
Abstract
Objective
To compare the diagnostic accuracy of diffusion-weighted imaging (DWI) and 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) for differentiating pulmonary nodules and masses.
Methods
We systematically searched six databases, including PubMed, EMBASE, the Cochrane Library, and three Chinese databases, to identify studies that used both DWI and PET/CT to differentiate pulmonary nodules. The diagnostic performance of DWI and PET/CT was compared and pooled sensitivity and specificity were calculated along with 95% confidence intervals (CIs). The Quality Assessment of Diagnostic Accuracy Studies 2 was used to assess the quality of the included studies, and STATA 16.0 software was utilized to perform statistical analysis.
Results
Overall, 10 studies that enrolled a total of 871 patients with 948 pulmonary nodules were included in this meta-analysis. DWI had greater pooled sensitivity (0.85 [95% CI 0.77–0.90]) and specificity (0.91 [95% CI 0.82–0.96]) than PET/CT (sensitivity, 0.82 [95% CI 0.70–0.90]); specificity, (0.81, [95% CI 0.72–0.87]). The area under the curve of DWI and PET/CT were 0.94 (95% CI 0.91–0.96) and 0.87 (95% CI 0.84–0.90) (Z = 1.58, P > 0.05), respectively. The diagnostic odds ratio of DWI (54.46, [95% CI 17.98–164.99]) was superior to that of PET/CT (15.77, [95% CI 8.19–30.37]). The Deeks’ funnel plot asymmetry test showed no publication bias. The Spearman correlation coefficient test revealed no significant threshold effect. Lesion diameter and reference standard could be potential causes for the heterogeneity of both DWI and PET/CT studies, and quantitative or semi-quantitative parameters used would be a potential source of bias for PET/CT studies.
Conclusion
As a radiation-free technique, DWI may have similar performance compare with PET/CT in differentiating malignant pulmonary nodules or masses from benign ones.
Similar content being viewed by others


Introduction
Due to the high morbidity and mortality rates of lung cancer worldwide [1], differentiating malignant from benign pulmonary nodules is critical. The early detection of lung cancer could improve the survival rate and reduce mortality rate and a complete treatment could be achieved by early tumor resection. In clinical practice, computed tomography (CT) has been widely used for discriminating malignant nodules from benign pulmonary nodules. However, due to the overlap of morphological signs, distinguishing malignant nodules from benign nodules only based on CT findings is a clinical challenge for radiologists and physicians.
Positron emission tomography/computed tomography (PET/CT), as a widely used technique in clinical practice, provides combined metabolic and morphological information, which has made a great contribution to staging lung cancer, detecting metastatic lymph nodes, and evaluating the response to treatment in lung cancer patients [2,3,4,5,6]. In addition, PET/CT has been used for differentiating the malignant nodules from benign pulmonary nodules, and it has shown a higher accuracy than CT [5,6,7].
Recently, with the rapid development of magnetic resonance imaging (MRI) techniques, diffusion-weighted imaging (DWI) has gradually become an alternative for diagnosing pulmonary lesions. It can quantitatively provide an apparent diffusion coefficient (ADC), which reflects the cellularity of biological tissues [8]. According to previous studies, DWI has shown to be advantageous not only for predicting lung cancer invasiveness and pathological type of pulmonary tumors, but also for discriminating malignant nodules from benign pulmonary nodules [9,10,11].
To date, there is only one meta-analysis that compared the diagnostic performance of DWI and PET/CT in differentiating malignant and benign nodules/masses [12]. However, it included only literature in English and failed to conduct a subgroup analysis in their primary analysis because of the small amount of included studies [12]. Dividing the studies into subgroups based on specific characteristics (e.g. lesion diameter, imaging modality, study design) is important and can help identify the sources of heterogeneity of published papers. Moreover, there have been a few relevant comparative studies published in English and Chinese during the past several years. Therefore, we aimed to perform an updated meta-analysis of comparative studies to conduct a comprehensive and detailed analysis of this topic and conducted subgroup analyses to further explore the influencing factors of DWI and PET/CT in differentiating pulmonary nodules.
Materials and methods
Search strategy
The PubMed, EMBASE, the Cochrane Library, Wanfang, China National Knowledge Infrastructure (CNKI), and VIP databases were systematically searched from inception until June 2021 to retrieve comparative studies related to the diagnostic performance of DWI and PET/CT. Two radiologists assessed titles and abstracts separately for identification of potentially eligible studies. The keywords that were used to comprehensively search for the relevant articles in the above-mentioned databases are presented in Additional file 1.
