
Abstract
Aim
Our aim was to evaluate the literature investigating proprioception improvement after anterior cruciate ligament reconstruction (ACLR) and test the hypothesis that ACL tibial remnant-preserving reconstruction (ACLR-R) is more beneficial than standard technique (ACLR-S) in terms of postoperative proprioceptive function with various reported tests, including joint position sense (JPS) and threshold to detect passive motion (TTDPM).
Methods
An online search was performed in Embase, MEDLINE/PubMed, Cochrane, SPORTDiscus, and Web of Science databases before 5 October 2020, on the basis of the guidelines of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement. Key terms [(‘ACLR’ or ‘ACL-R’ or ‘anterior cruciate ligament reconstruction’) AND (‘remnant’ or ‘stump’) AND (‘proprioception’ or ‘proprioceptive’)] were used. The Oxford Centre for Evidence-Based Medicine and The McMaster Critical Review Form for Quantitative Studies were used for quality assessment. In total, four articles comparing proprioceptive functions between ACLR-R and ACLR-S were included, two of which were randomized clinical trials rated as level of evidence II, and two were retrospective cohort studies rated as level of evidence III. The outcomes were then compared. Evaluation of proprioception involved joint position sense (JPS) [reproduction of active positioning (RAP) and reproduction of passive positioning (RPP)] and threshold to detect passive motion (TTDPM) tests.
Results
Only four studies were included, with a total of 234 patients (119 ACLR-R patients and 115 ACLR-S patients). High heterogeneity in characteristics and outcome measurements was observed among the studies. Three studies performed sparing technique, and one performed tensioning technique. One study tested RAP and reported better results at an average of 7 months follow-up in ACLR-R (P < 0.05). Three studies tested RPP, one of which measured RPP within 12 months after surgery and reported better results in ACLR-R than in ACLR-S (P < 0.05). The other two studies reported similar results; however, the findings of one study were statistically insignificant. TTDPM was tested in one study, with no statistically significant difference found.
Conclusion
The current literature, although limited, reported proprioception improvement after ACLR-R (compared with ACLR-S) in terms of JPS. However, owing to the heterogeneity of the relevant studies, further research is required to determine remnant preservation effect on knee proprioceptive restoration.
Level of evidence
Level III, systematic review of Level II and III studies.
Similar content being viewed by others
Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Proprioception, a sensory modality responsible for the sensation of joint movement and position, plays a crucial role in the afferent–efferent neuromuscular control arc and normal joint performance [26, 32, 41, 42].
Proprioceptors, including Ruffini endings, Pacinian corpuscles, and Golgi tendon organs, are located at the tibial bone insertion area of the anterior cruciate ligament (ACL) [1, 9].
Therefore, ACL injury can cause damage and loss of proprioceptive receptors (based on the time between injury and surgery [14]) and can translate into a decrease in afferent information input [15, 16], leading to mechanical instability [22, 41]. Such decreased proprioception can adversely affect the dynamic stability of the knee, strength, and balance and can increase the risk of secondary ACL injury by 30–40 times [6, 18, 49].
In addition to the role of proprioceptive rehabilitation programs [32, 36], remnant-preserving ACL reconstruction (ACLR) is potentially beneficial for proprioception restoration, based on histological findings of the presence of proprioceptors in injured ACL 3 years after injury [17]. Owing to the majority of ACL tears occurring at the femoral insertion, the tibial attachment remains relatively intact in the anatomic position [21]. Studies suggest a potential benefit of preserving the tibial remnant during ACLR in the retention of proprioceptors [21, 25]. However, the advantage of remnant preservation is shown mainly in basic histological studies rather than in clinical studies [25].
Various studies have reported that ACL remnant preservation facilitates recovery of stability, enhances tissue healing, and even decreases graft rupture after surgery [4, 12, 24, 38, 46]. However, the relationship between functional stability and proprioception was overlooked in such investigations [18]. The presence of proprioceptors in the ACL remnant [17] informs surgeons to consider remnant-preserving ACLR for better knee joint proprioceptive recovery, which raises the question of whether histological findings and benefits could be translated into clinical proprioceptive improvements.
