
Abstract
Background
Catecholamines are the first-line vasopressors used in patients with septic shock. However, the search for novel drug candidates is still of great importance due to the development of adrenergic hyposensitivity accompanied by a decrease in catecholamine activity. Terlipressin (TP) is a synthetic vasopressin analogue used in the management of patients with septic shock. In the current study, we aimed to compare the effects of TP and catecholamine infusion in treating septic shock patients.
Methods
A systematic review and meta-analysis was conducted by searching articles published in PUBMED, EMBASE, and the Cochrane Central Register of Controlled Trials between inception and July 2018. We only selected randomized controlled trials evaluating the use of TP and catecholamine in adult patients with septic shock. The primary outcome was overall mortality. The secondary outcomes were the ICU length of stay, haemodynamic changes, tissue perfusion, renal function, and adverse events.
Results
A total of 9 studies with 850 participants were included in the analysis. Overall, no significant difference in mortality was observed between the TP and catecholamine groups (risk ratio(RR), 0.85 (0.70 to 1.03); P = 0.09). In patients < 60 years old, the mortality rate was lower in the TP group than in the catecholamine group (RR, 0.66 (0.50 to 0.86); P = 0.002). There was no significant difference in the ICU length of stay (mean difference, MD), − 0.28 days; 95% confidence interval (CI), − 1.25 to 0.69; P = 0.58). Additionally, TP improved renal function. The creatinine level was decreased in patients who received TP therapy compared to catecholamine-treated participants (standard mean difference, SMD), − 0.65; 95% CI, − 1.09 to − 0.22; P = 0.003). No significant difference was found regarding the total adverse events (Odds Ratio(OR), 1.48(0.51 to 4.24); P = 0.47), whereas peripheral ischaemia was more common in the TP group (OR, 8.65(1.48 to 50.59); P = 0.02).
Conclusion
The use of TP was associated with reduced mortality in septic shock patients less than 60 years old. TP may also improve renal function and cause more peripheral ischaemia. PROSPERO registry: CRD42016035872.
Similar content being viewed by others
Background
Sepsis and septic shock are a grave consequence of infection, and the mortality is high [1, 2], despite the significant progress made in intensive care medicine. Volume resuscitation is the mainstay approach for management of septic shock, followed by vasoactive infusions to maintain appropriate arterial pressure and tissue perfusion. Early resuscitation in septic shock could raise the mean arterial pressure (MAP) to facilitate the tissue perfusion of organs and enhance the oxygen supply [3, 4].
No statistical significance has been shown in the survival benefit of one vasopressor over another. Norepinephrine is the first-recommended vasopressor according to the Surviving Sepsis Campaign [5]. The major cause of refractory hypotension in septic shock patients is insensitivity or no response to vasoactive agents [6]. Additionally, previous studies have reported significant adverse effects of high-dose catecholamines [7, 8].
Vasopressin (AVP) is an endogenously released stress hormone that is important during shock. Growing evidence has suggested that arginine vasopressin infusion is safe and effective, and it has been recommended as a first-line vasopressor for the treatment of septic shock [9, 10]. TP is an AVP analogue with a longer half-life (6 h) and duration of action (2 to 10 h) compared with vasopressin (half-life, 6 min; duration of action, 30 to 60 min). The preliminary clinical analysis revealed that TP effectively reduced the norepinephrine (NE) requirements of patients with septic shock [11, 12].
Studies comparing the use of TP and catecholamine showed conflicting results. In a meta-analysis, TP decreased the NE requirement and mortality rate in patients suffering from sepsis and septic shock [13]. A recent study demonstrated that there was no significant improvement in the 28-day mortality rate in patients treated with TP versus catecholamine. In this systematic review, we summarized the results from randomized controlled trials focusing on the comparison between TP and catecholamine treatments in septic shock using a meta-analysis. Our findings may provide important insights for future trial planning and the development of treatment guidelines.
Methods
Search for trials
This work was registered in the international prospective register of systematic reviews (PROSPERO registry number: CRD42016035872). We searched publications in the PUBMED, EMBASE and COCHRANE databases up to July 2018 using a sensitive search strategy combining the keywords and subject headings. Relevant articles were identified using the terms “shock, septic”, “terlipressin”, and “adults”. The reference lists of recent reviews and retrieved studies were examined. No date or language restrictions were used. We did not attempt to identify unpublished reports or contact authors for additional information.
