
Abstract
Background
Cervical cancer is the predominant cancer among women in Kenya and second most common in women in developing regions. Population-based cytological screening and early treatment reduces morbidity and mortality associated with the cancer. We determined the occurrence of cervical precancerous changes and cervical microbial infections (Trichomonas vaginalis, Candida albicans, Neisseria gonorrhea and Actinomyces) among women attending Family Health Option Kenya (FHOK) clinic in Thika.
Methods
This was a hospital based cross sectional study among women attending reproductive health screening clinic from November 2013 to January 2014. Cervical Intraepithelial Neoplasia (CIN) I, II, III, cervical cancer and microbial infection (Actinomyces, Trichomonas vaginalis and Yeast cells) diagnosis was based on Pap smear screening test and High Vaginal Swab wet preparation microscopy. Neisseria gonorrhea was diagnosed through Gram staining. Socio-demographic and reproductive health data was collected using a structured questionnaire administered to the study participants and analyzed using Epi Info version 3.5.1.
Results
Of the 244 women screened, 238 (97.5%) presented with cervical inflammation, 80 (32.8%) cervical microbial infections and 12 (4.9%) cervical precancerous changes; 10 (83.3%) with CIN I and 2 (16.7%) CIN II. Of the 80 cervical microbial infections, 62 (77.5%) were yeast cell and 18 (22.5%) T. vaginalis. One thirty four (55%) participants had no history of Pap smear screening of which 84 (62.7%) were 20–40 years. Use of IUCDs (OR: 2.47, 95% CI 1.3–4.6) was associated with cervical inflammation.
Conclusions
CIN I was the predominant cervical precancerous change. There is need to scale up cervical screening test to capture all categories of women.
Similar content being viewed by others


Background
Cervical cancer is a leading cause of morbidity and mortality among women of the reproductive age especially in low resource limited countries. Widespread screening programs, a catalyst for early detection and management of cervical precancerous changes, significantly reduce cervical cancer incidence [1]. However, these screening programs are limited in Africa and cervical precancerous changes data is scarce [2]. In Kenya, cervical cancer is the leading cancer among women in the reproductive age group [3] nevertheless the screening coverage is at 3.2% [4]. An estimated 4802 women are diagnosed with cervical cancer annually of which 51% (2451) die from the disease [3]. On the other hand, cervical microbial infections have not been quantified.
The recommended cervical cancer screening age is from 25 years and re-screening period is every 5 years except for at risk population [5]. However, cervical screening is mainly conducted in private health facilities which are out of reach to many women in this resource limited setting. We determined the prevalence of cervical precancerous changes and selected cervical microbial infections among women attending FHOK Clinic in Thika for Pap smear testing.
Methods
Study design and setting
This was a hospital based cross-sectional study carried out in FHOK Clinic in Thika town. The clinic serves a wide urban and peri-urban population across Kiambu County, Muranga County as well as neighboring outskirts of Nairobi County. The facility is recognized as a centre of excellence in female reproductive health services along with an established quality assured Pap smear screening program.To calculate the sample size, we used a prevalence of 50% estimated by Fisher and Van Belle [6] as no previous study had been done in the area.
Characteristics of participants
Study participants were consenting women aged 15 years and above seeking Pap smear test at the health facility from November 2013 to January 2014 who had not taken antibiotics within 72 h before study enrollment.
Data collection
Study participants were interviewed using a structured questionnaire to collect socio-demographic and reproductive health information. This was followed by collection of Pap smear and High Vagina Swab (HVS) samples. Pap smears specimens were processed and stained through the Papanicolaou staining technique [7] for detection of Candida infection, actinomyces and cervical precancerous changes using Cervical Intraepithelial Neoplasia (CIN) reporting system. High vaginal swabs were processed for wet mount and Gram stain [8] examination for the diagnosis of cervical microbial infections; Trichomonas vaginalis infection was indicated by microscopic observation of motile trichomonads in wet mount, Gram negative diplococci signified gonorrhea infection and presence of pseudohyphae or hyphae or yeast buds denoted Candida albicans infection in Gram stain. Presence of more than 10 white blood cells under microscopic high-power field examination of HVS was classified as cervical inflammation. Both specimens were examined using a light microscope.
