
Abstract
Objective
This study aimed at utilizing a Bayesian approach semi-competing risks technique to model the underlying predictors of early recurrence and postoperative Death in patients with colorectal cancer (CRC).
Methods
In this prospective cohort study, 284 patients with colorectal cancer, who underwent surgery, referred to Imam Khomeini clinic in Hamadan from 2001 to 2017. The primary outcomes were the probability of recurrence, the probability of Mortality without recurrence, and the probability of Mortality after recurrence. The patients ‘recurrence status was determined from patients’ records. The Bayesian survival modeling was carried out by semi-competing risks illness-death models, with accelerated failure time (AFT) approach, in R 4.1 software. The best model was chosen according to the lowest deviance information criterion (DIC) and highest logarithm of the pseudo marginal likelihood (LPML).
Results
The log-normal model (DIC = 1633, LPML = -811), was the optimal model. The results showed that gender(Time Ratio = 0.764: 95% Confidence Interval = 0.456–0.855), age at diagnosis (0.764: 0.538–0.935 ), T3 stage (0601: 0.530–0.713), N2 stage (0.714: 0.577–0.935 ), tumor size (0.709: 0.610–0.929), grade of differentiation at poor (0.856: 0.733–0.988), and moderate (0.648: 0.503–0.955) levels, and the number of chemotherapies (1.583: 1.367–1.863) were significantly related to recurrence. Also, age at diagnosis (0.396: 0.313–0.532), metastasis to other sites (0.566: 0.490–0.835), T3 stage (0.363: 0.592 − 0.301), T4 stage (0.434: 0.347–0.545), grade of differentiation at moderate level (0.527: 0.387–0.674), tumor size (0.595: 0.500–0.679), and the number of chemotherapies (1.541: 1.332–2.243) were the significantly predicted the death. Also, age at diagnosis (0.659: 0.559–0.803), and the number of chemotherapies (2.029: 1.792–2.191) were significantly related to mortality after recurrence.
Conclusion
According to specific results obtained from the optimal Bayesian log-normal model for terminal and non-terminal events, appropriate screening strategies and the earlier detection of CRC leads to substantial improvements in the survival of patients.
Similar content being viewed by others

Introduction
The third leading cause of cancer death is colorectal cancer, with a high level of burden [1]. Surveillance, Epidemiology, and End Results (SEER) 18 registry showed an incidence rate of up to 3.56 per 100,000 in gastrointestinal sites [2]] [[3]. The prevalence of colorectal cancer is higher in men than women [4]. Another study showed an increasing recent trends in colorectal cancer mortality [5]. Given that the burden of cancer is increasing, the goal is to reduce mortality from such non-communicable diseases by 2030. The burden of colorectal cancer can be reduced by intervening on modifying factors such as diet, lifestyle, and early detection of polyps using screening [6].
Considering that surgery as the initial treatment, the recurrence rate in the first 5 years after surgery is 12.8% for local recurrence and 25.6% for distant metastasis [7] [8]. In addition, 60–80% of recurrences of colorectal cancer appear in two years after surgery [5]. These patients have low survival if early recurrence occurs [6]. If recurrence and metastasis of the disease are diagnosed early, it may be possible to improve survival with curative surgery [7] [8]. By predicting recurrence and metastasis, appropriate treatment of patients with colorectal cancer can be prescribed after surgery [9]. The main goal of follow-up programs after colorectal cancer treatment is to increase survival.
Several studies have been carried out to study the risk factors of recurrence and survival in patients with colorectal cancer. The 3 and five year survival rates in patients without recurrence were 88.4% and 87.6%, respectively. Also, results showed that pT4 (HR: 4.06, 95%CI: 1.60-10.29, p = 0.003) was a risk factor for mortality [9]. Another study was conducted to recognize factors affecting recurrence in patients with colorectal cancer at a regional Australian hospital [10]. The study by Heinemann and Karl aimed to provide a brief overview of clinics, diagnosis, and management of some of the best colorectal cancer predispositions in this regard [11]. The incidence of colorectal cancer was lower in men than in women, so it was tried to improve the results of colorectal cancer in women by introducing new gender-specific methods [12]. In a five year cohort study, the effect of recurrence risk factors in patients with CRC after initial treatment revealed the effect of age, tumor location, lymphovascular invasion, and tumor stage on patient recurrence was significant [13]. Lymphovascular invasion, carcinoembryonic antigen (CEA), and prognostic factors, including metastatic and venous invasion, were identified as the risk factors for recurrence in colon and rectal cancers [14].