Eligibility criteria
The inclusion criteria were as follows: 1) type of study: randomized controlled trials; 2) population: adult patients (> 18 years old) with septic shock; 3) intervention: catecholamine or TP to raise blood pressure; and 4) outcomes: a) primary outcomes: mortality at hospital discharge and b) secondary outcomes: length of ICU stay, haemodynamic indices, and renal function including the variables of serum creatine and urine volume. Studies with patients < 18 years old or without a control group were excluded.
Study selection
Independent screening of the titles and abstracts was carried out by two researchers. The full-text articles were assessed for eligibility following the inclusion/exclusion criteria. A third researcher was solicited in case of discrepancies.
Data extraction and outcomes
Data from all manuscripts were collected independently by three researchers using a data-recording form. Then, the extracted information was reviewed. Discrepancies among researchers were solved by consensus. All additional information was obtained from the principal investigators of the included studies.
The primary outcome was mortality (all causes) at the longest follow-up time. The secondary outcomes were the ICU length of stay, haemodynamic changes, tissue perfusion, renal function and adverse events.
Quality assessment
The Cochrane Risk of Bias Tool was used for the quality assessment. The following domains were evaluated: sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other sources of bias [14]. The risk of bis was labelled as high, unclear, or low. Any disagreements were resolved by a consensus discussion. The quality of the evidence in this systematic review was rated by the Grading of Recommendation Assessment, Development and Evaluation (GRADE) instrument [15, 16].
Statistical analysis
A random-effects model was used for the meta-analysis. The effect of the treatment on outcome measures was analysed using random-effects models. The difference between groups was shown as the pooled OR/RR with a 95% CI. For continuous outcomes, MDs/SMDs and 95% CIs were calculated. In some studies, the median value was reported as the measure of treatment effect, accompanied by the range or interquartile range (IQR). Before analysing the data, we estimated the mean from the medians and standard deviations (SDs) from the IQRs, as previously described [17]. Heterogeneity was determined using the I2 statistic. I2 < 50% indicated insignificant heterogeneity, and a fixed-effect model was used, whereas I2 > 50% was considered significant heterogeneity, and a random-effects model was used. In cases where heterogeneity was identified, sensitivity analyses were performed to investigate the influence of the individual studies on the overall estimate. A subgroup analysis for the primary outcome was also performed to explore the influencing factors and to evaluate the robustness of the primary outcome. The network graphs were produced in Stata 12.0 using the networkplot package. GeMTC (version 0.14.3) and OpenBUGS (version 3.2.2) were used to evaluate the effect of six therapies (vasopressin, dopamine, norepinephrine, terlipressin, TP plus norepinephrine, TP plus norepinephrine plus dopamine) on mortality. Data analyses were performed using Review Manager (Version 5.3), and P < 0.05 indicated statistical significance.
Subgroup analyses
Pre-specified subgroup analyses were performed in studies enrolling patients with proven septic shock and focusing on the comparison between TP and catecholamine infusion in patients with septic shock. Elderly patients were defined as those aged more than 60 years according to the WHO. Therefore, we further separated the studies enrolling patients with an average age of ≥60 years vs. those enrolling patients with an average age of < 60 years to determine which subpopulation may benefit more from TP treatment.
Results
Literature search
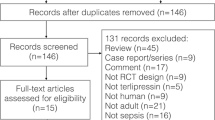
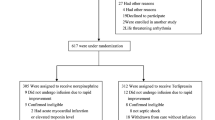
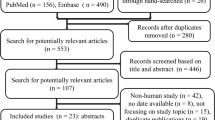
In a total of 171 citations, 148 were excluded after the initial title/abstract screening, leaving 23 articles for a full-text review. Of these, we selected 9 randomized controlled trials for the analysis (Fig. 1). Fourteen articles were excluded for the following reasons: animal studies (n = 6), paediatric subjects (n = 2), case report (n = 3), and outcome irrelevant (n = 3). Finally, 9 articles (850 patients) were included in the analysis [12, 18,19,20,21,22,23,24,25].

Study flow diagram
Study characteristics
The characteristics of the ten articles are presented in Table 1. Nine studies (850 patients) were included, in which 421 patients received TP and 429 patients received norepinephrine or dopamine. In all studies, conventional therapy with vasopressors/inotropes and volume resuscitation were given before the treatment with TP. In Fig. 2, the methodology of the quality assessment using the Cochrane Risk of Bias Tool is shown. There were three single- or double-blinded RCTs [20, 22, 25], and two open-label RCTs [18, 21]. The types of the other four RCTs were not mentioned in the articles [12, 19, 23, 24].

