
Abstract
Background
A number of biomarkers have been studied for the diagnosis of sepsis in paediatrics, but no gold standard has been identified. Procalcitonin (PCT) was demonstrated to be an accurate biomarker for the diagnosis of sepsis in adults and showed to be promising in paediatrics. Our study reviewed the diagnostic accuracy of PCT as an early biomarker of sepsis in neonates and children with suspected sepsis.
Methods
A comprehensive literature search was carried out in Medline/Pubmed, Embase, ISI Web of Science, CINAHL and Cochrane Library, for studies assessing PCT accuracy in the diagnosis of sepsis in children and neonates with suspected sepsis. Studies in which the presence of infection had been confirmed microbiologically or classified as “probable” by chart review were included. Studies comparing patients to healthy subjects were excluded. We analysed data on neonates and children separately.
Our primary outcome was the diagnostic accuracy of PCT at the cut-off of 2-2.5 ng/ml, while as secondary outcomes we analysed PCT cut-offs <2 ng/ml and >2.5 ng/ml. Pooled sensitivities and specificities were calculated by a bivariate meta-analysis and heterogeneity was graphically evaluated.
Results
We included 17 studies, with a total of 1408 patients (1086 neonates and 322 children). Studies on neonates with early onset sepsis (EOS) and late onset sepsis (LOS) were grouped together. In the neonatal group, we calculated a sensitivity of 0.85, confidence interval (CI) (0.76; 0.90) and specificity of 0.54, CI (0.38; 0.70) at the PCT cut-off of 2.0-2.5 ng/ml. In the paediatric group it was not possible to undertake a pooled analysis at the PCT cut-off of 2.0-2.5 ng/ml, due to the paucity of the studies.
Conclusions
PCT shows a moderate accuracy for the diagnosis of sepsis in neonates with suspected sepsis at the cut-off of 2.0-2.5 ng/ml. More studies with high methodological quality are warranted, particularly in neonates, studies considering EOS and LOS separately are needed to improve specificity.
Trial registration
PROSPERO Identifier: CRD42016033809. Registered 30 Jan 2016.
Similar content being viewed by others


Background
Sepsis is an on-going clinical problem, and a leading cause of death in adults and children. It has been defined as a systemic inflammatory response syndrome (SIRS) caused by bloodstream infections [1, 2] or, more recently, as life-threatening organ dysfunction caused by a deregulated host response to infection [3].
Several inflammatory mediators are involved in the pathogenesis of sepsis: coagulation, innate and adaptive immune response, intermediary metabolism products, all together interacting and leading to this abnormal response [4].
SIRS may not only be determined by infections but also non-infectious causes, such as autoimmune disorders, pancreatitis, vasculitis, thromboembolism, burns, or surgery procedures. SIRS in paediatrics is defined by at least two of the following parameters, one of which must be abnormal temperature or leukocyte count: hyperthermia or hypothermia (>38.5 °C or <36 °C), tachycardia (defined as a mean heart rate more than two standard deviations above normal for age) or bradycardia for children less than 1 year old (defined as a mean heart rate < 10th percentile for age), tachypnea (mean respiratory rate more than two standard deviations above normal for age), leukocyte count elevated or depressed for age, or >10% immature neutrophils [5].
Sepsis has been categorized in the neonatal period as early onset sepsis (EOS) and late onset sepsis (LOS) if occurring in the first 72 h after birth or later. The main risk factors and the pathogens associated are different, being in EOS chorioamnionitis, bacterial colonization of the birth canal, Group B streptococci (GBS) and Escherichia coli; in LOS healthcare acquired infections, preterm delivery and Coagulase negative streptococci [6].
The diagnosis of sepsis is made in children with SIRS in presence of a proven infection by a positive blood culture, or probable infection by a complete and often a posteriori review of clinical, laboratory and radiological data [2, 4, 5]. Blood culture is currently the reference standard for the confirmation of the diagnosis of sepsis. However, even if it represents a fundamental tool for the etiologic diagnosis and for the establishment of a targeted therapy, it has important and significant limitations, such as the time delay in obtaining results and a high percentage of false negatives [7, 8]. Delay in antibiotic treatment of infected children is associated with a significant risk in terms of mortality and morbidity [6].