Depending on the study conditions and the characteristics of patients, various factors may affect the recurrence and the interval between recurrence and death, and studies have shown that there is no appropriate agreement for its determinants [5] [6] [9]. On the other hand, semi-competing risks refer to situations in which the main scientific interest in estimating and inferring concerning a non-terminal event (e.g., premature recurrence), the occurrence of which depends on a terminal event (e.g., death) [15]. Each of these must be appropriately considered so as not to cause bias in the results [16]. Few articles have considered them simultaneously, and most have been within the framework of the Cox model for the hazard function. Bayesian framework semi-competing risks modelling, wherein data may include left-truncation and, or interval-censoring, are very robust. Therefore, this study aimed to identify the predictors of recurrence, death and death after recurrence after curative surgery in patients with colorectal cancer, utilizing a semi-competing risk approach under the illness-death model.
Methods
Study design and setting
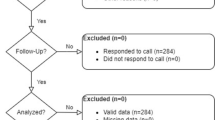
In this prospective cohort study, 284 patients with colorectal cancer, who underwent surgery, referred to Imam Khomeini clinic in Hamadan from 2001 to 2017.
Predictors
All demographic and clinical/pathological information were extracted from patients’ records. These included demographic variables such as age at the time of diagnosis (years), gender (female:1; male:2), and Body Mass Index (BMI: kg/m2), and clinical/pathological variables such as metastasis to other sites (no:0; yes:1), cancer site (colon:1; rectum:2), surgery (no:0; yes:1), radiotherapy (no:0; yes:1), chemotherapy (no:0; yes:1), number of chemotherapy (0:no; 1:<6; 2:6+), morphology (0:no adeno; 1:adeno), grade (differentiation level) (1:well; 2:moderate; 3:poor), tumor size (1:<4; 2: >=4 < 7; 3:=>7), disease stage(1:B; 2:C;3:D), PT-stage(1:T2; 2:T3; 3:T4; 4:Tx), and PN-stage(1:N2; 2:N3; 3:N4; 4:Nx).
Main outcome variables
Patients’ recurrence status was determined from patients’ records. The time to recurrence of patients, the non-terminal event, was computed from the date of surgery to local or distant recurrence in months (totally considered to experience the non-terminal event), and individuals who did not have recurrence or death until the end of the study were considered as censors. The death of the patients, the terminal event, was computed from the surgery date to their death according to the researchers’ telephone follow-up. Also, regarding the follow-up and the need to be in contact after the illness, the exact address and two contact numbers were received and recorded in the patient’s file.
Statistical analyses
Data were explained as mean (SD), median (min-max) for the normal and non-normal numeric variables, respectively, and frequency (percent) for categorical variables. The occurrence rate of the non-terminal event (recurrence) and the terminal event (death) was computed per 1000 persons. Log-rank tests were carried out to compare the survival rates across age at diagnosis, gender, BMI, metastasis to other sites, cancer site, surgery, radiotherapy, and chemotherapy, number of chemotherapy, morphology, grade of differentiation, tumor size, disease stage, PT-stage, and PN-stage. Also, the adjusted survival curves were plotted for significant variables in the multivariable analysis. These parts of the studies were conducted using Stata17 software (StataCorp, College Station, Texas, USA). To assess the relationship of above-mentioned variables with outcomes including the probability of the non-terminal event, the probability of the terminal event, and the conditional probability of the terminal event after non-terminal event, semi-competing risks analysis was utilized under the illness-death model with AFT approach. These outcomes were specified by three hazard functions in the Bayesian illness-death models. Accordingly, a Gibbs random sampling algorithm was used to generate samples from the complete posterior distribution. Deviance information criterion (DIC) and Logarithm of the pseudo marginal likelihood (LPML) were considered to compare the models.
Accelerated failure time models for independent semi-competing risks data
The AFT assumption can be used to compare survival times. One of the AFT model assumptions is that the effect of covariates on survival time is multiplicative [17]. The following AFT model was considered for the data analysis
Ti1 and Ti2 were considered as times to the non-terminal and terminal events, respectively. In each of the equations above, let xig be a vector of transition-specific covariates, let βg denote a vector of transition-specific regression parameters, and it is assumed εig is a transition-specific random variable, g = 1, 2, 3. Also, in each of expressions (1)–(3), γi is a study subject-specific frailty that instills positive dependence between the non-terminal and terminal events and It is assumed that γi is adopted from a normal distribution with mean of zero and variance of θ. In addition, it is considered the variance component θ adopted a conjugated inverse gamma distribution, which is defined by IG (a(θ), b(θ)). For regression parameters, βg is adopted non-informative flat prior on the real line parametric modeling, which was built on the log-normal distribution, and take the εig follows a normal (µg, σ2g) distribution. For µg, was assumed non-informative flat priors on the real line and for σ2g, independent inverse Gamma distributions, denoted by IG (ag(σ), bg(σ)).