Inclusion and exclusion criteria
Reviewers selected relevant studies that met the following inclusion criteria: (1) patients with pulmonary nodules who underwent both DWI and PET/CT in the same period; (2) the data of true-positive (TP), true-negative (TN), false-positive (FP), and false-negative (FN) were clearly reported; (3) the characteristics of pulmonary nodules should be detected by histological examination after surgical resection or imaging follow-up of more than 2 years without changing.
Data extraction and quality assessment
Two radiologists independently extracted the main characteristics of all the included articles, as shown in Tables 1 and 2, to reduce potential bias, and blindly evaluated the risk of bias using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) [13]. All disagreements were resolved through consensus.
Statistical analysis
A bivariate random-effects model was used to not only calculate the pooled sensitivities and specificities with 95% confidence intervals (CIs), but also to estimate the pooled positive likelihood ratio (PLR), negative likelihood ratio (NLR), and diagnostic odds ratios (DORs) with 95% CIs [14]. Forest plots were used to assess variability via examining the study results visually. Moreover, I2 > 50% indicated as high heterogeneity, and a two-tailed P-value < 0.05 was considered statistically significant. To identify the sources of heterogeneity, subgroup analyses of DWI and PET/CT were separately carried out (Tables 3 and 4). Moreover, summary receiver operating characteristic (SROC) curves were plotted based on sensitivity (Y-axis) and specificity (X-axis) to indicate the diagnostic accuracy of PET/CT and DWI. To assess the effect of threshold, the Spearman correlation coefficient was used, in which was calculated between the logit of sensitivity and the logit of (1-specificity), and a correlation coefficient (ρ) > 0.6 was considered as a significant correlation. Finally, publication bias was assessed by the Deeks’ funnel plot asymmetry test [15]. All statistical analyses were conducted by STATA 16.0 (StataCorp LLC, College Station, TX, USA) and Meta-DiSc.
(http://www.hrc.es/investigacion/metadisc_en.htm) software.
Analysis of diagnostic performance
The diagnostic performance of DWI and PET/CT was compared using the included studies. The parameters of both techniques used in the included studies were different, in which ADC and the contrast ratio between the lesions and spinal cord of signal intensity (SI-CR) were used in DWI, while the maximum standard uptake value (SUVmax) and the contrast ratio between the lesions and contralateral lung of SUV (SUV-CR) were utilized in PET/CT.
Results
Selection of eligible studies and quality assessment
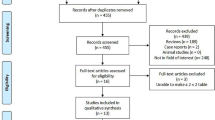
After comprehensively searching in the online databases, 150 articles were retrieved, while most of studies were excluded after scanning the abstracts and titles by two reviewers independently. Finally, 10 articles that enrolled 871 patients with 948 pulmonary nodules who underwent both PET/CT and DWI in the same period were included (Fig. 1).

Flow chart for studies selection in the meta-analysis
Methodological quality assessment was conducted among all the 10 studies with the QUADAS-2 tool (Fig. 2). Most of the studies were assessed as high risk in the index test domain and in the reference standard domain due to the use of an un-prespecified threshold or the different ways patients used as reference standard. As for the reference standard, samples that underwent histological diagnosis or follow-up of more than 2 years were identified [16, 17]. Therefore, only 2 studies were found with an unclear risk because they did not provide the appropriate time for radiological follow-up. What’s more, most of studies were also considered as unclear risk in the patients’ selection domain because the method (consecutive or random) of patients’ enrollment was not reported.

QUADAS-2 quality assessment of included studies
Characteristics of the eligible studies
All characteristics of the included studies that were published from 2008 to 2020 are summarized in Table 1 [8, 18,19,20,21,22,23,24,25,26]. Overall, a total of 10 studies were included, 5 studies were prospective and the other 5 were retrospective. As for DWI, 3 studies used 3.0-T MRI machines, and 6 studies utilized 1.5-T MRI machines to perform the scanning, the other one study [24] used both 1.5-T and 3.0-T MRI to carry out the DWI scanning, thus being counted twice as we extracted both results to analyze separately.
Furthermore, most of the studies used ADC as the parameter, while only one study utilized SI-CR. As for PET/CT, on the other hand, SUVmax was used as an index of FDG uptake in 6 studies, and SUV-CR was considered in the other studies. Besides, 3 studies used histopathological findings only as the reference standard, while 7 studies combined follow-up data with histopathological findings to identify the biological behaviors of pulmonary lesions.