Therefore, the purpose of this review was to evaluate the current literature and research work focusing on proprioception improvement after ACLR. In addition, since most reviews focused on clinical aspects of improvement rather than proprioception, we also aimed to determine whether ACL tibial remnant-preserving reconstruction (ACLR-R) is more beneficial than standard technique (ACLR-S) in terms of postoperative proprioceptive function with various reported tests. We hypothesized that proprioception functions are better in the ACL remnant-preserving technique than in standard reconstruction techniques, regardless of the methods of proprioceptive measurement.
Methods
Search strategy
A literature search was performed on the basis of the guidelines of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement [43]. Online databases (Embase, MEDLINE/PubMed, Cochrane, SPORTDiscus, and Web of Science) were searched for all English-language studies before 5 October 2020. Two reviewers separately searched these databases using key terms [(‘ACLR’ or ‘ACL-R’ or ‘anterior cruciate ligament reconstruction’) AND (‘remnant’ or ‘stump’) AND (‘proprioception’ or ‘proprioceptive’)]. References of the screened articles were also retrieved for potential inclusion. The authors of the studies were contacted for further clarifications when necessary.
Inclusion and exclusion criteria
Participants
Human unilaterally surgical ACL-reconstructed participants without other knee ligament interventions or repair of ACL avulsion fractures were included in this study. We excluded studies on patients with systematic disorders (e.g., cardiac vascular or neurological disorders) and congenital deformities of the lower extremities as well as those on animals and cadavers.
Interventions and comparisons
ACLR with remnant preservation was considered as the experimental intervention in this systematic review. Double-bundle and single-bundle ACLRs with different sources of grafts were included. The control intervention was non-remnant standard ACLR. Studies comparing the various amounts of remnants but not with the debridement procedure were excluded, while studies comparing the remnants with debridement were included if separate evaluations of each group were available.
Outcome measurements
In total, the outcome measurements included: (1) proprioceptive evaluation involving joint position sense (JPS) [13] [reproduction of active positioning (RAP) and reproduction of passive positioning (RPP)] and threshold to detect passive motion (TTDPM) tests [8]; (2) balance or postural control tests; (3) objective knee stability examinations such as the anterior drawer test, Lachman test, KT-arthrometer measurement, and pivot-shift test; (4) patient-reported outcomes, including the International Knee Documentation Committee (IKDC) score, Tegner activity scale, Lysholm score, and Hospital for Special Surgery (HSS) score.
Study type
In this study, we included all published English-language randomized controlled trials, prospective cohort studies without randomization, and retrospective cohort studies or case series with historical controls (evidence levels I, II, III, IV) that reported the proprioceptive outcomes of ACLR-R versus ACLR-S [51]. No minimum follow-up period was employed. Case series without controls, case reports, and expert opinions (level IV or V) [51] as well as studies solely depicting functional outcomes without further proprioceptive outcomes, meeting abstracts, trial protocols, and systematic reviews were excluded.
Data extraction
After the removal of duplicates, two independent reviewers screened the titles and abstracts of the studies for potential eligibility. Studies were further analyzed in full text if the abstract did not provide enough data to make a decision. A senior author was consulted when there were disagreements between the reviewers.
Data included: (1) general information (first author, publication year, country where study was performed, sample size, mean age, sex, mean time from injury to surgery, mean follow-up time, injury side, level of evidence, and study design); (2) ACLR surgical characteristics (ACL tear pattern, associated injury, remnant volume, number of bundles, graft diameter and type, surgical technique, tibial remnant management, complications, and rehabilitation); and (3) outcome measurements (proprioception assessment, balance or postural control tests, knee laxity and function, and patient-reported outcomes).
Studies that used ACL augmentation with selective ACL anteromedial or posterolateral bundle reconstruction were excluded from the review.
Quality assessment
To evaluate the methodological quality of the evidence, a critical appraisal of all included studies was performed. The level of evidence was assessed according to the Oxford Centre for Evidence-Based Medicine [51]. The McMaster Critical Review Form for Quantitative Studies [27] was used to rate the methodological quality by evaluating the risk of bias within studies. This form consists of nine categories: citation, study purpose, literature, design, sample, outcomes, intervention, results, and conclusions and implications. Responses are marked as yes (1 point), no or not addressed (0 point), or not applicable (item does not count). The sum of the outcomes (0–15 points) divided by the sum of the applicable items represents the overall quality of the study assessed.