To enrich the study, also was used a semi-parametric framework. In many cases, due to the unrealistic features of some common models, including the thin tail of the normal distribution, compared to the observed data distribution, the results of parametric models are not satisfactory, therefore, semi-parametric models can enrich the study.
So for each εig was adopted an independent non-parametric Dirichlet process mixtures (DPM) of Mg normal distributions with mean µgr and variance σ2gr, r∈ {1… Mg }.
Bayesian models were compared with two effective measures, DIC and LPML for recognizing the true model. The smaller DIC values indicate that the model has a better fit for the data [18]. The larger LPML values also indicate that the model has a good fit for the data [19].
This part of the analyses were carried out using R 4.1 software utilizing a SemiCompRisks package [20]. The significance level was set at 0.05.
Results
Patients profile
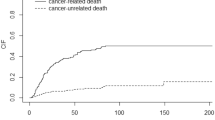
Out of 284 patients with resected CRC, 150 (52.8%) were mal. A total of 121 (42.6%) patients died, and 131 (46.1%) patients had a recurrence, of which 105 (80.2%) patients died by the end of the study. In addition, there were 16 (10.5%) patients who experienced death without experiencing the recurrence. The recurrence rate was about 46% in the colon, and rectum cancer sites. The mean age at diagnosis was 55.6 (SD 13.1) years, with an age range of 21–84 years. In addition, the mean age at diagnosis in patients with and without recurrence was 56.7 (SD 13.4) and 54.7 (SD 12.8) years, respectively. The median survival of patients was 61.0 (95% Confidence Interval (CI): 42.2–79.8) months. Besides, median survival was 47.0 (95% CI: 21.0–73.0) months for patients with recurrence. The total percentage of recurrences by the end of the first, second, third, fourth, and fifth years were 64.1%, 82.4%, 89.3%, 93.9%, and 96.2%, respectively. Only 3.8% of recurrences occurred after five years and the median recurrence time in patients with and without recurrence was 7 and 46 months, respectively. Moreover, the 1-, 3-, 5- and 10-year survival probabilities were 86.9%, 62.1%, 50.4%, and 42.3%, respectively, for the terminal event, and the 1-, 3-, 5- and 10-year survival probabilities were 67.4%, 51.9%, 45.3%, and 40.3%, respectively for the non-terminal event. The mean and median time distance between non-terminal and terminal events was 26.2 (95% CI: 19.1–33.2) and 10.0 (95% CI: 7.8–12.2) months, respectively. After disease recurrence, 1-, 3-, 5- and 10-year survival probabilities were 67.4%, 51.9%, 45.3%, and 40.3%, respectively.
Also, among patients who had a recurrence by the end of the study, 110 (84%) had metastases to other sites, 12 (9.2%) did not attend chemotherapy sessions, and 76 (58%) attended more than six sessions. Seven (5.3%) were in stage T2 and 92 (70.2%) were in stage T3, 11 (8.4%) were in stage Nx, and 55 (42%) were in stage N0. Among patients who had died by the end of the study, 94 (77.7%) had metastases to other sites, 12 (9.9%) had not attended chemotherapy sessions, and 61 (50.4%) had attended more than six sessions, 7 (5.8%) were in stage T2, and 85 (70.3%) were in stage T3, 10 (8.3%) were in stage Nx, and 45 (37.2%) were in stage N1.
Result of log-rank tests
According to the results of log-rank tests, age at diagnosis (years) (p = 0.001), metastasis to other sites (p = < 0.001), number of chemotherapies (p = 0.041), disease stage (p < 0.001), PT-stage (p < 0.001) and PN-stage (p < 0.001) were significant in both non-terminal and terminal events. In recurrence and dath outcomes, significantly higher outcome rates were observed among higher age categories, with substantially higher rates in age > 70. The rate of recurrences and death were 38.22, and 26.38, respectively. Also, those patients who had metastasis to other sites had much higher rates of both outcomes. The rate of recurrences and death were, 79.58, and 29.46, respectively. In addition, < 6 number of chemotherapies were associated with higher events than patients who had not had any chemotherapy. The rate of recurrences and death were, 17.40, and 16.38, respectively; however, the rates decreased when coming into 6 + chemotherapies. Non-terminal and terminal event rates raised significantly as the disease stage, PT-stage, and PN-stage levels increased a P < 0.05). Furthermore, comparing the occurrence rate in non-terminal and terminal events, it is evident that the occurrence rate is much higher in the recurrence than in the death outcome.
Model comparison
For Bayesian Independent AFT model with log-normal baseline survival distribution, we observed a DIC = 1633 and a LPML = -811. As well as, for Bayesian Independent AFT model with DPM baseline survival distribution we observed a DIC = 1759 and a LPML =-816. According to DIC and LPML, the Bayesian Independent AFT model with log-normal baseline survival distribution was the best model, accordingly the results of this optimal model were followed.