Analysis of diagnostic accuracy and heterogeneity
The results of the pooled analyses of the studies are presented in Table 1. As for DWI, the pooled sensitivity and specificity were 0.85 (95% CI 0.77–0.90) and 0.91 (95% CI 0.82–0.96), while the pooled sensitivity and specificity of PET/CT were 0.82 (95% CI 0.70–0.90) and 0.81 (95% CI 0.72–0.87), respectively (Fig. 3). Additionally, the area under the ROC curve (AUC) of DWI was 0.94 (95% CI 0.91–0.96), which was higher than that of 0.87 (95% CI 0.84–0.90) for PET/CT (Z = 1.58, P > 0.05) (Fig. 4). The DOR of DWI and PET/CT was 54.46 (95% CI 17.98–164.99) and 15.77 (95% CI 8.19–30.37), respectively (Fig. 5). The PLR of DWI and PET/CT was 9.58 (95% CI 4.56–20.13) and 4.22 (95% CI 2.87–6.22), while NLR was 0.17 (95% CI 0.11–0.26) and 0.22 (95% CI 0.13–0.38), respectively (Fig. 6).

Forest plots of pooled sensitivity and specificity for A DWI and B PET/CT of 10 included studies. One DWI study [24] was counted twice due to the use of both 1.5-T and 3.0-T MRI on all patients, resulting in a total of 11 studies in the table. DWI Diffusion weighted imaging, PET/CT Positron emission tomography/computed tomography, CI Confidence interval

Summary receiver operating characteristics curves for A DWI and B PET/CT of 10 eligible studies. One DWI study [24] was counted twice due to the use of both 1.5-T and 3.0-T MRI on all patients, resulting in a total of 11 studies in the table. AUC Area under the curve, SENS Sensitivity, SPEC Specificity, SROC Summary receiver operating characteristics

Forest plots of the estimated pooled diagnostic odds ratio A DWI and B PET/CT of 10 included studies. One DWI study [24] was counted twice due to the use of both 1.5-T and 3.0-T MRI on all patients, resulting in a total of 11 studies in the table. DWI Diffusion weighted imaging, PET/CT Positron emission tomography/computed tomography, CI Confidence interval

Forest plots of pooled diagnostic likelihood ratio A DWI and B PET/CT of 10 included studies. One DWI study [24] was counted twice due to the use of both 1.5-T and 3.0-T MRI on all patients, resulting in a total of 11 studies in the table. DWI Diffusion weighted imaging, PET/CT Positron emission tomography/computed tomography, CI Confidence interval
Regarding the diagnostic accuracy, there was significant heterogeneity for both sensitivity (I2 = 83.69 for DWI, I2 = 85.58 for PET/CT) and specificity (I2 = 81.39 for DWI, I2 = 60.75 for PET/CT). While both DWI and PET/CT studies indicated the absence of threshold effect under the Spearman correlation coefficient test [(ρ = − 0.068, P = 0.842 for DWI); (ρ = 0.224, P = 0.533 for PET/CT)]. Thus, subgroup analyses were independently carried out to assess the potential sources of heterogeneity presented in Tables 3 and 4. It was found that not only lesions included both nodules and masses, but also the sensitivities of DWI and PET/CT increased using histological results as the reference standard. While studies using SUV-CR in PET/CT have higher specificity.
Publication bias
In the present meta-analysis, the Deek’s funnel plot asymmetry testing of DWI and PET/CT (P = 0.750 and 0.150, respectively) revealed the absence of publication bias (Fig. 7).

The Deeks’ funnel plot asymmetry test for A DWI and B PET/CT of 10 eligible studies. One DWI study [24] was counted twice due to the use of both 1.5-T and 3.0-T MRI on all patients, resulting in a total of 11 studies in the table. ESS: effective sample size
Discussion
Accurate differentiation of malignant tumors from benign tumors is crucial for patient management. Although PET/CT has been used to evaluate suspicious nodules as a recognized technique, it still has some drawbacks, such as high cost and radiation exposure. MRI, as a promising tool, has been recommended for clinical imaging of pulmonary tumors [27], and showed to play an important role in thoracic oncology. In the present meta-analysis, we compared the diagnostic performance of DWI and PET/CT for differentiating the malignant from benign pulmonary nodules and masses.
