
Abstract
Background
Chronic kidney disease (CKD) affects 8 to 16% of the world’s population and is one of the top ten important drivers of increasing disease burden. Apart from genetic predisposition, lifestyle factors greatly contribute to the incidence and progression of CKD. The current bibliometric analysis aims to characterize the current focus and emerging trends of the research about the impact of modifiable lifestyle factors on CKD.
Methods
We searched articles addressing the impact of modifiable lifestyle factors on the incidence and/or progression of CKD, published between 2011 and 2020, from the Science Citation Index Expanded (SCIE) database. An adjusted citation index, which considered both the original citation count and publication year, was derived for the selection of most-cited publications. Publishing trends, co-authorship network, keywords, and research hotspots were analyzed and visualized.
Results
Among the top 100 most influential articles, 32 were narrative reviews, 16 systematic reviews and/or meta-analysis, 44 clinical research, and 8 basic research. The United States occupied a dominant position in the perspective of article numbers and international partnerships, followed by European countries. The modifiable factors that drew the most and constant attention over the decade were diet or nutrition management reported in 63 papers, followed by obesity or body mass index (n = 27), and physical activity or exercises (n = 8). Alcohol consumption, fish oil, chain fatty-acids, and water-soluble vitamins were emerging hotspots identified in the recent most cited publications.
Conclusions
Based on the bibliometric analysis of the most influential articles, our study provides a comprehensive description of publishing trends and research focus over a decade in the field of lifestyle factors’ impact on CKD. Diet, obesity, and physical activity were factors receiving the most attention in this topic.
Similar content being viewed by others

Background
Chronic kidney disease (CKD), defined as abnormalities of kidney structure or function presenting for >3 months with health implications [1], affects 8–16% of the world’s population [2]. CKD is closely associated with an increased risk of adverse events, including end-stage renal disease (ESRD), cardiovascular events, hospitalizations, and mortality [3,4,5,6,7]. The global all-age mortality rate from CKD increased by 41.5% from 1990 to 2017 [8]. It is currently ranking the 16th leading cause of years of life lost [2] and is projected to rise in the ranking, to the 5th, by 2040 [9].
CKD imposes great burdens in both developed and developing countries. For example, Medicare expenditures for ESRD in the United States (the US) increased by about 20.3% from 2009 to 2018 and accounted for 7.2% of overall Medicare fee-for-service spending in 2018 [10]. The burden of CKD is even more pronounced in low- and lower-middle-income countries [11]. In several regions, particularly Oceania, sub-Saharan Africa, and Latin America, the burden of CKD is much higher than expected for the level of development [8]. Thus, it is considered to be one of the top ten important drivers of increasing burden according to the latest analysis for the Global Burden of Disease Study [12].
CKD is affected by both genetic and environmental factors [13]. While modification of the genetic predisposition for CKD is quite challenging, evidence shows that the incidence and rapid progression of CKD can be protected via modifiable lifestyle factors, ie. diet, physical activity, alcohol consumption, tobacco smoking, sleep, and obesity [14,15,16,17,18]. Recently, growing literature has addressed the underlying mechanism and the health impact of modifiable factors on CKD. However, to our knowledge, there have been no bibliometric analyses on this topic.
Bibliometric analysis is a valuable tool for navigation in a particular research area [19, 20]. It has been used to provide qualitative and quantitative analysis of publications, enabling researchers to identify core articles, study hotspots, and publishing patterns within a given subject area [21]. Thus, bibliometric analysis is an integral part of the evaluation methodology for assessment of the research evolution and current development stage of the discipline [19, 22]. In this study, based on bibliometric analysis of the top-cited articles, we aim to elucidate the current focus, growing trends, and future direction of the research about the impact of modifiable factors on CKD.
Methods
Search strategy
We aimed to analyze the most influential publications within the last ten years. Inclusion criteria were (1) original articles or reviews which addressed the impact of modifiable lifestyles, ie. diet (including foods, nutrients, and dietary patterns), physical activity, alcohol consumption, smoking, sleep, and obesity, on the incidence and/or progression of CKD; (2) published between January 2011 to December 2020; (3) with restriction of language of English. The Science Citation Index Expanded database (SCIE) of Web of Science, which includes multidisciplinary bibliographic information and is now regarded as one of the collections of the highest impact, most influential international and regional journals [23, 24], was searched for the inclusion of publications. A comprehensive search strategy was performed to identify the intersect of search terms describing CKD and modifiable lifestyles, being limited to the field of “Topic”. Other document types, such as meeting abstracts, letters, and corrections, were excluded. The detailed search terms were listed in Table S1.
Study selection and data collection
Considering papers that were published earlier had innately higher opportunities to be cited than those published later, to ensure recently published influential papers also be included for analysis, we derived an adjusted citation index, which was defined as the mean number of citations per year, calculated by the equation: adjusted citation index = total cited count / (2021- publication year), to evaluate the publications for inclusion.