Result of bayesian AFT log-normal model
According to the results, the ratio of recurrence survival time was lower in men than in women (Time Ratio (TR) = 0.764: 95% CI 0.456–0.855). Age at diagnosis was associated with a lower survival time in all recurrence (0.764: 0.538–0.935), death without recurrence (0.396: 0.313–0.532) for, and death after recurrence (0.659: 0.559–0.803). Metastasis to other sites was associated with a lower time ratio of death without recurrence (0.566: 0.490–0.835). The number of chemotherapy sessions was associated with a higher survival time for all three recurrence (1.583: 1.367–1.863), death without recurrence (1.541: 1.332–2.243), and death after recurrence (2.029: 1.792–2.191). Grade of differentiation at moderate level was associated with a lower survival time for recurrence (0.648: 0.503–0.955) and death without recurrence (0.527: 0.387–0.674), however, at a weak level of differentiation, it was associated with a lower time ratio of recurrence (0.856: 0.733–0.988). Tumor size was linked with a lower time ratio for recurrence (0.709: 0.610–0.929), and for death without recurrence (0.595: 0.500–0.679). PT Stage at T3 was associated with a lower time ratio for recurrence (0.601: 0.530–0.713), and for death without recurrence (0.363: 0.592 − 0.301). T4 stage was associated with a lower time ratio for death without recurrence (0.434: 0.347–0.545). PN stage at N1 increased the time ratio for death without recurrence (1.974: 1.728–2.122) and N2 level also decreased the time ratio for recurrence (0.714: 0.577–0.935), (Table 1).
Result of bayesian AFT DPM model
According to the results, the time ratio of recurrence (0.835) was lower in men than in women. Age at diagnosis was associated with a decrease in the time ratio for recurrence (0.956). Metastasis to other sites was associated with an increase in the time ratio of recurrence (1.063), and a decrease in the time ratio for recurrence after death (0.946). The number of chemotherapy sessions significantly increased the time ratio of death after recurrence (1.045), (Table 2).
Discussion
This study aimed to utilize the Bayesian framework of semi-competing risks to model the effect of background and clinical characteristics on recurrence and postoperative death in patients with CRC. Therefore, the effect of these variables on the non-terminal event (recurrence), the probability of the terminal event (death without recurrence), and the conditional probability of the terminal event on the non-terminal event (death after recurrence). The results of this study demonstrate that, the Bayesian AFT log-normal model was the best model, consistent with DIC and LPML. Accordingly, the results showed that gender, age at diagnosis, T-stage, N-stage, tumor size, grade of differentiation, and number of chemotherapies were significantly related to the recurrence outcome. Also, age at diagnosis, metastasis to other sites, T-stage, grade of differentiation, tumor size, and the number of chemotherapies significantly predicted the death without recurrence. In addition, age at diagnosis, and the number of chemotherapies were significantly related to death after recurrence.
The illness-death model is utilized because of its association with common methods for survival analysis and also, its software is available although the hazard ratio, a commonly used measure of association in survival analysis. This is by no means the only measure that researchers may choose to calculate and report the outcomes. The AFT model has a perceptive physical explanation, and easily model the logarithm of the survival time over the explanatory variables [21]. There was a strong association between the terminal and non-terminal events in the current study, therefore, the simple utilization of a univariate survival model for the non-terminal event, would lead to an overestimation of the terminal event rates, because the analysis considers the terminal event as an independent censoring mechanism [22]. Utilizing semi-competing risk analysis, the terminal event is regarded as competing event, and the dependence between the two events is assumed to be part of the model specifications.
The Bayesian approach is a scientific and practical, and an alternative to the frequent approaches, and are simply possible due to computational advances and available software. Considering the analysis of semi-competing risks data, the proposed AFT illness-death model supply as a beneficial complement to the more traditional hazard-based approach [23][24]. In this study, a Bayesian framework was applied that allows to simultaneously address three important scientific goals in the semi-competing risk data settings: estimating regression parameters, describing the within-subject dependence between two event times, and predicting outcomes. Therefore, AFT models with frailty were fitted with log-normal parametric and DPM non-parametric baseline hazards functions.
Grzenda used a similar model to analyze the duration of the first job among young people. For this purpose, four Weibull, Gamma, Log-normal, and Log-Logistic models with the Bayesian approach were proposed. Based on the comparison of the models using the DIC index, the gamma model was a good fit for the data [25]. Lee outlined a new Bayesian framework for an AFT illness-death model, wherein DIC and LMPL indices were used to compare the models [26]. Ganjali conducted a study to evaluate the duration of unemployment in conditions where the proportional hazard assumption was not assumed. For this purpose Bayesian log-logistic, log-normal, and Weibull AFT models were used [27]. Marcus Abiso Arango utilized three common Bayesian joint models with AFT Weibull, log-normal, and log-logistics probability distributions, and they decided on Bayesian logistics model as the final model utilizing DIC, AIC, and BIC indices [28].
