
Abstract
Background
Emerging studies have investigated the association between different anthropometric indices with diabetes risk but the results were inconsistent. The aims of the study were to examine the associations of different anthropometric indices with incident diabetes risk and whether novel anthropometric indices improve diabetes prediction beyond traditional indices among elderly Chinese.
Methods
Nine thousand nine hundred sixty-two elderly individuals (age ≥ 60 years old) derived from the prospective Dongfeng-Tongji cohort were included. Hazard ratio (HR) and corresponding 95% confidence interval (CI) were evaluated by Cox proportional hazard model to examine the associations between traditional anthropometric indices (body mass index [BMI], waist circumference [WC], waist-to-height ratio [WHtR]), novel anthropometric indices (visceral adiposity index [VAI], a body shape index [ABSI], body roundness index [BRI]) and diabetes risk. Receiver operating characteristic (ROC) curve and area under curve (AUC) were applied to compare the novel anthropometric indices with the traditional indices in diabetes prediction.
Results
During mean 4.6 years of follow-up, 614 incident cases of type 2 diabetes (T2D) were identified. Significant positive associations were detected between BMI, WC, WHtR, VAI and BRI and incident T2D risk. For ABSI, no significant association was observed in either men or women. BMI was the strongest predictor in diabetes in men (AUC = 0.655) comparable with the other anthropometric indices (P < 0.05). Similar as men, BMI was the strongest predictor (AUC = 0.635) in women. Except for WC, the AUC of BMI was larger than WHtR, VAI, and BRI. In contrast, ABSI was not a good predictor in either men (AUC = 0.507) or women (AUC = 0.503).
Conclusions
In elderly Chinese, BMI, WC, WHtR, VAI and BRI were positively associated with incident T2D risk. Among them, BMI was the strongest predictor in both men and women.
Similar content being viewed by others

Background
In recent decades, type 2 diabetes (T2D) has increased rapidly and become a serious public health problem worldwide [1]. In China, the prevalence of T2D has risen to be 11.6% and over 100 million adults were affected [2].
Obesity is well recognized to be an important risk factor for the development of T2D. In epidemiological studies, anthropometric indices have been used to evaluate obesity for their simplicity and usefulness. Body mass index (BMI) has been the most commonly used anthropometric measure for defining obesity recommended by World Health Organization (WHO) [3] .Subsequently, studies found that BMI, an estimate of general obesity, could not reflect abdominal fat. Therefore waist circumference (WC) and waist-to-height ratio (WHtR) were suggested as an indicator of central adiposity [4,5,6], although they could not discriminate visceral fat from subcutaneous fat. In recent years, novel anthropometric indices, such as visceral adiposity index (VAI), a body shape index (ABSI), and body roundness index (BRI) have been proposed to be alternative indicators of obesity. VAI, an indicator of visceral fat dysfunction, has been reported to distinguish visceral fat from subcutaneous fat [7]. Bozorgmanesh et al. found VAI has a good predictive performance on diabetes in Tehran people [8]. In 2012, Krakauer developed a new anthropometric index named ABSI, and found ABSI was significantly associated with mortality [9]. In the following years, Thomas et al. developed another new anthropometric index known as BRI [10]. A recent study demonstrated that BRI was a potential and alternative obesity measure in assessment of T2D [11]. However, till now no comprehensive consensus has been reached about which one as the best anthropometric index to evaluate the risk and the predictive ability of diabetes, especially in elderly population.
The World Health Organization estimated that there were 600 million people aged 60 years or older in 2000, and that this number will increase to 1.2 billion in 2025 [12]. It is known that aging was related to significant changes in body composition, but it is unclear which anthropometric index is the best one to evaluate obesity and predict diabetes risk [13]. In the present study, based on the ongoing prospective Dongfeng-Tongji cohort study, we aim to examine the associations of different anthropometric indices with diabetes risk and to investigate whether these novel anthropometric indices could improve predictive ability of diabetes beyond traditional indices in elderly population.
Methods
Study participants
The participants in the present study were derived from the Dongfeng-Tongji (DFTJ) cohort study, which has been described elsewhere [14]. In brief, DFTJ, initiated in 2008, is a dynamic cohort study including 27,009 retirees from the Dongfeng Motor Corporation. The participants completed an epidemiology questionnaire including socio-demographic, lifestyle and medical history at baseline. The first follow-up was conducted from April to October 2013. As shown in (Additional file 1: Figure S1), participants with age below 60 years old (n = 7932), prevalent diabetes (n = 4344), coronary heart disease (n = 2607), stroke (n = 437) or cancer (n = 555) at baseline were excluded. Additionally, individuals were also ruled out if they had missing information on BMI (n = 292), WC (n = 56), triglyceride (TG, n = 766) or high-density lipoprotein cholesterol (HDL-c, n = 58). After exclusion, a total of 5998 men and 3964 women were eligible for the present study.
