
Abstract
Background
Robust evidence on whether diagnostic discordance exists between lumbar osteoporosis detected by quantitative computed tomography (QCT) vs. dual-energy X-ray absorptiometry (DXA) is still lacking. In this study involving a relatively large prospective cohort of older men (aged > 60 years) and postmenopausal women, we assessed lumbar QCT-derived volumetric bone mineral density (vBMD) and DXA-derived area BMD and evaluated their predictive performance for prevalent vertebral fracture (VF).
Methods
A total of 501 patients who underwent spinal surgery from September 2020 to September 2022 were enrolled. The criteria recommended by the American College of Radiology and the World Health Organization were used for lumbar osteoporosis diagnosis. The osteoporosis detection rates between QCT and DXA were compared. QCT-vBMD was plotted against the DXA T score, and the line of best fit was calculated based on linear regression. Multivariate logistic regression was used to analyze the associations between risk factors and VF. Receiver operating characteristic curve analysis was performed, and the corresponding area under the curve (AUC) was calculated.
Results
QCT screening showed that 60.7% of patients had osteoporosis, whereas DXA screening showed that 50.7% of patients had osteoporosis. Diagnoses were concordant for 325 (64.9%) patients. In all, 205 patients suffered a VF of at least one anatomic level. Of these, 84.4% (173/205) were diagnosed with osteoporosis by QCT, while only 73.2% (150/205) were diagnosed by DXA. Multivariate logistic regression showed that osteoporosis detected by QCT exhibited a stronger relationship with VF than that detected by DXA (unadjusted OR, 6.81 vs. 5.04; adjusted OR, 3.44 vs. 2.66). For discrimination between patients with and without VF, QCT-vBMD (AUC = 0.802) showed better performance than DXA T score (AUC = 0.76).
Conclusion
In older patients undergoing spinal surgery, QCT-vBMD is more helpful than DXA in terms of osteoporosis detection rate and prediction of patients with prevalent VFs.
Similar content being viewed by others

Background
Osteoporosis is a prevalent skeletal disorder characterized by bone mass loss and microarchitectural deterioration, leading to fragility and fracture. Although bone strength is multifactorial, the measurement of bone mineral density (BMD) plays a pivotal role and has been widely used in clinical practice due to its availability and affordability [1]. Currently, the most commonly used BMD measurement methods include dual X-ray absorptiometry (DXA) and quantitative computed tomography (QCT). The former provides a measurement of the area BMD (aBMD) in two dimensions, while the latter allows for quantification of the volumetric BMD (vBMD) of trabecular bone and avoids interference from aortic calcifications, bone spur formation, and abdominal fat [2]. As spinal BMD can provide useful information for surgical planning and decision-making, it is of greater clinical value to focus on BMD evaluation for patients about to undergo spinal surgery [3,4,5,6].
The diagnostic performance of spinal osteoporosis by QCT and DXA have been compared in several studies, including cross-sectional studies and case‒control studies, but their results have been discordant [7,8,9,10,11]. There are several factors that contribute to these discrepancies in results. Studies performed in small samples may lack statistical power [7]. A high prevalence of osteoporosis was identified in elderly patients undergoing spine surgery. Thus, the results obtained from populations with a relatively low prevalence of osteoporosis or young women with type I diabetes mellitus may not be generalizable to the specific population undergoing spine surgery [8,9,10]. Using the same diagnostic category may contribute to the comparability of data but cause serious deterioration in the accuracy of the procedures [11, 12]. It is inappropriate to use a threshold of T score = -2.5 for both QCT and DXA [13].
Various established risk factors are associated with bone mass loss, including smoking, older age, female sex, body mass index, and diabetes mellitus [14,15,16]. Meanwhile, osteoporosis is still the most sensitive predictor for fragility fractures [17]. To date, robust evidence on whether a diagnostic discordance exists between spinal osteoporosis detected by QCT and that detected by DXA remains lacking. Additional studies designed to assess spinal BMD by QCT and DXA are needed to examine these potential confounders and mediators of the association as well as the clinical outcomes.
Therefore, we assessed spinal QCT-vBMD and DXA-aBMD in a large prospective cohort of older men (aged > 60 years) and postmenopausal women and evaluated the predictive performance regarding vertebral fracture (VF).