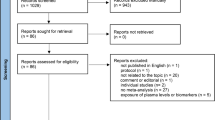
Among the original 20,157 records obtained via the above-mentioned search strategy, to facilitate the following study selection process, we firstly excluded studies after the 300th rank each year in descending order of total citation count. Next, for the 3000 remaining studies for further evaluation, the abstracts, as well as full texts when necessary, were thoroughly reviewed by investigators (YT and HY) independently to exclude ineligible studies. Any disagreement was resolved through discussion with another viewer (XZ). Finally, the top 100-cited articles according to the adjusted citation index were included in our bibliometric analysis. The information of titles, authors, institutions, abstracts, countries, publication years, journals, total citation number of the article, document types, author keywords and keywords plus, and research areas of these publications, were downloaded on 6 August 2021. The selection process of the articles was shown in Fig. 1.

Flow diagram of the article selection process used in the study
Bibliometric analysis
We read the abstract or full text of each article and classified the research into clinical research, basic research, review, and meta-analysis. We used ‘bibliometrix’ package in R software (version 3.6.3) to analyze the bibliographic information [25]. The country of origin of the articles was defined according to the corresponding author. H-index was used to evaluate scholars’ scientific output based on their published articles and citations. The value of H-index is equal to the number of papers (N) of a researcher that has been cited by others at least N times [26]. The annual percentage growth rate was calculated by ‘biblioAnalysis’ function in R software to describe the annual change in the scientific production.
VOSviewer software (version 1.6.16) [27] was used to visualize the co-authorship network and analyze keywords. The link in the co-authorship network represented authors’ collaborations and bigger nodes indicated more publications of the authors [28].
For keyword analysis, we extracted both the original keywords provided by the authors and the keywords plus, which were words or phrases that frequently appeared in the titles of an article’s references but did not appear in the title of the article itself. For articles that did not provide author keywords, keywords plus were used instead, since keywords plus were considered to be as effective as author keywords when investigating the knowledge structure of scientific fields [29]. We merged some synonym keywords and unified keywords with the same meaning (Table S2) [30]. For example, “chronic kidney disease”, “chronic renal insufficiency”, and “CKD” were merged into “chronic kidney disease”. We derived a word cloud to visualize the word significance, the dimensions of each word representing the frequency of occurrences in publications [31]. The keyword co-occurrence network, in which an edge between two nodes representing the co-occurrence of two words, was derived to reflect the research hotspots in the discipline fields. Bigger nodes represent higher importance of items. A shorter distance indicates stronger relation between nodes. The thicker of the line represents more co-occurrence between two keywords [32].
Results
Research areas, publishing trends, and citation index
Among the top 100 most influential articles, 32 were narrative reviews, 16 systematic reviews and/or meta-analysis, 44 clinical research, and 8 basic research. The modifiable factors that drew the most attention were diet or nutrition management in 63 papers, including plant-based diets, dietary sodium restriction, Mediterranean diet, dietary cadmium intake, red meat, high dietary acid load, high protein diet, among others, followed by obesity or body mass index (BMI; n = 27), and physical activity or exercises (n = 8). Other factors being investigated that obtain high citations included smoking, alcohol consumption, and lipid. The outcomes of interest were the risk of the incidence and progression of CKD, including, in three articles, kidney transplantation, as well as the management and prevention of adverse outcomes associated with CKD. Based on original information on research areas retrieved from the SCIE database, 65 papers were classified into urology and nephrology, 16 in nutrition dietetics, 10 in general internal medicine, 10 in transplantation, and 7 in endocrinology metabolism. The characteristics and methodology of the included top 20 and top 100-cited articles, and summarized authors’ views on the impact of modifiable lifestyles on CKD were listed in Table 1 and Table S3 respectively, ordered by descending adjusted citation index.
Despite minor recessions in certain years, the trend analysis demonstrated an annual growth rate of 4.6% in the number of publications across the decade and climbed to the peak in 2019 (n = 15; Fig. 2). The H-index was 60 of the retrieved articles. The original citation number of these articles ranged from 12 to 436, with an average citation number of 87.2 per paper. Among the included 48 narrative and systematic reviews/meta-analysis, 28 cited other top highly-cited articles listed in this study, but no duplicated publications were identified. The top three articles receiving the highest citation included one study investigating the interaction between obesity-induced hypertension with neurohumoral and renal mechanisms [33], a review on the association between obesity, oxidative stress, adipose tissue dysfunction, and health risks, including CKD [34], both published in 2015, and a study on the association between dietary sodium intake, ESRD, and mortality in diabetic patients published in 2011 [35]. If adjusted citation index was considered, in the latest three years, the most influential papers were three reviews addressing the impact of obesity and diet nutrition on CKD [36,37,38].