Data analysis
Data generated was entered in Microsoft Excel 2010 and analysed using Epi info version 3.5.1. Univariate analyses were calculated for both the dependent and independent variables. The association between socio-demographic characteristics and stages of cervical precancerous changes and cervical microbial infections were determined using linear regression for age, age at first sex experience and number of births; Chi square for comparing inflammation among the IUCDs users and non-IUCDs users; and fishers exact for marital status, literacy level, employment status, mode of contraception and history of Pap test.
Results
Demographics and socio-economics characteristics of participants
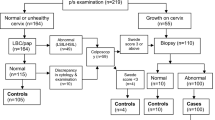
A total of 244 participants were interviewed and their Pap smear and HVS specimens examined. Their mean age was 42 (SD: 10.6) years, 134 (55%) had no history of previous Pap smear screening of which 84 (63%) falls within 20–40 years age group; 21–30 age group at 27% (36) and 31–40 age group at 36% (48). The mean age at first sexual experience was 20 (SD: 3) years, 230 (94%) parous of which 22.1% had 2 children, 159 (65.2%) were using various forms of contraceptives with Intrauterine Contraceptive Devices (IUCDs) being used by majority (23.8%) of the study participants (Table 1). Two hundred (81.9%) were married; 188 (94%) in monogamous unions and 12 (6%) in polygamous relationships, 196 (80.3%) were employment, 240 (98.4%) had attained basic formal education; 74 (30.3%) primary education, 84 (34.4%) secondary education and 82 (33.6%) post-secondary education.
Cervical precancerous changes
Fourteen (5.7%) participants presented with cervical cell abnormalities; 12 (4.9%) with cervical precancerous changes and 2 (0.8%) with viral changes. Of the 12 participants with cervical precancerous changes, 10 (83.3%) had CIN I and 2 (16.7%) had CIN II, with a mean age of 46 (SD: 8) years. Six (50%) had attained post-secondary education level, 10 (83%) were married, mean age at first sexual intercourse was 19 (SD: 2.3) years, 4 (33%) had their first sexual experience <18 years, 10 (83%) had experienced child birth with 8 (67%) having 3–5 children. Ten (83%) had observed the five yearly Pap smear screening recommendation in Kenya [5], that is, had a pap test between 2008 and 2013. Four of the study participants with CIN I, were having their first Pap screening. All (2) women with CIN II had previous screening in the year 2009.
There was no difference in the odds (OR: 1.11, 95% CI: 0.23–5.23) of cervical precancerous changes in women who were married and that of non-married women (single, separated and divorced). No significant association with precancerous changes was found with age, education level, employment status, age at first sexual intercourse, number of births, mode of contraception and history of Pap smear screening on the study participants.
Cervical inflammation
The prevalence of cervical inflammation was 238 (97.5%) while the prevalence of cervical microbial infection was 80 (32.8%). Of the 80 with cervical microbial infection, 62 (77.5%) were yeast cell and 18 (22.5%) were T. vaginalis infections. No actinomyces or gonorrhoea infection was identified. The distribution of yeast cell and T. vaginalis infections among study participants was statistically significant (P < 0.05). Among the different techniques employed in this study, HVS wet preparation had the highest positivity rate to inflammatory changes and their causes (Table 2). Of the 58 women using Intrauterine Contraceptive Devices (IUCDs), 26 (45%) exhibited cervical inflammation in their Pap smear results. Use of IUCDs (OR: 2.47, 95% CI 1.3–4.6, comparator were non-IUCDs users) was associated with having cervical inflammation.
Discussion
We observed two levels of cervical precancerous changes; CIN I and CIN II. Cervical intraepithelial neoplasia I (mild dysplasia) was the major dysplasia (83%) observed among the study participants during the study period. Candida and T. vaginalis were identified as cause of cervical inflammation among the study participants.
