
Abstract
Purpose
Early-onset sepsis (EOS) is one of the main causes for the admission of newborns to the neonatal intensive care unit. However, traditional infection markers are poor diagnostic markers of EOS. Pancreatic stone protein (PSP) is a promising sepsis marker in adults. The aim of this study was to investigate whether determining PSP improves the diagnosis of EOS in comparison with other infection markers.
Methods
This was a prospective multicentre study involving 137 infants with a gestational age of >34 weeks who were admitted with suspected EOS. PSP, procalcitonin (PCT), soluble human triggering receptor expressed on myeloid cells-1 (sTREM-1), macrophage migration inhibitory factor (MIF) and C-reactive protein (CRP) were measured at admission. Receiver-operating characteristic (ROC) curve analysis was performed.
Results
The level of PSP in infected infants was significantly higher than that in uninfected ones (median 11.3 vs. 7.5 ng/ml, respectively; p = 0.001). The ROC area under the curve was 0.69 [95 % confidence interval (CI) 0.59–0.80; p < 0.001] for PSP, 0.77 (95 % CI 0.66–0.87; p < 0.001) for PCT, 0.66 (95 % CI 0.55–0.77; p = 0.006) for CRP, 0.62 (0.51–0.73; p = 0.055) for sTREM-1 and 0.54 (0.41–0.67; p = 0.54) for MIF. PSP independently of PCT predicted EOS (p < 0.001), and the use of both markers concomitantly significantly increased the ability to diagnose EOS. A bioscore combining PSP (>9 ng/ml) and PCT (>2 ng/ml) was the best predictor of EOS (0.83; 95 % CI 0.74–0.93; p < 0.001) and resulted in a negative predictive value of 100 % and a positive predictive value of 71 %.
Conclusions
In this prospective study, the diagnostic performance of PSP and PCT was superior to that of traditional markers and a combination bioscore improved the diagnosis of sepsis. Our findings suggest that PSP is a valuable biomarker in combination with PCT in EOS.
Similar content being viewed by others

Introduction
While the implementation of intrapartum antibiotic prophylaxis has led to a significant decline of group B streptococcal (GBS) neonatal sepsis [1, 2], morbidity and mortality due to early-onset sepsis (EOS, presenting within 72 h of age) remain high. The incidence of EOS in term infants in developed countries is currently 0.5 per 1,000 live births, with a case fatality rate of 2 %. In preterm babies, the incidence is as high as 5 per 1,000 live births with a mortality reaching 25 % [2–5]. EOS is one of the main reasons for admitting term babies to the neonatal intensive care unit (NICU) and therefore imposes a considerable economic burden on the healthcare system [6]. It is crucial to promptly identify infants with EOS, since delaying antibiotic treatment is associated with neurologic impairment and increased mortality [7, 8]. Due to the lack of specific clinical signs, infection markers are commonly used to guide clinical decisions to initiate or stop empiric antibiotic treatment [6]. However, the positive and negative predictive values (PPV, NPV, respectively) of commonly used infection markers, such as C-reactive protein (CRP), white blood cell count (WBC) and immature by total ratio (I/T ratio) to diagnose EOS are poor [9]. Combination biomarker scores have been proposed to overcome the limitations inherent to many sepsis markers [10]. Some of the most promising marker candidates are procalcitonin (PCT), soluble triggering receptor expressed on myeloid cells-1 (sTREM-1), macrophage migration inhibitory factor (MIF) and pancreatic stone protein (PSP). PCT, a calcitonin precursor peptide of unknown physiological function, has become an established sepsis marker in adults and children [11]. PCT is known to show a physiological increase during the first days of life [9]. sTREM-1 is the soluble form of a receptor expressed on most phagocytic cells, and it becomes highly upregulated during sepsis [12, 13]. MIF is a pro-inflammatory mediator that is elevated in septic patients [14–16]. PSP has recently emerged as a promising sepsis marker in adults, with high PSP levels predicting sepsis, sepsis-associated multiple-organ failure and mortality [17, 18]. However, no data are available on PSP in the clinical setting of neonatal sepsis.