Annual publication numbers and citations per article by year
Journals, authors, and their countries and institutions
The top 100-cited articles were published in 40 journals, with 2020 impact factor (IF) ranging between 3.655 to 39.890. The four journals with the most publications were Journal of the American Society of Nephrology (n = 12; IF = 10.121), American Journal of Kidney Diseases (n = 12; IF = 8.860), and Kidney International (n = 9; IF = 10.612) based in the US, and Nephrology Dialysis Transplantation (n = 9; IF = 5.992) based in Europe (Fig. 3). The primary corresponding authors of the top 100-cited articles were from 37 countries. Table 2 and Table 3 list the corresponding authors’ countries who contributed to more than two articles and institutions that contributed more than five articles. The US occupied a dominant position in the perspective of article numbers and international partnerships (Fig. 4). Johns Hopkins University in the US was identified as the most productive institution for the highly-cited papers on this topic (n = 12), followed by University of California Irvine in the US (n = 11), and Karolinska Institute in Sweden (n = 8).

Journals that contribute 2 articles or more to the top 100-cited papers and journal impact factor in 2020. IF, impact factor; Am J Nephrol, American Journal of Nephrology; Clin Nutr, Clinical Nutrition; Cochrane Database Syst Rev., Cochrane Database of Systematic Reviews; Lancet Diabetes Endocrinol, Lancet Diabetes & Endocrinology; Nat Rev. Nephrol, Nature Reviews Nephrology; J Renal Nutr, Journal of Renal Nutrition; Clin J Am Soc Nephrol, Clinical Journal of the American Society of Nephrology; Kidney Int, Kidney International; Nephrol Dial Transplant, Nephrology Dialysis Transplantation; Am J Kidney Dis, American Journal of Kidney Diseases; J Am Soc Nephrol, Journal of the American Society of Nephrology

The cooperation relationships of countries that published the top 100-cited articles. The US, the United States; NLD, Netherlands; GBR, the United Kingdom; CHE, Switzerland; NZL, New Zealand; ARE, United Arab Emirates
A total of 591 authors contributed to the top 100-cited articles. The top ten researchers contributing to the field are listed in Table 4 based on their number of publications, and Fig. 5 shows the co-authorship network of authors who contributed at least two papers in the top 100-cited articles. The most productive author was, in the US, Kalantar-Zadeh, Kamyar based in University of California Irvine with active collaboration with other scholars, and outside the US, Campbell, Katrina L. based in Princess Alexandra Hospital, Brisbane, Australia. The above-mentioned information of authors’ institutions was based on their publications in 2020.

Network visualization map of the co-authorship network for authors in top 100-cited articles
Keywords and research focus
There were 254 keywords provided by original authors and 494 keywords plus in the top 100-cited articles. Analysis was mainly based on author keywords, except 37 papers in which author keywords were not provided and keywords plus were used instead. The top five keywords with the most frequent occurrence were obesity, diet, blood pressure, BMI, and hypertension; and the top five keywords reflecting outcomes were CKD, glomerular filtration rate, mortality, cardiovascular risk, and dialysis (Fig. S1). Generally, we found diet modification, physical activity, or moderate alcohol consumption was associated with a protective role for the incidence and progression of CKD and its related complications, while obesity or smoking was associated with increased risk for the above-mentioned outcomes (Table S3). Figure 6 presents a co-occurrence network of keywords being listed in at least two papers. They were classified into four clusters, which we assumed to reflect research themes. The leading keywords in the yellow cluster were CKD, dialysis, blood pressure, and hypertension, indicating the focus was mainly on the relationship between blood pressure and CKD, including dialysis. The leading keywords in the red cluster were glomerular filtration rate, cardiovascular risk, proteinuria, kidney disease, association, and progression. The keywords related to lifestyles included dietary protein restriction, low-protein diet, and red meat. We supposed the research focus of the red cluster lied in the impact of protein intake on CKD, especially on kidney function and cardiovascular comorbidities. Leading keywords in the green cluster included mortality, ESRD, kidney transplantation, obesity, BMI, physical activity, and metabolic syndrome. Smoking was also included in the group. Therefore, we assumed the cluster as a group referring to the relation between obesity, physical activities, smoking with the advanced CKD, and adverse outcomes. The leading keyword in the blue cluster was diet, followed by nutrition, vegetarian, protein-intake, disease progression, kidney, gut microbiota, and kidney function. This was considered a concrete cluster that discussed diet and CKD progression.