This study reported a low prevalence of cervical cell abnormalities (4.9%); 83.3% (10) Low-grade cervical lesions and 16.7% (2) high-grade cervical lesions. The results are comparable to a study done at an outpatient reproductive health clinic in Pakistan whereby 4.6% (32) cases had dysplastic changes of which 56.25% (18) were LSIL and 43.75% (14) HSIL [9]. Similar frequency of dysplastic smears were reported by Inamullah et al. [10]; 5% dysplasia of which 75% (6) were LSIL and 25% (2) HSIL, in a study done in Pakistan among women presenting with chronic discharge. Additionally, a study in women seeking care at a reproductive health clinic in Pakistan from February 2009 to February 2010, revealed dysplasia frequency of 3.7% (10 cases) of which 80% (8) had LSIL while 20% (2) HSIL [11]. These precancerous changes were detected among women on routine screening within age 34–60 years. This is important in Kenya; a country where 60% of cancer victims are below 70 years and 70–80% of the diagnose happening in late stages owing to lack of awareness, inadequate diagnostic facilities, lack of treatment facilities, inadequate personnel to manage invasive stages, high cost of treatment and high poverty Index [5, 12].
More than half (55%) of the study participant were having their first ever Pap smear screening of which 36% were 31–40 years. This falls within the reproductive age where most of the screening interventions should be done. The Centers for Disease Control and Prevention (CDC) epidemiological study found that 78% of the cervical cancer cases were diagnosed in women 30–39 years [13]. It is therefore not surprising that in Africa, where screening rates are low or non-existent, majority of women present with advanced disease. A study done by Sheikh and Manhua [14] in Saudi Arabia from January 2009 to January 2011 reported 83% (1224) of study participants had never been screened with Pap smear which was higher compared to our findings. In the current study, low uptake of Pap smear screening may be due to lack of awareness and/or shying away due to the invasive nature of Pap smear sample collection procedure. This illustrates that Pap smear screening programs need to be scaled up to reach more women and attain higher screening rates.
According to Burkadze and Gulisa [15], three out of four women who develop cervical cancer each year have never had a Pap smear or had not had one within the recommended intervals. Four cases (2.98%) of CIN I in this study had never had a Pap smear test before although not having a previous Pap smear test was not significantly associated with cervical precancerous changes in our study. Sheikh and Manhua [14] reported similar rates of cervical abnormalities among participants who were having Pap smear screening for the first time in Saudi Arabia, 2.91% (43). This suggests that earlier Pap smears screening would have meant earlier detection leading to an increased rate of recession and hence low mortality. Countries, such as Taiwan, with widespread organized screening programmes for cervical cancer, have substantially reduced cervical cancer incidence and mortality by 60–90% as well as increased survival rates [16,17,18]. Unfortunately in resource-limited countries, where Pap screening has not been effectively implemented, cervical cancer remains a major public health problem [19].
High prevalence of inflammatory changes (97.5%) was reported in this study. Cervical microbial infections accounted for 32.8% of the inflammation cases. These results contradict previous findings by a study at National Institute of Health, Islamabad in Pakistan where lower prevalence of inflammatory changes (55.31%) was reported [20]. Similarly, Rubia and Huma [11] found 55.7% (156) frequency of inflammation and 55% (88) was documented in another study by Inamullah et al. [10]. This higher prevalence of inflammatory changes among women with high literacy level and majority working women could be due to improved health seeking behaviour due to women empowerment.
Vaginal infections are common cause of inflammation of the genital tract in all women; some are associated with sexual activity while others, such as vaginal candidiasis, are not. In this study, Candida (25.4%) and Trichomonas vaginalis (7.4%) were the specific causes of inflammation identified in the High Vaginal Swab wet preparation. Differing findings have been documented in other studies. Bhojani and Garg [21] reported 0.5% prevalence of both Candida and Trichomonas vaginalis while Claeys et al. [22] reported a prevalence of 19.1% for Candida and 10.1% for Trichomonas vaginalis. Candida was the predominant (25.4%) specific cause of inflammation. This could be due to the fact that vaginal Candida species are emerging as significant opportunistic organisms that have increased over the past few decades attributed to both inappropriate use of antibiotics, increased use of hormonal contraceptives and the increasing population of immune-compromised individuals.
