
Abstract
Background
The objectives of the present study was to evaluate the effect of fluid challenge (FC) on ventriculo-arterial (V-A) coupling, its determinants: arterial elastance and ventricular elastance, and ability to predict fluid responsiveness.
Methods
Thirty patients admitted to cardio-thoracic ICU in whom the physician decided to perform FC were included. Arterial pressure, cardiac output, arterial elastance, and ventricular elastance, were measured before and after FC with 500 ml of lactated Ringer’s solution. Fluid responders were defined as patients with more than a 15% increase in stroke volume. V-A coupling was evaluated by the arterial elastance to ventricular elastance ratio.
Results
Twenty-three (77%) of the 30 patients included in the study were fluid responders. Before FC, responders had higher arterial elastance and arterial elastance to ventricular elastance ratio. FC significantly increased mean arterial pressure, stroke volume and cardiac output, and significantly decreased systemic vascular resistance, arterial elastance and consequently the arterial elastance to ventricular elastance ratio. Changes in arterial elastance were correlated with changes in stroke volume, systemic vascular resistance, and arterial compliance. Baseline arterial elastance to ventricular elastance ratio over 1.4 predicted fluid responsiveness (area under the curve [95% confidence interval]: 0.84 [0.66–1]; p < 0.0001).
Conclusions
Fluid responsiveness patients had V-A coupling characterized by increase arterial elastance to ventricular elastance ratio, in relation to an increase arterial elastance. Fc improved the V-A coupling ratio by decreasing arterial elastance without altering ventricular elastance. Arterial elastance changes were related to those of systemic vascular resistance (continue component) and of arterial compliance (pulsatile component).
Similar content being viewed by others


Background
Fluid challenge (FC) is the most commonly performed bedside haemodynamic intervention in critical care medicine. In conventional haemodynamic analysis, cardiac output (CO) is considered to be a continuous function, and the heart and vascular system are considered separately. Two different concepts have therefore been developed [1, 2]. Guyton et al. considered the heart to be a pump driven by continuous flow from a purely resistive circuit - despite the pulsatile nature of this flow (mean atrial pressure – right atrial pressure = CO x systemic vascular resistance) [1]. Several authors subsequently developed a model of stroke volume (SV) based on the pressure-volume relationships of the ventricle and the vascular system [2,3,4]. This model considers left ventricular (LV) energetics, myocardial function and ventricular performance by taking into account the interaction between the ventricle and the vascular system. Hence, LV end-systolic elastance (ELV) corresponds to LV contractility and arterial elastance (EA) corresponds to the effective elastance of the arterial system [2,3,4]. Given that the ventricular and the arterial systems operate simultaneously, ventriculo-arterial (V-A) coupling (i.e the EA/ELV ratio) reflects the mechanical efficiency of the cardiovascular system by analysing the interaction between cardiac performance and vascular function. V-A coupling determines the SV and the ejection pressure (i.e. arterial blood pressure) [2, 4].
Studies have demonstrated that V-A coupling can describe and characterize pathophysiological mechanisms, evaluate treatment effects, and may represent a parameter that describes the energetic cost [5,6,7]. Moreover, there is wide evidence that V-A coupling is a hemodynamic parameter that is associated with patient outcomes [5, 8, 9]. The relevance of V-A coupling as a parameter of hemodynamic optimization could be related to the fact that V-A coupling is a parameter of cardiovascular efficiency whereas the classical hemodynamic parameters are exclusively parameters of cardiovascular efficacy. The clinical relevance of this model is based on the fact that EA/ELV predicts outcomes independently from other parameters [5, 8, 9].
The optimal hemodynamic intervention in patients with acute circulatory failure would improve efficacy with the lowest energetic cost (high efficiency) for the cardiovascular system (i.e lower EA/ELV ratio) [8]. Because treatment of acute circulatory failure comprises several medications (fluid infusion, vasopressor use …), it would be of interest to know the effect of each treatment on V-A coupling [6, 8, 9]. Few studies have focused on FC from the perspective of the V-A coupling model [9]. A description of the cardiovascular effects of FC may improve our understanding of the pathophysiology of haemodynamic states.
The main objective of this study was therefore to evaluate the impact of FC on V-A coupling, and its determinants. The secondary objective was to determine the value of the pre-challenge EA/ELV ratio as a predictor of a post-challenge increase in SV.