Network visualization map of the keyword co-occurrence network
In addition, we visualized keywords according to the average publication year to evaluate the trends in the research focus over time. As shown in Fig. 7, the color of the nodes, from purple, blue, green to yellow, corresponds to the earliest to most recent keywords that were used in the publications [39], reflecting which keywords have become popular in recent years and indicating the trend of future hotspots [40]. The nodes for some keywords, ie. dietary sodium, water, and salt were small and colored in purple, indicating these were research topics gaining more popularity a few years ago. Keywords with highly frequent occurrences, such as CKD, physical activity, obesity, diet, nutrition, glomerular filtration rate, progression, mortality, blood pressure, cardiovascular risk, and ESRD were colored in green, we considered these were research topics receiving consistent attention over the decade. We noticed a trend of increasing attention on the gut-kidney axis in the field over 2014 to 2019, with four most-cited papers published [41,42,43,44]. Alcohol consumption, fish oil, chain fatty-acids, and water-soluble vitamins, colored in yellow, appeared in 2020 for the first time, indicating the recently emerging research hotspots. Among the newly emerging keywords colored in yellow, words related to diet accounted for a considerable portion.

Overlay visualization map of keywords according to the average publication time
Discussion
In this study, we used bibliometric analysis to identify and characterize the top 100-cited articles published between 2011 and 2020 in the field of lifestyle factors’ impact on CKD. Our study provides legible insights on the publishing trends and research themes on the topic. We found about two-thirds of the most cited papers addressing the association between modifiable factors and CKD were clinical research, while basic studies only accounted for a small fraction. Developed countries, especially the US, showed overwhelming influence in this field in terms of the number of top-cited publications. We also noticed the transition of research hotspots over the decade, with diet, nutrition, obesity, and physical activity being the factors constantly drawing attention, and alcohol consumption, gut-kidney axis, fish oil, chain fatty-acids, molecular-weight protein, and water-soluble vitamins being among the newly emerging keywords.
Our finding, that the modifiable factors gaining most popularity were diet or nutritional management, is consistent with the fact that diet contributes substantially to the incidence and progression of CKD, and stays focused in the academic community. Recommendations on protein and sodium intake have been incorporated into guidelines for clinical management of CKD, such as the Kidney Disease: Improving Global Outcomes guideline [1], National Institute for Health and Care Excellence guideline [45], and National Kidney Foundation Kidney Disease Outcomes Quality Initiative guideline [46]. However, as Suetonia C Palmer pointed out, current evidence for dietary interventions in the setting of CKD, with clinical uncertainty, is yet sufficient to guide comprehensive clinical practice [47]. For instance, there are very limited data available evaluating potential adverse effects and participants’ quality of life related to dietary protein restriction [48]. Thus, as indicated in our study, the impact of diet and nutrition on CKD remains an important research topic, and further studies to evaluate the effects of nutritional interventions in the general population for the prevention of incident CKD and in CKD participants for slowing the progression to ESRD are required [48].
Our study showed obesity and health-related behaviors, such as physical activity and smoking, were among the research hotspots of modifiable factors. This evidence supports the inclusion of advice on physical activity, healthy weight, and smoking cessation into CKD management guidelines [1]. This reflects the attention from the field of nephrology on the influence of emerging obesity issues and unhealthy behavioral factors on health outcomes. Both obesity and sedentary lifestyle have become major driving forces for global disease burdens [49,50,51]. Their associations with CKD are investigated intensely by scholars. For example, in the top-cited articles included in the study, obesity is associated with increased CKD risk, and obese or overweight CKD patients are suggested to maintain a healthy weight and lifestyle [14]. A study evaluated the risk of ESRD associated with obesity at the time of donation among live kidney donors and found that obese live kidney donors have a significant 86% increased risk of ESRD compared to non-obese donors [52]. Regular physical activity instead of sedentariness can reduce the risk and mortality of CKD in type 2 diabetes [53]. A randomized clinical trial found that dietary calorie restriction and aerobic exercise can improve the metabolic milieu in patients with moderate to severe CKD [54]. Besides, a low-intensity exercise program may improve physical performance and quality of life in dialysis patients [55]. Studies suggest that cigarette smoking is an independent risk factor for incident CKD [56, 57], and nonsmoking is associated with a lower risk of adverse outcomes in CKD patients [58] and all-cause mortality [59].
