
Abstract
Background
The pandemic of coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), had a significant impact worldwide. Vaccines against COVID-19 appear as a tool able to curb out mortality and reduce the circulation of the virus. Little is known so far about the clinical characteristics of individuals who developed SARS-CoV-2 infection after having received the vaccination, as well as the temporal relationship between vaccine administration and symptoms onset.
Methods
Retrospective cohort study among the 3219 healthcare workers (HCWs) of the Fondazione IRCCS Ospedale Maggiore Policlinico of Milano who received a full immunization with the BNT162b2 vaccine and who developed SARS-CoV-2 infection (documented through positive RT-PCR on nasopharyngeal swab) in March–April 2021.
Results
Overall, we have identified 15 HCWs with SARS-CoV-2 infection after vaccination, 7 (46.7%) of them were male and the mean age was 38.4 years (SD 14). In 4 of them, the presence of SARS-CoV-2 anti-nucleocapsid (anti-N) antibodies was assessed before vaccination and resulted positive in 1 case. In all HCWs the presence of SARS-CoV-2 anti-spike (anti-S1) antibodies was assessed, on average 42.2 days after the completion of vaccination, with a mean value of 2055 U/mL (SD 1927.3). SARS-CoV-2 infection was ascertained on average 56.2 days after vaccination. The mean cycle threshold (Ct) of SARS-CoV-2 PCR was 26.4, the lineage was characterized in 9 HCWs. None of the HCWs reported a primary or secondary immunodeficiency. Regarding symptoms, they were reported only by 7 (46.7%) HCWs and appeared on average 55 days after the second dose of vaccination. Of those who reported symptoms, one (14.3%) had fever, 7 (100%) rhinitis/conjunctivitis, 4 (57.1%) taste and smell alterations, none had respiratory symptoms, 4 headache/arthralgia (57.1%) and 1 gastrointestinal symptom (14.3%). All symptoms disappeared in a few days and no other unclassified symptoms were reported.
Conclusions
Infections occurring after vaccination with the BNT162b2 vaccine are mostly asymptomatic and are not associated with the serum titre of anti-S1 antibodies. We did not find a predominance of specific viral variants, with several lineages represented.
Similar content being viewed by others


Background
The pandemic of coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has caused significant morbidity and mortality. Vaccines against COVID-19 appear as a tool able to curb out mortality and reduce the circulation of the virus. Consequently, mass vaccination campaigns are ongoing worldwide [1, 2]. Healthcare workers (HCWs) are a population who has been vaccinated early in the pandemic due to their high exposure to the virus, the corresponding elevated risk of infection and the possible role in spreading the disease [3].
Little is known so far about the clinical characteristics of HCWs who developed SARS-CoV-2 infection after having received the vaccination, as well as the temporal relationship between vaccine administration and symptoms onset. To answer these questions, we conducted a retrospective study among the HCWs vaccinated with BNT162b2 who developed SARS-CoV-2 infection (documented through positive RT-PCR on nasopharyngeal swab) in a large university hospital, collecting their clinical characteristics.
Methods
All the HCWs of the IRCCS Ospedale Maggiore Policlinico, a university hospital in Milan, Italy, were offered the COVID-19 vaccination with BNT162b2 vaccine. Among the 3622 HCWs working in our centre at the time of the study, 3219 (88.9%) received the full schedule, 170 (4.7%) received only the first shot and 233 (6.4%) were not vaccinated. The two prescribed shots were administered during January and February 2021. The HCWs of our hospital who are working in direct contact with proven or possible COVID-19 patients are subject to mandatory surveillance nasopharyngeal swab (NPS) for SARS-CoV-2 every two weeks, irrespective of the presence of symptoms. We collected the demographic, clinical and virologic characteristics of those who had positive NPSs in the period 01/03/2021–30/04/2021. For SARS-CoV-2 RNA detection was used the Alinity m SARS-CoV-2 assay on Alinity m (Abbott Molecular, IL, USA). The test is an rRT-PCR that allow simultaneous detection of RdRp and N genes. Serologic analyses were performed with two electrochemiluminescence immunoassay (ECLIA), Elecsys Anti-SARS-CoV-2 and Elecsys Anti-SARS-CoV-2 Son Cobas e801 (Roche Diagnostic, Mannheim, Germany) for the detection of total antibodies (including IgG) directed against SARS-CoV-2 nucleocapsid (N) antigen and SARS-CoV-2 spike protein receptor-binding domain (RBD) respectively. Full genome sequences were obtained by amplifying using CleanPlex for SARS-CoV-2 Research and Surveillance NGS panel (Paragon Genomics, Hayward CA, USA). A library was prepared with the PCR products and sequencing was performed on the Illumina MiSeq platform. The results were aligned to the reference genome NC_045512.2 by SOPHiA DDM software, v4 (SOPHiA GENETICS, USA). The software used to assign lineages to SARS CoV-2 sequences was Phylogenetic Assignment of Named Global Outbreak LINeages (Pango COVID-19 Lineage Assigner) [4, 5]. Descriptive statistics were obtained for all the variables collected, analyses were performed with Stata 17 (StataCorp. 2019). All the enrolled patients signed written informed consent. The study protocol (#828_2021) was approved by the local (Milano Area 2) Ethics Committee.