Spearman correlation coefficient test was performed in our study, and the results showed that there existed an insignificant threshold effect between the logit of sensitivity and the logit of (1-specificity). The current study demonstrated that DWI yielded higher pooled sensitivity (0.85 vs. 0.82), specificity (0.91 vs. 0.81), and AUC (0.94 vs. 0.87, P > 0.05) compared with PET/CT. According to a previous review, the diagnostic performance of DWI with different b-values can achieve high sensitivity (70–89%) and specificity (61–97%) [28]. On the other hand, PET/CT derives sensitivity between 49 and 100% as well as specificity between 17 and 85% for this differentiation [18, 21, 29, 30]. Additionally, DOR is a measurement combining sensitivity with specificity to assess diagnostic performance [31]. In our study, the DOR of DWI was higher than that of PET/CT (54.46 vs. 15.77), suggesting that DWI could have a slightly better performance in the differential diagnosis of pulmonary nodules.
As the likelihood ratio has been regarded as a more meaningful estimate in clinical practice, a highly robust diagnostic test might have a PLR > 10 and an NLR < 0.1, while a moderately advantageous one should have a PLR of 5–10 and an NLR of 0.1–0.2[32, 33]. In our study, PLR values of DWI and PET/CT were 9.58 and 4.22, while NLR values of DWI and PET/CT were 0.17 and 0.22, respectively. The PLR of DWI was higher and the NLR was lower than PET/CT, which suggested that DWI could be a moderately advantageous test in clinical practice.
Despite that both imaging modalities have great potential for pulmonary nodule assessment, FP and FN results are inevitable. Some inflammatory diseases, such as fungal infections, have shown FP results on DWI because of the infiltration of inflammatory cells [34]. Meanwhile, Deppen et al. [35] and Croft et al. [36] reported that granulomatous disease could lead to FP scans on PET/CT due to the high glucose metabolism. Besides, some adenocarcinomas, especially well-differentiated type, may represent FN findings on both DWI and PET/CT, because they have lower tumor cellularity and more abundant mucus than other types of carcinoma [34, 37,38,39,40]. Usuda et al. [41] reported that after pulmonary resection for lung cancer, DWI is more useful to discriminate suture granuloma from suture recurrence compare with PET/CT. Thus, a study on the mismatched results between PET/CT and DWI should be essentially conducted.
In the present meta-analysis, we included eligible studies published in Chinese to decrease the probability of publication bias. Moreover, we performed subgroup analyses to examine sources of heterogeneity. In the subgroup analyses, lesions that included masses and nodules [22, 24] had higher sensitivities in both DWI (0.87 vs. 0.74) and PET/CT (0.97 vs. 0.77) in comparison with lesions that included only nodules [8, 18, 19, 25]. This may demonstrate that the smaller the lesion size is, the lower the diagnostic accuracy of DWI and PET/CT can be. Khalaf et al. [30] also found that the diagnostic performance of PET/CT depends on lesion diameters; the bigger they are, the higher sensitivity (91–100%) and the lower specificity (17–47%) it has. Furthermore, compared with using histological and follow-up examinations[8, 18, 19, 21, 22, 24, 25] as the reference standard, using only histological examinations[20, 23, 26] would have higher sensitivities in both techniques [DWI (0.82 vs. 0.90); PET/CT (0.75 vs. 0.92)]. It might be because patients with malignant nodules would more likely to undergo surgeries than those with benign nodules; therefore, more malignancies and fewer benign lesions might be included in studies using histology as the reference standard. This could lead to a higher sensitivity in these studies. Moreover, our results showed that SUV-CR [8, 19, 21, 24, 25] derived from PET/CT had a higher specificity compared with the SUVmax (0.84 vs. 0.78) [18, 20,21,22,23, 26]. In addition, SUV-CR has previously shown a higher sensitivity in comparison with SUVmax [8, 42]. SUV-CR, as a semi-quantitative parameter, is not likely affected by factors, such as lesion size, body size, etc., while SUVmax could be affected [43]; thus, SUV-CR could be more clinically valuable in discriminating benign nodules from malignant lung nodules.
Our study contains some limitations. First, the risk of bias in all the included studies was high, therefore, high-quality studies should be conducted in the future. Second, most of the studies used follow-up examinations as the reference standard, which might lead to misclassification and potential bias in the result [16, 17]. Third, our meta-analysis did not include unpublished studies, which might ignore some negative or insignificant results.