Risk of bias graph and risk of bias summary. Review authors’ judgement about each risk of bias item presented as percentages across all included studies and the authors’ judgement about each risk of bias item for each included study
Meta-analysis
Mortality in the hospital
TP infusion in patients with septic shock showed no significant impact on the mortality rate (RR, 0.85 (0.70 to 1.03); P = 0.09). In subgroups, the mortality rate in patients younger than 60 years old treated with TP was significantly decreased (RR, 0.66 (0.50 to 0.86); P = 0.002), whereas TP infusion did not influence mortality in patients older than 60 years (RR, 0.95 (0.80 to 1.12); P = 0.53) (Fig. 3).

Forest plot of the effect of terlipressin compared with catecholamine on mortality in patients with septic shock as determined by a meta-analysis using a random effects model
The network analysis showed no significant difference in the mortality between the TP group and the other five treatment regimen groups (all CIs crossed 1) (Table S2). The ‘TP plus norepinephrine’ regimen showed the best probability of cure (31%) compared to the other regimen groups (0 to 23%) (Fig. 4).

Rank probability graph of differences in mortality between different groups
Length of ICU stay
TP infusion in septic shock patients did not significantly decrease the ICU length of stay, with a pooled MD of − 0.28 days (reduction) and low heterogeneity (95% CI, − 1.25 to 0.69; I2 = 0%, P = 0.58) (Figure S1).
Haemodynamic variation
The addition of TP in septic shock treatment did not significantly decrease the cardiac index with a pooled SMD of − 0.19 and low heterogeneity (95% CI, − 0.58 to 0.19; I2 = 18%, P = 0.32) (Figure S2A). Compared to the catecholamine group, the TP group exhibited no significant effect on MAP variation, with a pooled SMD of 0.07 and intermediate heterogeneity (95% CI, − 0.51 to 0.66; I2 = 72%, P = 0.80) (Figure S2B). The addition of TP led to a significant reduction in the heart rate, with a pooled SMD of − 0.39 (reduction) and low heterogeneity (95% CI, − 0.73 to − 0,04; I2 = 44%, P = 0.03) (Figure S2C).
Tissue perfusion
The addition of TP in septic shock treatment may increase the risk of developing tissue ischaemia. Compared to the conventional treatment, TP resulted in a significant decrease in DO2 with a pooled SMD of − 0.58 and low heterogeneity (95% CI, − 1.15 to-0.02; I2 = 0%, P = 0.04) (Figure S3A). However, TP did not cause a significant reduction in VO2 (SMD, − 0.32(− 0.79 to 0.16); I2 = 0%, P = 0.20) (Figure S3B) and showed no significant effect on the Lac level (SMD, − 0.20(− 0.70 to 0.30); I2 = 0%, P = 0.43) (Figure S3C).
Organ function
Renal function was improved during TP infusion with the reestablishment of urine flow and a decrease in creatinine. Compared with catecholamine, TP increased the urine flow in septic shock patients with a pooled SMD of 0.49 and intermediate heterogeneity (95% CI, − 0.01 to 0.98; I2 = 55%, P = 0.05) (Figure S4A). Moreover, TP decreased the level of creatinine in patients with a pooled SMD of − 0.65 and low heterogeneity (95% CI, − 1.09 to 0.22; I2 = 0%, P = 0.003) (Figure S4B).
Adverse events
The pooled data displayed no significant difference in total adverse events between the two groups (OR 1.48, 95% CI, 0.51 to 4.24; I2 = 74%; P = 0.47) (Figure S5A). Arrhythmia was reported as an adverse event in three trials. However, the pooled data showed no difference in arrhythmia outcomes between the two groups (OR 0.66, 95% CI, 0.21 to 2.05; I2 = 32%; P = 0.47) (Figure S5B). Peripheral ischaemia was reported in two trials, and our pooled data showed that it was more common in the TP group (OR 8.65, 95% CI, 1.48 to 50.59; I2 = 71%; P = 0.02) (Figure S5C).