Biomarkers can play an important role in providing a timely diagnosis of sepsis, helping the differential diagnosis with non-infectious SIRS and the decision-making in the initial management. In paediatrics, the most frequently employed biomarker to differentiate sepsis from non-infectious SIRS is the C-reactive protein (CRP), which, however, is highly non-specific and has an unfavourable kinetics [9]. Among the different molecules investigated as biomarkers of sepsis, procalcitonin (PCT) seems to be one of the most promising [10,11,12]. PCT is a 116-aminoacids pro-hormone, physiologically produced by thyroid C-cells as precursor of calcitonin, an acute phase protein secreted by several tissues in response to various endogenous and exogenous stimuli such as cytokines and lipopolysaccharide, acting as a chemo-attractant factor on blood monocytes [13]. In healthy neonates, plasma PCT values increase gradually after birth, reach peak values after 24 h of age (mean 1.5-2.5 ng/ml, range 0.1-20 ng/ml) and then decrease to normal values below 0.5 ng/ml by 48-72 h of age. A number of studies in children and neonates after 72 h of age, demonstrated that PCT values less than 0.5 ng/ml seem to be normal; increases to 0.5-2 ng/ml seem to be related to non-infectious inflammation, viral or focal bacterial infections; increases above a PCT value of 2-2.5 ng/ml, seem to be related to bacterial or fungal systemic infections [14,15,16]. PCT as a diagnostic biomarker for sepsis in individuals with SIRS has been well evaluated in adults [11, 17,18,19,20,21,22,23,24,25]. Various meta-analyses in paediatric age groups have been done so far [16, 26, 27], but no one has evaluated the role of PCT in sepsis for children and neonates with SIRS or suspected sepsis, the most useful setting for clinicians. Therefore, our objective was to assess the diagnostic accuracy of PCT to differentiate between sepsis and systematic inflammatory response syndromes of non-infectious origin in children and neonates with suspected sepsis.
Methods
The protocol for this review was accepted and registered on PROSPERO international prospective register of systematic reviews under the number CRD42016033809.
Search strategy
We searched Medline/Pubmed, Embase, ISI Web of Science, CINAHL, Cochrane Library, for studies that assessed the accuracy of PCT for the diagnosis of sepsis in neonates and in children over 44 weeks, defined as “paediatric age”. The search algorithm used for each database is available in the Additional file 1. No start date limit was used and the search strategy was performed in August 2014 and updated until the cut off date of December 2015. To expand our search, reference lists of the retrieved articles were also screened for additional studies. We also searched grey literature through Open Sigle. No language limits were applied.
Selection criteria
We included all studies regardless of study design: prospective or retrospective that met the following criteria: assessing the accuracy of PCT for diagnosis of sepsis in children and neonates with SIRS or suspected sepsis, providing sensitivity (true-positive rate) and specificity (true-negative rate). The presence of infection had to be microbiologically confirmed (positive culture, microscopy or polymerase chain reaction) or evaluated as probable by chart review.
We excluded: a) articles not regarding sepsis or not assessing PCT; b) studies not in children or neonates; c) studies using only healthy children or neonates as controls; d) studies on children or neonates without probable infection; e) review articles, editorials or letters, expert opinions, comments and animal experiments.
At least two reviewers independently evaluated titles and abstracts and selected relevant studies for inclusion. If this could not be done reliably by title and abstract, the full text version was retrieved. Any disagreement was resolved by discussion within reviewers, or by an independent reviewer. Reason for exclusion of studies was recorded.
Data extraction
Data about the following variables were extracted independently by at least two reviewers: year of publication, clinical setting (neonatal or paediatric intensive care unit, or general ward), age at diagnosis, sample size, design of the study, prevalence of sepsis, laboratory methods, cut-off points, timing of tests, inclusion criteria (SIRS or suspected sepsis), outcome diagnosis (sepsis confirmed by microbiological test or by chart review) and when reported, the main measures of test accuracy. Any disagreement on data extraction was resolved by consensus.
Quality assessment
The methodological quality of each study was assessed using a checklist based on criteria adapted from the Cochrane Collaboration guidelines and the Quality Assessment Tool for Diagnostic Accuracy Studies (QUADAS-2 score) and applied to each included study. QUADAS-2 is made of four domains: patient selection, index test, reference standard, flow and timing. Each domain evaluates the risk of bias and for the first three there is also an assessment of applicability. Signalling questions are included to help in the judgement about risk of bias [28]. Each question was assessed by scoring it as “yes”, “no”, or “unclear” and the risks of bias and the concerns on applicability were scored as “high”, “low” or “unclear”, depending on the answers of the signalling questions. At least two authors scored independently, and differences were resolved by consensus or by a third reviewer.
Statistical analysis
We extracted information on true positives (tp), false negatives (fn), false positives (fp), and true negatives (tn) for each study. We carried out primary analyses considering neonates and children as two different groups. We then conducted further analyses on neonates with suspected EOS as a stand-alone group and on neonates with suspected LOS and children grouped together. We used two-by-two data in order to calculate sensitivities and specificities, along with their 95% confidence intervals. They were graphically evaluated by using forest plots and by plotting study results in ROC space.
Studies were divided into subgroups depending on the specific PCT cut-off considered in their test accuracy analyses. We grouped the studies according to three different PCT ranges: <2 ng/L; 2-2,5 ng/L; >2,5 ng/L on the basis of preliminary observational studies and PCT nomograms [14, 29]. These nomograms showed differences between neonatal and paediatric cut-off values of PCT in healthy populations. Moreover, the 2-2.5 ng/ml cut-off was chosen as proposed by the Expert Meeting on Neonatal and Paediatric Sepsis of European Medicines Agency [30]. If a study reported results at different cut-offs, we chose one of them for each subgroup.