Methods
Study design and population cohort
This study was approved by the local institutional review board (IRB) and conducted in accordance with the tenets of the Declaration of Helsinki. Older patients who visited the Spine Surgery Department of a single medical institution and were about to undergo spine surgery were enrolled in this study. Included patients’ demographic information was recorded at admission, including sex, age, BMI, smoking status, medication history, primary diagnosis, and comorbidities. All participants were scheduled for QCT and DXA examinations as well as blood testing for serological indicators within a week of their admission; they were not permitted to receive any antiosteoporotic treatment during this time except for calcium and vitamin D. Those with a history of spinal instrumentation surgery, a history of severe trauma, spinal tumors, spinal infection, and severe spinal deformity were excluded.
BMD evaluation and diagnostic category
An Aquilion 64-slice CT scanner (Toshiba Medical System Inc., Tokyo, Japan) with the Mindways QCT pro system (Mindways Software Inc., Austin, TX) was used for acquiring QCT image sequences and was asynchronously calibrated by a Model 4 calibration phantom that allowed for individuals’ BMD evaluations at a different time. The method of region of interest (ROI) selection has previously been described in detail [2]. Satisfying the point of caution involves maximizing the ROI while excluding the basal vertebral vein, cortical bone, and sclerotic regions. According to the manufacturer’s protocols, standard QCT measurements were utilized to evaluate BMD at the L1-L2 vertebrae. For the individuals in whom the ROI could not be measured at the L1-L2 levels, the adjacent vertebral body was used as a surrogate for measurement of vBMD. The diagnostic thresholds at the L1-L2 levels recommended by the American College of Radiology were used for lumbar osteoporotic diagnosis (normal, vBMD > 120 mg/cm3; osteopenia, 80 mg/cm3 ≤ vBMD ≤ 120 mg/cm3; osteoporosis, vBMD < 80 mg/cm3) [18]. The presence of vertebral fractures was assessed on sagittal CT images by applying the Genant semiquantitative visual approach.
GE Lunar scanners (GE Lunar Prodigy) and DAX Brovo DXA scanners (GE Healthcare, WI, USA) were used to obtain DXA-aBMD at the L1–L4 levels by a well-trained radiologist blinded to the study. The aBMD was then presented as the T score calculated using the following formula:
Quality assurance and quality control were previously described [2]. The diagnostic thresholds at the L1-L4 levels recommended by the World Health Organization (WHO) were used for diagnostic category (normal, -1.0 or above; osteopenia, between -1.0 and -2.5; osteoporosis, -2.5 or below). The possible difference in osteoporotic category between DXA and QCT was classified as a major or minor discordance [19]. The former indicates that the patient was diagnosed with osteopenia by one technique but osteoporosis or normal by the other, while the latter means the patient was diagnosed with osteoporosis by one technique but normal BMD by the other. In the study, all DXA and QCT scans were evaluated by the same experienced radiologist who was blinded to the study.
Statistical analysis
The normality of the data distribution was tested with the Kolmogorov‒Smirnov normality test. Continuous and categorical variables are expressed as the mean ± standard deviation and frequencies and percentages, respectively. The baseline characteristics between two groups were evaluated using one-way ANOVA if the homogeneity of variance requirement was met; otherwise, the rank sum test was used. Chi-square tests were used for comparison of proportions, which were adjusted using the Bonferroni correction for multiple pairwise comparisons. QCT-vBMD was plotted against the DXA T score, followed by calculation of the line of best fit based on linear regression. Contextually, a residual analysis, a “residuals versus fits plot” was conducted. It is a scatter plot of residuals on the y-axis and fitted values (estimated responses) on the x-axis. The plot was used to detect nonlinearity, unequal error variances, and outliers. Subgroup analysis of patient sex, age stratification in postmenopausal women, and presence of VF was performed similarly. Multivariate logistic regression was used to analyze the associations between risk factors and VF, and the odds ratio (OR) and 95% confidence interval (CI) of osteoporosis detected by QCT and DXA were calculated. Variables were transformed and standardized using z scores. Collinearity was assessed with variance inflation factors (VIF). Receiver operating characteristic (ROC) curve analysis was performed to estimate the VF diagnostic performance of the QCT-vBMD and DXA T scores, from which the corresponding area under the curve (AUC) was calculated. SPSS 25.0 (IBM Inc., Armonk, NY, USA), Origin 2021 (Origin Lab Corporation, Northampton, MA, USA) and GraphPad Prism 8 (GraphPad Software Inc., San Diego, CA, USA) were used for statistical analysis and production of all graphs and dot plots. Statistical significance was set at p < 0.05.