Methods
Ethics
The study’s objectives and procedures were approved by the local independent ethics committee (Comité de Protection des Personnes Nord-Ouest II, Amiens, France; RNI2014–39 on November 26th, 2014). According to French law, all patients received written information about the study and provided their verbal consent to participate. The present manuscript was drafted in compliance with the STROBE checklist for cohort studies [10].
Patients
This prospective, observational study was performed in the Amiens University Hospital cardiothoracic ICU (Amiens, France) during 1 year between 2015 and 2016. The main inclusion criteria were as follows: age 18 or over, controlled positive ventilation, and a clinical decision to perform FC for volume expansion within the first hours of admission to ICU. Exclusion criteria were permanent arrhythmia, cardiac conduction block, pacemaker (or need for temporary pacemaker using epicardial wires), norepinephrine, epinephrine or dobutamine, poor echogenicity, aortic regurgitation, and right heart dysfunction. The indications for FC were arterial hypotension (systolic arterial pressure (SAP) less than 90 mmHg, or mean arterial pressure (MAP) less than 65 mmHg), or SV change greater than 10% during a passive leg raising manoeuvre, or clinical signs of hypoperfusion (skin mottling, and capillary refill time greater than 3 s).
Haemodynamic parameters
Transthoracic echocardiography (with the CX50 ultrasound system and an S5–1 Sector Array Transducer, Philips Medical System, Suresnes, France) was performed by a physician blinded to the study outcomes. Left ventricular ejection fraction (LVEF), end-systolic volume (ESV), and end-diastolic volume (EDV) were measured using Simpson’s method on a four-chamber view. The aortic velocity-time integral (VTIAo), pre-ejection time and systolic time were measured by pulsed Doppler at the left ventricular outflow tract on a five-chamber view. Stroke volume (SV; mL) was calculated as VTIAo×SAo, and was expressed as indexed SV (SVi) = SV/body surface area (ml.m− 2). Cardiac output (CO) was calculated as SV × heart rate (HR), and was expressed as indexed CO (CI) = CO/ body surface area (ml min− 1 m− 2). Mean echocardiographic parameters were calculated from five measurements (regardless of the respiratory cycle) and analysed retrospectively.
Left ventricular end-systolic elastance, arterial elastance, ventricular-arterial coupling
ELV, an index of ventricular contractility, was evaluated by using the non-invasive, single-beat method described by Chen et al. [11]. This method is based on the assumption that time-variation of left ventricular elastance is not influenced by loading conditions or heart rate. ELV was calculated by the formula: ELV = (Pd – (ENd(test) * Pes * 0.9)) / (SV * ENd(test)). ENd(test) was obtained from a group-averaged normalized elastance curve value at this same time td (ENd(avg)), baseline LVEF and the ratio of diastolic to systolic arterial pressure (Pd / Pes) [12]. ENd(avg) was determined by a seven-term polynomial function that includes the ratio of pre-ejection period to total systolic period [11]. We calculated the coefficient of variation (CV), precision and least significant change (LSC) for ELV in the first ten patients. CV was 7.7% ± 0.6 and LSC was 10.9% ± 0.8.
Sunagawa et al. demonstrated that arterial load could be characterized in the time domain as arterial elastance (EA) [2]. EA was calculated as end systolic pressure (ESP)/ SV (mmHg ml− 1) where ESP is 0.9 x systolic arterial pressure (SAP) [13].
Arterial pressure was measured by an invasive radial artery approach. In healthy men and women, mean EA/ELV, EA, and ELV values measured invasively at rest are 1.0 ± 0.36, 2.2 ± 0.8 mmHg.ml− 1, and 2.3 ± 1.0 mmHg.ml− 1, respectively [14, 15]. In the present study, patients with an EA/ELV ratio over 1.36 were classified as uncoupled [15].
The total energy generated by each cardiac contraction is called the “pressure-volume area” (PVA), corresponding to the sum of the external mechanical work exerted during systole (SW) and the potential energy (PE) stored at the end of systole: PVA = SW + PE [16]. SW is calculated as end systolic pressure (ESP) x SV. PE is calculated as ESP x ((ESV-V0)/2), and assumes that V0 is negligible compared to ESV. The SW/PVA ratio corresponds to the mechanical efficiency of converting the total mechanical energy (PVA) available to the left ventricular SW [16]. The SW/PVA ratio is associated to myocardial oxygen consumption.