The independent reviewers examined the studies, and any discrepancy was resolved through discussions with the senior author. Kappa values were also calculated to assess the inter-rater agreement of each individual item.
Data analysis
The results of the review are presented as a synthesis with the extracted data descriptively reported as medians (minimum–maximum) and means (standard deviation and/or minimum–maximum) for continuous variables and percentages for categorical data. Completing a meta-analysis or quantitative analysis was not feasible owing to several reasons, including the heterogeneity of ACL tear patterns (partial or complete or not reported), ACL remnant and graft statuses, remnant management techniques (remnant tensioning or sparing), application of different proprioceptive evaluation methods, and testing conditions in included studies. All basic data and clinical results were qualitatively compared and summarized in this review.
Results
Search results
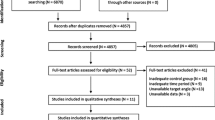
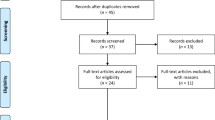
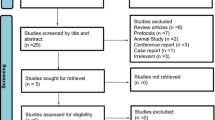
A total of 336 studies were selected after reviewing the literature: 56 from Embase, 47 from MEDLINE/PubMed, 11 trials from the Cochrane library, 131 from SPORTDiscus, and 91 from Web of Science. After the first screening (duplication removal, eligibility criteria, and title-based exclusion), 250 studies were selected. Of these, 226 studies were excluded on the basis of the abstracts and exclusion criteria, and subsequently, 20 studies were excluded after full-text review. Finally, four studies [5, 11, 19, 28] were identified for qualitative synthesis (Fig. 1). In total, 234 participants (154 males, 80 females) were included in the four selected studies, with 119 participants who underwent ACLR-R and 115 participants who underwent ACLR-S.

A flow diagram showing the PRISMA study selection of publications. ACLR-R, anterior cruciate ligament tibial remnant-preserving reconstruction; ACLR-S, anterior cruciate ligament standard reconstruction
Critical appraisal in included studies
Of the four studies, two [5, 19] were randomized clinical trials rated as level of evidence II, while the remaining studies [11, 28] were retrospective cohort studies rated as level of evidence III (Table 1). None of the studies met all the McMaster critical appraisal criteria. Only one study justified the sample size with a power calculation [19]. Unbiased group assignment was conducted in only two studies [5, 19]. Cointervention bias was adequately addressed in all included studies, and the selected studies also provided information about the inclusion criteria and rehabilitation protocol [5, 11, 19, 28] (Table 2).
Surgical characteristics
ACL injury and remnant and graft status
ACL remnant characteristics were described in all four studies [5, 11, 19, 28]. Only one of the studies reported the minimum remnant length to be quantitatively more than 20% of the native ACL [28]. Two of the studies reported a remnant diameter of over one-third [5] or half [19] of the original ACL diameter. Single-bundle ACLR was performed in all included studies [5, 11, 19, 28]. Two studies [5, 28] used an autologous hamstring graft, and the other studies [11, 19] used an allograft for reconstruction. The graft diameter ranged from 7 to 9 mm [11, 19, 28]. Only one study [5] did not describe the specific graft diameter (Table 3).
Surgical techniques and remnant management
The hypothesis of this study was that ACL tibial remnant-preserving reconstruction (ACLR-R) is more beneficial than standard technique (ACLR-S) in terms of postoperative proprioceptive function with various reported tests, including joint position sense (JPS) and threshold to detect passive motion (TTDPM). Therefore, the remnant preservation and resection referred solely to the tibial side rather than both the femoral and tibial sides. The femoral tunnel placement method was reported in all studies [5, 11, 19, 28]. The tunnels were created via the anteromedial (AM) or accessory anteromedial (AAM) portal in three studies [5, 11, 19], and via the outside-in technique [3] in one study [28]. Furthermore, the tibial tunnel was positioned in the center of the ACL remnant footprint [11, 19, 28] in both ACLR-R and ACLR-S, except in one study [5], which positioned the tip of the tibial tunnel guide anteromedial or posterolateral to the ACL posterolateral or anteromedial residual bundle for ACLR-R to prevent damage of the residual bundle. The tibial remnant was removed in all ACLR-S patients. In ACLR-R, three of four studies [5, 11, 28] performed the sparing technique described by Lee et al. [30], while only one study [19] used the tensioning technique described by Ahn et al.[2] (Table 3).