The aim of our study was to investigate the performance of novel sepsis markers in neonates with EOS and to determine whether a combination bioscore improves the diagnosis of EOS.
Methods
Study subjects
This study is a subset study based on the prospective, randomized-controlled multicentre Neonatal Procalcitonin Intervention Study (NeoPInS; see http://www.clinicaltrials.gov; Trial no. NCT00854932) [19]. Patients were recruited between 1 July 2009 and 31 December 2010 in three Swiss NICUs (University Children’s Hospital Bern; Children’s Hospital Lucerne; Department of Pediatrics, Cantonal Hospital Winterthur, Switzerland). Neonates born after 34 0/7 weeks who were admitted within the first 72 h of life to the NICU with suspicion of sepsis and empirically treated for EOS were eligible for enrolment in the study. At admission, blood was sampled and routine laboratory tests were performed for evaluation of neonatal infection (including CRP, PCT, I/T ratio and WBC count). Children with congenital malformations were excluded. The Ethics Committees of the Canton of Berne, Canton of Zurich and Canton of Lucerne, Switzerland, approved the study. Written consent from all parents of participating infants was obtained at enrolment.
Diagnosis of infection
The likelihood of infection was assessed at 24–72 h after admission into four categories based on culture results, perinatal sepsis risk factors, clinical signs of sepsis and laboratory test results [19]: (1) proven infection (positive blood or cerebrospinal fluid cultures), (2) probable infection (negative cultures, ≥3 abnormal findings), (3) possible infection (negative cultures, two abnormal findings) and (4) unlikely infection (negative cultures, single abnormal finding). The following factors were considered: (1) maternal risk factors (GBS positivity, prolonged rupture of membranes >18 h, chorioamnionitis), (2) clinical symptoms (respiratory distress/apnea, tachycardia/bradycardia, arterial hypotension/poor perfusion, seizures/irritability, lethargy/feeding intolerance, ileus), (3) results of conventional laboratory tests (WBC <5 × 109/l, CRP >10 mg/l, I/T ratio >0.2) and (4) results of blood and cerebrospinal fluid cultures.
For this marker study, we a priori defined an infected group (proven or probable infection) versus an uninfected group (possible or unlikely infection). This is in agreement with the study protocol that requires infants with proven or probable infection to be treated for at least 7 days, whereas treatment is usually stopped after 24–72 h in infants with possible or unlikely infection.
Blood sampling
A sample of venous blood (100 μl) was obtained upon admission of the infant to the NICU; this occurred simultaneously with sampling for blood cultures, CRP, WBC count and I/T ratio. Venous blood was taken by venipuncture from a peripheral vein or from the umbilical vein if an umbilical venous catheter was present. Samples were centrifuged directly after sampling for 6 min at 3,000 g, and the serum obtained was immediately frozen in sterile tubes at −80 °C. All measurements were performed when the study was finished.
In order to describe changes in PSP over the first days of life, we also measured PSP in cord blood of 56 uninfected neonates born after 34 weeks gestational age and postnatally in uninfected infants from this study, including sequential samples during the first 5 days of life. Cord blood was collected immediately after delivery of the child from the umbilical vein at the placental side of the cord.
Infection marker measurements
Procalcitonin
Plasma PCT concentrations were measured using a time-resolved amplified cryptate emission (TRACE) technology assay (Kryptor® PCT; BRAHMS, Hennigsdorf, Germany).
C-reactive protein
C-reactive protein was determined using the Tina-Quant C-Reactive Protein Gen 3 assay (Roche Diagnostics, Indianapolis, IN) on a Roche Modular P800 system. CRP levels below the detection limit were set at 1 mg/l for the analyses.
Macrophage migration inhibiting factor
The levels of MIF were measured by an enzyme-linked immunosorbent assay (ELISA) using the 4-span approach, as described previously [20]. Briefly, microtiter plates were coated with a duck anti-chicken antibody. Anti-human MIF polyclonal antibodies raised in chicken and rabbit were used as capture and trapping antibodies. A horseradish peroxidase-labeled goat anti-rabbit antibody (Sigma, St. Louis, MO) was used for detection, and recombinant human MIF was used as a standard. The analytical sensitivity of the human MIF ELISA was 39 pg/ml. Intrarun and interrun coefficients of variation were 6 and 12 %, respectively.