Indexed systemic vascular resistance (SVRi) (mmHg.ml-1.m− 2) was calculated as MAP-central venous pressure (CVP)/ cardiac index (CI), and total arterial compliance (CA) (ml.mmHg− 1) was calculated as SV/arterial pulse pressure [17].
Study procedures
The following clinical parameters were recorded: demographic, ventilation parameters, and primary diagnosis. After an equilibration period, capillary refill time (measured at the distal phalanx of the index finger), heart rate (HR), systolic arterial pressure (SAP), MAP, diastolic arterial pressure (DAP), CVP, SVi, CI, EDV, ESV, pre-ejection time, systolic time interval, and blood gas levels were measured at baseline. In the present study, FC always consisted of a 10-min infusion of 500 ml of lactated Ringer’s solution [18, 19]. A second set of measurements was performed immediately after FC. All patients were mechanically ventilated in volume-controlled mode with a tidal volume set at 7–9 ml kg− 1 ideal body weight, and a positive end-expiratory pressure (PEEP) of 5–8 cmH2O. Ventilator settings were not modified during the study period.
Statistical analysis
The sample size was calculated on the reproducibility initially measured in the study reported by Chen et al. [11]. With a reproducibility of 20%, we calculated that a sample of thirty patients would be sufficient to demonstrate an absolute change of more than 20% in the EA/ELV ratio in response to FC. The distribution of the variables was assessed by a Shapiro-Wilk test. Data are expressed as number, proportion (in per cent), mean ± standard deviation (SD) or median [interquartile range (IQR)], as appropriate. Fluid response was defined as a greater than 15% increase in SV after FC [19, 20]. This cutoff value was considered to be clinically relevant and in accordance with measurement variability. The non-parametric Wilcoxon rank sum test, Student’s paired t test, Student’s t test, and the Mann-Whitney test were used to assess statistical significance, as appropriate. A receiver-operating characteristic curve was established for the ability of EA, ELV, the EA/ELV ratio to predict a greater than 15% increase in SV. The limit for statistical significance was p < 0.05. SPSS® software (version 22, IBM, New York, NY, USA) was used for all statistical analyses.
Results
Thirty patients were included and analysed (Fig. 1). These patients had undergone cardiovascular surgery (n = 29) or thoracic surgery (n = 1) (Table 1). The main indications for fluid expansion were arterial hypotension (n = 17), SV change greater than 10% with PLR (n = 9), skin mottling (n = 4). No significant difference in indications was observed between SV responders and SV non-responders (p = 0.336). Values for EA, ELV and EA/ELV ratio were not significantly different between men and women, or according to type of surgery or medical characteristics (p-value > 0.05), therefore allowing pooled analysis (Table 1). No patients developed complications (arrhythmia, hypoxaemia, left heart failure) during FC.

Study flow chart
Effect of FC on haemodynamic parameters in the overall study population
Prior to FC, median EA was 2.3 [1.7–2.8] mmHg.ml− 1, median ELV was 1.5 [1–1.7] mmHg.ml− 1, and median EA(ESP)/ELV ratio was 1.8 [1.3–2.3]. Twenty-three (80%) of the 30 patients were classified as “uncoupled”. After FC, median EA was 2.1 [1.5–3], median EA/ELV ratio was 1.6 [1.3–2.1], and median ELV was 1.4 [0–1.7]. Twenty-three (77%) of the 30 patients were classified as fluid responders. Most uncoupled patients (21 out of 23 (91%); p = 0.003) were fluid responders.
Effect of FC on haemodynamic parameters depending on SV changes
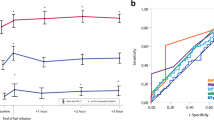
At baseline, EA, EA/ELV, were higher and CA, CI, SVi were lower in fluid responders than in fluid non-responders (Table 2, Fig. 2). In fluid responders, FC was associated with higher values for blood pressure, SVi, CI, SW, PVA, and SW/PVA ratio, and lower values for HR, SVRi, EA and EA/ELV ratio (Table 2, Fig. 2, supplementary file 1). In fluid non-responders, FC was associated with higher values for CVP and EA/ELV ratio and a lower SW/PVA ratio (Table 2).

