD and the value of various biomarkers. The large sample size, high level of participation, with more than 40 Spanish centers involved, exhaustive clinic evaluations, including motor and non-motor features (more than 500 variables collected from the baseline assessment), biomarkers, study design and interesting future possibilities are strong points of this project. COPPADIS-2015 will enable us to identify different complications that develop over time in a very large population of patients with PD. Therefore, we expect to be able to identify the incidence of different problems, their impact on QoL and predictive factors that will allow us to identify these problems early in order to act.
This project is based on four aspects/concepts: 1) PD as a global disease (motor and non-motor symptoms); 2) QoL and caregiver issues; 3) Biomarkers; 4) Disease progression. For years, PD management was focused on motor symptoms. However, more recently, non-motor features have been gaining in importance. Non-motor symptoms are important for different reasons [33]: they are frequent and disabling; some non-motor symptoms such as hyposmia, constipation, depression or REM sleep behavior disorders can precede motor symptoms and, in the future, such symptoms could be used to establish an earlier diagnosis of premotor PD; non-motor symptoms can sometimes be difficult to manage (orthostatic hypotension, behavioral disorders, etc.); some non-motor symptoms (dementia, psychosis, etc.) increase the risk of institutionalization and generate a high economic cost; and they are not always sufficiently recognized by the neurologist. Additionally, various studies have demonstrated that non-motor symptoms impact negatively on patient QoL, and that by improving these symptoms, we help improve QoL [34, 35]. Early identification and proper management should currently be a priority in daily clinical practice [4], but for many reasons, this is not always the case. In COPPADIS-2015, we will exhaustively evaluate different non-motor features (NMSS, PDSS, VAS-Pain, VAFS, MMSE, PD-CRS, BDI-II, NPI, QUIP-RS) in a large population of PD patients. We will also compare these features with a control group and analyze their evolution with disease progression. Finally, we will try to identify related (cross-sectional assessment) and predictive (prospective follow-up) factors for the development of different non-motor symptoms. For example, factors related to mild cognitive impairment at baseline and risk factors that could predict the chance of mild cognitive impairment progressing to dementia will be identified [36]. We will also compare non-motor symptoms (and other features of the disease) and disease progression in patients with different phenotypes and motor laterality asymmetry. Moreover, we will try to determine if non-motor symptoms (NMSS) predict acute hospitalization in PD patients [37].
At present we have no cure for PD. We use different therapies to improve patient symptoms, health status, degree of autonomy and QoL. The key is to understand what factors affect QoL (depression, pain, motor complications, etc.), given that interventions will be based on these factors. Moreover, the role of the patient’s primary caregiver is also very important because PD is a neurodegenerative disorder and the patient will become increasingly dependent. We will need to determine which factors cause caregivers’ stress and increase their burden in order to carry out an early intervention, since caregiver burden generates poor care and, in the long term, often leads to the patient’s institutionalization [7]. In this regard, it has been observed that patient QoL is correlated with the caregiver’s status, and interventions targeted at improving caregiver burden to also improve the patient’s QoL have been suggested [38]. Although there are several studies focused on factors related to caregiver burden [39–41], there is no information about caregiver strain changes during disease progression. In COPPADIS-2015 we will analyze changes in QoL, mood and burden experimented by principal caregivers and we will attempt to correlate these with changes in different aspects of the disease (motor symptoms, mood, cognition, behavior, other non-motor symptoms, etc.) observed in patients.
A top priority at present in PD is to identify a diagnostic and prognostic biomarker [42, 43]. In COPPADIS-2015, different molecular markers in blood will be evaluated (S-100b protein, TNF-ɑ, IL-1, IL-2, IL-6, vitamin B12, methylmalonic acid, homocysteine, uric acid, C-reactive protein, ferritin and iron) [44–57], and genetic studies (DNA and RNA) [58], and cranial MRI (MTAi, volumetry and tractography) [30, 59–65] will be performed in a subgroup of patients and controls. We will try to identify markers with diagnostic and/or prognostic value, either alone or in combination (clinical and/or paraclinical). For example, we will analyze the role of serum S-100b protein and uric acid as possible prognostic biomarkers [44–46, 56], the relationship between serum levels of TNF-ɑ, IL-1, IL-2, IL-6 and C-reactive protein and different non-motor symptoms [47–51], or the sensitivity and specificity of a simple puzzle test as a cognitive impairment screening test. Moreover, biomarkers included in this project have some of the characteristics needed in an ideal marker: fast and affordable to obtain; available; repeatable; and safe [66, 67]. Finally, in the future, other molecular biomarkers could be analyzed from stored blood samples and other complementary studies could be done. Moreover, creation of a brain bank (COPPADIS Brain Donation Program) from patients included in this project is being developed.