It is interesting to investigate the evolution of research hotspots over time. For example, water intake and dietary sodium were factors receiving high citation years ago. A cross-sectional analysis of the National Health and Nutrition Examination Survey found that higher total water intake, particularly plain water, has a protective effect on CKD [60]. Julie Lin had analyzed longitudinal cohort data to fill the research vacancy of the influence of sodium intake on microalbuminuria and estimated glomerular filtration rate decline and found that less sodium intake can reduce the risk for estimated glomerular filtration rate decline [61]. Besides, dietary salt restriction is essential in patients with CKD and hypertension [62]. Nowadays, alcohol consumption, gut-kidney axis, fish oil, chain fatty-acids, and water-soluble vitamins have drawn more attention. Consuming a low or moderate amount of alcohol may lower the risk of developing CKD [63]. Gut microbiota dysbiosis induces gut-derived uremic toxins formation and is associated with CKD progression [64]. A recent study finds that omega-3 polyunsaturated fatty acids supplementation, such as fish oil can reduce cardiovascular mortality in patients on hemodialysis [65]. Short-chain fatty acids, being derived from fiber-rich diets [42], can delay CKD progression [66]. Vitamin K deficiency in patients on dialysis is associated with vascular calcification, bleeding risk, and cardiovascular disease [67]. Diet modification has been receiving persistent attention from scholars as most newly emerging keywords were related to diet. More research is needed to determine the optimal dietary patterns to prevent kidney disease and its progression [68]. Meanwhile, we noticed, certain research hotspot in other academic fields has not drawn as much attention in nephrology yet. For example, sleep, one of the important modifiable lifestyle factors, which was reported to be associated with a wide range of diseases [69], including CKD [18, 70, 71], was not found in the top 100-cited list. The low citation might be caused by the most recent publication time not allowing the papers to be fully cited, or might indicate not so many scholars were dedicated to the research of sleep and its relation to CKD. Lifestyle modification of sleep in CKD patients requires more attention.
The results showed the US was the most productive country on the current topic and with the most active international partnership. Journal of the American Society of Nephrology, American Journal of Kidney Diseases, Kidney International based in the US, and Nephrology Dialysis Transplantation based in Europe were the four journals with the most publications, indicating the US and European were pilots in the research field about the impact of modifiable factors on CKD; while developing countries were not active in producing highly influential research. The disparity of the quantity of academic publications between developing and developed world has long been recognized, which might be attributed to multifaced causes, to name a few, lacking of research capacity in developing countries [72], funding and principal investigator status owned by developed world [73], language and writing barriers, and editorial bias [74]. Considering the disease burden of CKD in developing countries are rising and might be more pronounced than that in developed countries, high-quality research about the impact of modifiable factors on CKD conducted in population from less developed regions, and more cooperations between developed countries and developing countries are required, such that the evidence can be disseminated to these population more precisely.
Our study has many strengths. To our knowledge, this is the first bibliometric analysis of the relationship between modifiable lifestyles and CKD. Our study finds the evolution of hot topics over the decade and provides clues for scholars to choose research themes. However, there are some limitations of our study. First, only English literature was included in the study, so we may fail to capture some landmark articles published in other languages. Second, all data were extracted from the SCIE of Web of Science, thus, we may fail to capture certain related publications provided in other sources. Third, despite we analyzed the top-cited articles in this field representing the research hotspots, we admit certain research topics with few publications due to publication bias [75], may be missed. In addition, ‘obliteration by incorporation’, which represents that the older publications are no longer cited because their findings are common-use and incorporated into the current discipline, is a notable concern in the bibliometric analysis [76]. Thus, we included publications within the last ten years and ranked articles based on an adjusted citation index rather than the number of citations received in the current year.
Conclusions
In summary, in the bibliometric analysis of the top 100-cited articles addressing the influence of modifiable factors on CKD, our study provides a comprehensive description of publishing trends and research focus over a decade. The association between modifiable factors and CKD has been among the research focus over the decade. While the study hotspots are evolving over time, diet, obesity, and physical activity were factors receiving the most attention in this topic.
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Abbreviations
- CKD:
-
Chronic kidney disease
- ESRD:
-
End-stage renal disease
- The US:
-
The United States
- SCIE:
-
Science Citation Index Expanded database
- IF:
-
Impact factor
References
Levin A, Stevens PE, Bilous RW, Coresh J, De Francisco ALM, De Jong PE, et al. Kidney disease: Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1):1–150.
Chen TK, Knicely DH, Grams ME. Chronic Kidney Disease Diagnosis and Management: A Review. Jama-J Am Med Assoc. 2019;322(13):1294–304.
Herzog CA, Asinger RW, Berger AK, Charytan DM, Diez J, Hart RG, et al. Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2011;80(6):572–86.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–305.
Lees JS, Welsh CE, Celis-Morales CA, Mackay D, Lewsey J, Gray SR, et al. Glomerular filtration rate by differing measures, albuminuria and prediction of cardiovascular disease, mortality and end-stage kidney disease. Nat Med. 2019;25(11):1753–60.
Chronic Kidney Disease Prognosis C, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–81.
Schrauben SJ, Chen HY, Lin E, Jepson C, Yang W, Scialla JJ, et al. Hospitalizations among adults with chronic kidney disease in the United States: A cohort study. PLoS Med. 2020;17(12):e1003470.
Bikbov B, Purcell C, Levey AS, Smith M, Abdoli A, Abebe M, et al. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395(10225):709–33.
Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018;392(10159):2052–90.
System USRD. 2020 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2020. p. 2020.
Xie Y, Bowe B, Mokdad AH, Xian H, Yan Y, Li TT, et al. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018;94(3):567–81.
Diseases GBD, Injuries C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–22.