Changes in ventricular pressure-volume relationships in fluid responders with fluid challenge. Stroke volume increased (SV➔SV1), and end-diastolic volume (EDV➔EDV1) increased more than end-systolic pressure (ESP➔ESP1), resulting in decreased arterial elastance (EA➔EA1). Ventricular elastance (EEL) remained unchanged, resulting in a decreased EA/EEL ratio
Correlations between haemodynamic parameters, EA and their changes
EA changes were correlated with those of SV (r = 0.858, p < 0.001), SVRi (r = − 0.898, p < 0.001), CA (r = 0.729, p < 0.001), and LVEF (r = − 0.620, p < 0.001). MAP changes were correlated with those of EA (r = 0.479, p = 0.0001), SVRi (r = 0.468, p = 0.009), ELV (r = 0.421, p = 0.021), and CA (r = − 0.543, p = 0.002).
Predictive value of EA, ELV, EA/ELV ratio and PPV
At baseline, the EA/ELV ratio predict fluid responsiveness with an AUC of 0.84 [95% confidence interval (95% CI)] (0.66–1), An EA/ELV cut-off of 1.4 gave a sensitivity of 87% [66–97], a specificity of 86% [42–100], a positive likelihood ratio of 6.1, negative likelihood ratio of 0.15, a positive predictive value of 95 and a negative predictive value of 67. With an AUC [95% CI] of 0.75 [0.58–0.94] (p = 0.001), EA was poorly predictive of fluid responsiveness. With an AUC [95% CI] of 0.39 [0.13–0.66] (p = 0.541), ELV did not predict fluid responsiveness.
Discussion
In fluid responders, V-A coupling was characterized by a high pre-challenge EA/ELV ratio due to high EA with respect to ELV. Because FC was associated with SV increase, it has improved V-A coupling. The baseline EA/ELV ratio was a predictor of fluid responsiveness. This effect was associated with a decrease of EA without changes of ELV. EA changes were related to those of systemic vascular resistance (continue component) and of arterial compliance (pulsatile component). Improving V-A coupling was associated with a better myocardial work efficiency (i.e lower myocardial work for a better SV and blood pressure).
Few studies have specifically evaluated the effect of FC on V-A coupling. One study in postoperative cardiac surgical patient found an increase in SW, PVA and afterload, as a result of increased SV [21]. A subsequent study of septic shock patients assessed the impact of FC on EA and its components [17]. According to V-A coupling concept, an increase of preload may lead to an increase of SV and EA [2]. We observed a decrease after FC [21]. These results are close to those of Guarracino et al. who demonstrated a decrease of EA with FC [17]. Several explanations for our findings can be proposed.
The sympathetic nervous system plays a key role (via the baroreflex) in regulating blood volume, blood flow and blood pressure [22]. Accordingly, preload-dependent patients probably have higher levels of sympathetic activation than non-dependent patients, as evidenced by higher EA, higher systemic vascular resistance, and lower arterial compliance values at a given blood pressure. This response is designed to adapt blood flow to the patient’s needs, which appears to be effective, as ScVO2 and arterial lactate levels were not significantly different between the two groups of patients. FC restores preload and blood flow, and thus meets the patient’s needs. A decrease in EA might be caused by several interlinked mechanisms affecting the resistive component (HR and SVR) and the pulsatile component (CA) of arterial load. The increase in blood pressure induced by an increase in CO decreases sympathetic activation, systemic vascular resistance and EA. The baroreflex has been shown to maintain adequate blood pressure by modulating EA, ELV and blood volume [23]. An increase in blood flow decreases vascular tone by activating the NO pathway and by initiating vascular recruitment [24]. As a result of shear stress, blood flow modulates the diameter of blood vessels and can influence aortic compliance [25]. Segers et al. used a heart-artery interaction model to show that the contribution of the resistive component to this effect is threefold higher than that of the pulsatile component [26].
V-A coupling in clinical practice
The present study demonstrated that neither EA nor ELV, but only EA/ELV ratio defines the response of left ventricle to fluid expansion. In other words, the EA/ELV ratio, which characterizes the interaction between the ventricle and the arterial vascular system defines which patient will be fluid responder. We specifically included patients not treated with vasopressors and inotropes to avoid any treatment-related bias. Hence, we can safely assume that our results were related to the sole effect of FC. Based on our results and those of previous studies performed in ICU, anaesthesia and cardiologic area, the V-A coupling represents a hemodynamic model that is able to predict the effects of each hemodynamic therapeutic, and their impact on clinical outcomes [6,7,8,9]. Authors have already demonstrated that optimizing V-A coupling was associated with better lactate clearance and patient survival [8, 9].