Therefore, well-designed, longitudinal prospective studies must be conducted to identify a biomarker of linear progression and also to understand the natural progression of PD. Today, we still do not know what relationship exists between the progression of motor symptoms and non-motor symptoms in the long term. Different longitudinal studies with prospective follow-up of patients have provided an understanding of the development of motor complications and their relationship with the type of symptomatic therapy initially used [68–70], cognitive impairment and/or dementia [71–74], the course following a given intervention (e.g., deep brain stimulation) [75, 76] or other data on the course of the disease [77–86]. There are other promising studies currently underway with a fundamental objective of identifying a disease progression biomarker [87]. Nevertheless, many of the studies have significant limitations, such as an insufficient sample size and follow-up, significant losses to follow-up, limitations in the recruitment or origin of the sample and performance of analyses not specifically allowed for in the design. As seen for other neurodegenerative diseases like Huntington’s disease [88], the most beneficial study model for achieving relevant advances in the understanding of PD is likely to be a study that includes a baseline cross-sectional assessment of patients (with a control group) with analysis of multiple variables (clinical and complementary tests; for example, serum molecular markers, other biological samples like cerebrospinal fluid, saliva or skin, structural neuroimaging, functional neuroimaging, ophthalmological studies, neurophysiological tests, etc.) followed by a subsequent prospective follow-up (ideally over a long period of follow-up and without losses of cases) of the population studied with multiple periodic analyses that would make it possible to compare the course of the different variables analyzed. These features are all covered by the described project, COPPADIS-2015. Unlike the PPMI Study, PD patients at all Hoenh & Yahr stages who meet the selection criteria and not only early patients will be included in the COPPADIS Study. That’s because we focused firstly on studying very exhaustively a large population of PD patients from different areas of Spain analyzing the relationship between different variables according to cross-sectional study methodology. Changes observed in different variables during the follow-up will be adjusted and interestingly, different groups of subjects according to disease duration, motor stage or to have motor complications at baseline could be defined to compare evolution. Some original aspects in COPPADIS are to include the caregivers (the principal caregiver of the patient was also included in a previous Spanish Study, the ELEP Study –Estudio Longitudinal de pacientes con Enfermedad de Parkinson/Longitudinal Parkinson’s Disease Patient Study [89] –), to study the incidence and predictors of acute hospitalization and to analyze the value of the MTAi. Furthermore, as it was mentioned, we are working to develop a COPPADIS Donation Brain Program. Indeed, the long-term goal is to design a Spanish PD patients clinical-pathological registry (with the inclusion of early new patients) with long-term monitoring and implementation of many additional tests.
In conclusion, COPPADIS-2015 is a challenging and original initiative. We hope that this project will provide important information regarding the natural history of PD, including changes in motor and non-motor symptoms, QoL and caregiver burden over time, and the value of various biomarkers.
Abbreviations
- ADLS:
-
Schwab & England activities of daily living scale
- AEMPS:
-
Agencia Española del Medicamento y Productos Sanitarios
- BDI:
-
beck depression inventory
- CSI:
-
caregiver strain index
- e-CRF:
-
electronic case report form
- EUROHIS-QOL:
-
European health interview survey-quality of life
- FOGQ:
-
freezing of gait questionnaire
- HY:
-
hoenh & yahr
- IL:
-
interleukin
- MMSE:
-
mini mental state examination
- MRI:
-
magnetic resonance imaging
- MTAi:
-
medial temporal atrophy index
- NMSS:
-
non-motor symptoms scale
- NPI:
-
neuropsychiatric inventory
- PD:
-
parkinson’s disease
- PD-CRS:
-
parkinson’s disease cognitive rating scale
- PDQ-39SI:
-
39-item Parkinson’s disease quality of life questionnaire summary index
- PDSS:
-
parkinson’s disease sleep scale
- QoL:
-
quality of life
- QUIP-RS:
-
questionnaire for Impulsive-compulsive disorders in parkinson’s disease-rating scale
- TNF:
-
tumor necrosis factor
- UPDRS:
-
unified parkinson’s disease rating scale
- VAFS:
-
visual analog fatigue scale
- VAS-Pain:
-
visual analog scale-pain
- ZCBI:
-
zarit caregiver burden inventory
References
Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008;79:368–76.
Tolosa E, Gaig C, Santamaría J, Compta Y. Diagnosis and the premotor phase of Parkinson’s disease. Neurology. 2009;72 Suppl 7:12–20.
Olanow CW, Obeso JA. The significance of defining preclinical or prodromal Parkinson’s disease. Mov Disord. 2012;27:666–9.
Seppi K, Weintraub D, Coelho M, et al. The Movement Disorder Society Evidence-Based Medicine Review Update: Treatments for the non-motor symptoms of Parkinson’s disease. Mov Disord. 2011;26 Suppl 3:42–80.
Marek K, Jennings D, Tamagnan G, Seibyl J. Biomarkers for Parkinson’s [corrected] disease: tools to assess Parkinson’s disease onset and progression. Ann Neurol. 2008;64 Suppl 2:111–21.
Martinez-Martin P, Kurtis MM. Health-related quality of life as an outcome variable in Parkinson’s disease. Ther Adv Neurol Disord. 2012;5:105–17.
Tan SB, Williams AF, Kelly D. Effectiveness of multidisciplinary interventions to improve the quality of life for people with Parkinson’s disease: a systematic review. Int J Nurs Stud. 2014;51:166–74.
Daniel SE, Lees AJ. Parkinson’s Disease Society Brain Bank, London: overview and research. J Neural Transm Suppl. 1993;39:165–72.