Anthropometric measurement
Height and weight were measured without shoes and heavy clothes, using standard device and methods, recorded to the nearest 0.5 cm and 0.1 kg. WC was determined at midway level between the lower rib margin and the iliac-crest at minimal respiration. BMI was calculated as weight (kg) divided by height (m) squared. WHtR was calculated as dividing WC (cm) by height (cm). VAI was defined as the following formula [7]:
ABSI was defined as: ABSI=WC(m)/ (BMI2/3 × height(m)1/2). BRI was defined as: BRI = 364.2–365.5× {1 – [(WC(m)/2π)/ (0.5 × height(m))] 2}1/2.
Type 2 diabetes definition
Type 2 diabetes cases were defined as self-reported physician-diagnosed diabetes or taking diabetes medications (oral hypoglycemic agent or insulin) or fasting glucose concentration (FBG) ≥ 7.0 mmol/L according to the WHO criteria [15]. In the study, a total of 614 incident diabetes were diagnosed.
Covariates assessment
Overnight fasting blood specimens were obtained and FBG level was measured by Abbott Aroset analyzer. TG, TC, HDL-c and high-density lipoprotein cholesterol (LDL-c) levels were measured by ARCHITECT Ci8200 automatic analyzer (ABBOTT Laboratories. Abbott Park, Illinois, U.S.A). Smokers were defined as those who smoke at least one cigarette per day for more than half a year, and smoking status was classified as never smoking, current smoking, and former smoking. Similarly, drinkers were defined as those who drink at least once per week for more than half a year, and drinking status was classified as never drinking, current drinking, and former drinking. Physical activity was defined as those who exercise at least 20 min per time regularly over the past 6 months. Education status was categorized into two levels: low level (middle or primary school or below) and high level (high school or beyond). Hypertension was defined if blood pressure ≥ 140/90 mmHg, or using antihypertensive medication or self-reported physician-diagnosed hypertension. Hyperlipidemia was defined if TC > 5.72 mmol/L or TG > 1.70 mmol/L or using lipid-lowing medication, or self-reported physician-diagnosed hyperlipidemia.
Statistical analysis
Categorical variables were presented in number (percentage) and continuous variables in mean (SD) or median. Student’s t-test, Mann-Whiney U test or Chi-square test were used for comparison between groups. In the present analysis, central obesity was defined as WC ≥85 cm in men and WC ≥ 80 cm in women. The cut-off point of WHtR was 0.5 [16]. According to the China criterion, BMI < 24 kg/m2 was defined as normal, 24–27.9 kg/m2 overweight, and BMI ≥ 28 kg/m2 obesity. VAI, ABSI and BRI were stratified into sex-specific tertiles. Partial correlation was used to examine the linear relationship between various anthropometric indices after adjustment for age. Cox proportional hazard model was used to calculate hazard ratio (HR) and corresponding 95% confidence intervals (CIs) of incident diabetes for different anthropometric indices. Receiver operating characteristic (ROC) analysis was used to compare discrimination ability and determine optimal cut-off value. Sensitivity and specificity were calculated based on cut-off values, which were estimated using the maximized Youden index. The areas under the ROC curves (AUC) was compared by a non-parametric test [17]. Statistical analyses were performed with SPSS Statistics 23.0 (SPSS, Chicago, Illinois, USA), except for the ROC analysis, which was tested using MedCalc V.17.9 (MedCalc Software, Belgium). A two-side value of P < 0.05 was considered statistically significant.
Results
Characteristics of participants
During mean 4.6 years of follow-up, 365 incident cases of T2D in the 5998 men (14.09/1000 person-years) and 249 cases in the 3964 women (14.45/1000 person-years) were identified. Baseline characteristics of the 614 (6.2%) participants who did and 9348 (93.8%) who did not develop to T2D are shown in Table 1. The average age of participants who did and who did not develop to T2D was 66.44 and 66.81 years old respectively. As expected, participants who developed to T2D were more likely to have higher levels of WC, WHtR, BMI, VAI, BRI, diastolic blood pressure (DBP), systolic blood pressure (SBP), TG, FBG (all P < 0.001), TC (P = 0.019) and lower levels of HDL-c (P = 0.001). Moreover, the rate of drinking (P = 0.02) in participants who developed to T2D was higher than who did not. No significant difference was observed in ABSI (P = 0.441), smoking (P = 0.854), physical activity (P = 0.213), education level (P = 0.244), and family history of T2D (P = 0.09) between participants who did and who did not develop to T2D.