When the EA/ELV ratio is over 1.36, the main determinant to be firstly optimized should be EA. Arterial elastance is easy to obtain at bedside. Hypotensive preload dependent patients have often V-A uncoupling because of high EA (> 2.2) in relation to low SV and higher sympathetic activation in order to maintain tissue perfusion. The hemodynamic therapeutic would be to decrease EA by using FC [17]. The second step may evaluate ELV to evaluate the EA/ELV ratio. One limitation could be the measure of ELV because of Chen ‘s formula. A mobile phone application has been developed to easily calculate ELV. Simpler formulas have been developed but they are not interchangeable to track variations of EA/ELV ratio with therapeutic intervention [27].
Another method based on V-A coupling could be the use of the dynamic arterial elastance which is the ratio of stroke volume variation to pulse pressure variation [28]. The dynamic arterial elastance can be easely measured with invasive and non-invasive hemodynamic devices [29,30,31]. Dynamic arterial elastance is a real time indicator of the interaction between the heart and the vascular system that has been challenged as an indicator of V-A coupling [32, 33]. Several clinical studies have demonstrated that dynamic arterial elastance is able to predict SV and blood pressure response to FC or norepinephrine, and it can be used to optimize treatment [17, 29,30,31,32, 34]. Recently, dynamic arterial elastance was demonstrated to be inversly correlated to V-A coupling, and track its changes [33]. The final clinical relevance of V-A coupling for ICU patients will require well designed interventional trials evaluating a hemodynamic optimization based on V-A coupling, its determinants or a surrogate such as dynamic arterial elastance.
This study presents a number of limitations. We did not register the study on clinical trial database. The study population may have differed from septic shock patients. Most of our patients presented perioperative hypovolaemia, whereas septic patients generally have acute circulatory failure with a combination of hypovolaemia, changes in microvascular perfusion and central-to-peripheral arterial decoupling. The methods used to calculate ELV and EA can be open to criticism because we did not use a high-fidelity ventricular pressure catheter. We measured ELV by a non-invasive single-beat method based on a linear end-systolic pressure-volume relationship, and a constant volume axis intercept of the end-systolic pressure volume relationship [10, 29]. Calculation of ELV assumes that the end-systolic pressure-volume relationship is load-independent, with a linear slope, and that V0 is not influenced by inotropes [29]. We calculated ESP from a radial artery signal, which may differ from the aortic pressure signal. However, radial artery pressure has been reported to provide a good estimate of ESP [14, 35]. It can be argued that estimation of ESP from the radial artery has not been fully validated, any error in this method would only affect the precision of absolute values of EA and ELV, but not the EA/ELV ratio, as the error in end-systolic pressure would be similar. The predictive value of EA/ELV for increased SV can therefore be considered to be valid. Arterial load assessment was based on a two-element Windkessel model and integrative simplification. More precise models have been developed, such as three- and four-element Windkessel models that include arterial impedance and wave reflection. However, these methods would be difficult to apply at the bedside. Despite these limitations, non-invasive evaluation of ELV and EA was validated against the gold standard method, and has been used in cardiac surgery [5]. In the present study, EA and ELV must be considered to be approximations of EA and ELV.
Conclusions
In fluid responders, V-A coupling was characterized by a high pre-challenge EA/ELV ratio due to high EA with respect to ELV. Because FC was associated with SV increase, it has improved V-A coupling. This effect was associated with a decrease of EA without changes of ELV. Measuring V-A coupling can characterize the patient’s haemodynamic status and predict the cardiovascular system’s response to FC. Further studies are need to confirm the clinical relevance of optimizing V-A coupling in ICU patients.
Availability of data and materials
Unfortunately, we do not have permissions to share these data. However, we would be happy to collaborate with requests from individual research groups would like to access our raw data. Please contact the corresponding author for further information.
Abbreviations
- CA :
-
Arterial compliance
- CO:
-
Cardiac output
- CI:
-
Cardiac index
- CV:
-
Coefficient of variation
- CVP:
-
Central venous pressure
- EA :
-
Arterial elastance
- ELV :
-
Ventricular elastance
- EDV:
-
End diastolic volume
- ESP:
-
End systolic pressure
- ESV:
-
End systolic volume
- FC:
-
Fluid challenge
- HR:
-
Heart rate
- LVEF:
-
Left ventricular ejection fraction
- LSC:
-
Least significant change
- PVA:
-
Pressure volume area
- V-A coupling:
-
Ventriculo-arterial coupling
- SVRi:
-
Indexed systemic vascular resistance
- SV:
-
Stroke volume
- SW:
-
Stroke work
References
Guyton AC. Textbook of medical physiology. 5th ed. Philadelphia: W.B. Saunders; 1976.