Dubois B, Burn D, Goetz C, Aarsland D, Brown RG, Broe GA, et al. Diagnostic procedures for Parkinson’s disease dementia: recommendations from the movement disorder society task force. Mov Disord. 2007;22:2314–24.
Martinez Martin P, Arroyo S, Rojo-Abuin JM, Rodrigues-Blazquez C, Frades B, de Pedro Cuesta J, the Longitudinal Parkinson's disease Patients Study Group. Burden, perceived health status, and mood among caregivers of Parkinson’s disease patients. Mov Disord. 2008;23:1673–80.
Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology. 1967;17:427–42.
Fanhn S, Elton RL, Members of the UPDRS Development Committee. Unified Parkinson’s Disease Rating Scale. In: Fahn S, Marsden CD, Calne DB, Goldstein M, editors. Recent developments in Parkinson’s disease, Vol 2. Florham Park, NJ: Macmillan Health Care Information; 1987. p. 153–64.
Giladi N, Shabtai H, Simon ES, Biran S, Tal J, Korczyn AD. Construction of freezing of gait questionnaire for patients with Parkinsonism. Parkinsonism Relat Disord. 2000;6:165–70.
Chaudhuri KR, Martinez-Martin P, Brown RG, Sethi K, Stocchi F, Odin P, et al. The metric properties of a novel non-motor symptoms scale for Parkinson’s disease: Results from an international pilot study. Mov Disord. 2007;22:1901–11.
Chaudhuri KR, Pal S, DiMarco A, Whately-Smith C, Bridgman K, Mathew R, et al. The Parkinson’s disease sleep scale: a new instrument for assessing sleep and nocturnal disability in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2002;73:629–35.
Burckhardt CS, Jones KD. Adult measures of pain: The McGill Pain Questionnaire (MPQ), Rheumatoid Arthritis Pain Scale (RAPS), Short Form McGill Pain Questionnaire (SF-MPQ), Verbal Descriptive Scale (VDS), Visual Analog Scale (VAS), and West Haven-Yale Multidisciplinary Pain Inventory (WHYMPI). Arthritis Rheum. 2003;49:96–104.
Tseng BY, Gajewski BJ, Kluding PM. Reliability, responsiveness, and validity of the visual analog fatigue scale to measure exertion fatigue in people with chronic stroke: a preliminary study. Stroke Res Treat. 2010. Pii:412964. doi: 10.4061/2010/412964.
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–98.
Pagonabarraga J, Kulisevsky J, Llebaria G, García-Sánchez C, Pascual-Sedano B, Gironell A. Parkinson’s disease-cognitive rating scale: a new cognitive scale specific for Parkinson’s disease. Mov Disord. 2008;23:998–1005.
Richarson JTE, Vecchi T. A jigsaw-puzzle imagery tasl for assessing active visuoespacial processes in old and young people. Behav Res Methods Instruments Comput. 2002;34:69–82.
Beck AT, Steer RA, Brown GK. Beck Depression Inventory-second edition. Manual. San Antonio: The Psychological Corporation; 1996.
Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994;44:2308–14.
Weintraub D, Hoops S, Shea JA, Hurtig HI, Colcher A, Horn SS, et al. Validation of the questionnaire for impulsive-compulsive disorders in Parkinson’s disease. Mov Disord. 2009;24:1461–7.
Schwab RS. England AC. In: Third Symposium on Parkinson’s disease. Edinburgh: E. And S. Livingstone; 1969. p. 152–7.
Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson’s Disease Questionnaire (PDQ-39): development and validation of a Parkinson’s disease summary index score. Age Ageing. 1997;26:353–7.
Santos García D, de la Fuente-Fernández R. Impact of non-motor symptoms on health-related and perceived quality of life in Parkinson’s disease. J Neurol Sci. 2013;332:136–40.
Da Rocha NS, Power MJ, Bushnell DM, Fleck MP. The EUROHIS-QOL 8-item index: comparative psychometric properties to its parent WHOQOL-BREF. Value Health. 2012;15:449–57.
Novak M, Guest C. Application of a multidimensional caregiver burden inventory. Gerontol. 1989;29:798–803.
Robinson BC. Validation of a Caregiver Strain Index. J Gerontol. 1983;38:344–8.
Menéndez-González M, López-Muñiz A, Vega J, Arias-Carrión O. MTA index: a simple 2D-method for assessing atrophy of the medial temporal lobe using clinically available neuroimaging. Front Aging Neurosci. 2014;6:23.
Cervantes-Arriaga A, Rodríguez-Violante M, Zúñiga-Ramírez C, López-Ruíz M, Estrada-Bellman E, Oteiro-Cerdeira E, et al. Protocolo de estudio de una cohorte multicéntrica de pacientes mexicanos con enfermedad de Parkinson para evaluar los determinantes motores, no motores y genéticos sobre la progresión. Arch Neurocien Mex. 2012;17:159–64.
Tabachnick BG, Fidell LS. Multiple regression New York; Harper Collins College Publications. 1996.
Goldman JG, Postuma R. Premotor and non motor features of Parkinson’s disease. Curr Opin Neurol. 2014;27:431–44.
Li H, Zhang M, Chen L, Zhang J, Pei Z, Hu A, et al. Nonmotor symptoms are independently associated with impaired health-related quality of life in Chinese patients with Parkinson’s disease. Mov Disord. 2010;25:2740–6.