The correlation coefficients between various anthropometric indices are shown in (Additional file 1: Table S1). All anthropometric indices showed significant correlation with each other (P < 0.001). The strongest correlation coefficient was found between WHtR and BRI (r = 0.87 and r = 0.83) and the weakest one between BMI and ABSI (r = − 0.047 and r = − 0.161). Similar findings were observed in both men and women.
Association of anthropometric indices with incident T2D risk
The relationships between anthropometric indices including WC, WHtR, BMI, VAI, ABSI, and BRI and incident T2D risk in men and women are shown in Table 2. For ABSI, no significant association was observed in either men (P for trend = 0.098) or women (P for trend = 0.313).WC, WHtR, BMI, VAI, and BRI were significantly associated with increased risk of T2D in both men and women after adjustment for potential confounders including age, smoking, drinking, physical activity and education. Further adjustment for hypertension, hyperlipidemia (except VAI), FBG (except VAI) and family history of T2D reduced the associations but still remained significant. In men, the hazard risks (95% CI; top vs lowest) were 1.43 (1.14–1.78) for WC, 1.43 (1.22–1.82) for WHtR, 2.59 (1.91–3.53) for BMI, 2.00 (1.49–2.67) for VAI, 0.79(0.61, 1.03) for ABSI, and 1.60(1.20–2.13) for BRI. For women, the corresponding HRs (95% CI) were 1.46 (1.11–1.92), 1.51 (1.10–2.09), 2.01(1.41–2.87), 1.85 (1.31–2.61), 0.83(0.61, 1.41), and 1.73 (1.21–2.46) for WC, WHtR, BMI, VAI, ABSI and BRI respectively.
ROC analysis
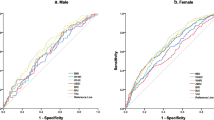
Figure 1 and Table 3 presents the results of ROC analysis and AUC (95% CIs) for BMI, WC, WHtR, VAI, ABSI, and BRI. Comparison of AUC in different anthropometric indices is shown in (Additional file 1: Table S2). In men, ROC analysis revealed that BMI was the strongest predictor in diabetes (AUC = 0.655) comparable with the other anthropometric indices (P < 0.05) including WC (AUC =0.629), WHtR (AUC =0.629), VAI (AUC = 0.609) and BRI (AUC = 0.629). Similar as men, BMI was the strongest predictor (AUC = 0.635) in women. Except for WC (AUC = 0.616, P = 0.165 vs. BMI), the AUC of BMI was larger than other indices such as WHtR (AUC = 0.609, P = 0.051 vs. BMI), VAI (AUC = 0.582, P = 0.017 vs. BMI) and BRI (AUC = 0.609, P = 0.051vs. BMI). In contrast, ABSI was not a good predictor in either men (AUC = 0.507) or women (AUC = 0.503).

ROC curves for WC, WHtR, BMI, VAI, ABSI and BRI in men (a) and women (b) The ROC curves were constructed for T2D as a response to each anthropometric index. In men (a): WC: AUC = 0.629 (95% CI: 0.600–0.659). WHtR: AUC = 0.629 (95% CI: 0.600–0.658). BMI: AUC = 0.655 (95% CI: 0.626–0.684). VAI: AUC = 0.609 (95% CI: 0.578–0.639). ABSI: AUC = 0.507 (95% CI: 0.477–0.538). BRI: AUC = 0.629 (95% CI: 0.600–0.658). In women (b): WC: AUC = 0.616 (95% CI: 0.581–0.651). WHtR: AUC = 0.609 (95% CI: 0.574–0.644). BMI: AUC = 0.635 (95% CI: 0.602–0.667). VAI: AUC = 0.582 (95% CI: 0.548–0.617). ABSI: AUC = 0.503 (95% CI: 0.465–0.540). BRI: AUC = 0.609 (95% CI: 0.574–0.644)
Optimal cutoff points of anthropometric indices in T2D risk prediction
Table 4 summarized the optimal cutoff points of the five significant anthropometric indices in prediction of T2D risk (P < 0.05 vs. AUC = 0.50). For men, optimal WC cut-off point was 84.90 cm in terms of Youden index; for women, the optimal cut-off point was 81.10 cm. The optimal cut-off point of BMI in men was 25.78 kg/m2 and 24.86 kg/m2 in women. The cut-off points for WHtR were similar in men (0.512) and women (0.514). For VAI, it was 1.34 in men and 1.23 in women. The optimal cut-off point of BRI in men was 3.58 and 3.62 in women.