In conclusion, DWI may have similar performance compared with PET/CT for differentiating the malignant from benign pulmonary nodules or masses. DWI has some advantages over PET/CT in terms of lower cost and no exposure to ionizing radiation. Therefore, DWI could be considered as a potential alternative for differentiating pulmonary lesions. However, prospective studies with higher quality and larger sample sizes should be carried out to validate the clinical value of DWI.
Availability of data and materials
The data supporting this meta-analysis are from previously reported studies and datasets, which have been cited. The processed data are available from the coresponding author upon request.
Abbreviations
- CT:
-
Computed tomography
- PET/CT:
-
Positron emission tomography/computed tomography
- MRI:
-
Magnetic resonance imaging
- DWI:
-
Diffusion-weighted imaging
- ADC:
-
Apparent diffusion coefficient
- TP:
-
True-positive
- TN:
-
True-negative
- FP:
-
False-positive
- FN:
-
False-negative
- QUADAS-2:
-
Quality Assessment of Diagnostic Accuracy Studies 2
- CIs:
-
Confidence intervals
- PLR:
-
Positive likelihood ratio
- NLR:
-
Negative likelihood ratio
- DORs:
-
Diagnostic odds ratios
- SROC:
-
Summary receiver operating characteristic
- SI-CR:
-
The contrast ratio between the lesions and spinal cord of signal intensity
- SUVmax :
-
The maximum standard uptake value
- SUV-CR:
-
The contrast ratio between the lesions and contralateral lung of SUV
- AUC:
-
The area under the ROC curve
References
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71(1).
Groheux D, Quere G, Blanc E, Lemarignier C, Vercellino L, de Margerie-Mellon C, et al. FDG PET-CT for solitary pulmonary nodule and lung cancer: literature review. Diagn Interv Imaging. 2016;97(10):1003–17.
Kandathil A, Sibley RC, Subramaniam RM. Lung cancer recurrence: F-FDG PET/CT in clinical practice. AJR Am J Roentgenol. 2019;213(5):1136–44.
Dissaux G, Visvikis D, Da-Ano R, Pradier O, Chajon E, Barillot I, et al. Pretreatment F-FDG PET/CT radiomics predict local recurrence in patients treated with stereotactic body radiotherapy for early-stage non-small cell lung cancer: a multicentric study. J Nucl Med: Off Publ Soc Nucl Med. 2020;61(6):814–20.
Kandathil A, Kay FU, Butt YM, Wachsmann JW, Subramaniam RM. Role of FDG PET/CT in the eighth edition of TNM staging of non-small cell lung cancer. Radiogr: Rev Publ Radiol Soc North Am. 2018;38(7):2134–49.
Li W, Pang H, Liu Q, Zhou J. The role of 18F-FDG PET or 18F-FDG-PET/CT in the evaluation of solitary pulmonary nodules. Eur J Radiol. 2015;84(10):2032–7.
Gilbert FJ, Harris S, Miles KA, Weir-McCall JR, Qureshi NR, Rintoul RC, et al. Comparative accuracy and cost-effectiveness of dynamic contrast-enhanced CT and positron emission tomography in the characterisation of solitary pulmonary nodules. Thorax. 2021;77(10):988–96.
Ohba Y, Nomori H, Mori T, Ikeda K, Shibata H, Kobayashi H, et al. Is diffusion-weighted magnetic resonance imaging superior to positron emission tomography with fludeoxyglucose F 18 in imaging non-small cell lung cancer? J Thorac Cardiovasc Surg. 2009;138(2):439–45.
Çakmak V, Ufuk F, Karabulut N. Diffusion-weighted MRI of pulmonary lesions: Comparison of apparent diffusion coefficient and lesion-to-spinal cord signal intensity ratio in lesion characterization. J Magn Reson Imag: JMRI. 2017;45(3):845–54.
Kanauchi N, Oizumi H, Honma T, Kato H, Endo M, Suzuki J, et al. Role of diffusion-weighted magnetic resonance imaging for predicting of tumor invasiveness for clinical stage IA non-small cell lung cancer. Eur J Cardiothorac Surg. 2009;35(4):706–11.
Wan Q, Deng Y-S, Lei Q, Bao Y-Y, Wang Y-Z, Zhou J-X, et al. Differentiating between malignant and benign solid solitary pulmonary lesions: are intravoxel incoherent motion and diffusion kurtosis imaging superior to conventional diffusion-weighted imaging? Eur Radiol. 2019;29(3):1607–15.