Results
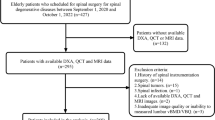
The final sample comprised 501 participants (395 women and 106 men; mean age: 71.3 ± 7.2 and 67.6 ± 10.4 years, respectively), and the flowchart of participants is shown in Fig. 1. The mean BMI of women and men was 23.8 ± 3.6 and 23.7 ± 3.6 kg/m2, respectively. A comparison of baseline characteristics between male and female patients is shown in Table 1. In this cohort, the most frequent primary diagnosis was VF (38.3%), followed by lumbar disc herniation (36.9%). Cardiovascular disease (46.3%), such as hypertension and coronary heart disease, was the most widely reported comorbidity, followed by diabetes mellitus (15.6%). The proportion of elderly men with spinal osteoporosis was significantly lower than that of postmenopausal women (25.5% vs. 57.5% according to DXA category and 44.3% vs. 65.1% according to QCT category, P < 0.01).

Flow chart of patient enrollment
Discordance in osteoporosis diagnoses between QCT and DXA
In this cohort, QCT screening showed that 60.7% had osteoporosis, 30.3% had osteopenia, and 9% had normal BMD, whereas DXA screening showed that 50.7% of patients had osteoporosis, 27.5% had osteopenia, and 21.8% had normal BMD. Diagnoses were concordant for 325 (64.9%) patients. Of the other 176 patients with diagnostic discordance, 14 (2.8%) were major and 162 (32.3%) were minor. A total of 83 (16.5%) patients met the criteria for osteoporosis via QCT but were diagnosed with osteopenia or normal BMD according to the DXA criteria, while 33 (6.6%) were diagnosed with osteoporosis by DXA but not by QCT (Table 2). Similar results of the distribution of diagnostic category for QCT-vBMD and DXA T score were also obtained in the subgroup analysis of male and female patients (Supplementary Tables 1 and 2).
BMD distribution and subgroup analysis
Normality test by Kolmogorov‒Smirnov test showed that the distributions of data for QCT-vBMD and DXA T score are normal (P = 0.152 and 0.069, respectively). BMD distributions for QCT and DXA are plotted separately in Fig. 2. Both were relatively symmetric bell curves with similar distributional characteristics. The X-axis values relative to the peak of the curves of DXA T score distributions were near X = -2.5, while a similar point of the QCT-vBMD distribution curve was at the left of X = 80 mg/cm3. Similar results were also obtained in the subgroup of male and female patients (Supplementary Figures 1 and 2).

Curve fitting of BMD distribution (a bar plot superimposed with the probability density function) for all enrolled patients was performed using a nonlinear least-squares curve-fitting program with a Gaussian product function
Scatter plots (Fig. 3) were drawn to analyze the correlations between QCT-vBMD and DXA T score, including the following subgroup analyses: sex, age stratification in postmenopausal women, and presence of VF. The line of best fit for DXA T score (x-axis) against QCT-vBMD (y-axis) was calculated as follows (Fig. 3 A): y = 14.1*x + 102.9, with a of slope from 12.9 to 15.3 and R2 = 0.508. The residual-versus-fitted plot, Supplementary Figure 3, shows that fitted values do not have an obvious trend of failure. Depending on different sex (Fig. 3 B), the line of best fit was y = 15.8*x + 108.7, R2 = 0.516 (female) and y = 11.7*x + 94.8, R2 = 0.478 (male). Depending on the age stratification in postmenopausal women (Fig. 3 C), the line of best fit was y = 16.1*x + 120, R2 = 0.573 (age ≤ 65 years) and y = 10.5*x + 83.5, R2 = 0.314 (age ≥ 66 years). Depending on the presence of VF (Fig. 3 D), the line of best fit was y = 12.7*x + 106.2, R2 = 0.451 (non-VF) and y = 10.6*x + 83.9, R2 = 0.308 (VF).