We utilized a non-informative prior distribution such as Jeffrey’s prior, because it gives inferential results similar to those of the best frequentist methods [29]. In Bayesian analysis, a balance is always seek for between prior information and information from data; in the one hand, the prior information should not overwhelm the evidence from the data, in the other hand, a strong enough prior is required to support weak evidence that usually comes from insufficient data. This, sometimes is decided after performing sensitivity analysis to check the dependence of the results on the choice of a prior, a controversial issues associated with Bayesian analysis. So, choosing non-informative priors can be a great solution to achieve this balance, as well, by assigning equal probabilities to all possible states of the parameter space, can rectify the subjectivity problem. Another positive point about the Bayesian analysis and considering a non-informative prior is that even if the prior is improper, the corresponding posterior distribution may still be proper [30].
Recurrence affects survival and death in the first five years after recurrence in patients with curative resection, as reported in some studies [31][32][33]. In some studies, the 5-year cumulative recurrence rates were 4.9%, 11.0%, and 23.5% for stage I, stage II, and stage III tumors, respectively [8]. In patients with colon cancer, local recurrence was less than in patients with rectal cancer [34].
In this study, the postoperative survival rate was decreased in older ages. In the line of this study, Baghestani showed that age at diagnosis was significantly related to a patient’s survival time [35], as well, some studies reported similar results [36][37]. Also, in other studies, age was significantly associated with local and distance recurrence [38][39][40]. Also, age was significantly associated with the survival of patients with colorectal cancer. In these studies, it has been reported that higher age was associated with a decrease in patient survival [41][42][43]. However, in some other studies, no significant association was reported [44][45][46][47]. In addition, several studies have shown a significant association between age and 5-year survival [48][40]. For that reason, early screening in adults to diagnose cases can increase the survival time ratio in patients with colorectal cancer.
The findings of several studies are in the line with the results of the current study, wherein the ratio of survival time was lower in men than women for recurrence outcome. Although in some studies, results have shown that sex was not significantly associated with survival time [49][36], in one study showed that men had lower survival than women [50], and in another study, 5-year survival in the second step was higher in women than men [40]. So appropriate screening strategies should be considered.
Metastasis to other sites was another factor that showed a significant association with non-terminal and terminal events. Other studies showed similar results [38][39]. The rate of grade I tumors was significantly upper in the group that had late metastasis (35.1% vs. 64.9%, P = 0.001)[51]. In this study metastasis to other sites was associated with decreased survival time of Death without experiencing recurrence. Another study showed that the liver and lung were the first and second well-known sites of recurrence, respectively [34]. As a result, patients should be under intensive care in this regard.
According to the current study, grade of differentiation and tumor size were associated with a decrease in recurrence survival time. Moderate differentiation grade and tumor size was associated with decreased time ratio for death without recurrence. in some studies, patients with stage III tumors had low recurrence rates [52][53].
As a complementary treatment after surgery, the number of chemotherapies was significantly related to greater survival of non-terminal and terminal events and non-terminal event condition of the terminal event. Several studies have reported that postoperative adjuvant therapy with fluorouracil and levamisole, as standard adjuvant chemotherapy, reduces mortality in patients with colorectal cancer [54][55], as well as, chemotherapy effectively reduced the recurrence [56][57]. Therefore, chemotherapy can be suggested to decline the hazard of recurrence and death.
In the present study, PT stages, and T-stages were associated with decreased time ratio for death without recurrence, and PN-stage, and PT-stages were associated with a decrease in recurrence survival time. It has been shown that T3 to T4 were significantly and effectively associated with stage in patients CRC [58], as well, PT-stage and PN-stage were significantly related to early recurrence [59]. Also it was reported that the mortality rate was higher in patients with higher stages of colon cancer [60][61]. According to a study, in the higher stages of CRC, the rate of local recurrence and metastasis has been shown to be higher [62]. PN-Stage hase been shown to be effective on recurrence [63]. Therefore, cancer extent in the body should be determined and appropriate treatment should be assigned according to the stage of cancer.
Limitation of the study
As the first limitation, there was a difficulty in fitting Bayesian models, which was minimized by using appropriate approaches in modeling, selecting the appropriate initial values in the models, and selecting the appropriate amount of memory for the systems running the program. In particular, more cases are needed to achieve higher statistical precision. Another limitation of the present study was its generalizability, because the participants in this study were specific in terms of environmental, cultural, social, and geographical conditions, so the results of this study should be interpreted with cautions when would be generalize to other individuals and communities. There are some restricting assumptions in utilizing the proposed models in the current study, and only linear effects of the predictors were considered. Accordingly, machine learning methods such as neural networks, classification algorithms, and regression trees automatically consider linear and nonlinear interaction relationships and possibly provide more accurate results. For our upcoming project, we intend to follow machine learning methods.