Discussion
In this meta-analysis, we compared the use of TP and catecholamine in patients with septic shock. No significant difference was observed in the mortality risk between TP- and catecholamine-treated adult patients, which was consistent with a previous meta-analysis [26]. Furthermore, we showed, for the first time, that TP infusion was associated with a lower mortality rate in patients less than 60 years old. Previous studies found that TP caused a significantly higher rate of digital ischaemia [22], and ageing was a major risk factor for ischaemic disorders, suggesting that TP may lead to more severe digital ischaemia in elderly patients. DeBacker et al. considered microcirculatory flow as a stronger predictor of outcome [27], which might be the reason that TP did not reduce mortality in elderly patients with septic shock. Studies have also shown that TP improved oxygenation [28]. Therefore, the mortality of these patients may be lower with the use of TP.
According to the results from the network analysis and the rank probability graphs, ‘TP plus norepinephrine’ ranked first, and treatments including TP ranked in the top three. In animal models, TP treatment improved the blood flow of the kidney, intestine, and liver. Additionally, combined treatment with TP and NE was superior to TP alone [29]. Thus, the administration of TP plus norepinephrine might serve as a therapeutic option for patients with septic shock.
Haemodynamic and oxygenation variables were summarized in this meta-analysis. The TP group did not show a significant elevation in MAP or a reduction in CI and MAP. TP can reduce cardiac performance by decreasing cardiac output. In a large group of septic shock patients, TP plus norepinephrine reversed hypotension at the expense of oxygen delivery and CI [30]. In our meta-analysis, however, TP did not affect cardiac performance compared with catecholamine.
We further showed that TP significantly decreased the heart rate, indicating that TP might prevent the progression of septic shock-associated myocardial dysfunction [31]. Recent evidence suggests that diastolic dysfunction is a common symptom and a key predictor of mortality in septic shock patients [32]. Additionally, adequate ventricular filling can be achieved with a decrease in heart rate in patients with diastolic dysfunction. Unfortunately, most articles included in this review did not report the causes of septic shock or the results of echocardiography.
Our meta-analysis demonstrated that TP ameliorated renal failure, increased urine flow and decreased creatinine. TP treatment has been encouraged for hepato-renal syndrome as it significantly increased urine output compared with baseline values and promoted creatinine clearance in a prospective open-label study [30]. However, the p-value for the analysis of urine flow was 0.05. Our data suggested that a larger sample size of patients would be needed to reach conclusive results.
We observed that the TP and catecholamine groups had the same rate of total adverse events, which was consistent with a previously published meta-analysis [26]. Furthermore, TP was associated with a higher risk of peripheral ischaemia in comparison to catecholamine treatment. TP acts on V1 receptors, which are located on the vascular smooth muscle, leading to vasoconstriction. Thus, patients treated with TP may have a higher risk of developing tissue ischaemia [33]. However, only four of the included studies reported total adverse events, which may not completely reflect TP-related adverse events during the study period.
TP regulates vascular tone by stimulating the contraction of vascular smooth muscle cells, and TP has been used to treat hypotension in septic shock patients with catecholamine resistance [34, 35]. Emerging evidence has shown that continuous infusion of TP at low doses is effective and safe in controlling sepsis-induced arterial hypotension. TP infusion also had similar survival outcomes as other first-line vasopressor agents [12, 36,37,38].
There are some limitations in our meta-analysis. First, most studies had a small sample size of less than 100 participants. Small-study effects might have led to a publication bias. Second, most studies were unblended (7 of 9), which may have affected the quality of the analysis and resulted in a risk of bias. Third, significant heterogeneity was seen in some outcomes, and the dose and usage were different in these trials. Fourth, the underlying causes of septic shock varied across these studies. Finally, the earliest study was published in 2005, the latest study was published in 2018, and the definition of sepsis changed over the duration.
Conclusions
The present meta-analysis has demonstrated the benefit of terlipressin in reducing mortality in younger patients (whose age was less than 60 years old) with septic shock. In addition, terlipressin can improve renal function in patients with septic shock, but it can also induce more peripheral ischaemia.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- APACHE:
-
Acute Physiology and Chronic Health Evaluation
- AVP:
-
Vasopressin
- CI:
-
Confidence interval
- GRADE:
-
Grading of Recommendation Assessment, Development and Evaluation
- ICU:
-
intensive care unit
- IQR:
-
Interquartile range
- MAP:
-
Mean arterial pressure
- MD:
-
Mean difference
- NE:
-
Norepinephrine
- RR:
-
Risk ratio
- SMD:
-
Standard mean difference
- SOFA:
-
Sequential Organ Failure Assessment
- TP:
-
Terlipressin
References
Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546–54.