Results
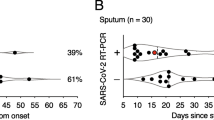
Overall, we have identified 15 HCWs with SARS-CoV-2 infection after vaccination, 7 (46.7%) of them were male and the mean age was 38.4 years (SD 14). In 4 of them, the presence of SARS-CoV-2 anti-nucleocapsid (anti-N) antibodies was assessed before vaccination and resulted positive in 1 case. In all HCWs the presence of SARS-CoV-2 anti-spike (anti-S1) antibodies was assessed, on average 42.2 days after the completion of vaccination, with a mean value of 2055 U/mL (SD 1927.3). SARS-CoV-2 infection was ascertained on average 56.2 days after vaccination. The mean cycle threshold (Ct) of SARS-CoV-2 PCR was 26.4, the lineage was characterized in 9 HCWs (Table 1). None of the HCWs reported a primary or secondary immunodeficiency.
Regarding symptoms, they were reported only by 7 (46.7%) HCWs and appeared on average 55 days after the second dose of vaccine. Of those who reported symptoms, one (14.3%) had fever, 7 (100%) rhinitis/conjunctivitis, 4 (57.1%) taste and smell alterations, none had respiratory symptoms, 4 headache/arthralgia (57.1%) and 1 gastrointestinal symptom (14.3%). All symptoms disappeared in a few days and no other unclassified symptoms were reported (Table 2).
Discussion
We have identified 15 HCWs who developed SARS-CoV-2 infection after completing the vaccination schedule with the BNT162b2 vaccine. Symptoms were reported by less than half of those included in the study, were mild, with only one case of fever, and disappeared quickly. The infections were detected through the mandatory surveillance system applied in our hospital, on average almost 2 months after the completion of the vaccination schedule.
The absence of important symptoms is a reassuring finding, which confirms the data about the efficacy of the BNT162b2 vaccine in preventing the severe form of COVID-19 reported in the registration study [6]. Intriguingly is the high incidence of rhinitis and conjunctivitis, which resulted in the most frequently reported symptom. Conjunctivitis is usually reported in about 1% of COVID-19 patients, with a higher prevalence (3%) among severe cases. The expression on the conjunctiva of the entry receptor for SARS-CoV-2, ACE-2, is disputed [7, 8], even though it has been shown how the inoculation in the ocular conjunctiva of SARS-CoV-2 can cause mild COVID-19 in rhesus macaques [9]. It is possible to speculate that the conjunctiva represents the site with the highest viral concentration in patients with the infection after vaccination, and this is reflected by the presence of a vigorous inflammatory response. Further studies are necessary to assess the concentration of immunoglobulins against SARS-CoV-2 in the ocular fluids after vaccination and their neutralizing activity.
In a previous publication from our group, we described how SARS-CoV-2 reinfections occurring in HCWs with a previous diagnosis of COVID-19 were mostly asymptomatic (7/9) [10]. Instead, we have previously observed during the first wave of COVID-19 pandemic how only a minority of HCWs has asymptomatic SARS-CoV-2 infections (17/139) [11]. This reinforces the concept of reduced/absent symptoms in those who probably have developed immunity against SARS-CoV-2, both through infection or vaccination.
Regarding the mean value of the serum anti-S1 antibodies, we observed in those who developed SARS-CoV-2 infection a value superior to the mean value of all the vaccinated HCWs of our hospital (1577 U/mL) and also superior to the mean value of the vaccinated HCWs without a previous SARS-CoV-2 infection (1374 U/mL) [12]. This suggest that the raw value of the anti-S1 antibodies cannot predict the future development of infection, the neutralizing activity of these antibodies could be a better tool to predict the efficacy of the humoral response.
Interestingly, we did not find a predominance of specific viral variants, with several lineages represented. This is in accordance with published data, which highlighted a reduced but still efficacious immune response against viral variants in those vaccinated with BNT162b2, and suggest that the risk of infection after vaccination is not currently related to the viral genotype but to other variables yet to be uncovered [1, 13]. Of note, the prevalence of SARS-CoV-2 lineages detected is adherent to the Italian scenario at the time, with the Alpha variant the most frequently reported [14].
A limitation of our study is the short observation time post-vaccination, restricted to two months, which led to the identification of only 15 infections post-vaccination in a large cohort of HCWs. A longer observation time might have led to the identification of a higher number of cases, increasing the chance of also finding infections with severe clinical manifestations.