Complication
Only two studies described complications after ACLR [11, 19]. Hong et al. [19] reported cyclops lesion formation (n = 3/55) during second-look arthroscopic evaluation and subsequently resected it. Chen et al. [11] found no complications such as bone tunnel enlargement, impingement, or cyclops lesion. No significant difference was reported between the ACLR-R and ACLR-S groups (Table 3).
Rehabilitation
Three studies [11, 19, 28] reported weight-bearing rehabilitation after ACLR. Partial weight-bearing and full weight-bearing exercises started at least 2 weeks and 6 weeks after reconstruction, respectively (Table 3). Rehabilitation protocols were identical for treatments and controls in all studies that provided such details.
Outcomes
Proprioception assessment
JPS test-RPP
Three of four studies [11, 19, 28] measured RPP at different follow-up times. Chen et al. [11] analyzed RPP test results at 3, 6, and 12 months after surgery and found that the ACLR-R group had significantly better RPP results than ACLR-S in all testing conditions (knee flexion of 15°, 30°, and 45°; P < 0.05). Two studies [19, 28] followed up on participants for more than 24 months (24–36 months). One of the two studies that used the sparing technique reported a statistically significant difference in RPP test, indicating better proprioception in ACLR-S (knee flexion of 15° and 30°; P = 0.40 and P = 0.010). The other study [19] analyzed RPP test results at 3, 6, 9, 12, 18, and 24 months, but presented statistically insignificant findings (P = 0.739) (Table 4). Interestingly, both studies reporting JPS-RPP improvement were observational studies, while the one study reporting no significant difference was a clinical trial.
JPS test—RAP
Only one study [5] tested RAP before and after surgery with a mean follow-up duration of 7 months. The test results showed greater improvement of proprioception in ACLR-R compared with that in ACLR-S (P < 0.05) (Table 4).
JPS test—recording and testing
Three studies [11, 19, 28] recorded and compared the mean JPS value (test angle minus setting angle) of the reconstructed knees, while one study [5] recorded the inaccuracy of both legs (involved and contralateral normal knees) and reported side-to-side differences in the JPS value. Two studies used the Biodex system to measure JPS [5, 19], one study [28] used Thomas splint and Pearson attachment, while the remaining study [11] did not report on the testing apparatus. Only one study [19] described the test speed (with a speed of 5°/s) (Table 4).
TTDPM test
One study [28] measured TTDPM by continuous passive motion at final follow-up. Patients were tested at three angles of knee flexion with a speed of 0.5°/s. There was no statistically significant difference between ACLR-S and ACLR-R; however, the ACLR-R group showed better results at all angles (Table 5).
Balance tests, knee stability, and patient-reported outcomes
Only one study [28] reported on balance or postural tests. They conducted the one-leg hop test and single-limb standing test and found a statistically significant difference between the two groups (P < 0.05). Regarding knee stability and patient-reported outcomes, only one study [5] reported significantly greater improvement in anterior laxity tested by Rolimeter after ACLR-R compared with ACLR-S (P < 0.0001). None of the remaining studies found a significant difference (Table 4).
Discussion
The most important observation of this review was that patients with ACLR-R showed improved postoperative proprioceptive evaluation results compared with those of the non-remnant ACLR-S. However, the long-term improvement of proprioception in ACLR-R remains unclear since the majority of studies failed to report long-term (> 16 months) follow-up results. Additionally, the heterogeneity of the characteristics and proprioceptive assessment of the studies prevented us from statistically evaluating the clinical outcomes.