A scatter plot was drawn to demonstrate the relationship between QCT-vBMD (y-axis) and DXA T score (x-axis). The line of best fit for x against y is given by y = 14.1*x + 102.9, with a 95% CI of the slope ranging from 12.9 to 15.3 and R2 = 0.508 (A). B, C, and D indicate male versus female, age ≤ 65 years versus age ≥ 66 years, and VCF versus non-VCF
Association between spinal BMD and VF
A total of 205 patients suffered a VF of at least one anatomic level. The VF occurred most commonly in the thoracolumbar spine: 101 fractures involved the L1 level and 79 involved the T12 level. Details regarding the VF status are shown in Fig. 4. Patients with VF had significantly lower BMD (49 mg/cm3 vs 84.9 mg/cm3, P < 0.01) and T-score (-3.25 vs. -1.67, P < 0.01) than those without VF. Among patients with VF, 84.4% (173/205) were diagnosed with osteoporosis by QCT, while only 73.2% (150/205) were diagnosed by DXA. A comparison of the baseline characteristics between the subgroups of patients with VF vs those without VF is shown in Table 3.

The distribution of fractured vertebrae at different levels (A). The distribution of the number of patients with single-level or multilevel VFs (B)
On the basis of univariate analysis, the factors that significantly correlated with VF status were further evaluated using multivariate logistic regression (Table 4). Collinearity analysis demonstrated no collinearity among the variables (i.e., all VIF < 1.1). Model 1 revealed that osteoporosis was an independent risk factors for VF when evaluated either by QCT or DXA. In the case of BMD evaluation using QCT, the OR value for osteoporosis was 6.81 (95%CI: 4.38–10.59), while the OR value for osteoporosis diagnosed by DXA was 5.04 (95%CI: 3.41–7.44). After adjusting for age, BMI, serum uric acid, creatinine clearance, and alkaline phosphatase in Model 2, the OR value for the osteoporosis by QCT and DXA were reduce to 3.44 (95% CI: 2.07–5.71) and 2.66 (95% CI: 1.68–4.21), respectively.
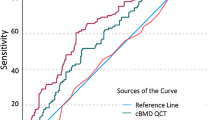
For discrimination between patients with and without VF, QCT-vBMD (AUC = 0.802) showed better performance than DXA T score (AUC = 0.76) (Fig. 5). Similar VF identification results were found in the subgroup analysis of only female patients (AUC = 0.798 for QCT-vBMD vs. AUC = 0.748 for DXA T score) but not in the subgroup of older male patients (AUC = 0.779 for QCT-vBMD vs. AUC = 0.780 for DXA T score). The detailed ROC analysis is shown in Supplementary Table 3.

ROC plots for QCT-vBMD and DXA T score used for prediction of patients with prevalent VFs. A, B, and C indicate all patients, men, and women, respectively
Discussion
The present study involved a comparison between lumbar BMD measurements obtained by QCT-vBMD and by DXA T score in postmenopausal women and older men. Overall, BMD evaluation using QCT-vBMD resulted in identifying more patients with osteoporosis than that using DXA T score. In this cohort, using QCT enabled us to identify 10% more cases of osteoporosis than DXA (60.7% vs. 50.7%). A previous study in postmenopausal women with central obesity showed similar results, wherein spinal osteoporosis was found in 61.4% of women by QCT and in 47.7% of women by DXA [20]. The small sample size (44 postmenopausal women) limited further statistical analysis and generalization of the results. A recent age- and sex-matched study with a relatively large sample size reported that spinal osteoporosis detection rates for QCT were almost twice as high as those for DXA (58.16% vs. 30.63%), which is considerably different than the results in the present study[12]. Differences in the study population may be one of the reasons for this discrepancy; a higher prevalence of osteoporosis in patients undergoing spine surgery has previously been confirmed [21]. Another plausible explanation of the discrepancy may the different diagnostic criteria of spinal osteoporosis. A DXA T score = -2.5 diagnostic category recommended by the WHO was unreasonably applied in QCT; this situation, previously described in full, has been shown to result in a substantial overestimation of the diagnostic performance of QCT [2].