If adequate data were available, meta-analyses were performed by using the bivariate model [31] to produce summary sensitivities and specificities. A random-effects model jointly synthesizes sensitivity and specificity by allowing for correlation between them across studies. Average operating points, along with their confidence and predictive regions for each subgroup were calculated whenever possible (i.e. they were not calculated if there were less than three studies in a subgroup). Heterogeneity was graphically evaluated [32]; where heterogeneity was high, the 95% prediction region was much larger than the 95% confidence region. All analyses were performed using Review Manager [33] and STATA 13 software [34].
Results
Selected studies
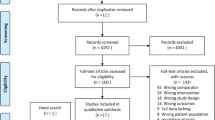
The literature search generated 993 articles. After reviewing the titles and abstracts, we excluded 807 studies, because they were either reviews or studies in adults or not focused on sepsis or using only healthy subjects as controls. A total of 186 studies were retrieved in full text and assessed for eligibility. Of these 169 were excluded due to their poor design and/or because of identified biases, mostly spectrum bias, or because SIRS was not among the inclusion criteria. Indeed, many studies have been focusing on PCT for the diagnosis of serious bacterial infections such as pneumonia, meningitis or pyelonephritis, but not SIRS and sepsis. In total, 17 studies comprising 1408 patients (1086 neonates and 322 children) were included in the qualitative and quantitative analysis. Of these, 13 studies were in neonates, 3 studies were in children, while one study included both [35]. The selection of the studies has been summarized in the flow chart (see Fig. 1).

Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow chart. Literature search and selection. *One study assessed both neonates and children over 44 weeks of gestational age
Study characteristics
We split the studies in two groups according to age: neonatal [35,36,37,38,39,40,41,42,43,44,45,46,47,48] and paediatric [35, 49,50,51]. Moreover, we stratified the data in subgroups according to the cut-off considered in the primary study. PCT cut-offs varied, ranging from 0.5 ng/ml [39, 43] to 25 ng/ml [37] in the neonatal group, and from 0.28 ng/ml [35] to 10 ng/ml [52] in the paediatric group. The study design was prospective for both neonatal and paediatric age, with the only exception of a retrospective cross-sectional study [45] in the neonatal age group. The setting of the studies was uniform, being mostly neonatal or paediatric intensive care units, with the exception of four studies [41, 45, 49, 51] in which patients were treated in hospital wards. Most of the studies (15 out of 17) used a qualitative semi-manual PCT assay. The characteristics of the included studies considering neonates and older children are presented respectively in Table 1 and in Table 2. The judgments on the methodological quality of the included studies according to the QUADAS-2 assessments [28] are presented in the Additional file 2.
Data synthesis in neonatal age
Meta-analytic results show that when using a PCT cut-off of between 2.0 and 2.5 ng/ml, pooled sensitivity is 0.85 (95% CI 0.76; 0.90) and pooled specificity is 0.54 (95% CI 0.38; 0.70) (see Table 3). Figure 2 shows study results in neonates plotted in the ROC space, broken down by cut-off subgroups with the 95% confidence interval and predictive regions for the summary sensitivity and specificity. The data extracted for the analysis are presented extensively in the Additional file 3. The forest plot for neonatal age is presented in the Additional file 4. When using a PCT cut-off of <2.0 ng/ml, pooled sensitivity is 0.84 (95% CI 0.75; 0.90) and pooled specificity is 0.51 (95% CI 0.37; 0.65). With a PCT cut-off of >2.5 ng/ml, pooled sensitivity is 0.68 (95% CI 0.52; 0.80) and pooled specificity is 0.85 (95% CI 0.70; 0.93). The Galbraith plot does not show heterogeneity among the results (see the Fig. 3). Plotting the studies divided by cut-off subgroups and neonatal EOS or LOS in the ROC suggests that PCT accuracy changes considerably depending on the onset: neonates with EOS need a higher PCT cut-off, while neonates with LOS require a lower PCT cut-off (see Additional file 5).

Representation in the ROC space of neonatal studies. Representation in the ROC space of studies on PCT for diagnosis of sepsis in neonatal age, divided by cut-off subgroup, and summary sensitivity and specificity points along with their 95% confidence and prediction regions. (ROC, receiver operating characteristic). Legend:  PCT neon – cut-off <2
PCT neon – cut-off <2  PCT neon – cut-off > 2.5
PCT neon – cut-off > 2.5  PCT neon – cut-off =2/2.5
PCT neon – cut-off =2/2.5

Galbraith plot. Heterogeneity of selected neonatal studies. Galbraith plot for neonatal studies. The standardised lnDOR = lnDOR/se was plotted (y-axis) against the inverse of the se (1/se) (x-axis). A regression line going through the origin was calculated, together with 95% boundaries (starting at +2 and −2 on the y-axis). (DOR, diagnostic odds ratio)
The additional analyses performed on the four studies which included only neonates with suspected EOS at a PCT cut-off of ≥2.5 ng/ml identified a pooled sensitivity of 0.75 (95% CI 0.64; 0.84), and a pooled specificity of 0.83 (95% CI 0.71; 0.91) (see Additional files 6 and 7).