Currently, there have been several meta-analyses or systematic reviews debating whether ACL tibial remnants should be saved during surgery [20, 25, 33, 34, 47, 48, 50]. Such reviews reported equivalent or superior postoperative clinical outcomes with ACLR-R compared with ACLR-S; however, there is insufficient scientific evidence supporting a definite conclusion. Moreover, these reviews [20, 25, 33, 34, 47, 48, 50] mainly concentrated on graft healing, synovial coverage, revascularization and ligamentization, knee stability function, and patient-reported outcomes, with a limited focus on proprioception or proprioceptive assessment. Therefore, our current review aimed to fill that gap by focusing on proprioception improvement.
Histological animal studies proved that ACL remnant preservation promoted new ingrowth of proprioceptors, neural cells, and nerve-related gene expression 6–12 weeks after surgery [23, 31, 45, 52], indicating the enhancement of proprioception of the knee joints in the early stage. The histological findings partially explained the results of our review, which reported a greater proprioceptive improvement in ACLR-R (compared with ACLR-S) in the short follow-up (≤ 12 months) period. Although there were a few findings of studies with longer follow-up that reported similar results, they lacked statistical significance [19, 28]. Histological studies in humans showed a reduction in the concentration of neural analogs in ACL grafts years after ACLR, regardless of graft source (allograft or autograft) [53]. Moreover, the effect of graft source on proprioceptive recovery has been unclear in several studies [7, 10, 39, 40] that have reported similar outcomes from ACLR with autograft, allograft, and artificial synthesis grafts. These results jointly indicate the potential benefits of remnant-sparing ACLR over the tensioning technique, and further comparisons of two techniques with different follow-up durations and graft sources in proprioception assessment and clinical outcomes are required in future studies.
Several human studies have evaluated the remnant-preserving effect after surgery with respect to remnant volume and surgical timing [29, 35, 44, 47]. However, the optimal volume and timing (time between the injury and the surgical procedure) for remnant-preserving ACLR in clinical practice require further investigation since only few studies reported the results of proprioceptive assessment. Only one study [19] (of those included in this review) described the mean time from injury to surgery. The varied descriptions of remnant volume in three included studies [5, 19, 28] also prevented us from performing subgroup analysis of the relationship between the remnant amount and proprioceptive restoration. Therefore, the effect of remnant volume and surgical timing during ACLR-R on proprioceptive recovery should be further studied.
Proprioception in this current review was mainly assessed with JPS (position sense) and TTDPM (movement sense). JPS is relatively easy to perform [37]. All studies included in the review reported on JPS [5, 11, 19], while only one study reported on TTDPM [28]. However, the two tests are commonly used for proprioception assessment, and both should be interpreted cautiously owing to the complexity of proprioception [37]. Furthermore, proprioceptors in the ACL and surrounding capsules and muscles [28] cannot be differentiated by any existing tests during assessment; thus, although JPS and TTDPM provided valuable information about joint position and movement sense, new tests are still needed for further investigation.
Limitations
This study has few limitations. First, only four studies (level of evidence II or III) were finally extracted and analyzed in the review, and heterogeneity in study characteristics and outcome measures was encountered. Thus, the results were qualitatively summarized. Therefore, high-quality studies with validated outcomes are required in the future. Second, studies that used ACL augmentation with selective ACL anteromedial or posterolateral bundle reconstruction were excluded from the review to reduce the risk of bias between ACL reconstruction and augmentation. Further studies with respect to the different remnant-preserving ACLR techniques are needed for further investigation. Third, publication bias might have existed because only online-published English-language articles were included.
Conclusion
The potential and benefits of remnant-preserving ACLR are apparent since improved results were observed in postoperative proprioceptive evaluation compared with the non-remnant standard ACLR.
More high-quality studies with validated tests are required to distinguish the effect of remnant preservation on knee proprioceptive restoration owing to the heterogeneity of existing studies.