Discussion
To the best of our knowledge, this is the largest prospective study to compare the novel anthropometric indices with the traditional indices in the risk prediction of T2D in elderly population. BMI, WC, WHtR, VAI, BRI were positively associated with incident T2D risk in the elderly, independent of the potential confounders. For ABSI, no significant association was observed in either men or women. BMI appeared to be the strongest predictor of incident T2D risk in both elderly men and women. In comparison with traditional anthropometric indices, novel anthropometric indices did not improve prediction of T2D in elderly population.
In the present study, BMI was the strongest predictor in both elderly men and women, while WC and WHtR showed similar prediction ability in men. These results were consistent with other studies. In Pima Indians, BMI was the best predictors of diabetes [18]. In the Health Professionals Follow-Up Study, BMI and WC showed similar associations with T2D in men aged 40–75 years; in contrast, WHR was the weakest predictor [19]. In the Atherosclerosis Risk in Communities (ARIC) Study, BMI, WC, and WHR showed similar associations in adults aged 40–64 years [20].
A large amount of studies examined the associations of novel anthropometric indices such as VAI, ABSI and BRI with diabetes risk and their performances on diabetes risk prediction. In cross-sectional [21, 22] and cohort studies [23, 24], VAI was associated with increased risk for T2D. The result was validated in the Tehran Lipid and Glucose cohort study [25]. Besides, researchers observed that VAI was a useful surrogate marker to identify risk of diabetes [23, 24], but whether the ability of the VAI to identify diabetes risk was superior to easily measurable anthropometric markers, such as BMI, WC, WHtR was still a matter of debate [22, 23, 25].
For ABSI, no significant association was observed in either men or women. ABSI was not a good discriminator of T2D in the present study. Some studies observed that ABSI was positively correlated with mortality from cardiovascular diseases and cancer [26]. Studies investigating the ABSI to predict T2D are scarce, especially in elderly population. Furthermore, until now studies have not shown that ABSI is superior to BMI or waist circumference in predicting T2D.
BRI was significantly associated with increased risk of diabetes and potential for use as an alternative index in assessment of T2D, which was consistent with previous study [11]. Till now no comprehensive consensus has been reached which one is the best anthropometric index to evaluate the risk and the predictive ability of diabetes in elderly Chinese. Whereas, compared with other anthropometric indices, BMI was taken as a useful indicator for measuring obesity in epidemiological surveys for its simplicity [3]. Our study confirmed that increased BMI was associated with type 2 diabetes in elderly Chinese population, which could be useful in initiating early interventional measures including balanced diet and regular physical exercise to prevent overweight, obesity and type 2 diabetes in the elderly population [27].
Our study also proposed optimal cut-off points for these anthropometric indices. An obvious difference was observed in WC, VAI and BRI between men and women, suggesting that gender-specific reference values should be recommended in practice. The appropriate cutoff points to best identify T2D were not consistent among different age ranges and different population. Aging not only promotes increased body fat, but also changes its distribution. Furthermore, although numerous studies proposed alternative BMI criteria specific to Asian populations [28], no consistent findings were obtained. Our ROC analysis suggested that the ideal BMI cutoffs were 25.78 kg/m2 and 24.86 kg/m2 for identifying diabetes risk in Chinese elderly men and women, respectively. Besides, in the present study WC threshold was about 85 cm for men and 81 cm for women, similar as the findings from a meta-analysis in China with WC cut-off points of 85 cm in men and 80 cm in women. While in Japan the optimal WC cutoff for abdominal obesity in men and women was 85 and 90 cm [29]. Thus, WC cutoff points cannot be used universally across gender, race or different age ranges [30]. As for VAI or BRI, there was no study about its cutoff points previously. Therefore, the definition of obesity among the elderly is still a matter of debate and our findings still need further verification.
To our knowledge, it is the first prospective study focused on elderly Chinese to comparing the novel indices with the traditional indices for diabetes risk prediction. Moreover, a notable strength was its prospective design, sex-specific analysis and relative large sample size. The study also has some limitations. Firstly, the duration of follow-up (mean 4.6 years) was relatively short and limited T2D cases were identified. Secondly, although a variety of relevant confounding factors were controlled, residual confounders could not be eliminated.