Yende S, Austin S, Rhodes A, Finfer S, Opal S, Thompson T, et al. Long-term quality of life among survivors of severe Sepsis: analyses of two international trials. Crit Care Med. 2016;44(8):1461–7.
Hollenberg SM, Ahrens TS, Annane D, Astiz ME, Chalfin DB, Dasta JF, et al. Practice parameters for hemodynamic support of sepsis in adult patients: 2004 update. Crit Care Med. 2004;32(9):1928–48.
Holmes CL, Walley KR. Vasoactive drugs for vasodilatory shock in ICU. Curr Opin Crit Care. 2009;15(5):398–402.
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving Sepsis campaign: international guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017;43(3):304–77.
Landry DW, Oliver JA. The pathogenesis of vasodilatory shock. N Engl J Med. 2001;345(8):588–95.
Mullner M, Urbanek B, Havel C, Losert H, Waechter F, Gamper G. Vasopressors for shock. Cochrane Database Syst Rev. 2004;(3):Cd003709..
Schmittinger CA, Torgersen C, Luckner G, Schroder DC, Lorenz I, Dunser MW. Adverse cardiac events during catecholamine vasopressor therapy: a prospective observational study. Intensive Care Med. 2012;38(6):950–8.
Bassi E, Park M, Azevedo LC. Therapeutic strategies for high-dose vasopressor-dependent shock. Crit Care Res Pract. 2013;2013:654708.
Scarpati G, Piazza O. Vasopressin vs Terlipressin in treatment of refractory shock. Transl Med UniSa. 2013;5:22–7.
Leone M, Albanese J, Delmas A, Chaabane W, Garnier F, Martin C. Terlipressin in catecholamine-resistant septic shock patients. Shock. 2004;22(4):314–9.
Morelli A, Ertmer C, Rehberg S, Lange M, Orecchioni A, Cecchini V, et al. Continuous terlipressin versus vasopressin infusion in septic shock (TERLIVAP): a randomized, controlled pilot study. Crit Care. 2009;13(4):R130.
Serpa Neto A, Nassar AP, Cardoso SO, Manetta JA, Pereira VG, Esposito DC, et al. Vasopressin and terlipressin in adult vasodilatory shock: a systematic review and meta-analysis of nine randomized controlled trials. Crit Care. 2012;16(4):R154.
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–6.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5.
Albanese J, Leone M, Delmas A, Martin C. Terlipressin or norepinephrine in hyperdynamic septic shock: a prospective, randomized study. Crit Care Med. 2005;33(9):1897–902.
Xiao X, Zhang J, Wang Y, Zhou J, Zhu Y, Jiang D, et al. Effects of terlipressin on patients with sepsis via improving tissue blood flow. J Surg Res. 2016;200(1):274–82.
Chen Z, Zhou P, Lu Y, Yang C. Comparison of effect of norepinephrine and terlipressin on patients with ARDS combined with septic shock: a prospective single-blind randomized controlled trial. Zhonghua wei zhong bing ji jiu yi xue. 2017;29(2):111–6.
Choudhury A, Kedarisetty CK, Vashishtha C, Saini D, Kumar S, Maiwall R, et al. A randomized trial comparing terlipressin and noradrenaline in patients with cirrhosis and septic shock. Liver Int. 2017;37(4):552–61.
Liu ZM, Chen J, Kou Q, Lin Q, Huang X, Tang Z, et al. Terlipressin versus norepinephrine as infusion in patients with septic shock: a multicentre, randomised, double-blinded trial. Intensive Care Med. 2018;44(11):1816–25.
Morelli A, Ertmer C, Lange M, Dunser M, Rehberg S, Van Aken H, et al. Effects of short-term simultaneous infusion of dobutamine and terlipressin in patients with septic shock: the DOBUPRESS study. Br J Anaesth. 2008;100(4):494–503.
Hua F, Wang X, Zhu L. Terlipressin decreases vascular endothelial growth factor expression and improves oxygenation in patients with acute respiratory distress syndrome and shock. J Emerg Med. 2013;44(2):434–9.
Svoboda P, Scheer P, Kantorova I, Doubek J, Dudra J, Radvan M, et al. Terlipressin in the treatment of late phase catecholamine-resistant septic shock. Hepato-gastroenterology. 2012;59(116):1043–7.
Zhu Y, Huang H, Xi X, Du B. Terlipressin for septic shock patients: a meta-analysis of randomized controlled study. J Intensive Care. 2019;7:16.