Conclusion
This study demonstrated, according to the Bayesian AFT log-normal model, as the best model, that gender, older age, higher pathological, higher T/N stage, and fewer chemotherapy sessions were significantly related to the lower survival time ratio of patients with CRC. According to specific results obtained for terminal and non-terminal events, appropriate screening strategies and the earlier detection of CRC may lead to substantial improvements in the survival of patients.
Availability of data and materials
The data that support the findings of this study are available from MAJ, but restrictions are applied to the availability of these data, which were used under license for the current study, and are not publicly available.
Data are, however, available from the authors upon reasonable request by MAJ.
References
Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Gastroenterol Rev Gastroenterol. 2019;14(2):89–103.
Dasari A, et al. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017;3(10):1335–42.
Grossi U, et al. Mixed adenoneuroendocrine carcinoma (MANEC) of the lower gastrointestinal tract: A systematic review with Bayesian hierarchical survival analysis. Eur J Surg Oncol. 2021;47(11):2893–9.
Wild CP, Stewart BW, Wild C. World cancer report 2014. Switzerland: World Health Organization Geneva; 2014.
Alves CMM, Souza VGB, Bastos RR. “Colorectal cancer mortality in Mato Grosso, Brazil: Spatiotemporal trends,” Geospat. Health, vol. 15, no. 1, 2020.
Alvares D, Haneuse S, Lee C, Lee KH. SemiCompRisks: an R package for the analysis of independent and cluster-correlated semi-competing risks data. R J. 2019;11(1):376.
Abulafi AM, Williams NS. Local recurrence of colorectal cancer: the problem, mechanisms, management and adjuvant therapy. J Br Surg. 1994;81(1):7–19.
Manfredi S, Bouvier AM, Lepage C, Hatem C, Dancourt V, Faivre J. Incidence and patterns of recurrence after resection for cure of colonic cancer in a well defined population. J Br Surg. 2006;93(9):1115–22.
Inoue A, et al. Risk Factors for Recurrence in Patients with Pathological Stage II Colorectal Cancer. Gan To Kagaku Ryoho. 2021;48(13):1938–40.
Holt J, Schwalb H, Elbourne H, Te Marvelde L, Reid C. Risk factors for recurrence in colorectal cancer: a retrospective analysis in a regional Australian hospital. ANZ J Surg. 2021;91(11):2482–6.
Heinimann K. Hereditary Colorectal Cancer: Clinics, Diagnostics and Management. Ther Umsch. 2018;75(10):601–6.
Sung-Eun HY, Paik H, Yoon JE, Lee N, Kim, Sung M-K. Sex-and gender-specific disparities in colorectal cancer risk. World J Gastroenterol WJG. 2015;21(17):5167.
Zare-Bandamiri M, Fararouei M, Zohourinia S, Daneshi N, Dianatinasab M. Risk factors predicting colorectal cancer recurrence following initial treatment: a 5-year cohort study. Asian Pac J cancer Prev APJCP. 2017;18(9):2465.
Yamano T, et al. Evaluation of appropriate follow-up after curative surgery for patients with colorectal cancer using time to recurrence and survival after recurrence: a retrospective multicenter study. Oncotarget. 2018;9(39):25474.
Fine JP, Jiang H, Chappell R. On semi-competing risks data. Biometrika. 2001;88(4):907–19.
Odell PM, Anderson KM, D’Agostino RB. “Maximum likelihood estimation for interval-censored data using a Weibull-based accelerated failure time model,” Biometrics, pp. 951–959, 1992.
Gail M, Krickeberg K, Samet JM, Tsiatis A, Wong W. “Statistics for Biology and Health Series Editors.” Atlanta: Springer, 2012.
Spiegelhalter DJ, Best NG, Carlin BP, Van Der Linde A. Bayesian measures of model complexity and fit. J R Stat Soc Ser b (statistical Methodol. 2002;64(4):583–639.
Liu JS. The collapsed Gibbs sampler in Bayesian computations with applications to a gene regulation problem. J Am Stat Assoc. 1994;89(427):958–66.
Alvares D, Haneuse S, Lee C, Lee KH. SemiCompRisks: an R package for the analysis of independent and cluster-correlated semi-competing risks data. R J. 2019;11(1):376.
Wei L-J. The accelerated failure time model: a useful alternative to the Cox regression model in survival analysis. Stat Med. 1992;11:no. 14–5. pp. 1871–1879.