Despite the obvious overlap of ROI selection between the two technologies, there have been some inconsistent results regarding osteoporosis detection and VF prediction given the different imaging principles and diagnostic categories. A discordance in osteoporosis diagnoses between DXA and QCT was observed in 176 patients. A total of 72.7% (128/176) were detected with a lower BMD by QCT. A plausible explanation may be that bone loss is not uniform in age-related osteoporosis; trabecular bone is at a greater risk than cortical bone [22]. QCT can be used to quantify the vBMD of trabecular bone based on three-dimensional imaging while avoiding cortical bone interference. Moreover, limited by two-dimensional X-ray imaging, DXA-aBMD may be overestimated because of obesity, osteophytes, sclerosis, and aortic calcifications [23]. On these grounds, QCT may exhibit a higher sensitivity for BMD evaluation in patients with dominant cancellous bone loss. This interpretation is also supported by the BMD distribution curves (Fig. 2). After drawing a black reference line to mark the threshold for osteoporosis (dotted black line), we could easily see that the X-axis values relative to the peak of the curves of DXA T score distributions were near X = -2.5, while a similar point of the QCT-vBMD distribution curve was at the left of X = 80 mg/cm3. The osteoporosis detection rates of QCT initially peaked with decreased vBMD and then gradually declined with further lowering of vBMD, indicating a greater proportion of osteoporosis. In contrast, osteoporosis detection rates of DXA declined continuously with decreased BMD. This was similarly expressed in the level-specific BMD distribution [2]. The difference in these BMD distribution curves could also be explained by the age-related degeneration. With increasing age, systemic bone is lost gradually, especially cancellous bone; [22] at the same time, osteophytes, osteosclerosis, and abdominal aortic calcification gradually progress [24, 25]. In other words, older patients have lower BMD, more severe degeneration, and greater basis for DXA error, but QCT may not be affected by these factors.
The paucity of evidence-based data regarding the comparison between vBMD and T score distribution prompted us to perform linear correlation analysis. The model between QCT-vBMD as the reference method and DXA T score did not work very well (R2 = 0.508). To eliminate interference from confounding factors, such as age, sex, and VF status, linear regression of the scatter plots was performed for different subgroups, including male vs. female, age ≤ 65 years vs. ≥ 66 years, and with VF vs. without. However, performing additional subgroup analysis did not improve the goodness-of-fit of the regression models (R2 ranged from 0.308 to 0.516). Such a mismatch might not be explained by age, sex, and VF status. Future research should couple imaging characteristics at the measured ROI level with BMD data. Thus, it might be more helpful to explore the differences between QCT and DXA.
In most previous studies comparing diagnostic performance between QCT and DXA, the researchers have not investigated performance in identifying patients with and without VF. Our results revealed that osteoporosis detected by either QCT or DXA was an independent risk factor for prevalent VF (unadjusted/adjusted OR = 6.81/3.44 for QCT, unadjusted/adjusted OR = 5.04/2.66 for DXA). Using the multivariate model adjusted by as many factors as possible could lead to relatively lower ORs than models adjusted by age and sex only (OR from 4.02 to 6.9 for QCT-vBMD) [26, 27]. In other studies of any incident fractures instead of prevalent VFs, a lower OR is also a reasonable result (OR from 1.8 to 2.4 for QCT-vBMD) [28, 29]. Even though there were different OR values in the cited study, our results are in line with the findings in these studies; trabecular vBMD at the spinal lumbar region exhibited a stronger relationship with VF than lumbar DXA. QCT was more sensitive to age-related changes in vertebral body strength, which may justify its better performance for lumbar BMD evaluation in the older population.
Bone and muscle are the two major integrated components in the musculoskeletal system. With their complementary roles, both are vital for maintaining human health. A loss of skeletal muscle mass and function is considered an independent risk factor for fragility fractures as individuals so affected are at a higher risk of falling. The coexistence of sarcopenia and osteoporosis might ultimately worsen disability and health-related quality of life, especially for those characterized by physical frailty and functional impairment [30]. In oncology, the results of CT-based quantitative assessment of skeletal muscle are considered likely to be of prognostic value and be associated with postoperative complications, increased mortality, and overall survival in several cancers [31]. Both BMD and muscular quantity assessments should be integrated to optimize the comprehensive management of musculoskeletal health [32].