De Backer D, Donadello K, Sakr Y, Ospina-Tascon G, Salgado D, Scolletta S, et al. Microcirculatory alterations in patients with severe sepsis: impact of time of assessment and relationship with outcome. Crit Care Med. 2013;41(3):791–9.
Kalambokis G, Baltayiannis G, Tsiouris S, Pappas K, Kokkinou P, Fotopoulos A, et al. Scintigraphic evaluation of intrapulmonary shunt in normoxemic cirrhotic patients and effects of terlipressin. Hepatol Res. 2010;40(10):1015–21.
Xiao X, Zhu Y, Zhen D, Chen XM, Yue W, Liu L, et al. Beneficial and side effects of arginine vasopressin and terlipressin for septic shock. J Surg Res. 2015;195(2):568–79.
Morelli A, Rocco M, Conti G, Orecchioni A, De Gaetano A, Cortese G, et al. Effects of terlipressin on systemic and regional haemodynamics in catecholamine-treated hyperkinetic septic shock. Intensive Care Med. 2004;30(4):597–604.
Richard C. Stress-related cardiomyopathies. Ann Intensive Care. 2011;1(1):39.
Landesberg G, Gilon D, Meroz Y, Georgieva M, Levin PD, Goodman S, et al. Diastolic dysfunction and mortality in severe sepsis and septic shock. Eur Heart J. 2012;33(7):895–903.
Holmes CL, Patel BM, Russell JA, Walley KR. Physiology of vasopressin relevant to management of septic shock. Chest. 2001;120(3):989–1002.
Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, et al. Surviving Sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36(1):296–327.
Ryckwaert F, Virsolvy A, Fort A, Murat B, Richard S, Guillon G, et al. Terlipressin, a provasopressin drug exhibits direct vasoconstrictor properties: consequences on heart perfusion and performance. Crit Care Med. 2009;37(3):876–81.
Morelli A, Ertmer C, Westphal M. “Terlipressin in the treatment of septic shock: the earlier the better”? Best Pract Res Clin Anaesthesiol. 2008;22(2):317–21.
Rehberg S, Ertmer C, Kohler G, Spiegel HU, Morelli A, Lange M, et al. Role of arginine vasopressin and terlipressin as first-line vasopressor agents in fulminant ovine septic shock. Intensive Care Med. 2009;35(7):1286–96.
Morelli A, Ertmer C, Pietropaoli P, Westphal M. Terlipressin: a promising vasoactive agent in hemodynamic support of septic shock. Expert Opin Pharmacother. 2009;10(15):2569–75.
Acknowledgements
Not applicable.
Funding
This work is partially supported by grants from the National Natural Science Foundation of China (grant number: 81571847), the project of Jiangsu Province’s medical key discipline (ZDXKA2016025), and the Key Research and Development Plan of Jiangsu Province (BE2018743).
Author information
Authors and Affiliations
Contributions
Drs. LH and HQ had full access to all the data in the study and take responsibility for their integrity and the accuracy of the data analysis. Drs. LH, SL, and HQ performed the systematic review, study selection, statistical analysis, and preparation of the article for publication. Drs. YY, WC, SZ and FX contributed to the data extraction and quality assessment. All authors participated in writing the article and preparing the figures. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1 Figure S1.
Forest plot of the effect of terlipressin compared with catecholamine on the length of ICU stay in patients with septic shock as determined by a meta-analysis.
Additional file 2 Figure S2.
Forest plot of the effect of terlipressin compared with catecholamine on the haemodynamic variation in patients with septic shock as determined by a meta-analysis.
Additional file 3 Figure S3.
Forest plot of the effect of terlipressin compared with catecholamine on tissue perfusion in patients with septic shock as determined by a meta-analysis.
Additional file 4 Figure S4.
Forest plot of the effect of terlipressin compared with catecholamine on renal function in patients with septic shock as determined by a meta-analysis.
Additional file 5 Figure S5.
Forest plot of the adverse events of terlipressin compared with catecholamine in patients with septic shock as determined by a meta-analysis.
Additional file 6 Table S1.
Head-to-Head Comparisons of the RRs from the Network Analysis.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Huang, L., Zhang, S., Chang, W. et al. Terlipressin for the treatment of septic shock in adults: a systematic review and meta-analysis. BMC Anesthesiol 20, 58 (2020). https://doi.org/10.1186/s12871-020-00965-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-020-00965-4