Data synthesis in paediatric age
In the older patient group, it was only possible to meta-analyse studies using a PCT cut-off of <2.0 ng/ml: the pooled sensitivity was 0.78 (95% CI 0.66; 0.87) and the pooled specificity of 0.57 (95% CI 0.40; 0.73). Figure 4 shows the study results in the paediatric age in the ROC space, broken down by cut-off subgroups, along with the 95% confidence and predictive regions for pooled sensitivity and specificity. The Galbraith plot does not show heterogeneity among the results (see the Fig. 5). The data extracted for the analysis are presented extensively in the Additional file 8. The forest plot for paediatric age is presented in the Additional file 9. Grouping neonates with suspected LOS and paediatric patients together allows for the assessment of PCT accuracy at the only cut-off of <2 ng/ml: the pooled sensitivity was 0.79 (95% CI 0.71; 0.85); the pooled specificity was 0.63 (95% CI 0.48; 0.75) (see the Additional file 10 and the Additional file 11).

Representation in the ROC space of paediatric studies. Representation in the ROC space of the studies of PCT for diagnosis of sepsis in paediatric age, divided by cut-off subgroup, and summary sensitivity and specificity points along with their 95% confidence and prediction regions. (ROC, receiver operating characteristic). Legend:  PCT paed – cut-off <2
PCT paed – cut-off <2  PCT paed – cut-off > 2.5
PCT paed – cut-off > 2.5  PCT paed – cut-off =2/2.5
PCT paed – cut-off =2/2.5

Galbraith plot. Heterogeneity of selected paediatric studies. Galbraith plot for paediatric studies. The standardised lnDOR = lnDOR/se was plotted (y-axis) against the inverse of the se (1/se) (x-axis). A regression line going through the origin was calculated, together with 95% boundaries (starting at +2 and −2 on the y-axis). (DOR, diagnostic odds ratio)
Discussion
This is the first systematic review assessing PCT accuracy for sepsis in neonates and children with suspected sepsis or SIRS excluding healthy subjects, and therefore providing more useful information for clinicians. According to our meta-analysis, PCT at the cut-off of 2-2.5 ng/ml shows the best sensitivity and moderate accuracy for the diagnosis of sepsis in neonates with suspected sepsis. The sensitivity is high, but associated with a low specificity. Even if suboptimal, this could be considered acceptable, because of the high mortality rate of the condition, and the need to maintain a low false negative ratio.
In neonates, the PCT cut-off of <2 ng/ml shows a high sensitivity with a low specificity, similar to those of cut-off of 2-2.5 ng/mL; the PCT cut-off of >2.5 ng/ml shows lower, unacceptable values for sensitivity, and higher specificity. It is noteworthy to consider that studies on EOS with a PCT cut-off <2 ng/ml were all grouped together with LOS, and the two studies focusing on LOS only [42, 47] found that the PCT at this cut-off had a better accuracy, higher specificity and similar sensitivity, if compared with studies grouping EOS and LOS. This suggests that the use of two different cut-offs could improve accuracy in these two populations: PCT cut-off could be higher for neonates with EOS than for neonates with LOS. This is consistent with existing studies on healthy neonates [14, 29]. It is important that in future studies on EOS the diagnostic value of age-adjusted PCT cut-offs will be assessed in association with other serum biomarkers [46, 53].
Unfortunately, at present, there are not enough studies to perform a meta-analysis on the diagnostic accuracy of PCT at the cut-off of 2-2.5 ng/ml in older children with suspected sepsis or SIRS. In this population, the results on the PCT cut off of <2.0 ng/ml show an overall moderate accuracy, but the limited sample size and quality of the studies included indicate that further studies are needed and no clinical recommendation is possible at this stage. Additional analyses that considered the few studies only on EOS, and grouped together LOS and paediatric patients cannot overcome this limitation.
The study showed limitations linked to the current methodology of primary sepsis research, such as the non-uniform definition of sepsis: some studies considered sepsis only if confirmed by positive blood culture, microscopy or polymerase chain reaction (microbiologically confirmed) while others considered also “probable sepsis”, after a complete review of the patient chart with assessment of clinical, radiological and laboratory data. We included studied that considered both microbiologically confirmed and probable sepsis, but they did not provide detailed information about how the infection was confirmed. In addition, blood samples were drawn without a precise timing (i.e. “at time of admission” or “before antibiotic therapy”, which do not necessarily coincide). Furthermore, the scarcity of studies differentiating EOS and LOS in neonates hampered a more specific and informative analysis.