Webster AC, Nagler EV, Morton RL, Masson P. Chronic Kidney Disease. Lancet. 2017;389(10075):1238–52.
Chang Y, Ryu S, Choi Y, Zhang Y, Cho J, Kwon MJ, et al. Metabolically Healthy Obesity and Development of Chronic Kidney Disease: A Cohort Study. Ann Intern Med. 2016;164(5):305–12.
Garofalo C, Borrelli S, Minutolo R, Chiodini P, De Nicola L, Conte G. A systematic review and meta-analysis suggests obesity predicts onset of chronic kidney disease in the general population. Kidney Int. 2017;91(5):1224–35.
Kelly JT, Su G, Zhang QX, Marshall S, Gonzalez-Ortiz A, et al. Modifiable lifestyle factors for primary prevention of CKD: a systematic review and meta-analysis. J Am Soc Nephrol. 2021;32(1):239–53.
Li J, Huang Z, Hou J, Sawyer AM, Wu Z, Cai J, et al. Sleep and CKD in Chinese Adults: A Cross-Sectional Study. Clin J Am Soc Nephrol. 2017;12(6):885–92.
Park S, Lee S, Kim Y, Lee Y, Kang MW, Kim K, et al. Short or Long Sleep Duration and CKD: A Mendelian Randomization Study. J Am Soc Nephrol. 2020;31(12):2937–47.
Ellegaard O, Wallin JA. The bibliometric analysis of scholarly production: How great is the impact? Scientometrics. 2015;105(3):1809–31.
Doskaliuk B, Yatsyshyn R, Klishch I, Zimba O. COVID-19 from a rheumatology perspective: bibliometric and altmetric analysis. Rheumatol Int. 2021;41(12):2091–103.
Liu W, Wu L, Zhang Y, Shi L, Yang X. Bibliometric analysis of research trends and characteristics of oral potentially malignant disorders. Clin Oral Investig. 2020;24(1):447–54.
Wang Y, Liu Q, Chen Y, Qian Y, Pan B, Ge L, et al. Global Trends and Future Prospects of Child Nutrition: A Bibliometric Analysis of Highly Cited Papers. Front Pediatr. 2021;9:633525.
Science Citation Index: Coverage in Web of Science Core Collection compared to print and CD/DVD. https://support.clarivate.com/ScientificandAcademicResearch/s/article/Science-Citation-Index-Coverage-in-Web-of-Science-Core-Collection-compared-to-print-and-CDDVD?language=en_US. Accessed 15 Oct 2021.
Hu L-H, Liao Z, Gao R, Li Z-S. High quality medical journals and impact factors. Int J Cardiol. 2010;140(3):362–3.
Aria M, Cuccurullo C. bibliometrix: An R-tool for comprehensive science mapping analysis. J Informetrics. 2017;11(4):959–75.
Hirsch JE. An index to quantify an individual's scientific research output. Proc Natl Acad Sci U S A. 2005;102(46):16569–72.
van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–38.
Guo J, Pei L, Chen L, Chen H, Gu D, Xin C, et al. Research Trends of Acupuncture Therapy on Cancer Over the Past Two Decades: A Bibliometric Analysis. Integr Cancer Ther. 2020;19:1534735420959442.
Zhang J, Yu Q, Zheng F, Long C, Lu Z, Duan Z. Comparing keywords plus of WOS and author keywords: A case study of patient adherence research. J Assoc Inf Sci Technol. 2016;67(4):967–72.
Shen L, Wang S, Dai W, Zhang Z. Detecting the Interdisciplinary Nature and Topic Hotspots of Robotics in Surgery: Social Network Analysis and Bibliometric Study. J Med Internet Res. 2019;21(3):e12625.
Cebrino J, Portero de la Cruz S. A worldwide bibliometric analysis of published literature on workplace violence in healthcare personnel. PLoS One. 2020;15(11):e0242781.
Tang M, Luo L, Li C, Chiclana F, Zeng X-J. A Bibliometric Analysis and Visualization of Medical Big Data Research. Sustainability. 2018;10:166.
Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res. 2015;116(6):991–1006.
Manna P, Jain SK. Obesity, oxidative stress, adipose tissue dysfunction, and the associated health risks: causes and therapeutic strategies. Metab Syndr Relat Disord. 2015;13(10):423–44.
Thomas MC, Moran J, Forsblom C, Harjutsalo V, Thorn L, Ahola A, et al. The association between dietary sodium intake, ESRD, and all-cause mortality in patients with type 1 diabetes. Diabetes Care. 2011;34(4):861–6.
Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity, kidney dysfunction and hypertension: mechanistic links. Nat Rev Nephrol. 2019;15(6):367–85.
Schetz M, De Jong A, Deane AM, Druml W, Hemelaar P, Pelosi P, et al. Obesity in the critically ill: a narrative review. Intensive Care Med. 2019;45(6):757–69.