Sunagawa K, Maughan WL, Burkhoff D, Sagawa K. Left ventricular interaction with arterial load studied in isolated canine ventricle. Am J Phys. 1983;245:773–80.
Sagawa K, Suga H, Shoukas AA, et al. End-systolic pressure/volume ratio: a new index of ventricular contractility. Am J Cardiol. 1977;40:748–53.
Sunagawa K, Sagawa K, Maughan WL. Ventricular interaction with the loading system. Ann Biomed Eng. 1984;12:163–89.
Maurer MS, Sackner-Bernstein JD, El-Khoury Rumbarger L, Yushak M, King DL, Burkhoff D. Mechanisms underlying improvements in ejection fraction with Carvedilol in heart failure. Circ Heart Fail. 2009;2:189–96.
Guinot PG, Longrois D, Kamel S, Lorne E, Dupont H. Ventriculo-arterial coupling analysis predicts the hemodynamic response to norepinephrine in hypotensive postoperative patients: a prospective observational study. Crit Care Med. 2018;46:e17–25.
Aslanger E, Assous B, Bihry N, et al. Association between baseline cardiovascular mechanics and exercise capacity in patients with coronary artery disease. Anatol J Cardiol. 2016;16:608–13.
Chang MC, Mondy JS, Meredith JW, et al. Redefining cardiovascular performance during resuscitation: ventricular stroke work, power, and the pressure-volume diagram. J Trauma. 1998;45:470–8.
Morelli A, Ertmer C, Westphal M, et al. Effect of heart rate control with esmolol on hemodynamic and clinical outcomes in patients with septic shock: a randomized clinical trial. JAMA. 2013;310:1683–91.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147:573–7.
Chen CH, Fetics B, Nevo E, Rochitte CE, Chiou KR, Ding PA, Kawaguchi M, Kass DA. Noninvasive single-beat determination of left ventricular end-systolic elastance in humans. J Am Coll Cardiol. 2001;38:2028–34.
Asanoi H, Sasayama S, Kameyama T. Ventriculo arterial coupling in normal and failing heart in humans. Circ Res. 1989;65:483–93.
Kelly RP, Ting CT, Yang TM, Liu CP, Maughan WL, Chang MS, Kass DA. Effective arterial elastance as index of arterial vascular load in humans. Circulation. 1992;865:513–21.
Starling MR. Left ventricular-arterial coupling relations in the normal human heart. Am Heart J. 1993;125:1659–66.
Chen CH, Nakayama M, Nevo E, Fetics BJ, Maughan WL, Kass DA. Coupled systolic-ventricular and vascular stiffening with age: implications for pressure regulation and cardiac reserve in elderly. J Am Coll Cardiol. 1998;32:1221–7.
Takaoka H, Takeuchi M, Odake M, Yokoyama M. Assessment of myocardial oxygen consumption (VO2) and systolic pressure volume area (PVA) in human hearts. Eur Heart J. 1992;13:85–90.
Guarracino F, Bertini P, Pinsky MR. Cardiovascular determinants of resuscitation from sepsis and septic shock. Crit Care. 2019;23(1):118.
Guinot PG, Marc J, de Broca B, Archange T, Bar S, Abou-Arab O, Dupont H, Fischer MO, Lorne E. The predictability of dynamic preload indices depends on the volume of fluid challenge: a prospective observational study in the operating theater. Medicine (Baltimore). 2018;97(42):e12848.
Guinot PG, Urbina B, Broca B, Bernard E, Dupont H, Lorne E. Predictability of the respiratory variation of stroke volume varies according to the definition of fluid responsiveness. Br J Anaesth. 2014;112:580–1.
De Broca B, Garnier J, Fischer MO, et al. Stroke volume changes induced by a recruitment maneuver predict fluid responsiveness in patients with protective ventilation in the operating theater. Medicine (Baltimore). 2016;95(28):e4259.
Mangano DT, Van Dyke DC, Ellis RJ. The effect of increasing preload on ventricular output and ejection in man. Limitations of the Frank-Starling Mechanism. Circulation. 1980;62:535–41.