In 2016, a new definition of sepsis attributing a primary role to organ dysfunction was proposed in adults, aiming to offer greater consistency for epidemiological studies and clinical trials [3]. In order to improve diagnosis and decrease the mortality of sepsis in neonatal and paediatric population, we need soon additional studies of high methodological quality, accounting the specificity of pathophysiology and age dependent variables.
Conclusions
In conclusion, in this study we show that PCT has an overall moderate accuracy for the diagnosis of sepsis in neonates with suspected sepsis at the cut-off of 2.0-2.5 ng/ml.
In order to deepen our scientific knowledge on the role of PCT in the diagnosis of neonatal and paediatric sepsis, larger, high quality studies are necessary. More specifically, we need studies responding to the Standards for Reporting of Diagnostic Accuracy (STARD) guidelines, with a previously published and registered protocol, and an adequate sample size. It would also be of paramount importance to include suspected sepsis and exclude healthy subjects, in order to provide more useful information for the clinicians, and be clearly able to differentiate neonates with EOS and LOS. An updated definition of sepsis for paediatric population, similarly to that one proposed for adults, which considers the different pathophysiology and age dependent variables and overrule the current heterogeneity is warranted.
Key messages
1. PCT shows a moderate diagnostic accuracy at the cut-off of 2-2.5 ng/ml for the diagnosis of sepsis in neonates with SIRS or suspected sepsis.
2. In neonates, the PCT values should be critically evaluated differentiating EOS and LOS.
3. Further studies with better methodological quality in older children with suspected sepsis evaluating the PCT cut-off of 2-2.5 ng/ml are warranted.
Abbreviations
- AUC:
-
Area under the curve
- CI:
-
Confidence interval
- CR:
-
Chart review
- CRP:
-
C-reactive protein
- EOS:
-
Early onset sepsis
- FN:
-
False negative
- FP:
-
False positive
- LOS:
-
Late onset sepsis
- MC:
-
Microbiologically confirmation
- NICU:
-
Neonatal intensive-care unit
- NPV:
-
Negative predictive value
- PCT LIA:
-
Procalcitonin immunoluminometric assay
- PCT:
-
Procalcitonin
- PCT-Q:
-
procalcitonin semiquantitative rapid assay
- PPV:
-
Positive predictive value
- QUADAS score:
-
Quality Assessment Tool for Diagnostic Accuracy Studies
- ROC:
-
Receiver operating characteristic
- SIRS:
-
Systemic inflammatory response syndrome
- STARD:
-
Standard for Reporting of Diagnostic Accuracy
- TN:
-
True negative
- TP:
-
True positive
References
American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20(6):864–74.
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G, SCCM/ESICM/ACCP/ATS/SIS. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit Care Med. 2003;31(4):1250–6.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–10.
Reinhart K, Bauer M, Riedemann NC, Hartog CS. New approaches to sepsis: molecular diagnostics and biomarkers. Clin Microbiol Rev. 2012;25(4):609–34.
Goldstein B, Giroir B, Randolph A. International consensus conference on Paediatric sepsis: international paediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in paediatrics. Pediatr Crit Care Med. 2005;6(1):2–8.
Plunkett A, Tong J. Sepsis in children. BMJ. 2015 Jun 9;350:h3017.
Carrigan SD, Scott G, Tabrizian M. Toward resolving the challenges of sepsis diagnosis. Clin Chem. 2004;50(8):1301–14.
Sands KE, Bates DW, Lanken PN, Graman PS, Hibberd PL, Kahn KL, Parsonnet J, Panzer R, Orav EJ, Snydman DR, Black E, Schwartz JS, Moore R, Johnson Jr BL, Platt R, Academic Medical Center Consortium Sepsis Project Working Group. Epidemiology of sepsis syndrome in 8 academic medical centers. JAMA. 1997;278(3):234–40.
Povoa P, Coelho L, Almeida E, Fernandes A, Mealha R, Moreira P, Sabino H. C-reactive protein as a marker of infection in critically ill patients. Clin Microbiol Infect. 2005;11(2):101–8.
Pacifico L, Osborn JF, Natale F, Ferraro F, De Curtis M, Chiesa C. Procalcitonin in paediatrics. Adv Clin Chem. 2013;59:203–63.
Rowland T, Hilliard H, Barlow G. Procalcitonin: potential role in diagnosis and management of sepsis. Adv Clin Chem. 2015;68:71–86.