Soluble triggering receptor expressed on myeloid cells-1
Human serum sTREM-1 levels were determined by an in-house optimized ELISA using the anti-human TREM-1 monoclonal antibody clone 6B1.1G12 (generous gift from M. Radsak, University of Mainz, Germany [21]) at 10 μg/ml for coating and reagents from the Human TREM-1 Duoset (R&D Systems, Minneapolis, MN) for detection (according to manufacturers’ instructions).
Pancreatic stone protein
The levels of PSP were determined using an isoform-specific ELISA as previously described [18]. In brief, serum collected from the patient was incubated with guinea pig anti-human PSP/reg antibody precoated plates. Rabbit anti-human PSP/reg was added and subsequently detected by phosphatase-conjugated anti-rabbit immunoglobulin G. The detection limit was <0.1 ng/ml and the interplate variance was <10 %.
Statistical methods
Because of non-normal distributions, measurements are reported as medians and ranges. Correlations were assessed using Spearman’s rank test for univariate analyses and linear regression for multivariate analysis. Differences between the infected and uninfected groups were assessed using the Mann–Whitney test. Receiver-operating characteristic (ROC) curve analysis was used to assess the performance of each test. Optimal cut-offs were evaluated based on ROC curves using the Yuden’s index. Sepsis markers with a significance of p < 0.10 were included in the biomarker score models. The bioscore was based on a scoring system which attributed one point for each biomarker with a value above the cut-off point. Bioscores were constructed using two, three and four sepsis markers. In addition, we performed multivariate logistic regression analyses to investigate the strength of association between sepsis markers or bioscore models with EOS. Models were adjusted for gestational age, birth weight, sex and postnatal age at study sampling. Sensitivity analyses were performed comparing PSP levels in infected infants with those in (1) healthy newborns (cord blood) and (2) the subgroup of included infants with unlikely infection; both confirmed the main results (details not shown).
A p level <0.05 was considered to be significant. SPSS ver. 18.0 software was used (SPSS, Chicago, IL).
Results
Description of the study population
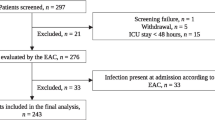
During the study period, 170 infants who met the inclusion criteria were admitted with suspected EOS. Fifteen patients could not be included due to lack of informed consent (10 parents denied consent, 5 were not approached), resulting in 155 infants eligible for entry into this marker study. In 18 infants, the amount of sampled blood was insufficient to perform additional laboratory analyses, leaving 137 infants in whom PSP was determined. No infant died. One infant required vasopressor support for septic shock. Three infants developed positive blood cultures, all with GBS. In total, 33/137 infants were classified as infected (including 3 with proven infection and 30 classified as probable infection), in contrast to 104 uninfected infants who were used as the control group (52 classified as possible infection and 52 as unlikely infection). Baseline characteristics of the infected versus the uninfected group are shown in Table 1. Of all infants enrolled in the study, 77 % were evaluated for EOS within 24 h after delivery and 96 % within 48 h after delivery.
PSP and infection markers in infected versus uninfected infants
In the 137 children included in the EOS study, the median PSP concentration was 8.8 [range 2.0–99.4, interquartile range (IQR) 5.2–13.3] ng/ml. PSP concentration was weakly correlated with birth weight (Spearman’s Rho 0.16; p = 0.08), gestational age (Rho 0.18; p = 0.03), male sex (Rho 0.16; p = 0.06) and postnatal age at study sampling (Rho 0.17; p = 0.04). PSP at admission correlated significantly with CRP at admission (Rho 0.35; p < 0.001), maximal CRP during hospitalization (Rho 0.46; p ≤ 0.001), PCT (Rho 0.23; p = 0.028), sTREM-1 (Rho 0.21; p = 0.025) and WBC count (Rho −0.23; p = 0.008), but not with MIF or I/T ratio. PSP was significantly higher in infected infants than in uninfected infants (median 11.3 vs. 7.5 ng/ml, respectively; Mann–Whitney p = 0.001; Fig. 1). Infected infants had significantly higher PCT than unifected infants (median 20.33 vs. 2.0 ng/ml, respectively; p < 0.001), higher CRP (6 vs. 1 mg/l, respectively; p = 0.004) and trendwise higher sTREM-1 levels (1,436 vs. 1,234 pg/ml, respectively; p = 0.055), while MIF levels, I/T ratio and WBC were not significantly different between the groups (p > 0.1).