Kalantar-Zadeh K, Joshi S, Schlueter R, Cooke J, Brown-Tortorici A, Donnelly M, et al. Plant-Dominant Low-Protein Diet for Conservative Management of Chronic Kidney Disease. Nutrients. 2020;12(7):1931.
Yao RQ, Ren C, Wang JN, Wu GS, Zhu XM, Xia ZF, et al. Publication trends of research on sepsis and host immune response during 1999-2019: a 20-year bibliometric analysis. Int J Biol Sci. 2020;16(1):27–37.
Deng Z, Wang H, Chen Z, Wang T. Bibliometric analysis of dendritic epidermal T Cell (DETC) research From 1983 to 2019. Front Immunol. 2020;11:259.
Mafra D, Borges N, Alvarenga L, Esgalhado M, Cardozo L, Lindholm B, et al. Dietary components that may influence the disturbed gut microbiota in chronic kidney disease. Nutrients. 2019;11(3):496.
Cases A, Cigarran-Guldris S, Mas S, Gonzalez-Parra E. Vegetable-based diets for chronic kidney disease? it is time to reconsider. Nutrients. 2019;11(6):1263.
Vaziri ND, Liu SM, Lau WL, Khazaeli M, Nazertehrani S, Farzaneh SH, et al. High amylose resistant starch diet ameliorates oxidative stress, inflammation, and progression of chronic kidney disease. PLoS One. 2014;9(12):e114881.
Coppo R. The gut-kidney axis in IgA nephropathy: role of microbiota and diet on genetic predisposition. Pediatr Nephrol. 2018;33(1):53–61.
Chronic kidney disease in adults. assessment and management. London: National Institute for Health and Care Excellence: Guidelines; 2015.
Ikizler TA, Burrowes JD, Byham-Gray LD, Campbell KL, Carrero J-J, Chan W, et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am J Kidney Dis. 2020;76(3, Supplement 1):S1–S107.
Palmer SC, Maggo JK, Campbell KL, Craig JC, Johnson DW, Sutanto B, et al. Dietary interventions for adults with chronic kidney disease. Cochrane Database Syst Rev. 2017;4:CD011998.
Hahn D, Hodson EM, Fouque D. Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst Rev. 2020;10:CD001892.
Lascar N, Brown J, Pattison H, Barnett AH, Bailey CJ, Bellary S. Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol. 2018;6(1):69–80.
Staerk L, Sherer JA, Ko D, Benjamin EJ, Helm RH. Atrial fibrillation: epidemiology, pathophysiology, and clinical outcomes. Circ Res. 2017;120(9):1501–17.
Friedenreich CM, Ryder-Burbidge C, McNeil J. Physical activity, obesity and sedentary behavior in cancer etiology: epidemiologic evidence and biologic mechanisms. Mol Oncol. 2021;15(3):790–800.
Locke JE, Reed RD, Massie A, MacLennan PA, Sawinski D, Kumar V, et al. Obesity increases the risk of end-stage renal disease among living kidney donors. Kidney Int. 2017;91(3):699–703.
Dunkler D, Kohl M, Heinze G, Teo KK, Rosengren A, Pogue J, et al. Modifiable lifestyle and social factors affect chronic kidney disease in high-risk individuals with type 2 diabetes mellitus. Kidney Int. 2015;87(4):784–91.
Ikizler TA, Robinson-Cohen C, Ellis C, Headley SAE, Tuttle K, Wood RJ, et al. Metabolic effects of diet and exercise in patients with moderate to severe CKD: a randomized clinical trial. J Am Soc Nephrol. 2018;29(1):250–9.
Manfredini F, Mallamaci F, D'Arrigo G, Baggetta R, Bolignano D, Torino C, et al. Exercise in patients on dialysis: a multicenter, randomized clinical trial. J Am Soc Nephrol. 2017;28(4):1259–68.
Stengel B, Tarver-Carr ME, Powe NR, Eberhardt MS, Brancati FL. Lifestyle factors, obesity and the risk of chronic kidney disease. Epidemiology. 2003;14(4):479–87.
Xia J, Wang L, Ma Z, Zhong L, Wang Y, Gao Y, et al. Cigarette smoking and chronic kidney disease in the general population: a systematic review and meta-analysis of prospective cohort studies. Nephrol Dial Transplant. 2017;32(3):475–87.
Ricardo AC, Anderson CA, Yang W, Zhang X, Fischer MJ, Dember LM, et al. Healthy lifestyle and risk of kidney disease progression, atherosclerotic events, and death in CKD: findings from the Chronic Renal Insufficiency Cohort (CRIC) Study. Am J Kidney Dis. 2015;65(3):412–24.
Ricardo AC, Madero M, Yang W, Anderson C, Menezes M, Fischer MJ, et al. Adherence to a healthy lifestyle and all-cause mortality in CKD. Clin J Am Soc Nephrol. 2013;8(4):602–9.