Honig H, Antonini A, Martinez-Martin P, Forgacs I, Faye GC, Fox T, et al. Intrajejunal levodopa infusion in Parkinson’s disease: a pilot multicenter study of effects on nonmotor symptoms and quality of life. Mov Disord. 2009;24:1468–74.
Anang JB, Gagnon JF, Bertrand JA, Romenets SR, Latreille V, Panisset M, et al. Predictors of dementia in Parkinson disease: a prospective cohort study. Neurology. 2014;83:1253–60.
Gerlach OH, Winogrodzka A, Weber WE. Clinical problems in the hospitalized Parkinson’s disease patient: systematic review. Mov Disord. 2011;26:197–208.
Oguh O, Kwasny M, Carter J, Stell B, Simuni T. Caregiver strain in Parkinson’s disease: National Parkinson Foundation Quality Initiative Study. Parkinsonism Relat Disord. 2013;19:975–9.
Schrag A, Hovris A, Morley D, Quinn N, Jahanshahi M. Caregiver-burden in Parkinson’s disease is closely associated with psychiatric symptoms, falls, and disability. Parkinsonism Relat Disord. 2006;12:35–44.
Aarsland D, Brønnick K, Ehrt U, De Deyn PP, Tekin S, Emre M, et al. Neuropsychiatric symptoms in patients with Parkinson’s disease and dementia: frequency, profile and associated caregiver stress. J Neurol Neurosurg Psychiatry. 2007;78:36–42.
Santos-García D, de la Fuente-Fernández R. Factors contributing to caregivers’ stress and burden in Parkinson’s disease. Acta Neurol Scand. 2015;131:203–10.
Adler CH, Beach TG, Hentz JG, Shill HA, Caviness JN, Driver-Dunckley E, et al. Low clinical diagnostic accuracy of early vs advanced Parkinson disease: Clinicopathologic study. Neurology. 2014;83:406–12.
McGhee DJ, Royle PL, Thompson PA, Wright DE, Zajicek JP, Counsell CE. A systematic review of biomarkers for disease progression in Parkinson’s disease. BMC Neurol. 2013;13:35.
Sathe K, Maetzler W, Lang JD, Mounsey RB, Fleckenstein C, Martin HL, et al. S100B is increased in Parkinson’s disease and ablation protects against MPTP-induced toxicity through the RAGE and TNF-a pathway. Brain. 2012;135(Pt 11):3336–47.
Schaf DV, Tort AB, Fricke D, Schestatsky P, Portela LV, Souza DO, et al. S100B and NSE serum levels in patients with Parkinson’s disease. Parkinsonism Relat Disord. 2005;11:39–43.
Rothermundt M, Peters M, Prehn JH, Arolt V. S100B in brain damage and neurodegeneration. Microsc Res Tech. 2003;60:614–32.
Lindqvist D, Kaufman E, Brundin L, Hall S, Surova Y, Hansson O. Non-motor symptoms in patients with Parkinson’s disease - correlations with inflammatory cytokines in serum. PLoS One. 2012;7, e47387.
Nagatsu T, Mogi M, Ichinose H, Togari A. Changes in cytokines and neurotrophins in Parkinson’s disease. J Neural Transm Suppl. 2000;60:277–90.
Reale M, Iarlori C, Thomas A, Gambi D, Perfetti B, Di Nicola M, et al. Peripheral cytokines profile in Parkinson’s disease. Brain Behav Immun. 2009;23:55–63.
Dufek M, Hamanová M, Lokaj J, Goldemund D, Rektorová I, Michálková Z, et al. Serum inflammatory biomarkers in Parkinson’s disease. Parkinsonism Relat Disord. 2009;15:318–20.
Sawada H, Oeda T, Umemura A, Tomita S, Hayashi R, Kohsaka M, et al. Subclinical elevation of plasma C-reactive protein and illusions/hallucinations in subjects with Parkinson’s disease: case–control study. PLoS One. 2014;9, e85886.
Zhang L, Yan J, Xu Y, Long L, Zhu C, Chen X, et al. The combination of homocysteine and C-reactive protein predicts the outcomes of Chinese patients with Parkinson’s disease and vascular parkinsonism. PLoS One. 2011;6, e19333.
Madenci G, Bilen S, Arli B, Saka M, Ak F. Serum iron, vitamin B12 and folic acid levels in Parkinson’s disease. Neurochem Res. 2012;37:1436–41.
Rogers JD, Sánchez-Saffon A, Frol AB, Díaz-Arrastia R. Elevated plasma homocysteine levels in patients treated with levodopa: association with vascular disease. Arch Neurol. 2003;60:59–64.
Toth C, Breithaupt K, Ge S, Duan Y, Terris JM, Thiessen A, et al. Levodopa, methylmalonic acid, and neuropathy in idiopathic Parkinson’s disease. Ann Neurol. 2010;68:28–36.
Schwarzschild MA, Schwid SR, Marek K, Watts A, Lang AE, Oakes D, et al. Serum urate as a predictor of clinical and radiographic progression in Parkinson disease. Arch Neurol. 2008;65:716–23.