In the present study, discrimination between patients with and without VF based on QCT-vBMD was superior in relation to DXA T score (AUC = 0.802 vs. 0.76). It was reported from a recent study that vBMD obtained by routine CT compared to DXA can also improve the prediction of patients with prevalent VFs (AUC: 0.885 vs. 0.67). Another retrospective cohort study revealed the improved prediction of incident VF using opportunistic QCT compared to DXA (AUC: 0.76 vs. 0.63) [27]. The AUCs were different in the cited studies. However, owing to the heterogeneity of the study design, as well as differences in scanning protocols and study populations, any direct comparison between studies is not appropriate. Considering that BMD data obtained from the same individuals allowed for the elimination of influence from individual differences, this difference could be attributed to the advantage of the QCT technology itself. Studies in level-specific BMD evaluation also yielded similar results [2, 33].
The present study has several limitations. The study population was highly homogeneous, including only patients who were about to undergo spine surgery. Generalizability of the study results to patients from internal medicine services or other types of surgical practice may therefore be limited. Additionally, CT scans involve larger radiation doses and impose a greater financial burden on patients than DXA. However, unlike DXA, CT for patients scheduled for spine surgery is not restricted to BMD measurements and includes screening for other related disease and surgical planning. In future work, we should couple imaging characteristics at the measured ROI level with the BMD data. This approach might be more helpful in exploring the difference between QCT and DXA. Some importance should also be given to studying the effect of spinal-related degeneration and abdominal calcification on BMD evaluation, especially in patients classified with major discordance.
In conclusion, this study showed that preoperative QCT in older patients who undergo spine surgery is helpful to increase the spinal osteoporosis detection rate and improve the prediction of prevalent VF when compared to DXA.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request (Zhiyun Wang, E-amil: Dragon201@126.com).
Abbreviations
- BMD:
-
Bone mineral density
- DXA:
-
Dual-energy X-ray absorptiometry
- QCT:
-
Quantitative computed tomography
- vBMD:
-
Volumetric BMD
- aBMD:
-
Area BMD
- VF:
-
Vertebral fracture
- ROI:
-
Region of interest
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
References
Iolascon G, Paoletta M, Liguori S, Gimigliano F, Moretti A. Bone fragility: conceptual framework, therapeutic implications, and COVID-19-related issues. Ther Adv Musculoskelet Dis. 2022;14:1759720X221133429.
Lin W, He C, Xie F, et al. Discordance in lumbar bone mineral density measurements by quantitative computed tomography and dual-energy X-ray absorptiometry in postmenopausal women: a prospective comparative study. Spine J. 2022;23(2):295-304.
Kuprys TK, Steinmetz LM, Fischer CR, et al. Preoperative Assessment of Bone Quality in Spine Deformity Surgery: Correlation With Clinical Practice and Published Recommendations. Spine (Phila Pa 1976). 2019;44(12):E735–41.
Weiser L, Huber G, Sellenschloh K, et al. Insufficient stability of pedicle screws in osteoporotic vertebrae: biomechanical correlation of bone mineral density and pedicle screw fixation strength. Eur Spine J. 2017;26(11):2891–7.
Lee BG, Choi JH, Kim DY, Choi WR, Lee SG, Kang CN. Risk factors for newly developed osteoporotic vertebral compression fractures following treatment for osteoporotic vertebral compression fractures. Spine J. 2019;19(2):301–5.
Kim DH, Hwang RW, Lee GH, et al. Comparing rates of early pedicle screw loosening in posterolateral lumbar fusion with and without transforaminal lumbar interbody fusion. Spine J. 2020;20(9):1438–45.
Dheeraj D, Chauhan U, Khapre M, Kant R. Comparison of Quantitative Computed Tomography and Dual X-Ray Absorptiometry: Osteoporosis Detection Rates in Diabetic Patients. Cureus. 2022;14(3): e23131.