Comparison of sepsis markers between infected and uninfected infants. Dashed lines Cut-offs used in this study. The medians with interquartile ranges (IQR) and p values (Mann–Whitney test) are shown. PSP Pancreatic stone protein, PCT procalcitonin, sTREM-1 soluble triggering receptor expressed on myeloid cells-1, MIF macrophage migration inhibitory factor, CRP C-reactive protein, WBC white blood cell count, I/T ratio immature by total neutrophil ratio
ROC curve analysis to diagnose EOS
Pancreatic stone protein and PCT performed best among all parameters studied to distinguish infected infants from uninfected infants (Table 2). The ROC area under the curve (AUC) was 0.69 [95 % confidence interval (CI) 0.59–0.80; p < 0.001] for PSP and 0.77 (95 % CI 0.66–0.87; p < 0.001) for PCT. The AUC was 0.66 (p = 0.006) for CRP and 0.62 for sTREM-1 (p = 0.055), whereas the AUC for the other markers studied were not significant. Based on ROC analyses, the optimal cut-off for each sepsis marker was defined and compared (Table 2). A cut-off for PSP of >9 ng/ml resulted in a sensitivity of 79 % and a specificity of 62 % with a NPV of 90 %.
Performance of bioscores to predict EOS
Based on the ROC curve analyses, PSP, PCT, sTREM-1 and CRP were included in the bioscore models. Bioscores were constructed using two, three or four sepsis markers (Table 2; Fig. 2). The bioscore based on PSP and PCT performed best in terms of distinguishing infected infants from uninfected infants, with an AUC of 0.83 (95 % CI 0.74–0.93; p < 0.001) and was superior to PCT or PSP alone. The combined PSP/PCT score had a NPV of 100 % if both markers were below the cut-off and a PPV of 71 % if both were positive.

Positive predictive values of different bioscores based on two (a), three (b) and four (c) sepsis markers with the corresponding 95 % confidence intervals (CI). Dashed line Regression line. PSP pancreatic stone protein, PCT procalcitonin, sTREM-1 soluble triggering receptor expressed on myeloid cells-1, CRP C-reactive protein
Multivariate logistic regression models showed that increased PSP and PCT were independent strong predictors of EOS (Table 3), while other markers were not significant. PSP showed the strongest association with EOS with an odds ratio (OR) of 26.4 (p < 0.001), followed by PCT (OR 7.9, p = 0.038). The bioscore based on PSP and PCT was significantly associated with EOS with an OR of 20.0 (p < 0.001) per increasing score. Again, the bioscore based on PSP and PCT performed similar to or better than the bioscores that included sTREM-1 or CRP, suggesting that neither sTREM-1 nor CRP provided additional independent information.
Changes in PSP concentrations over the first days of life
Finally, we investigated the changes in PSP serum concentration during the first days of life in uninfected infants. The median PSP concentration in cord blood was 6.2 ng/ml and increased slowly over the first days of life (median values in ng/ml; day 1: 7.2; day 2: 7.7; day 3: 10.3; day 4/5: 13.7; see Fig. 3). PSP concentrations at >48 h of life were significantly higher that that at <48 h of life (p < 0.01).