Farhoudi M, Taheraghdam A, Farid GA, Talebi M, Pashapou A, Majidi J, et al. Serum iron and ferritin level in idiopathic Parkinson’s disease. Park J Biol Sci. 2012;15:1094–7.
Lesage S, Brice A. Parkinson’s disease: from monogenic forms to genetic susceptibility factors. Hum Mol Genet. 2009;18(R1):R48–59.
Ibarretxe-Bilbao N, Junque C, Marti MJ, Tolosa E. Brain structural MRI correlates of cognitive dysfunctions in Parkinson’s disease. J Neurol Sci. 2011;310:70–4.
Lee JE, Cho KH, Song SK, Kim HJ, Lee HS, Sohn YH, et al. Exploratory analysis of neuropsychological and neuroanatomical correlates of progressive mild cognitive impairment in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2014;85:7–16.
Ziegler E, Rouillard M, André E, Coolen T, Stender J, Balteau E, et al. Mapping track density changes in nigrostriatal and extranigral pathways in Parkinson’s disease. Neuroimage. 2014;99:498–508.
Brück A, Kurki T, Kaasinen V, Vahlberg T, Rinne JO. Hippocampal and prefrontal atrophy in patients with early non-demented Parkinson’s disease is related to cognitive impairment. J Neurol Neurosurg Psychiatry. 2004;75:1467–9.
Goldman JG, Stebbins GT, Dinh V, Bernard B, Merkitch D, DeToledo-Morrell L, et al. Visuoperceptive region atrophy independent of cognitive status in patients with Parkinson’s disease with hallucinations. Brain. 2014;137:849–59.
Vercruysse S, Leunissen I, Vervoort G, Vandenberghe W, Swinnen S, Nieuwboer A. Microstructural changes in white matter associated with freezing of gait in Parkinson’s disease. Mov Disord. 2014;30:567–76.
Agosta F, Kostic VS, Davidovic K, Kresojević N, Sarro L, Svetel M, et al. White matter abnormalities in Parkinson’s disease patients with glucocerebrosidase gene mutations. Mov Disord. 2013;28:772–8.
Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. 2001;13:89–95.
Brooks DJ, Frey KA, Marek KL, Oakes D, Paty D, Prentice R, et al. Assessment of neuroimaging techniques as biomarkers of the progression of Parkinson’s disease. Exp Neurol. 2003;184 Suppl 1:68–79.
Katzenschlager R, Head J, Schrag A, Ben-Shlomo Y, Evans A, Lees AJ. Parkinson’s Disease Research Group of the United Kingdom. Fourteen-year final report of the randomized PDRG-UK trial comparing three initial treatments in PD. Neurology. 2008;71:474–80.
Hely MA, Morris JGL, Reid WGJ, Trafficante R. Sydney Multicentre Study of Parkinson’s disease: non-levodopa responsive problems dominate at 15 years. Mov Disord. 2005;20:190–9.
PD MED Collaborative Group. Long-term effectiveness of dopamine agonists and monoamine oxidase B inhibitors compared with levodopa as initial treatment for Parkinson’s disease (PD MED): a large, open-label, pragmatic randomised trial. Lancet. 2014;384:1196–205.
Zhu K, Van Hilten JJ, Marinus J. Predictors of dementia in Parkinson’s disease; findings from a 5-year prospective study using the SCOPA-COG. Parkinsonism Relat Disord. 2014;20:980–5.
Stewart T, Liu C, Ginghina C, Cain KC, Auinger P, Cholerton B, et al. Cerebrospinal fluid a-synuclein predicts cognitive decline in Parkinson disease progression in the DATATOP cohort. Am J Pathol. 2014;184:966–75.
Balzer-Geldsetzer M, Costa AS, Kronenbürger M, Schulz JB, Röske S, Spottke A, et al. Parkinson’s disease and dementia: a longitudinal study (DEMPARK). Neuroepidemiology. 2011;37:168–76.
Pedersen KF, Larsen JP, Tysnes OB, Alves G. Prognosis of mild cognitive impairment in early Parkinson disease: the Norwegian ParkWest study. JAMA Neurol. 2013;70:580–6.
Tsai ST, Hung HY, Hsieh TC, Lin SH, Lin SZ, Chen SY. Long-term outcome of young onset Parkinson’s disease after subthalamic stimulation-- a cross-sectional study. Clin Neurol Neurosurg. 2013;115:2082–7.
Merola A, Zibetti M, Angrisano S, Rizzi L, Ricchi V, Artusi CA, et al. Parkinson’s disease progression at 30 years: a study of subthalamic deep brain-stimulated patients. Brain. 2011;134:2074–84.
Hiorth YH, Larsen JP, Lode K, Pedersen KF. Natural history of falls in a population-based cohort of patients with Parkinson’s disease: An 8-year prospective study. Parkinsonism Relat Disord. 2014;20:1059–64.
Bugalho P, Viana-Baptista M. REM sleep behavior disorder and motor dysfunction in Parkinson’s disease--a longitudinal study. Parkinsonism Relat Disord. 2013;19:1084–7.
Williams-Gray CH, Mason SL, Evans JR, Foltynie T, Brayne C, Robbins TW, et al. The CamPaIGN study of Parkinson’s disease: 10-year outlook in an incident population-based cohort. J Neurol Neurosurg Psychiatry. 2013;84:1258–64.