Pontrelli G, De Crescenzo F, Buzzetti R, Calò Carducci F, Jenkner A, Amodio D, De Luca M, Chiurchiù S, Haf Davies E, Simonetti A, Ferretti E, Della Corte M, Gramatica L, Livadiotti S, Rossi P. Diagnostic value of soluble triggering receptor expressed on myeloid cells in paediatric sepsis: a systematic review. Ital J Pediatr. 2016; in press
Fendler WM, Piotrowski AJ. Procalcitonin in the early diagnosis of nosocomial sepsis in preterm neonates. J Paediatr Child Health. 2008;44(3):114–8.
Chiesa C, Panero A, Rossi N, Stegagno M, De Giusti M, Osborn JF, Pacifico L. Reliability of procalcitonin concentrations for the diagnosis of sepsis in critically ill neonates. Clin Infect Dis. 1998;26(3):664–72.
Gendrel D, Assicot M, Raymond J, Moulin F, Francoual C, Badoual J, Bohuon C. Procalcitonin as a marker for the early diagnosis of neonatal infection. J Pediatr. 1996;128(4):570–3.
van Rossum AM, Wulkan RW, Oudesluys-Murphy AM. Procalcitonin as an early marker of infection in neonates and children. Lancet Infect Dis. 2004;4(10):620–30.
Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis. 2013;13(5):426–35.
Tang BM, Eslick GD, Craig JC, McLean AS. Accuracy of procalcitonin for sepsis diagnosis in critically ill patients: systematic review and meta-analysis. Lancet Infect Dis. 2007;7(3):210–7.
Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohuon C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet. 1993;341(8844):515–8.
Garnacho-Montero J, Huici-Moreno MJ, Gutierrez-Pizarraya A, Lopez I, Marquez-Vacaro JA, Macher H, Guerrero JM, Puppo-Moreno A. Prognostic and diagnostic value of eosinopenia, C-reactive protein, procalcitonin, and circulating cell-free DNA in critically ill patients admitted with suspicion of sepsis. Crit Care. 2014;18(3):R116.
Masson S, Caironi P, Spanuth E, Thomae R, Panigada M, Sangiorgi G, Fumagalli R, Mauri T, Isgro S, Fanizza C, Romero M, Tognoni G, Latini R, Gattinoni L, ALBIOS Study Investigators. Presepsin (soluble CD14 subtype) and procalcitonin levels for mortality prediction in sepsis: data from the albumin Italian outcome sepsis trial. Crit Care. 2014;18(1):R6.
Prkno A, Wacker C, Brunkhorst FM, Schlattmann P. Procalcitonin-guided therapy in intensive care unit patients with severe sepsis and septic shock--a systematic review and meta-analysis. Crit Care. 2013;17(6):R291.
Uzzan B, Cohen R, Nicolas P, Cucherat M, Perret GY. Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: a systematic review and meta-analysis. Crit Care Med. 2006;34(7):1996–2003.
Kibe S, Adams K, Barlow G. Diagnostic and prognostic biomarkers of sepsis in critical care. J Antimicrob Chemother. 2011;66(Suppl 2):ii33–40.
Gattas DJ, Cook DJ. Procalcitonin as a diagnostic test for sepsis: health technology assessment in the ICU. J Crit Care. 2003;18(1):52–8.
Simonsen KA, Anderson-Berry AL, Delair SF, Davies HD. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014;27(1):21–47.
Vouloumanou EK, Plessa E, Karageorgopoulos DE, Mantadakis E, Falagas ME. Serum procalcitonin as a diagnostic marker for neonatal sepsis: a systematic review and meta-analysis. Intensive Care Med. 2011;37(5):747–62.
Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA, Bossuyt PM, QUADAS-2 Group. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011 Oct 18;155(8):529–36.
Turner D, Hammerman C, Rudensky B, Schlesinger Y, Goia C, Schimmel MS. Procalcitonin in preterm infants during the first few days of life: introducing an age related nomogram. Arch Dis Child Fetal Neonatal Ed. 2006;91(4):F283–6.
Rossi P, Botgros R, et al. Report on the expert meeting on neonatal and Paediatric sepsis. 2010. http://www.ema.europa.eu/docs/en_GB/document_library/Report/2010/12/WC500100199.pdf
Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol. 2005;58(10):982–90.
Macaskill P, Gatsonis C, Deeks JJ, Harbord RM, Takwoingi Y. Chapter 10: Analysing and Presenting Results. In: Deeks JJ, Bossuyt PM, Gatsonis C, editors. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy Version 1.0. The Cochrane Collaboration, 2010. Available from: http://srdta.cochrane.org/.
RevMan [Computer program]. Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012. http://community.cochrane.org/tools/review-production-tools/revman-5/about-revman-5.
StataCorp. Stata statistical software: release 13. College Station: StataCorp LP; 2013.
Groselj-Grenc M, Ihan A, Pavcnik-Arnol M, Kopitar AN, Gmeiner-Stopar T, Derganc M. Neutrophil and monocyte CD64 indexes, lipopolysaccharide-binding protein, procalcitonin and C-reactive protein in sepsis of critically ill neonates and children. Intensive Care Med. 2009;35(11):1950–195836.