Detection of Trichomonas vaginalis, a sexually transmitted micro-organism, was suggestive of existence of potential for HIV transmission and the probable explanation would be due to low utilization of barrier method of contraception such as condom, which would provide protection from sexually transmitted diseases as well as cervical cancer. Actinomyces infection is usually detected in IUCD users. The infection was not reported in even among the IUCD users. This can be attributed to the fact that all IUCD users had a history of a previous Pap tests and therefore might have been treated previously. However, inflammation characterized by presence of polymorphonuclear cells (granulocytes) was evident in 26 (44.8%) of the IUCD users through Pap smear examination and with a significant statistical association (OR 2.47 at 95% C.I.). Studies in other parts of the world revealed similar association between vaginitis, and use of IUCDs. Sieber and Dietz [23] and Amsel et al., [24] found a strong association of nonspecific vaginitis with the use of IUCDs. This could be related to the insertion method and technique leading to introduction of bacteria into the uterine cavity or the IUCDs mobilizing polymorphonuclear leucocytes since it is a foreign body. Women using IUCDs requires a regular follow up and clinical examination.
Conclusions
Low prevalence of cervical precancerous changes and high prevalence of cervical microbial infection was reported. Majority of the participants were having Pap smear screening for the first time with the most un-screened persons falling within 21–40 years. Yeast cell was the predominant microbial organism detected with most causes of inflammation remaining non-specific.
Recommendation
There is need to scale up cervical cancer screening awareness in order to capture all categories of women in all age groups in the cervical cancer screening programs. Pap smear screening and high vaginal swab should be offered as one package to identify both precancerous changes and microbial infections not as stand-alone tests. Further studies on the non-specific cause of cervical inflammation should be conducted.
Abbreviations
- CI:
-
Confidence interval
- CIN:
-
Cervical Intraepithelial Neoplasia
- FHOK:
-
Family Health Option Kenya
- HIV:
-
Human Immunodeficiency Virus
- HSIL:
-
High grade squamous intraepithelial lesion
- HVS:
-
High Vagina Swab
- IUCDs:
-
Intrauterine Contraceptive Devices
- KUERC:
-
Kenyatta University Ethics Review Committee
- LSIL:
-
Low grade squamous intraepithelial lesion
- NGPMCBPC:
-
National Guidelines for Prevention and Management of Cervical, Breast and Prostate Cancer
- OR:
-
Odds Ratio
- Pap smears:
-
Papanicolaou smear
- SD:
-
Standard deviation
- T. vaginalis:
-
Trichomonas vaginalis
References
Douglas D, Rebecca F. Encyclopedia of Alternative Medicine. Detroit: The Gale Group Inc; 2005.
Ferlay J, Hai-Rim S, Freddie B, David F, Colin M, Donald MP. Estimates of worldwide burden of cancer in 2008. Int J Cancer. 2010;127(12):2893–917.
Bruni L, Barrionuevo-Rosas L, Serrano B, Brotons M, Cosano R, Muñoz J, Bosch FX, de Sanjosé S, Castellsagué X. ICO Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in Kenya. Summary Report; 2014. p. 03–17.
WHO/ICO Information Centre on HPV and Cervical Cancer (HPV Information Centre). Human Papillomavirus and Related Cancers in Kenya. Summary Report 2010.
National Guidelines for Prevention and Management of Cervical, Breast and Prostate Cancer (NGPMCBPC). Kenya Ministry of Public Health and Sanitation and Ministry of Medical Services 2012.
Fisher L, van Belle G. Biostatistics: a methodology for the health sciences. New York: John Wiley & Sons; 1993.
Koss LG. Diagnostic cytology and its histopathologic bases. Lippincott Company Philadelphia. J.B. 1992; 1:4.
Hucker GJ. A New Modification and Application of the Gram Stain. J Bacteriol. 1921;6(4):395–7.
Chandra M, Nasreen S, Ambreen G, Farkhunda K, Zakia Z. Prevalence and Risk Factors for Cervical Intraepithelial Neoplasia. J Liaquat Univ Med Health Sci. 2013;12:01.
Inamullah K, Faisal K, Ayesha RA. PAP Smear Screening in Women Presenting with Chronic Discharge At a Tertiary Care Setting. Ann Pak Inst Med Sci. 2013;9(2):61–3.
Rubia N, Huma Q. ‘Pap Smear’ for Screening of Precancerous Conditions of Cervix. J Ayub Med Coll Abbottabad. 2011;23(2):41–4.