Zhu K, Van Hilten JJ, Putter H, Marinus J. Risk factors for hallucinations in Parkinson’s disease: results from a large prospective cohort study. Mov Disord. 2013;28:755–62.
Clark AJ, Ritz B, Prescott E, Rod NH. Psychosocial risk factors, pre-motor symptoms and first-time hospitalization with Parkinson’s disease: a prospective cohort study. Eur J Neurol. 2013;20:1113–20.
Winder-Rhodes SE, Evans JR, Ban M, Mason SL, Williams-Gray CH, Foltynie T, et al. Glucocerebrosidase mutations influence the natural history of Parkinson’s disease in a community-based incident cohort. Brain. 2013;136:392–9.
Kasten M, Hagenah J, Graf J, Lorwin A, Vollstedt EJ, Peters E, et al. Cohort Profile: a population-based cohort to study non-motor symptoms in parkinsonism (EPIPARK). Int J Epidemiol. 2013;42:128–128k.
Auyeung M, Tsoi TH, Mok V, Cheung CM, Lee CN, Li R, et al. Ten year survival and outcomes in a prospective cohort of new onset Chinese Parkinson’s disease patients. J Neurol Neurosurg Psychiatry. 2012;83:607–11.
Chen YY, Cheng PY, Wu SL, Lai CH. Parkinson’s disease and risk of hip fracture: an 8-year follow-up study in Taiwan. Parkinsonism Relat Disord. 2012;18:506–9.
Velseboer DC, Broeders M, Post B, Van Geloven N, Speelman JD, Schmand B, et al. Prognostic factors of motor impairment, disability, and quality of life in newly diagnosed PD. Neurology. 2013;80:627–33.
Initiative PPM. The Parkinson Progression Marker Initiative (PPMI). Prog Neurobiol. 2011;95:629–35.
Paulsen JS, Long JD, Johnson HJ, Aylward EH, Ross CA, Williams JK, et al. Clinical and Biomarker Changes in Premanifest Huntington Disease Show Trial Feasibility: A Decade of the PREDICT-HD Study. Front Aging Neurosci. 2014;6:78.
Grupo ELEP. A longitudinal study of patients with Parkinson´s disease (ELEP): aims and methodology. Rev Neurol 2006;42:360–5.
Ford B. Pain in Parkinson’s disease. Mov Disord. 2010;25 Suppl 1:98–103.
Marsh L, McDonald WM, Cummings J, Ravina B, NINDS/NIMH Work Group on Depression and Parkinson’s Disease. Provisional diagnostic criteria for depression in Parkinson’s disease: report of an NINDS/NIMH Work Group. Mov Disord. 2006;21:148–58.
Judd LL, Rapaport MH, Paulus MP, Brown JL. Subsyndromal symptomatic depression: a new mood disorder? J Clin Psychiatry. 1994;55(Suppl):18–28.
Jankovic J, McDermott M, Carter J, Gauthier S, Goetz C, Golbe L, et al. Variable expression of Parkinson’s disease: a base-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology. 1990;40:1529–34.
Stebbins GT, Goetz CG, Burn DJ, Jankovic J, Khoo TK, Tilley BC. How to identify tremor dominant and postural instability/gait difficulty groups with the movement disorder society unified Parkinson’s disease rating scale: comparison with the unified Parkinson’s disease rating scale. Mov Disord. 2013;28:668–70.
Cubo E, Martín PM, Martin-Gonzalez JA, Rodríguez-Blázquez C, Kulisevsky J, ELEP Group Members. Motor laterality asymmetry and nonmotor symptoms in Parkinson’s disease. Mov Disord. 2010;25:70–5.
Acknowledgments
We would like the thank all patients, caregivers and all persons, companies or institutions collaborating in this project.
We would also like to thank Marie Cheeseman who provided English editing services on behalf of Springer Healthcare Communications.