Conclusions
In conclusion, significant associations were observed between BMI, WC, WHtR, VAI and BRI and incident risk of T2D in both elderly men and women. BMI was the strongest and best predictor of incident diabetes in elderly population. In comparison with traditional anthropometric indices, novel anthropometric indices did not improve prediction of T2D in elderly Chinese. Future studies should examine this issue in much larger samples and different population. The underlying mechanism also need to be further elucidated. Given that anthropometric indices are potentially modifiable factors, our findings may provide important public health implications for the prevention and management of T2D, especially in elderly population.
Abbreviations
- ABSI:
-
A body shape index
- ARIC:
-
Atherosclerosis Risk in Communities
- AUC:
-
Area under curve
- BMI:
-
Body mass index
- BRI:
-
Body round index
- CI:
-
Confidence interval
- DBP:
-
Diastolic blood pressure
- EDTA:
-
Ethylene diamine tetraacetic acid
- FBG:
-
Fasting glucose concentration
- HDL-c:
-
High-density lipoprotein cholesterol
- HR:
-
Hazard ratio
- LDL-c:
-
Low-density lipoprotein
- OGTT:
-
Oral glucose tolerance test
- SBP:
-
Systolic blood pressure
- T2D:
-
Type 2 diabetes
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- VAI:
-
Visceral adiposity index
- WC:
-
Waist circumstance
- WHO:
-
World Health Organization
- WHtR:
-
Waist-to-height ratio
References
Chan JC, Malik V, Jia W, Kadowaki T, Yajnik CS, Yoon KH, et al. Diabetes in Asia: epidemiology, risk factors, and pathophysiology. JAMA. 2009;301:2129–40.
Xu Y, Wang L, He J, Bi Y, Li M, Wang T, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310:948–59.
Misra A. Ethnic-specific criteria for classification of body mass index: a perspective for Asian Indians and American Diabetes Association position statement. Diabetes Technol Ther. 2015;17:667–71.
Daniels SR, Khoury PR, Morrison JA. Utility of different measures of body fat distribution in children and adolescents. Am J Epidemiol. 2000;152:1179–84.
Li C, Ford ES, McGuire LC, Mokdad AH. Increasing trends in waist circumference and abdominal obesity among US adults. Obesity (Silver Spring). 2007;15:216–24.
Esmaillzadeh A, Mirmiran P, Azizi F. Waist-to-hip ratio is a better screening measure for cardiovascular risk factors than other anthropometric indicators in Tehranian adult men. Int J Obes Relat Metab Disord. 2004;28:1325–32.
Amato MC, Giordano C, Galia M, Criscimanna A, Vitabile S, Midiri M, et al. Visceral adiposity index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care. 2010;33:920–2.
Bozorgmanesh M, Hadaegh F, Azizi F. Predictive performance of the visceral adiposity index for a visceral adiposity-related risk: type 2 diabetes. Lipids Health Dis. 2011;10:88.
Krakauer NY, Krakauer JC. A new body shape index predicts mortality hazard independently of body mass index. PLoS One. 2012;7:e39504.
Thomas DM, Bredlau C, Bosy-Westphal A, Mueller M, Shen W, Gallagher D, et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity (Silver Spring). 2013;21:2264–71.
Chang Y, Guo X, Chen Y, Guo L, Li Z, Yu S, et al. A body shape index and body roundness index: two new body indices to identify diabetes mellitus among rural populations in Northeast China. BMC Public Health. 2015;15:794.
Dodds RM, Roberts HC, Cooper C, Sayer AA. The epidemiology of sarcopenia. J Clin Densitom. 2015;18:461–6.
Michalakis K, Goulis DG, Vazaiou A, Mintziori G, Polymeris A, Abrahamian-Michalakis A. Obesity in the ageing man. Metabolism. 2013;62:1341–9.
Wang F, Zhu J, Yao P, Li X, He M, Liu Y, et al. Cohort profile: the Dongfeng-Tongji cohort study of retired workers. Int J Epidemiol. 2013;42:731–40.
Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15:539–53.
Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012;13:275–86.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–45.
Tulloch-Reid MK, Williams DE, Looker HC, Hanson RL, Knowler WC. Do measures of body fat distribution provide information on the risk of type 2 diabetes in addition to measures of general obesity? Comparison of anthropometric predictors of type 2 diabetes in Pima Indians. Diabetes Care. 2003;26:2556–61.