Changes in PSP levels during the first days of life. Line in boxes Median, boxes 25th and 75th percentiles, whiskers 5th and 95th percentile, dashed line cut-off of 9 ng/ml. p values of Mann–Whitney U test are shown
Discussion
In this prospective multicentre study on term and late preterm infants with EOS, we show that the diagnostic performance of PSP and PCT is superior to that of traditional sepsis markers and that a combination score may improve the diagnosis of sepsis. Our preliminary findings thus suggest that PSP is a valuable biomarker to diagnose EOS, especially in combination with PCT. To the best of our knowledge, this is the first study investigating PSP in neonatal sepsis.
EOS remains one of the leading causes of NICU admission in term and late preterm infants and causes an estimated 390 deaths annually in the USA [22]. However, overdiagnosis of EOS results in prolonged hospitalization, unnecessary exposure to the toxicity of aminoglycosides and a higher risk of necrotizing enterocolitis [23] and also favours the development of bacterial resistance. The use of sepsis markers may enable clinicians to safely reduce the duration of hospitalization and antibiotic treatment while improving early recognition of infants at high risk [6, 9, 24]. Several studies have reported the significantly superior performance of PCT in comparison to traditional sepsis markers in the diagnosis of late-onset sepsis [25–27]. However, the physiological increase of PCT during the first 48 h of life limits the performance of PCT in the setting of EOS [9]. This was demonstrated in a recent meta-analysis by Vouloumanou et al. who found that the AUC of PCT (0.95) was excellent to diagnose neonatal late-onset sepsis, but was less efficient (AUC 0.78; 95 % CI 0.74–0.81) for EOS [28]. Based on this rationale, we investigated whether a combination of novel markers could improve the diagnosis of EOS.
In our study, increased PSP levels were strongly associated with EOS independently of PCT and showed the strongest risk prediction in multivariate models. While the ROC curve analysis results were comparable between PSP and PCT, a bioscore combining PSP and PCT significantly improved the ability to diagnose EOS, with a NPV of 100 % if neither PCT nor PSP were positive, and a PPV of 71 % if both were positive. PSP has so far only been studied in adults; in these studies it was shown to accurately predict multi-organ failure and mortality in patients with ventilator-associated pneumonia and post-traumatic sepsis [17, 18]. Interestingly, maximum PSP levels in our study cohort were lower than those in adults with sepsis. We observed a slow increase in PSP concentrations over the first days of life. While this indicates that optimal PSP cut-offs may need to be adjusted over the first days of life, it is very unlikely that it relevantly affected our finding of increased PSP levels in infected infants: the age at blood sampling was not significantly different between infected and uninfected infants, and multivariate analyses were adjusted for age at blood sampling. In addition, the sensitivity analyses limited to neonates included <24 and <48 h of life confirmed the main results (not shown). Based on these preliminary results, we suggest that larger prospective trials are required to assess whether the combination of PCT and PSP can safely guide the decision to initiate or to stop empirical antibiotic treatment in infants with suspected EOS. We measured PSP in simultaneously obtained capillary heel-prick versus venous samples and found a good level of agreement (Rho 0.99, bias 3 %; details not shown), suggesting that capillary sampling for PSP is sufficiently accurate, which may facilitate further studies in neonates.
Although sTREM-1 was trendwise associated with EOS, sTREM-1 provided no additional independent information in the bioscore models. Sarafidis et al. recently reported elevated sTREM-1 levels in 52 newborns with suspected late-onset sepsis using a commercial assay [12]. The performance of sTREM-1 in our study was slightly weaker compared to their study. In contrast to PCT, PSP and sTREM-1, no significant difference was observed between MIF levels in infected versus non-infected newborns. In both groups, MIF levels were strikingly elevated compared to values reported in healthy adults and adults with septic shock [29]. This finding is in agreement with previous reports showing physiologically elevated MIF levels in healthy term and premature newborns [30]. The absence of a difference in MIF levels between the infected and the non-infected groups in our study may be due to the fact that septic shock was a rare event.
The strengths of this study include its protocol-based prospective multicentre design, the use of clearly defined clinical and laboratory criteria to diagnose EOS and the inclusion of several novel infection markers. We used combination biomarker score models to investigate whether combining infection markers increases diagnostic accuracy [10]. Notably, the sensitivity, specificity and AUC of PCT to diagnose EOS in our study obtained results that were very similar to those of a recent meta-analysis which reported pooled sensitivity for PCT of 76 % (95 % CI 68–82 %) with a specificity of 76 % (95 % CI 60–87 %) [28].