Blanks RG, Moss SM, Coleman DA, Swerdlow AJ. An examination of the role of opportunistic smear taking in the NHS cervical screening programme using data from the CSEU cervical screening cohort study. Br J Obstet Gynaecol. 2007;114:1408–13.
Benard VB, Watson M, Castle PE, Saraiya M. Cervical carcinoma rates among young females in the United States. J Obstet Gynecol. 2012;120:1117–23.
Sheikh H, Manhua C. Role of Pap smear in early diagnosis of cervical cancer - A Case Study of women in Saudi Arabia. Life Sci J. 2012;9(2):1027–36.
Burkadze G, Gulisa T. Cytology Interpretations of Cervical PAP Smears in Georgia. Int J Gynecol Obstet. 2004;3:2.
Kalliala I, Anttila A, Pukkala E, Nieminen P. Risk of cervical and other cancers after treatment of cervical intraepithelial neoplasia: retrospective cohort study. Br Med J. 2005;331:1183.
Taylor R, Morrell S, Mamoon H, Wain G, Ross J. Decline in cervical cancer incidence and mortality in New South Wales in relation to control activities (Australia). Cancer Causes Control. 2006;17(3):299–306.
Su S, Huang J, Ho C, Liaw Y. Evidence for cervical cancer mortality with screening program in Taiwan, 1981–2010: age-period-cohort model. Biomed Central Public Health. 2013;13:13.
Franco EL, Coutlee F, Ferenczy A. Integrating human papillomavirus vaccination in cervical cancer control programmes. Public Health Genomics. 2009;12(5–6):352–61.
Khan MS, Raja FY, Ishfaq G, Tahir F, Subhan F, Kazi BM. PAP Smear Screening for Pre-cancerous Conditions of the Cervical Cancer. Pak J Med Res. 2005;44(3):111–3.
Bhojani KR, Garg R. Cytopathological study of cervical smears and correlation of findings with risk factors. Int J Biol Med Res. 2011;2(3):757–61.
Claeys P, Gonzalez C, Gonzalez M, Van Renterghem L, Temmerman M. Prevalence and risk factors of sexually transmitted infections and cervical neoplasia in women’s health clinics in Nicaragua. J Sex Transm Infect. 2002;78:204–7.
Sieber R, Dietz U. Lactobacillus acidophilus and Yogurt in the Prevention and Therapy of Bacterial Vaginosis. Int Dairy J. 1998;8:599–607.
Amsel R, Totten P, Spiegel C, Chen K, Eschenbach D, Holmes K. Nonspecific Vaginitis: Diagnostic Criteria and Microbial and Epidemiology Association. Am J Med. 1983;74:14–21.
Acknowledgements
We acknowledge the management and staff of FHOK Clinic in Thika, for supporting the investigation.
Funding
No funding was received from any funding body for this study.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request. The data will also be deposited in publicly available repositories after manuscript publication.
Author information
Authors and Affiliations
Contributions
EWK was responsible for overall study design, protocol preparation, data collection, specimen collection and analysis, data analysis, report and manuscript writing. LK contributed in protocol development and manuscript writing. MM contributed in protocol development and manuscript writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Authors’ information
Evalyne Wambui Kanyina: BSc. Medical Laboratory Sciences, MSc. Infectious Diseases, MSc Laboratory Management and Epidemiology Lucy Kamau: Ph.D. Margaret Muturi: Ph.D.
Ethics approval and consent to participate
This protocol was approved by Kenyatta University Ethics Review Committee (KUERC) and FHOK management before the commencement of the study. All study participants gave an informed consent before participation. Participant’s data was stored in a lockable filing cabinet and computer which was accessed by only authorized persons through a password to avoid a breach in confidentiality. Slight discomfort is experienced during the cervical examination using the speculum in Pap smear and HVS specimen collection. The study participants benefited from cervical cancer screening and cervical microbial testing as well as referral for treatment where appropriate.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kanyina, E.W., Kamau, L. & Muturi, M. Cervical precancerous changes and selected cervical microbial infections, Kiambu County, Kenya, 2014: a cross sectional study. BMC Infect Dis 17, 647 (2017). https://doi.org/10.1186/s12879-017-2747-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-017-2747-4