Adib M, Bakhshiani Z, Navaei F, Saheb Fosoul F, Fouladi S, Kazemzadeh H. Procalcitonin: a reliable marker for the diagnosis of neonatal sepsis. Iran J Basic Med Sci. 2012;15(2):777–82.
Bender L, Thaarup J, Varming K, Krarup H, Ellermann-Eriksen S, Ebbesen F. Early and late markers for the detection of early-onset neonatal sepsis. Dan Med Bull. 2008;55(4):219–23.
Bonac B, Derganc M, Wraber B, Hojker S. Interleukin-8 and procalcitonin in early diagnosis of early severe bacterial infection in critically ill neonates. Pflugers Arch. 2000;440(5 Suppl):R72–4.
Boo NY, Nor Azlina AA, Rohana J. Usefulness of a semi-quantitative procalcitonin test kit for early diagnosis of neonatal sepsis. Singap Med J. 2008;49(3):204–8.
Guibourdenche J, Bedu A, Petzold L, Marchand M, Mariani-Kurdjian P, Hurtaud-Roux MF, Aujard Y, Porquet D. Biochemical markers of neonatal sepsis: value of procalcitonin in the emergency setting. Ann Clin Biochem. 2002;39(Pt 2):130–5.
Koskenvuo MM, Irjala K, Kinnala A, Ruuskanen O, Kero P. Value of monitoring serum procalcitonin in neonates at risk of infection. Eur J Clin Microbiol Infect Dis. 2003;22(6):377–8.
Lopez Sastre JB, Perez Solis D, Roques Serradilla V, Fernandez Colomer B, Coto Cotallo GD, Krauel Vidal X, Narbona Lopez E, Garcia del Rio M, Sanchez Luna M, Belaustegui Cueto A, Moro Serrano M, Urbon Artero A, Alvaro Iglesias E, Cotero Lavin A, Martinez Vilalta E, Jimenez Cobos B, Grupo de Hospitales Castrillo. Procalcitonin is not sufficiently reliable to be the sole marker of neonatal sepsis of nosocomial origin. BMC Pediatr. 2006;6:16.
Naher BS, Mannan MA, Noor K, Shahiddullah M. Role of serum procalcitonin and C-reactive protein in the diagnosis of neonatal sepsis. Bangladesh Med Res Counc Bull. 2011;37(2):40–6.
Resch B, Gusenleitner W, Muller WD. Procalcitonin and interleukin-6 in the diagnosis of early-onset sepsis of the neonate. Acta Paediatr. 2003;92(2):243–5.
Sakha K, Husseini MB, Seyyedsadri N. The role of the procalcitonin in diagnosis of neonatal sepsis and correlation between procalcitonin and C-reactive protein in these patients. Pak J Biol Sci. 2008;11(14):1785–90.
Schlapbach LJ, Graf R, Woerner A, Fontana M, Zimmermann-Baer U, Glauser D, Giannoni E, Roger T, Muller C, Nelle M, Stocker M. Pancreatic stone protein as a novel marker for neonatal sepsis. Intensive Care Med. 2013;39(4):754–73.
Vazzalwar R, Pina-Rodrigues E, Puppala BL, Angst DB, Schweig L. Procalcitonin as a screening test for late-onset sepsis in preterm very low birth weight infants. J Perinatol. 2005;25(6):397–402.
Zahedpasha Y. AhmadpourKacho M, Hajiahmadi M, Haghshenas M. Procalcitonin as a marker of neonatal sepsis. Iran J Paediatric. 2009;19(2):117–22.
Calo Carducci FI, Aufiero LR, Folgori L, Vittucci AC, Amodio D, De Luca M, Li Pira G, Bergamini A, Pontrelli G, Finocchi A, D'Argenio P. Serum soluble ST2 as diagnostic marker of systemic inflammatory reactive syndrome of bacterial etiology in children. Pediatr Infect Dis J. 2014;33(2):199–203.
Simon L, Saint-Louis P, Amre DK, Lacroix J, Gauvin F. Procalcitonin and C-reactive protein as markers of bacterial infection in critically ill children at onset of systemic inflammatory response syndrome. Pediatr Crit Care Med. 2008;9(4):407–13.
Pourakbari B, Mamishi S, Zafari J, Khairkhah H, Ashtiani MH, Abedini M, Afsharpaiman S, Rad SS. Evaluation of procalcitonin and neopterin level in serum of patients with acute bacterial infection. Braz J Infect Dis. 2010;14(3):252–5.
Arkader R, Troster EJ, Lopes MR, Júnior RR, Carcillo JA, Leone C, Okay TS. Procalcitonin does discriminate between sepsis and systemic inflammatory response syndrome. Arch Dis Child. 2006;91(2):117–20.