Li N, Li XM, Xu L, Sun WJ, Cheng XG, Tian W. Comparison of QCT and DXA: Osteoporosis Detection Rates in Postmenopausal Women. Int J Endocrinol. 2013;2013: 895474.
Xu XM, Li N, Li K, et al. Discordance in diagnosis of osteoporosis by quantitative computed tomography and dual-energy X-ray absorptiometry in Chinese elderly men. J Orthop Translat. 2019;18:59–64.
Jiang H, Robinson DL, Nankervis A, et al. Bone Measures by Dual-Energy X-Ray Absorptiometry and Peripheral Quantitative Computed Tomography in Young Women With Type 1 Diabetes Mellitus. J Clin Densitom. 2021;24(2):259–67.
Bergot C, Laval-Jeantet AM, Hutchinson K, Dautraix I, Caulin F, Genant HK. A comparison of spinal quantitative computed tomography with dual energy X-ray absorptiometry in European women with vertebral and nonvertebral fractures. Calcif Tissue Int. 2001;68(2):74–82.
Kulkarni AG, Thonangi Y, Pathan S, et al. Should Q-CT Be the Gold Standard for Detecting Spinal Osteoporosis? Spine (Phila Pa 1976). 2022;47(6):E258–64.
Engelke K, Adams JE, Armbrecht G, et al. Clinical use of quantitative computed tomography and peripheral quantitative computed tomography in the management of osteoporosis in adults: the 2007 ISCD Official Positions. J Clin Densitom. 2008;11(1):123–62.
Li T, Hu L, Yin XL, Zou Y, Fu HY, Li HL. Prevalence and Risk Factors of Osteoporosis in Patients with Type 2 Diabetes Mellitus in Nanchang (China): A Retrospective Cohort Study. Diabetes Metab Syndr Obes. 2022;15:3039–48.
Weng W, Li H, Zhu S. An Overlooked Bone Metabolic Disorder: Cigarette Smoking-Induced Osteoporosis. Genes (Basel). 2022;13(5):806.
Barron RL, Oster G, Grauer A, Crittenden DB, Weycker D. Determinants of imminent fracture risk in postmenopausal women with osteoporosis. Osteoporos Int. 2020;31(11):2103–11.
Nawrat-Szoltysik A, Miodonska Z, Zarzeczny R, et al. Osteoporosis in Polish Older Women: Risk Factors and Osteoporotic Fractures: A Cross-Sectional Study. Int J Environ Res Public Health. 2020;17(10):3725.
American College of Radiology. Acr–Spr–Ssr Practice Parameter for The Performance of Musculoskeletal Quantitative Computed Tomography (QCT). 2018. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/qct.pdf?la=en. Accessed 18 Jan 2023.
Mounach A, Abayi DA, Ghazi M, et al. Discordance between hip and spine bone mineral density measurement using DXA: prevalence and risk factors. Semin Arthritis Rheum. 2009;38(6):467–71.
Milisic L, Vegar-Zubovic S, Valjevac A, Hasanovic-Vuckovic S. Bone Mineral Density Assessment by DXA vs. QCT in Postmenopausal Females with Central Obesity. Curr Aging Sci. 2020;13(2):153–61.
Zou D, Jiang S, Zhou S, et al. Prevalence of Osteoporosis in Patients Undergoing Lumbar Fusion for Lumbar Degenerative Diseases: A Combination of DXA and Hounsfield Units. Spine (Phila Pa 1976). 2020;45(7):E406–10.
Christiansen BA, Kopperdahl DL, Kiel DP, Keaveny TM, Bouxsein ML. Mechanical contributions of the cortical and trabecular compartments contribute to differences in age-related changes in vertebral body strength in men and women assessed by QCT-based finite element analysis. J Bone Miner Res. 2011;26(5):974–83.
Graeff C, Marin F, Petto H, et al. High resolution quantitative computed tomography-based assessment of trabecular microstructure and strength estimates by finite-element analysis of the spine, but not DXA, reflects vertebral fracture status in men with glucocorticoid-induced osteoporosis. Bone. 2013;52(2):568–77.
El Maghraoui A, Rezqi A, Mounach A, et al. Vertebral fractures and abdominal aortic calcification in postmenopausal women A cohort study. Bone. 2013;56(1):213–9.