COPPADIS Study group (collaborators)
de Deus Fonticoba T1, de Fábregues-Boixar O2, Hernández Vara J2, Borrue C3, Aguilar M4, Tijero B5, Chacón J6, Seijo M7, Cabo I7, Puente V8, Legarda I9, Carrillo Padilla F10, López Manzanares L11, Valero C12, Pagonabarraga J13, García-Moreno JM14, Galeano B15, Caballol N16, Gastón Zubimendi MI17, Sánchez Alonso P18, Catalán MJ19, López Díaz LM20, Alonso Losada MG21, López Ariztegui N22, Kurtis M23, Sierra M24, Escalante S25, Martínez Castrillo JC26, Ribacoba R27, González Ardura J28, López del Val J29, Ávila MA30, Alonso-Navarro H31, Solano B32, García Caldentey J33, Rojo A34, Martí Martínez S35, Domínguez Morán JA36, Martínez Torres I37, Álvarez Sauco MA38, Prieto Jurczynska C39, Menéndez González M27,40, Carrillo-García F41, Jesús S41, Cáceres MT41, Oropesa JM41, Gómez-Garre MP41, Huertas I41, Vargas L41, Mariscal N42, Macías Y43, Ruíz Martínez J44, Delgado M44, Mondragón E44, Barandiarán M44, Malo R45, Planella L46, Cámara A46, Martí G2, Mata M3, Pastor P4, Quílez P4, Badenes D4, Casas L4, Arribas S4, Romero S4, Tomé G4, Comes L4, Guardia G4, López J4, Gómez Esteban JC5, Berganzo K5, González A5, Acera M5, Rodríguez Bóveda I5, Álvarez López M6, Fernández-Espejo E6,47, Vives B9, Pueyo M10, de Toledo M11, Sobrado M11, González García B11, Bosca M12, Salazar C12, Campos A12, Pascual B13, Damas F14, Pacheco E14, Merino R15, Clavero P17, Erró E17, Lacruz F17, Cabello C17, Díez Álvarez M18, Montero P19, Villanueva C19, Meitín T20, Murcia S22, Clemente J22, Sánchez P23, González Aramburu I24, Esteve P25, Reverté S25, Alonso A26, Avilés I26, Suárez E27, Sánchez P27, Guijarro M28, Bellosta E29, López García E29, Jiménez-Jiménez FJ31, Coll C32, Montserrat M32, Ferriol MM33, Finally, this author will not participate in the study., Leiva C35, Hernández L35, López Pesquera P36, Luca L36, Rubio I37, Satre I37, Freire E38, Ordás C39, Torres G39, Cazorla R39, Vengas B39, López Seoane B48, Faraldo A48, Fernández Guillán N48, Moreno Diéguez A48, Lage Castro M49, Vázquez Gómez R49. A48.
1Sección de Neurología, Hospital Arquitecto Marcide, Complexo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña; 2Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital Universitario Vall d’Hebron, Barcelona; 3Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital Infanta Sofía, Madrid; 4Unidad de Trastornos del Movimiento, Hospital Universitario Mutua de Terrasa, Terrasa, Barcelona; 5Unidad de Neurología Funcional y Enfermedad de Parkinson, Hospital de Cruces, Bilbao; 6Unidad de Neurología, Hospital Infanta Luisa, Sevilla; 7Servicio de Neurología, Complejo Hospitalario de Pontevedra (CHOP), Pontevedra; 8Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital del Mar, Barcelona; 9Servicio de Neurología, Hospital Universitario Son Espases, Palma de Mallorca; 10Servicio de Neurología, Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife; 11Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital La Princesa, Madrid; 12Unidad de Neurología, Hospital Arnau de Vilanova, Valencia; 13Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital de Sant Pau, Barcelona; 14Unidad de Trastornos del Movimiento, Hospital Universitario Virgen Macarena, Sevilla; 15Sección de Neurología, Hospital Universitario de Ceuta, Ceuta; 16Unidad de Trastornos del Movimiento, Consorci Sanitari Integral, Hospital Moisés Broggi, Sant Joan Despí, Barcelona; 17Unidad de Trastornos del Movimiento, Servicio de Neurología, Complejo Hospitalario de Navarra; 18Servicio de Neurología, Hospital Puerta de Hierro, Madrid; 19Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital Clínico San Carlos; 20Sección de Neurología, Hospital da Costa Burela, Burela, Lugo; 21Servicio de Neurología, Hospital Meixoeiro, Complejo Hospitalario Universitario de Vigo (CHUVI), Vigo; 22Unidad de Trastornos del Movimiento, Complejo Hospitalario de Toledo, Toledo; 23Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital Ruber Internacional, Madrid; 24Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital Universitario Marqués de Valdecilla, Santander; 25Servicio de Neurología, Hospital de Tortosa Verge de la Cinta (HTVC), Tortosa, Tarragona; 26Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital Ramón y Cajal, Madrid; 27Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital Central de Asturias; 28Servicio de Neurología, Hospital Universitario Lucus Augusti (HULA), Lugo; 29Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital Clínico Universitario Lozano Blesa, Zaragoza; 30Unidad de Trastornos del Movimiento, Consorci Sanitari Integral, Hospital General de L’Hospitalet, L’Hospitalet de Llobregat, Barcelona; 31Sección de Neurología, Hospital Universitario del Sureste, Arganda del Rey, Madrid; 32Servicio Assistencial de Neurologia Institut Català de la Salut (ICS)- Insitut d’Assistència Sanitària, Girona; 33Unidad de Neurología, Centro Neurológico OMS 42, Palma de Mallorca; 34Unidad de Parkinson y Movimientos Anormales, Servicio de Neurología, Hospital Universitario Príncipe de Asturias, Madrid; 35Servicio de Neurología, Hospital General de Alicante, Alicante; 36Unidad de Neurología, Hospital de la Rivera, Alcira, Valencia; 37Unidad de Trastornos del Movimiento, Servicio de Neurología, Hospital La Fe; 38Servicio de Neurología, Hospital General Universitario de Elche, Elche; 39Unidad de Trastornos del Movimiento, Hospital Infanta Elena-Hospital Rey Juan Carlos-Hospital Collado Villalba, Madrid; 40Unidad de Neurología, Hospital Álvarez-Buylla, Mieres, Asturias; 41Unidad de Trastornos del Movimiento, Servicio de Neurología y Neurofisiología Clínica, Instituto de Biomedicina de Sevilla, Hospital Universitario Virgen del Rocío, CSIC y Universidad de Sevilla; 42Servicio de Neurología, Hospital Universitario de Burgos; 43Unidad de Neurología, Fundación Hospital de Alcorcón, Madrid; 44Hospital Universitario Donostia, Instituto de Investigación Biodonostia, San Sebastián; 45Unidad de Trastornos del Movimiento y enfermedad de Parkinson, Servicio de Neurología, Hospital Universitario Insular de Gran Canaria, Las Palmas de Gran Canaria; 46Unidad de Parkinson y Trastornos del Movimiento, Servicio de Neurología, Instituto Clínico de Neurociencias, Hospital Clínic, Barcelona; 47Departamento de Fisiología Médica y Biofísica de la Facultad de Medicina de Sevilla, Universidad de Sevilla; 48Hospital General Juan Cardona, Servicio de Radiología, Ferrol, A Coruña; 49Servicio de Psiquiatría, Complejo Hospitalario de Pontevedra (CHOP), Pontevedra.