A limitation of this study is the low incidence of culture-proven EOS. The observed incidence of bacteremia is in agreement with data showing that culture-proven EOS represents only a small fraction of the total burden of EOS [5, 31]. A recent study reported that only 2.2 % of infants evaluated for suspected bacterial infection had proven bacteremia [32]. Exposure of neonates to maternal antibiotic treatment during labor and delivery increases the rate of false negative blood cultures. In addition, the small blood volumes collected when obtaining blood cultures (0.5–1.0 ml) and the high proportion of low colony count bacteremia result in a diminished sensitivity of blood cultures to diagnose sepsis [6, 33].
In conclusion, we report that combining PSP and PCT improved the diagnosis of EOS in comparison to PCT alone or to traditional sepsis markers. PSP represents a promising novel biomarker for neonatal sepsis. Future trials are needed to assess whether determining PSP and PCT in infants with EOS can reduce unnecessary antibiotic treatment and shorten hospital stay [24].
Abbreviations
- AUC:
-
Area under the curve
- CRP:
-
C-reactive protein
- EOS:
-
Early-onset sepsis
- I/T:
-
Immature by total ratio
- MIF:
-
Macrophage migration inhibiting factor
- PCT:
-
Procalcitonin
- PSP:
-
Pancreatic stone protein
- ROC:
-
Receiver-operating characteristic
- sTREM-1:
-
Soluble human triggering receptor expressed on myeloid cells-1
- WBC:
-
White blood cell count
References
Phares CR, Lynfield R, Farley MM, Mohle-Boetani J, Harrison LH, Petit S, Craig AS, Schaffner W, Zansky SM, Gershman K, Stefonek KR, Albanese BA, Zell ER, Schuchat A, Schrag SJ (2008) Epidemiology of invasive group B streptococcal disease in the United States, 1999–2005. JAMA 299:2056–2065
Stafford IA, Stewart RD, Sheffield JS, Wendel GD Jr, Sanchez PJ, McIntire DD, Roberts SW (2012) Efficacy of maternal and neonatal chemoprophylaxis for early-onset group B streptococcal disease. Obstet Gynecol 120:123–129
Stoll BJ, Hansen NI, Sanchez PJ, Faix RG, Poindexter BB, Van Meurs KP, Bizzarro MJ, Goldberg RN, Frantz ID 3rd, Hale EC, Shankaran S, Kennedy K, Carlo WA, Watterberg KL, Bell EF, Walsh MC, Schibler K, Laptook AR, Shane AL, Schrag SJ, Das A, Higgins RD (2011) Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics 127:817–826
Al-Taiar A, Hammoud MS, Cuiqing L, Lee JK, Lui KM, Nakwan N, Isaacs D (2012) Neonatal infections in China, Malaysia, Hong Kong and Thailand. Arch Dis Child Fetal Neonatal Ed [Epub ahead of print]
Kuhn P, Dheu C, Bolender C, Chognot D, Keller L, Demil H, Donato L, Langer B, Messer J, Astruc D (2010) Incidence and distribution of pathogens in early-onset neonatal sepsis in the era of antenatal antibiotics. Paediatr Perinat Epidemiol 24:479–487
Polin RA (2012) Management of neonates with suspected or proven early-onset bacterial sepsis. Pediatrics 129:1006–1015
Bassler D, Stoll BJ, Schmidt B, Asztalos EV, Roberts RS, Robertson CM, Sauve RS (2009) Using a count of neonatal morbidities to predict poor outcome in extremely low birth weight infants: added role of neonatal infection. Pediatrics 123:313–318
Kermorvant-Duchemin E, Laborie S, Rabilloud M, Lapillonne A, Claris O (2008) Outcome and prognostic factors in neonates with septic shock. Pediatr Crit Care Med 9:186–191
Stocker M, Fontana M, El Helou S, Wegscheider K, Berger TM (2010) Use of procalcitonin-guided decision-making to shorten antibiotic therapy in suspected neonatal early-onset sepsis: prospective randomized intervention trial. Neonatology 97:165–174