Basso Dias A, Zanon M, Altmayer S, Sartori Pacini G, Henz Concatto N, Watte G, et al. Fluorine 18-FDG PET/CT and diffusion-weighted MRI for malignant versus benign pulmonary lesions: a meta-analysis. Radiology. 2019;290(2):525–34.
Whiting PF, Rutjes AWS, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–36.
Chu H, Cole SR. Bivariate meta-analysis of sensitivity and specificity with sparse data: a generalized linear mixed model approach. J Clin Epidemiol. 2006;59(12):1331–2.
Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol. 2005;58(9):882–93.
Soubani AO. The evaluation and management of the solitary pulmonary nodule. Postgrad Med J. 2008;84(995):459–66.
Midthun DE, Swensen SJ, Jett JR. Approach to the solitary pulmonary nodule. Mayo Clin Proc. 1993;68(4):378–85.
Ohno Y, Kishida Y, Seki S, Yui M, Miyazaki M, Koyama H, et al. Amide proton transfer-weighted imaging to differentiate malignant from benign pulmonary lesions: comparison with diffusion-weighted imaging and FDG-PET/CT. J Magn Reson Imag. 2018;47(4):1013–21.
Nomori H, Cong Y, Sugimura H, Kato Y. Comparing diffusion-weighted imaging and positron emission tomography for pulmonary nodules measuring from 1 to 3 cm in size. Surg Today. 2015;45(12):1535–41.
Selcuk CT, Gulfidan U. Comparison of the diagnostic accuracy of diffusion-weighted magnetic resonance imaging and positron emission tomography/computed tomography in pulmonary nodules: a prospective study. Polish J Radiol. 2019;84:498–503.
Kang H, Zhang W, Jin R, Chen J. Comparison of whole-body diffusion-weighted magnetic resonance imaging and positron emission tomography in lung cancer. Radiol Pract. 2011;26(3):286–9.
Katsuo U, Motoyasu S, Nozomu M, Masakatsu U, Makoto T, Yuichiro M, et al. Diagnostic performance of diffusion weighted imaging of malignant and benign pulmonary nodules and masses: comparison with positron emission tomography. Asian Pacific J Cancer Prev: APJCP. 2014;15(11):4629–35.
Liu L, Deng Y, Lei Q. Differentiation of solitary pulmonary lesions with Bi-exponential and mono-exponential model of diffusion weighted imaging versus PET-CT. J Clin Radiol. 2020;39(01):201–5.
Ohba Y, Nomori H, Mori T, Shiraishi K, Namimoto T, Katahira K. Diffusion-weighted magnetic resonance for pulmonary nodules: 1.5 versus 3 Tesla. Asian Cardiovasc Thorac Ann. 2011;19(2):108–14.
Mori T, Nomori H, Ikeda K, Kawanaka K, Shiraishi S, Katahira K, et al. Diffusion-weighted magnetic resonance imaging for diagnosing malignant pulmonary nodules/masses: comparison with positron emission tomography. J Thorac Oncol. 2008;3(4):358–64.
Zhang J, Cui L-B, Tang X, Ren X-L, Shi J-R, Yang H-N, et al. DW MRI at 3.0 T versus FDG PET/CT for detection of malignant pulmonary tumors. Int J Cancer. 2014;134(3):606-11.
Hatabu H, Ohno Y, Gefter WB, Parraga G, Madore B, Lee KS, et al. Expanding applications of pulmonary MRI in the clinical evaluation of lung disorders: fleischner society position paper. Radiology. 2020;297(2):286–301.
Kim HS, Lee KS, Ohno Y, van Beek EJR, Biederer J. PET/CT versus MRI for diagnosis, staging, and follow-up of lung cancer. J Magn Reson Imag: JMRI. 2015;42(2):247–60.
Kim SK, Allen-Auerbach M, Goldin J, Fueger BJ, Dahlbom M, Brown M, et al. Accuracy of PET/CT in characterization of solitary pulmonary lesions. J Nucl Med: Off Publ Soc Nucl Med. 2007;48(2):214–20.
Khalaf M, Abdel-Nabi H, Baker J, Shao Y, Lamonica D, Gona J. Relation between nodule size and 18F-FDG-PET SUV for malignant and benign pulmonary nodules. J Hematol Oncol. 2008;1:13.