He Y, Du WX, Jiang HY, Ai Q, Feng J, Liu Z, Yu JL. Multiplex cytokine profiling identifies interleukin-27 as a novel biomarker for neonatal early onset sepsis. Shock. 2017 Feb;47(2):140–7.
Acknowledgments
The research leading to these results has received funding from the European Union’s Seventh Framework Programme for research, technological development and demonstration under grant agreement no. 261060 (Global Research in Paediatrics – GRiP network of excellence).
Funding
The research leading to these results has received funding from the European Union’s Seventh Framework Programme for research; technological development and demonstration under grant agreement no. 261060 (Global Research in Paediatrics – GRiP network of excellence).
Availability of data and materials
This study is a systematic review. The primary studies are available in literature, and the summary tables have been included in or attached to the present manuscript.
Authors’ contributions
GP, SL, PR, conceived of the study, and participated in its design and coordination and helped to draft the manuscript. FDC, RB performed the search strategy, extracted the data, provided methodological support and drafted the manuscript. RB, SB performed the statistical analyses. DA, MDL, SC, EF, VDF, VR, MDC, LG screened the search results, extracted the data and drafted the manuscript. AJ, FCC, EHD, AS, VDF, GC, participated in this study design, gave clinical expertise and revised thoroughly the drafted manuscript. MC revised the paper and participated in the new analyses in the review phase. All authors read and approved the final manuscript.
Competing interests
The author(s) declare that they have no competing interests.
Consent for publication
The authors provided their consent for publication.
Ethics approval and consent to participate
This study is a systematic review. The primary studies evaluated included a statement on ethics approval and consent.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional files
Additional file 1:
Search strategy. (PDF 54 kb)
Additional file 2:
Table of bias. Table of bias of neonatal and paediatric studies according to QUADAS-2. (PDF 84 kb)
Additional file 3:
Table of included neonatal studies. CR, Chart review; DOR, diagnostic odds ratio; LR +, positive likelihood ratio; LR -, negative likelihood ratio; MC, Microbiologically confirmation; PCT, procalcitonin; SIRS, systemic inflammatory response syndrome; MC (Microbiologically confirmation). (PDF 130 kb)
Additional file 4:
Forest plot of studies on PCT for diagnosis of sepsis in neonatal age. The forest plot represents in each study the sensitivity and the specificity of PCT, together with the 95% CI for diagnosis of sepsis in neonatal age stratified according cut-off subgroup. (CI, confidence interval; FP, false positive; FN, false negative; PCT, procalcitonin; TP, true positive; TN, true negative). (PDF 743 kb)
Additional file 5:
Representation in the ROC space of neonatal studies divided in EOS and LOS. Representation in the ROC space of studies on PCT for diagnosis of sepsis in neonatal age, divided by cut-off subgroup and EOS/LOS. (ROC, receiver operating characteristic). (PDF 46 kb)
Additional file 6:
Forest plot and summary statistics of studies on PCT for diagnosis of EOS. The forest plot represents in each study the sensitivity and the specificity of PCT, together with the 95% CI for diagnosis of EOS. (CI, confidence interval; FP, false positive; FN, false negative; PCT, procalcitonin; TP, true positive; TN, true negative). (PDF 323 kb)
Additional file 7:
Representation in the ROC space of studies in EOS. Representation in the ROC space of studies on PCT for diagnosis of EOS. (ROC, receiver operating characteristic). (PDF 157 kb)
Additional file 8:
Table of included paediatric studies. (DOR, diagnostic odds ratio; LR+, positive likelihood ratio; LR-, negative likelihood ratio; PCT, procalcitonin; SIRS, systemic inflammatory response syndrome; MC, Microbiologically confirmation; CR Chart Review). (PDF 19 kb)
Additional file 9:
Forest plot of studies on PCT for diagnosis of sepsis in paediatric age. The forest plot represents in each study the sensitivity and the specificity of PCT, together with the 95% CI for diagnosis of sepsis in paediatric age stratified according cut-off subgroup. (PDF 377 kb)
Additional file 10:
Forest plot and summary statistics of studies on PCT for diagnosis of LOS and paediatric sepsis. The forest plot represents in each study the sensitivity and the specificity of PCT, together with the 95% CI for diagnosis of LOS and paediatric sepsis. (CI, confidence interval; FP, false positive; FN, false negative; PCT, procalcitonin; TP, true positive; TN, true negative). (PDF 337 kb)
Additional file 11:
Representation in the ROC space of studies in LOS and paediatric sepsis. Representation in the ROC space of studies on PCT for diagnosis in LOS and paediatric sepsis. (PDF 154 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Pontrelli, G., De Crescenzo, F., Buzzetti, R. et al. Accuracy of serum procalcitonin for the diagnosis of sepsis in neonates and children with systemic inflammatory syndrome: a meta-analysis. BMC Infect Dis 17, 302 (2017). https://doi.org/10.1186/s12879-017-2396-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-017-2396-7