Wang Y, Rimm EB, Stampfer MJ, Willett WC, Hu FB. Comparison of abdominal adiposity and overall obesity in predicting risk of type 2 diabetes among men. Am J Clin Nutr. 2005;81:555–63.
Vazquez G, Duval S, Jacobs DR Jr, Silventoinen K. Comparison of body mass index, waist circumference, and waist/hip ratio in predicting incident diabetes: a meta-analysis. Epidemiol Rev. 2007;29:115–28.
Du T, Sun X, Huo R, Yu X. Visceral adiposity index, hypertriglyceridemic waist and risk of diabetes: the China health and nutrition survey 2009. Int J Obes. 2014;38:840–7.
Yang Y, Feng Y, Ma X, Chen K, Wu N, Wang D, et al. Visceral adiposity index and insulin secretion and action in first-degree relatives of subjects with type 2 diabetes. Diabetes Metab Res Rev. 2015;31:315–21.
Wang Y, He S, He J, Wang S, Liu K, Chen X. Predictive value of visceral adiposity index for type 2 diabetes mellitus: a 15-year prospective cohort study. Herz. 2015;40(Suppl 3):277–81.
Chen C, Xu Y, Guo ZR, Yang J, Wu M, Hu XS. The application of visceral adiposity index in identifying type 2 diabetes risks based on a prospective cohort in China. Lipids Health Dis. 2014;13:108.
Ghasemi A, Tohidi M, Derakhshan A, Hasheminia M, Azizi F, Hadaegh F. Cut-off points of homeostasis model assessment of insulin resistance, beta-cell function, and fasting serum insulin to identify future type 2 diabetes: Tehran lipid and glucose study. Acta Diabetol. 2015;52:905–15.
Dhana K, Kavousi M, Ikram MA, Tiemeier HW, Hofman A, Franco OH. Body shape index in comparison with other anthropometric measures in prediction of total and cause-specific mortality. J Epidemiol Community Health. 2016;70:90–6.
Olafsdottir E, Aspelund T, Sigurdsson G, Thorsson B, Benediktsson R, Harris TB, et al. Unfavourable risk factors for type 2 diabetes mellitus are already apparent more than a decade before onset in a population-based study of older persons: from the age, gene/environment susceptibility-Reykjavik study (AGES-Reykjavik). Eur J Epidemiol. 2009;24:307–14.
Misra A. Revisions of cutoffs of body mass index to define overweight and obesity are needed for the Asian-ethnic groups. Int J Obes Relat Metab Disord. 2003;27:1294–6.
Oda E. New criteria for ‘obesity disease’ in Japan. Circ J. 2006;70:150 author reply 150.
Misra A, Wasir JS, Vikram NK. Waist circumference criteria for the diagnosis of abdominal obesity are not applicable uniformly to all populations and ethnic groups. Nutrition. 2005;21:969–76.
Acknowledgements
The authors would like to thank all study subjects for participating in the present DFTJ cohort study as well as all volunteers for assisting in collecting the samples and data.
Funding
This work was supported by the grants from the National Natural Science Foundation (grants NSFC-81473051 and 81522040) and the Program for HUST Academic Frontier Youth Team. The funders were not involved in the design, conduct, or reporting of the study.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request and subject to appropriate ethics approvals.
Author information
Authors and Affiliations
Contributions
JY analyzed the data, interpreted the results, and wrote the manuscript. JY and FW conceptualized the research question and designed the study. JW, XH, HH and CZY provided consultation on methodology and helped with analysis interpretation. XPM and SW performed the statistical data analysis, and contributed to the interpretation of results. JY, PY, YJW, WHC, YL, HG, XMZ, DZ, YHT, HDY and MAH provided critical revisions to the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study approved by Ethics and Human Subject Committee of the School of Public Health, Tongji Medical College, and Dongfeng General Hospital, the Dongfeng Motor Corporation. All participants provided written informed consents.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. Age-adjusted correlation coefficient among anthropometric indices in men and women. Table S2. Comparison of AUC among different anthropometric indices in men and women. Figure S1. Flowchart of the participants included in the present analysis. (PDF 91 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Yang, J., Wang, F., Wang, J. et al. Using different anthropometric indices to assess prediction ability of type 2 diabetes in elderly population: a 5 year prospective study. BMC Geriatr 18, 218 (2018). https://doi.org/10.1186/s12877-018-0912-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-018-0912-2