Sontrop JM, Dixon SN, Garg AX, Buendia-Jimenez I, Dohein O, Huang SH, et al. Association between water intake, chronic kidney disease, and cardiovascular disease: a cross-sectional analysis of NHANES data. Am J Nephrol. 2013;37(5):434–42.
Lin J, Hu FB, Curhan GC. Associations of diet with albuminuria and kidney function decline. Clin J Am Soc Nephrol. 2010;5(5):836–43.
Judd E, Calhoun DA. Management of hypertension in CKD: beyond the guidelines. Adv Chronic Kidney Dis. 2015;22(2):116–22.
Hu EA, Lazo M, Rosenberg SD, Grams ME, Steffen LM, Coresh J, et al. Alcohol consumption and incident kidney disease: results from the atherosclerosis risk in communities study. J Ren Nutr. 2020;30(1):22–30.
Melekoglu E, Samur FG. Dietary strategies for gut-derived protein-bound uremic toxins and cardio-metabolic risk factors in chronic kidney disease: A focus on dietary fibers. Crit Rev Food Sci Nutr. 2021. https://doi.org/10.1080/10408398.2021.1996331.
Saglimbene VM, Wong G, van Zwieten A, Palmer SC, Ruospo M, Natale P, et al. Effects of omega-3 polyunsaturated fatty acid intake in patients with chronic kidney disease: Systematic review and meta-analysis of randomized controlled trials. Clin Nutr. 2020;39(2):358–68.
Wang S, Lv D, Jiang S, Jiang J, Liang M, Hou F, et al. Quantitative reduction in short-chain fatty acids, especially butyrate, contributes to the progression of chronic kidney disease. Clin Sci (Lond). 2019;133(17):1857–70.
Carrero JJ, Gonzalez-Ortiz A, Avesani CM, Bakker SJL, Bellizzi V, Chauveau P, et al. Plant-based diets to manage the risks and complications of chronic kidney disease. Nat Rev Nephrol. 2020;16(9):525–42.
Kramer H. Diet and Chronic Kidney Disease. Adv Nutr. 2019;10(Suppl_4):S367–S79.
Kecklund G, Axelsson J. Health consequences of shift work and insufficient sleep. BMJ. 2016;355:i5210.
Bo Y, Yeoh EK, Guo C, Zhang Z, Tam T, Chan TC, et al. Sleep and the risk of chronic kidney disease: a cohort study. J Clin Sleep Med. 2019;15(3):393–400.
Cheungpasitporn W, Thongprayoon C, Gonzalez-Suarez ML, Srivali N, Ungprasert P, Kittanamongkolchai W, et al. The effects of short sleep duration on proteinuria and chronic kidney disease: a systematic review and meta-analysis. Nephrol Dial Transplant. 2017;32(6):991–6.
Gonzalez Block MA, Mills A. Assessing capacity for health policy and systems research in low and middle income countries. Health Res Policy Syst. 2003;1(1):1.
Manchanda R, Varma R. Representation of authors and editors from poor countries: observed publication bias may reflect who is funding research. BMJ. 2004;329(7457):110.
Horton R. North and South: bridging the information gap. Lancet. 2000;355(9222):2231–6.
Dickersin K. The existence of publication bias and risk factors for its occurrence. JAMA. 1990;263(10):1385–9.
McCain K. Assessing obliteration by incorporation in a full-text database: JSTOR, Economics, and the concept of “bounded rationality”. Scientometrics. 2014;101(2):1445–59.
Acknowledgments
We thank the reviewers and editors for their suggestions to improve the work.
Funding
Xiaoxi Zeng was supported by the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYJC18010); Funding from National Natural Science Foundation of China (81900614), Science and Technology Department of Sichuan Province (2021YF0035), and Chengdu Science and Technology Bureau (2020-YF09–00117-GX) for obtaining the original articles and for the support of publication.
Author information
Authors and Affiliations
Contributions
HY, XZ, and PF were responsible for the study’s design and revised the manuscript. TY, LT, HY, and XZ searched and evaluated papers for inclusion. TY and YC extracted data and performed the bibliometric analyses. TY and XZ drafted the manuscript. The authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
The detailed search strategy.
Additional file 2: Supplementary Table 2.
Keywords merging details. Supplementary Table 3. Bibliometric information of the top 100-cited articles on the impact of modifiable lifestyles on CKD.
Additional file 3: Figure S1.
Word cloud of keywords of the top 100-cited articles.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yin, T., Chen, Y., Tang, L. et al. Relationship between modifiable lifestyle factors and chronic kidney disease: a bibliometric analysis of top-cited publications from 2011 to 2020. BMC Nephrol 23, 120 (2022). https://doi.org/10.1186/s12882-022-02745-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-022-02745-3