Haneuse S, Lee KH. Semi-Competing Risks Data Analysis: Accounting for Death as a Competing Risk When the Outcome of Interest Is Nonterminal. Circ Cardiovasc Qual Outcomes. 2016;9(3):322–31. doi:https://doi.org/10.1161/circoutcomes.115.001841.
Xu J, Kalbfleisch JD, Tai B. Statistical analysis of illness–death processes and semicompeting risks data. Biometrics. 2010;66(3):716–25.
Lee KH, Haneuse S, Schrag D, Dominici F. Bayesian semi-parametric analysis of semi-competing risks data: investigating hospital readmission after a pancreatic cancer diagnosis. J R Stat Soc Ser C Appl Stat. 2015;64(2):253.
Grzenda W. “Modelling the duration of the first job using Bayesian accelerated failure time models,” Acta Univ. Lodz. Folia Oeconomica, vol. 4, no. 330, 2017.
Lee KH, Rondeau V, Haneuse S. Accelerated failure time models for semi-competing risks data in the presence of complex censoring. Biometrics. 2017;73(4):1401–12.
Ganjali M, Baghfalaki T. “Bayesian analysis of unemployment duration data in the presence of right and interval censoring,” J. Reliab. Stat. Stud., pp. 17–32, 2012.
Erango MA, Goshu AT, Buta GB, Dessisoa AH. Bayesian joint modelling of survival of HIV/AIDS patients using accelerated failure time data and longitudinal CD4 cell counts. Br J Med Med Res. 2017;20(6):1–12.
Agresti A. An introduction to categorical data analysis. John Wiley & Sons; 2018.
Thompson J. Bayesian analysis with Stata. Stata Press College Station, TX; 2014.
Kaibori M, et al. Predictors and outcome of early recurrence after resection of hepatic metastases from colorectal cancer. Langenbeck’s Arch Surg. 2012;397(3):373–81.
Viganò L, et al. Early recurrence after liver resection for colorectal metastases: risk factors, prognosis, and treatment. A LiverMetSurvey-based study of 6,025 patients. Ann Surg Oncol. 2014;21(4):1276–86.
Yamashita Y, et al. Risk factors for early recurrence after curative hepatectomy for colorectal liver metastases. Surg Today. 2011;41(4):526–32.
Ryuk JP, et al. Predictive factors and the prognosis of recurrence of colorectal cancer within 2 years after curative resection. Ann Surg Treat Res. 2014;86(3):143–51.
Baghestani AR, Daneshvar T, Pourhoseingholi MA, Asadzade H. Survival of colorectal cancer patients in the presence of competing-risk. Asian Pac J Cancer Prev. 2014;15(15):6253–5.
Li X-P, et al. Colorectal cancer concealment predicts a poor survival: a retrospective study. Asian Pac J Cancer Prev. 2013;14(7):4157–60.
Morrison DS, et al., “Behavioural and metabolic risk factors for mortality from colon and rectum cancer: analysis of data from the Asia-Pacific Cohort Studies Collaboration,” 2013.
Alafchi B, Roshanaei G, Tapak L, Abbasi M, Mahjub H. Joint modelling of colorectal cancer recurrence and death after resection using multi-state model with cured fraction. Sci Rep. 2021;11(1):1–10.
Safari M, Mahjub H, Esmaeili H, Abbasi M, Roshanaei G. “Specific causes of recurrence after surgery and mortality in patients with colorectal cancer: A competing risks survival analysis,” J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci., vol. 26, 2021.
Heidarnia MA, Monfared ED, Akbari ME, Yavari P, Amanpour F, Mohseni M. Social determinants of health and 5-year survival of colorectal cancer. Asian Pac J Cancer Prev. 2013;14(9):5111–6.
Dancourt V, Quantin C, Abrahamowicz M, Binquet C, Alioum A, Faivre J. Modeling recurrence in colorectal cancer. J Clin Epidemiol. 2004;57(3):243–51.
Ansari R, et al. Survival analysis of colorectal cancer in patients underwent surgical operation in Shariati and Mehr Hospital-Tehran, in a retrospective study. Govaresh. 2007;12(1):7–15.
Vakili M, Aghakoochak A, Pirdehghan A, Shiryazdy M, Saffarmoghadam A, “The survival rate of patients with colorectal cancer in Yazd during 2001–2011,” SSU_Journals, vol. 22, no. 3, pp. 1187–1195, 2014.
Chong DQ, et al. Association of family history and survival in patients with colorectal cancer: a pooled analysis of eight epidemiologic studies. Cancer Med. 2018;7(5):2192–9.
Jayasekara H, et al. Associations of alcohol intake, smoking, physical activity and obesity with survival following colorectal cancer diagnosis by stage, anatomic site and tumor molecular subtype. Int J cancer. 2018;142(2):238–50.