Conclusions
Infections occurring after vaccination with the BNT162b2 vaccine are mostly asymptomatic and are not associated with the serum titre of anti-S1 antibodies.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
08 February 2022
In the original publication an error was spot in an author's family name. The article has been updated to correct it.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- HCWs:
-
Healthcare workers
- ECLIA:
-
Electrochemiluminescence immunoassay
References
Haas EJ, Angulo FJ, Mclaughlin JM, Anis E, Singer SR, Khan F, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. 2021;397(10287):1819–29. https://doi.org/10.1016/S0140-6736(21)00947-8.
Lombardi A, Bozzi G, Ungaro R, Villa S, Castelli V, Mangioni D, et al. Mini review immunological consequences of immunization with COVID-19 mRNA vaccines: preliminary results. Front Immunol. 2021;12:677.
Lombardi A, Mangioni D, Consonni D, Cariani L, Bono P, Cantù AP, et al. Seroprevalence of anti-SARS-CoV-2 IgG among healthcare workers of a large university hospital in Milan, Lombardy, Italy: a cross-sectional study. BMJ Open. 2021;11(2): e047216. https://doi.org/10.1136/bmjopen-2020-047216.
Rambaut A, Holmes EC, O’Toole Á, Hill V, McCrone JT, Ruis C, et al. Addendum: A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat Microbiol. 2021;6(3):415. https://doi.org/10.1038/s41564-021-00872-5.
Rambaut A, Holmes EC, O’Toole Á, Hill V, McCrone JT, Ruis C, et al. A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat Microbiol. 2020;5(11):1403–7. https://doi.org/10.1038/s41564-020-0770-5.
Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA covid-19 vaccine. N Engl J Med. 2020;383(27):2603–15.
Zhou L, Xu Z, Castiglione GM, Soiberman US, Eberhart CG, Duh EJ. ACE2 and TMPRSS2 are expressed on the human ocular surface, suggesting susceptibility to SARS-CoV-2 infection. Ocul Surf. 2020;18(4):537–44. https://doi.org/10.1016/j.jtos.2020.06.007.
Lange C, Wolf J, Auw-Haedrich C, Schlecht A, Boneva S, Lapp T, et al. Expression of the COVID-19 receptor ACE2 in the human conjunctiva. J Med Virol. 2020;92(10):2081–6.
Deng W, Bao L, Gao H, Xiang Z, Qu Y, Song Z, et al. Ocular conjunctival inoculation of SARS-CoV-2 can cause mild COVID-19 in rhesus macaques. Nat Commun. 2020;11(1):1–7.
Comelli A, Consonni D, Lombardi A, Viero G, Oggioni M, Bono P, et al. Nasopharyngeal testing among healthcare workers (HCWs) of a Large University Hospital in Milan, Italy during two epidemic waves of COVID-19. Int J Environ Res Public Health. 2021;18(16):8748.
Lombardi A, Consonni D, Carugno M, Bozzi G, Mangioni D, Muscatello A, et al. Characteristics of 1573 healthcare workers who underwent nasopharyngeal swab testing for SARS-CoV-2 in Milan, Lombardy, Italy. Clin Microbiol Infect. 2020;26(10):1413.
Lombardi A, Consonni D, Oggioni M, Bono P, Renteria SU, Piatti A, et al. SARS-CoV-2 anti-spike antibody titres after vaccination with BNT162b2 in naïve and previously infected individuals. J Infect Public Health. 2021;14(8):1120–2. https://doi.org/10.1016/j.jiph.2021.07.005.
Liu Y, Liu J, Xia H, Zhang X, Fontes-Garfias CR, Swanson KA, et al. Neutralizing activity of BNT162b2-elicited serum. N Engl J Med. 2021;384(15):1466–8. https://doi.org/10.1056/NEJMc2102017.
Prevalenza e distribuzione delle varianti del virus SARS-CoV-2 di interesse per la sanità pubblica in Italia.
Acknowledgements
None.
Funding
This study was partially supported by the Ministry of Health RC 2021 and by Intesa San Paolo 2020 Fund. These funds covered the costs of laboratory consumables employed in the study.
Author information
Authors and Affiliations
Contributions
AL, DC and AG conceived the study. PB, SUR, DC, FC, MO collected the data. DC performed the statistical analysis. AL and GR wrote the first draft of the manuscript. AL, DC, AG, PB, SURC, FC, MO, GR, AB, ACP, SC, AM, LR, AP reviewed the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All the enrolled patients signed a written informed consent. The study protocol (#828_2021) was approved by the local (Milano Area 2) Ethics Committee.
Competing interests
We declare that we have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lombardi, A., Renisi, G., Consonni, D. et al. Clinical characteristics of healthcare workers with SARS-CoV-2 infection after vaccination with BNT162b2 vaccine. BMC Infect Dis 22, 97 (2022). https://doi.org/10.1186/s12879-022-07083-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-022-07083-1