Gibot S, Bene MC, Noel R, Massin F, Guy J, Cravoisy A, Barraud D, De Carvalho Bittencourt M, Quenot JP, Bollaert PE, Faure G, Charles PE (2012) Combination biomarkers to diagnose sepsis in the critically ill patient. Am J Respir Crit Care Med 186:65–71
van Rossum AM, Wulkan RW, Oudesluys-Murphy AM (2004) Procalcitonin as an early marker of infection in neonates and children. Lancet Infect Dis 4:620–630
Sarafidis K, Soubasi-Griva V, Piretzi K, Thomaidou A, Agakidou E, Taparkou A, Diamanti E, Drossou-Agakidou V (2010) Diagnostic utility of elevated serum soluble triggering receptor expressed on myeloid cells (sTREM)-1 in infected neonates. Intensive Care Med 36:864–868
Jiyong J, Tiancha H, Wei C, Huahao S (2008) Diagnostic value of the soluble triggering receptor expressed on myeloid cells-1 in bacterial infection: a meta-analysis. Intensive Care Med 35(4):587–595
Calandra T, Roger T (2003) Macrophage migration inhibitory factor: a regulator of innate immunity. Nat Rev Immunol 3:791–800
Emonts M, Sweep FC, Grebenchtchikov N, Geurts-Moespot A, Knaup M, Chanson AL, Erard V, Renner P, Hermans PW, Hazelzet JA, Calandra T (2007) Association between high levels of blood macrophage migration inhibitory factor, inappropriate adrenal response, and early death in patients with severe sepsis. Clin Infect Dis 44:1321–1328
Calandra T, Echtenacher B, Roy DL, Pugin J, Metz CN, Hultner L, Heumann D, Mannel D, Bucala R, Glauser MP (2000) Protection from septic shock by neutralization of macrophage migration inhibitory factor. Nat Med 6:164–170
Boeck L, Graf R, Eggimann P, Pargger H, Raptis DA, Smyrnios N, Thakkar N, Siegemund M, Rakic J, Tamm M, Stolz D (2011) Pancreatic stone protein: a marker of organ failure and outcome in ventilator-associated pneumonia. Chest 140:925–932
Keel M, Harter L, Reding T, Sun LK, Hersberger M, Seifert B, Bimmler D, Graf R (2009) Pancreatic stone protein is highly increased during posttraumatic sepsis and activates neutrophil granulocytes. Crit Care Med 37:1642–1648
Stocker M, Hop WC, van Rossum AM (2010) Neonatal Procalcitonin Intervention Study (NeoPInS): effect of Procalcitonin-guided decision making on duration of antibiotic therapy in suspected neonatal early-onset sepsis: a multi-centre randomized superiority and non-inferiority Intervention Study. BMC Pediatr 10:89
Radstake TR, Sweep FC, Welsing P, Franke B, Vermeulen SH, Geurts-Moespot A, Calandra T, Donn R, van Riel PL (2005) Correlation of rheumatoid arthritis severity with the genetic functional variants and circulating levels of macrophage migration inhibitory factor. Arthritis Rheum 52:3020–3029
Radsak MP, Taube C, Haselmayer P, Tenzer S, Salih HR, Wiewrodt R, Buhl R, Schild H (2007) Soluble triggering receptor expressed on myeloid cells 1 is released in patients with stable chronic obstructive pulmonary disease. Clin Dev Immunol 2007:52040
Weston EJ, Pondo T, Lewis MM, Martell-Cleary P, Morin C, Jewell B, Daily P, Apostol M, Petit S, Farley M, Lynfield R, Reingold A, Hansen NI, Stoll BJ, Shane AJ, Zell E, Schrag SJ (2011) The burden of invasive early-onset neonatal sepsis in the United States, 2005–2008. Pediatr Infect Dis J 30:937–941
Cotten CM, Taylor S, Stoll B, Goldberg RN, Hansen NI, Sanchez PJ, Ambalavanan N, Benjamin DK Jr (2009) Prolonged duration of initial empirical antibiotic treatment is associated with increased rates of necrotizing enterocolitis and death for extremely low birth weight infants. Pediatrics 123:58–66