This study was presented in abstract form at the 19TH International Congress of Parkinson’s Disease and Movement Disorders held in San Diego (CA, USA, 14–18 June, 2015).
Funding
The project funding is both public and private. There will be an ambitious campaign (COPPADIS Social Project; www.coppadis.com and curemoselparkinson.org) designed to have a huge social impact, developed under a clear and unique concept to engage society.
Funding sources
ABBVIE, ACEBRE, ALTER, ASOCIACIÓN PARKINSON ARAGON, ASOCIACIÓN PARKINSON PALENCIA, ASOCIACIÓN PARKINSON VALENCIA, AYUNTAMIENTO DE A CORUÑA, CLIMANOSA, CONSTRUDECO NORTE, FEDERACION GALLEGA ATLETISMO, ESTEVE, LUNDBECK, QUALIGEN, UCB PHARMA, VALENCIA CONCIERGE, VIAJES GALITUR, ZAMBON and many individual donors.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
Financial competing interests (for the preceding twelve months)
Diego Santos-García has received honoraria for educational presentations by Abbvie, UCB Pharma and Lundbeck. Pablo Mir has received honoraria for lecturing or advisory boards from AbbVie, UCB, Zambon, Allergan and Merz, and research grants from the Ministerio de Economía y Competitividad de España [SAF2007-60700], the Instituto de Salud Carlos III [PI10/01674, CP08/00174, PI13/01461], the Consejería de Economía, Innovación, Ciencia y Empleo de la Junta de Andalucía [CVI-02526, CTS-7685], the Consejería de Salud y Bienestar Social de la Junta de Andalucía [PI-0377/2007, PI-0741/2010, PI-0437-2012], the Sociedad Andaluza de Neurología, the Jacques and Gloria Gossweiler Foundation and the Fundación Alicia Koplowitz. Esther Cubo has received travel funding from Abbvie, Allergan and UCB Pharmaceuticals, and received research support from the Movement Disorder Society, World Federation of Neurology and Junta de Castilla y León. Lydia Vela has received honoraria for educational presentations by Abbvie, UCB Pharma and Lundbeck. Maria C Rodriguez-Oroz has received payment for lectures, travel and accommodation to attend scientific meetings from UCB, Lundbeck, Abbvie and Boston Scientific. She has received grants from CIBERNED, Government of Basque Country and Guipuzcoa, Spanish Health Institute and Era-net. Maria J Marti has received speaking fees from Ipsen, Merz, Allergan and UCB Pharma and research grants from Ministery of Health and Social Services, Marató TV3, Centro Investigacion Biomedica en Red and Michael J Fox Foundation for Parkinson’s research. Jose M Arbelo has received honoraria for educational presentations or clinical studies participation by Abbvie, UCB Pharma and Italfarmaco. Jon Infante has received honoraria as a speaker from UCB Pharma and traveling grants from Abbvie. Jaime Kulisevsky has received honoraria for lecturing or advisoring from Abbvie, UCB and Zambon. Pablo Martínez-Martin has received honorarium from Abbvie for a symposium and participation in the Advisory Board for an epidemiological study, Editorial Viguera for a master course, UCB for lecturing in International University Menendez Pelayo summer course.
Authors’ contributions
DS, MD PhD conception, organization, and execution of the project; writing of the first draft of the manuscript. PM, MD PhD participation in the consensus protocol; review and critique of this manuscript. EC, MD PhD participation in the consensus protocol; review and critique of this manuscript. LV, MD PhD participation in the consensus protocol; review and critique of this manuscript. MCR, MD PhD participation in the consensus protocol; review and critique of this manuscript. MJM, MD PhD participation in the consensus protocol; review and critique of this manuscript. JMA, MD PhD participation in the consensus protocol; review and critique of this manuscript. JI, MD PhD review and critique of this manuscript. JK, MD PhD review and critique of this manuscript. PM, MD PhD review and critique of this manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Santos-García, D., Mir, P., Cubo, E. et al. COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015), a global –clinical evaluations, serum biomarkers, genetic studies and neuroimaging– prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurol 16, 26 (2016). https://doi.org/10.1186/s12883-016-0548-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-016-0548-9