Wehrwein EA, Joyner MJ. Regulation of blood pressure by the arterial baroreflex and autonomic nervous system. Handb Clin Neurol. 2013;117:89–102.
Sakamoto T, Kakino T, Sakamoto K, Tobushi T, Tanaka A, Saku K, Hosokawa K, Onitsuka K, Murayama Y, Tsutsumi T, Ide T, Sunagawa K. Changes in vascular properties, not ventricular properties, predominantly contribute to baroreflex regulation of arterial pressure. Am J Physiol Heart Circ Physiol. 2015;308:H49–58.
Calver A, Collier J, Green D, Vallance P. Effect of acute plasma volume expansion on peripheral arteriolar tone in healthy subjects. Clin Sci (Lond). 1992;83:541–7.
Snow HM, McAuliffe SG, Moors JA, Brownlie R. The relationship between blood flow and diameter in the iliac artery of the anaesthetized dog: the role of endothelium-derived relaxing factor and shear stress. Exp Physiol. 1994;79:635–45.
Segers P, Stergiopulos N, Westerhof N. Relation of effective arterial elastance to arterial system properties. Am J Physiol Heart Circ Physiol. 2002;282:H1041–6.
Nguyen M, Berhoud V, Bartamian L, Martin A, Ellouze O, Bouhemad B, Guinot PG. Agreement between different non-invasive methods of ventricular elastance assessment for the monitoring of ventricular-arterial coupling in intensive care. J Clin Monit Comput. 2019. https://doi.org/10.1007/s10877-019-00397-7.
Monge García MI, Gil Cano A, Gracia RM. Dynamic arterial elastance to predict arterial pressure response to volume loading in preload-dependent patients. Crit Care. 2011;15(1):R15.
Cecconi M, Monge García MI, Gracia Romero M, et al. The use of pulse pressure variation and stroke volume variation in spontaneously breathing patients to assess dynamic arterial elastance and to predict arterial pressure response to fluid administration. Anesth Analg. 2015;120:76–84.
Bar S, Leviel F, Abou Arab O, et al. Dynamic arterial elastance measured by uncalibrated pulse contour analysis predicts arterial-pressure response to a decrease in norepinephrine. Br J Anaesth. 2018;121:534–40.
Guinot PG, Bernard E, Levrard M, Dupont H, Lorne E. Dynamic arterial elastance predicts mean arterial pressure decrease associated with decreasing norepinephrine dosage in septic shock. Crit Care. 2015;19:14.
Bar S, Huette P, Abou-Arab O, Dupont H, Lorne E, Guinot PG. Dynamic arterial elastance might not be an indicator of ventriculo-arterial coupling. Br J Anaesth. 2018;121:672–3.
Monge García MI, Jian Z, Hatib F, Settels JJ, Cecconi M, Pinsky MR. Dynamic arterial Elastance as a Ventriculo-arterial coupling index: an experimental animal study. Front Physiol. 2020;11:284.
Guinot PG, Abou-Arab O, Guilbart M, et al. Monitoring dynamic arterial elastance as a means of decreasing the duration of norepinephrine treatment in vasoplegic syndrome following cardiac surgery: a prospective, randomized trial. Intensive Care Med. 2017;43(5):643–51.
Monge Garcia MI, Jian Z, Settels JJ, Hatib F, Cecconi M, Pinsky MR. Reliability of effective arterial elastance using peripheral arterial pressure as surrogate for left ventricular end-systolic pressure. J Clin Monit Comput. 2019;33(5):803–13.
Acknowledgements
None.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Data acquisition: PGG, PH, OAA; Analysis and interpretation: PGG, PH, OAA; DL; Drafting of the manuscript for important intellectual content: PGG, DL. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted by the Comité de Protection des Personnes Nord-Ouest II, Amiens, France, RNI2014–39). According to French law, all patients had written information and gave verbal consent to participate.
Consent for publication
Not applicable.
Competing interests
Guinot Pierre-Grégoire and Abou-Arab Osama are members of the editorial board of the BMC Anesthesiology journal (associate Editor).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huette, P., Abou-Arab, O., Longrois, D. et al. Fluid expansion improve ventriculo-arterial coupling in preload-dependent patients: a prospective observational study. BMC Anesthesiol 20, 171 (2020). https://doi.org/10.1186/s12871-020-01087-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-020-01087-7