Kopterides P, Siempos II, Tsangaris I, Tsantes A, Armaganidis A (2010) Procalcitonin-guided algorithms of antibiotic therapy in the intensive care unit: a systematic review and meta-analysis of randomized controlled trials. Crit Care Med 38:2229–2241
Jacquot A, Labaune JM, Baum TP, Putet G, Picaud JC (2009) Rapid quantitative procalcitonin measurement to diagnose nosocomial infections in newborn infants. Arch Dis Child Fetal Neonatal Ed 94:F345–F348
Chiesa C, Panero A, Rossi N, Stegagno M, De Giusti M, Osborn JF, Pacifico L (1998) Reliability of procalcitonin concentrations for the diagnosis of sepsis in critically ill neonates. Clin Infect Dis 26:664–672
Auriti C, Fiscarelli E, Ronchetti MP, Argentieri M, Marrocco G, Quondamcarlo A, Seganti G, Bagnoli F, Buonocore G, Serra G, Bacolla G, Mastropasqua S, Mari A, Corchia C, Prencipe G, Piersigilli F, Rava L, Di Ciommo V (2011) Procalcitonin in detecting neonatal nosocomial sepsis. Arch Dis Child Fetal Neonatal Ed [Epub ahead of print]
Vouloumanou EK, Plessa E, Karageorgopoulos DE, Mantadakis E, Falagas ME (2011) Serum procalcitonin as a diagnostic marker for neonatal sepsis: a systematic review and meta-analysis. Intensive Care Med 37:747–762
Roger T, David J, Glauser MP, Calandra T (2001) MIF regulates innate immune responses through modulation of Toll-like receptor 4. Nature 414:920–924
Prencipe G, Auriti C, Inglese R, Devito R, Ronchetti MP, Seganti G, Rava L, Orzalesi M, De Benedetti F (2011) A polymorphism in the macrophage migration inhibitory factor promoter is associated with bronchopulmonary dysplasia. Pediatr Res 69:142–147
Murphy K, Weiner J (2012) Use of leukocyte counts in evaluation of early-onset neonatal sepsis. Pediatr Infect Dis J 31:16–19
Gomez B, Mintegi S, Benito J, Egireun A, Garcia D, Astobiza E (2010) Blood culture and bacteremia predictors in infants less than three months of age with fever without source. Pediatr Infect Dis J 29:43–47
Connell TG, Rele M, Cowley D, Buttery JP, Curtis N (2007) How reliable is a negative blood culture result? Volume of blood submitted for culture in routine practice in a children’s hospital. Pediatrics 119:891–896
Acknowledgements
The authors thank Claudia Schad (Division of Neonatology, University of Bern, Switzerland) for help in data acquisition; Martha Bain (University Hospital Zurich, Switzerland) for excellent technical support with PSP measurements; Silvia Rihs and Leslie Saurer (Department of Pathology, University of Bern, Switzerland) for help in performing sTREM-1 ELISA; Fred C. G. J. Sweep (Department of Laboratory Medicine, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands) for kindly providing antibodies used in the MIF ELISA; Marlies Knaup Reymond (Infectious Diseases Service, Centre Hospitalier Universitaire Vaudois and University of Lausanne, Lausanne, Switzerland) for performing the MIF ELISA. This study was funded by a grant from the Vinetum Foundation, Biel, Switzerland (LJS) and supported by grants from the Swiss National Science Foundation (TR, Grant 310030_138488) and the Amelie Waring Foundation, Zurich, Switzerland (RG).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schlapbach, L.J., Graf, R., Woerner, A. et al. Pancreatic stone protein as a novel marker for neonatal sepsis. Intensive Care Med 39, 754–763 (2013). https://doi.org/10.1007/s00134-012-2798-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-012-2798-3