Yu W, Gluer CC, Fuerst T, et al. Influence of degenerative joint disease on spinal bone mineral measurements in postmenopausal women. Calcif Tissue Int. 1995;57(3):169–74.
Loffler MT, Jacob A, Scharr A, et al. Automatic opportunistic osteoporosis screening in routine CT: improved prediction of patients with prevalent vertebral fractures compared to DXA. Eur Radiol. 2021;31(8):6069–77.
Loffler MT, Jacob A, Valentinitsch A, et al. Improved prediction of incident vertebral fractures using opportunistic QCT compared to DXA. Eur Radiol. 2019;29(9):4980–9.
Allaire BT, Lu D, Johannesdottir F, et al. Prediction of incident vertebral fracture using CT-based finite element analysis. Osteoporos Int. 2019;30(2):323–31.
Johannesdottir F, Allaire B, Kopperdahl DL, et al. Bone density and strength from thoracic and lumbar CT scans both predict incident vertebral fractures independently of fracture location. Osteoporos Int. 2021;32(2):261–9.
Wilson AC, Bon JM, Mason S, et al. Increased chest CT derived bone and muscle measures capture markers of improved morbidity and mortality in COPD. Respir Res. 2022;23(1):311.
Shah P, Supanich M. Chest CT-Derived Muscle Metrics for Sarcopenia: Choosing the Right Target. Ann Surg Oncol. 2022;29(3):1511–2.
de Sire A, Lippi L, Aprile V, et al. Pharmacological, Nutritional, and Rehabilitative Interventions to Improve the Complex Management of Osteoporosis in Patients with Chronic Obstructive Pulmonary Disease: A Narrative Review. J Pers Med. 2022;12(10):1626.
Dieckmeyer M, Loffler MT, El Husseini M, et al. Level-Specific Volumetric BMD Threshold Values for the Prediction of Incident Vertebral Fractures Using Opportunistic QCT: A Case-Control Study. Front Endocrinol (Lausanne). 2022;13: 882163.
Acknowledgements
Not applicable.
Funding
The author (ZW) received funding from Guangdong Basic and Applied Basic Research Foundation (2021A1515011508) and the Scientific Research Start Plan of Shunde Hospital, Southern Medical University (CRSP2019010). Another author (WL) received funding from the Scientific Research Start Plan of Shunde Hospital, Southern Medical University (SRSP2021007).
Author information
Authors and Affiliations
Contributions
Study conceptualization and design: Wentao Lin, Zhiyun Wang; Data acquisition: Chaoqin He, Tao Chen, Guanghao Zheng, Houjie Yin; Data analysis: Faqin Xie, Haixiong Chen; Manuscript drafting: Wentao Lin; Technical support: Haixiong Chen; All authors contributed to revising and approving the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in accordance with the ethical standards proposed by the 1964 Declaration of Helsinki. This study was carried out in accordance with relevant regulations of the US Health Insurance Portability and Accountability Act (HIPAA). Details that might disclose the identity of the subjects under study have been omitted. Informed consent was obtained from all subjects or their legal guardians. Ethical approval was obtained from the Institutional Review Board of Shunde Hospital of Southern Medical University (LWLS202207003).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Distribution of diagnostic category for lumbar BMD in female.
Additional file 2: Supplementary Table 2.
Distribution of diagnostic category for lumbar BMD in male.
Additional file 3: Supplemental Table 3.
AUCs with 95% CIs, Youden’s indices, and the resulting QCT/DXA thresholds and sensitivity and specificity values.
Additional file 4: Supplementary Figure 1.
Curve fitting of BMD distribution for older men.
Additional file 5: Supplementary Figure 2.
Curve fitting of BMD distribution for postmenopausal women.
Additional file 6: Supplementary Figure 3.
The residual-versus-fitted plot shows that fitted values do not have an obvious trend of failure.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lin, W., He, C., Xie, F. et al. Quantitative CT screening improved lumbar BMD evaluation in older patients compared to dual-energy X-ray absorptiometry. BMC Geriatr 23, 231 (2023). https://doi.org/10.1186/s12877-023-03963-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-03963-6