Meyerhardt JA, et al. Physical activity and survival after colorectal cancer diagnosis. J Clin Oncol. 2006;24(22):3527–34.
Fernandez FG, Drebin JA, Linehan DC, Dehdashti F, Siegel BA, Strasberg SM. Five-year survival after resection of hepatic metastases from colorectal cancer in patients screened by positron emission tomography with F-18 fluorodeoxyglucose (FDG-PET). Ann Surg. 2004;240(3):438.
Wrigley H, Roderick P, George S, Smith J, Mullee M, Goddard J. Inequalities in survival from colorectal cancer: a comparison of the impact of deprivation, treatment, and host factors on observed and cause specific survival. J Epidemiol Community Heal. 2003;57(4):301–9.
Azadeh S, Reza FS, Sara A, Mohsen V, Bijan M-D, Zali ZR. Four years incidence rate of colorectal cancer in Iran: a survey of national cancer registry data-implications for screening. Asian Pac J Cancer Prev. 2012;13(6):2695–8.
Aarts MJ, Lemmens VEPP, Louwman MWJ, Kunst AE, Coebergh JWW. Socioeconomic status and changing inequalities in colorectal cancer? A review of the associations with risk, treatment and outcome. Eur J Cancer. 2010;46(15):2681–95.
Yazilitas D, Özdemir N, Hocazade C, Demirci NS, Zengin N. The clinical and pathological features affecting the time of relapse in patients with early stage colorectal cancer. J Cancer Res Ther. 2016;12(4):1257.
André T, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol. 2009;27(19):3109–16.
Obrand DI, Gordon PH. Incidence and patterns of recurrence following curative resection for colorectal carcinoma. Dis colon rectum. 1997;40(1):15–24.
Wolmark N, et al. The benefit of leucovorin-modulated fluorouracil as postoperative adjuvant therapy for primary colon cancer: results from National Surgical Adjuvant Breast and Bowel Project protocol C-03. J Clin Oncol. 1993;11(10):1879–87.
Zaniboni A. Adjuvant chemotherapy in colorectal cancer with high-dose leucovorin and fluorouracil: impact on disease-free survival and overall survival. ” J Clin Oncol. 1997;15(6):2432–41.
Newland RC, et al. Competing risks analysis of the effect of local residual tumour on recurrence and cancer-specific death after resection of colorectal cancer: implications for staging. Pathology. 2018;50(6):600–6.
Tsikitis VL, Larson DW, Huebner M, Lohse CM, Thompson PA. Predictors of recurrence free survival for patients with stage II and III colon cancer. BMC Cancer. 2014;14(1):1–7.
Wang B, et al. Tumor location as a novel high risk parameter for stage II colorectal cancers. PLoS ONE. 2017;12(6):e0179910.
Lan Y-T, et al. Comparison of clinicopathological characteristics and prognosis between early and late recurrence after curative surgery for colorectal cancer. Am J Surg. 2014;207(6):922–30.
Kaiser AM, Kang J, Chan LS, Beart RW. The prognostic impact of the time interval to recurrence for the mortality in recurrent colorectal cancer. Color Dis. 2006;8(8):696–703.
Aquina CT, et al. The impact of age on complications, survival, and cause of death following colon cancer surgery. Br J Cancer. 2017;116(3):389–97.
Belot A, Remontet L, Launoy G, Jooste V, Giorgi R. Competing risk models to estimate the excess mortality and the first recurrent-event hazards. BMC Med Res Methodol. 2011;11(1):1–9.
Miyoshi N, et al. Novel prognostic prediction models for patients with stage IV colorectal cancer after concurrent curative resection. ESMO open. 2016;1(3):e000052.
Acknowledgements
We would like to appreciate the collaboration of the department of biostatistics and epidemiology, the school of medicine, Zanjan University of medical sciences, for providing the environment for modeling data and manuscript writing.
Funding
This study was supported by a research deputy of Zanjan University of medical sciences (Project no: A-11-1721-1).
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript. LM and GR conceived the study and participated in the design and data collection. LM, GR, RF, and MAJ participated in the data analysis and manuscript preparation.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The institutional review board of Zanjan university of medical sciences approved the protocol of the study (ethics code: IR.ZUMS.REC.1400.419). The participants’ privacy was preserved. All participants filled and signed the informed consent and assent. Also, all methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mahmoudi, L., Fallah, R., Roshanaei, G. et al. A bayesian approach to model the underlying predictors of early recurrence and postoperative death in patients with colorectal Cancer. BMC Med Res Methodol 22, 269 (2022). https://doi.org/10.1186/s12874-022-01746-y
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-022-01746-y