Glas AS, Lijmer JG, Prins MH, Bonsel GJ, Bossuyt PMM. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol. 2003;56(11):1129–35.
Shen G, Lan Y, Zhang K, Ren P, Jia Z. Comparison of 18F-FDG PET/CT and DWI for detection of mediastinal nodal metastasis in non-small cell lung cancer: a meta-analysis. PLoS ONE. 2017;12(3):e0173104.
Li B, Li Q, Nie W, Liu S. Diagnostic value of whole-body diffusion-weighted magnetic resonance imaging for detection of primary and metastatic malignancies: a meta-analysis. Eur J Radiol. 2014;83(2):338–44.
Wan Q, Deng Y-S, Zhou J-X, Yu Y-D, Bao Y-Y, Lei Q, et al. Intravoxel incoherent motion diffusion-weighted MR imaging in assessing and characterizing solitary pulmonary lesions. Sci Rep. 2017;7:43257.
Deppen S, Putnam JB, Andrade G, Speroff T, Nesbitt JC, Lambright ES, et al. Accuracy of FDG-PET to diagnose lung cancer in a region of endemic granulomatous disease. Ann Thorac Surg. 2011;92(2):428–33.
Croft DR, Trapp J, Kernstine K, Kirchner P, Mullan B, Galvin J, et al. FDG-PET imaging and the diagnosis of non-small cell lung cancer in a region of high histoplasmosis prevalence. Lung Cancer (Amsterdam, Netherlands). 2002;36(3):297–301.
Uto T, Takehara Y, Nakamura Y, Naito T, Hashimoto D, Inui N, et al. Higher sensitivity and specificity for diffusion-weighted imaging of malignant lung lesions without apparent diffusion coefficient quantification. Radiology. 2009;252(1):247–54.
Ambrosini V, Nicolini S, Caroli P, Nanni C, Massaro A, Marzola MC, et al. PET/CT imaging in different types of lung cancer: an overview. Eur J Radiol. 2012;81(5):988–1001.
Lee HY, Lee KS. Ground-glass opacity nodules: histopathology, imaging evaluation, and clinical implications. J Thorac Imaging. 2011;26(2):106–18.
Liu S, Cheng H, Yao S, Wang C, Han G, Li X, et al. The clinical application value of PET/CT in adenocarcinoma with bronchioloalveolar carcinoma features. Ann Nucl Med. 2010;24(7):541–7.
Usuda K, Iwai S, Yamagata A, Iijima Y, Motono N, Matoba M, et al. Differentiation between suture recurrence and suture granuloma after pulmonary resection for lung cancer by diffusion-weighted magnetic resonance imaging or FDG-PET/CT. Transl Oncol. 2021;14(2):100992.
Obrzut S, Pham RH, Vera DR, Badran K, Hoha CK. Comparison of lesion-to-cerebellum uptake ratios and standardized uptake values in the evaluation of lung nodules with 18F-FDG PET. Nucl Med Commun. 2007;28(1):7–13.
Nomori H, Watanabe K, Ohtsuka T, Naruke T, Suemasu K, Uno K. Visual and semiquantitative analyses for F-18 fluorodeoxyglucose PET scanning in pulmonary nodules 1–3 cm in size. Ann Thorac Surg. 2005;79(3):984–8.
Acknowledgements
Not applicable
Funding
This work is supported by the Foundation of Guangzhou Municipal Science and Technology Bureau (202102010253), Guangdong Demonstration Base for Joint Training of Graduate Students (20201), Open Project Fund of the Sixth Affiliated Hospital of Guangzhou Medical University (2020-11-370), and Project of Guangzhou Municipal Health Bureau (20201A010051).
Author information
Authors and Affiliations
Contributions
Conception and design: QW and XL, Administrative support: QW and XL, Provision of study materials or patients: QW and JL, Collection and assembly of data: JL and XX and YL, Data analysis and interpretation: JL and XX and XX, Manuscript writing: All authors. Final approval of manuscript: All authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. The search strategy of PubMed.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, J., Xia, X., Zou, Q. et al. Diagnostic performance of diffusion-weighted imaging versus 18F-FDG PET/CT in differentiating pulmonary lesions: an updated meta-analysis of comparative studies. BMC Med Imaging 23, 37 (2023). https://doi.org/10.1186/s12880-023-00990-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-023-00990-y