Availability of data and materials
Not applicable.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- ACLR:
-
Anterior cruciate ligament reconstruction
- ACLR-R:
-
Anterior cruciate ligament tibial remnant-preserving reconstruction
- ACLR-S:
-
Standard technique
- AM:
-
Anteromedial
- AAM:
-
Accessory anteromedial
- HSS:
-
Hospital for Special Surgery
- IKDC:
-
International Knee Documentation Committee
- JPS:
-
Joint position sense
- RAP:
-
Reproduction of active positioning
- RPP:
-
Reproduction of passive positioning
- TTDPM:
-
Threshold to detect passive motion
References
Adachi N, Ochi M, Uchio Y, Iwasa J, Ryoke K, Kuriwaka M (2002) Mechanoreceptors in the anterior cruciate ligament contribute to the joint position sense. Acta Orthop Scand 73:330–334
Ahn JH, Lee YS, Ha HC (2009) Anterior cruciate ligament reconstruction with preservation of remnant bundle using hamstring autograft: technical note. Arch Orthop Trauma Surg 129:1011–1015
Ahn JH, Lee YS, Lee SH (2014) Creation of an anatomic femoral tunnel with minimal damage to the remnant bundle in remnant-preserving anterior cruciate ligament reconstruction using an outside-in technique. Arthrosc Tech 3:e175-179
Ahn JH, Wang JH, Lee YS, Kim JG, Kang JH, Koh KH (2011) Anterior cruciate ligament reconstruction using remnant preservation and a femoral tensioning technique: clinical and magnetic resonance imaging results. Arthroscopy 27:1079–1089
Andonovski A, Topuzovska S, Samardziski M, Bozinovski Z, Andonovska B, Temelkovski Z (2017) The influence of anterior cruciate ligament remnant on postoperative clinical results in patients with remnant preserving anterior cruciate ligament reconstruction. Open Access Maced J Med Sci 5:624–629
Arumugam A, Strong A, Tengman E, Roijezon U, Hager CK (2019) Psychometric properties of knee proprioception tests targeting healthy individuals and those with anterior cruciate ligament injury managed with or without reconstruction: a systematic review protocol. BMJ Open 9:e027241
Biz C, Cigolotti A, Zonta F, Belluzzi E, Ruggieri P (2019) ACL reconstruction using a bone patellar tendon bone (BPTB) allograft or a hamstring tendon autograft (GST): a single-center comparative study. Acta Biomed 90:109–117
Boerboom AL, Huizinga MR, Kaan WA, Stewart RE, Hof AL, Bulstra SK, Diercks RL (2008) Validation of a method to measure the proprioception of the knee. Gait Posture 28(4):610–614. https://doi.org/10.1016/j.gaitpost.2008.04.007 (Epub 2008 Jun 2)
Çabuk H, Kuşku Çabuk F (2016) Mechanoreceptors of the ligaments and tendons around the knee. Clin Anat 29:789–795
Chen T, Zhang P, Chen J, Hua Y, Chen S (2017) Long-term outcomes of anterior cruciate ligament reconstruction using either synthetics with remnant preservation or hamstring autografts: a 10-year longitudinal study. Am J Sports Med 45:2739–2750
Chen TZ, Wang YS, Li XS (2019) Anterior cruciate ligament reconstruction using an anterior cruciate ligament stump. Wideochir Inne Tech Maloinwazyjne 14:461–467
Choi S, Kim MK, Kwon YS, Kang H (2017) Clinical and arthroscopic outcome of single bundle anterior cruciate ligament reconstruction: comparison of remnant preservation versus conventional technique. Knee 24:1025–1032
Corrigan JP, Cashman WF, Brady MP (1992) Proprioception in the cruciate deficient knee. J Bone Joint Surg Br 74(2):247–250. https://doi.org/10.1302/0301-620X.74B2.1544962
Denti M, Monteleone M, Berardi A, Panni AS (1994) Anterior cruciate ligament mechanoreceptors. Histologic studies on lesions and reconstruction. Clin Orthop Relat Res 308:29–32
Dhillon MS, Bali K, Prabhakar S (2012) Differences among mechanoreceptors in healthy and injured anterior cruciate ligaments and their clinical importance. Muscles Ligaments Tendons J 2:38–43
Gao F, Zhou J, He C, Ding J, Lou Z, Xie Q et al (2016) A morphologic and quantitative study of mechanoreceptors in the remnant stump of the human anterior cruciate ligament. Arthroscopy 32:273–280
Georgoulis AD, Pappa L, Moebius U, Malamou-Mitsi V, Pappa S, Papageorgiou CO et al (2001) The presence of proprioceptive mechanoreceptors in the remnants of the ruptured ACL as a possible source of re-innervation of the ACL autograft. Knee Surg Sports Traumatol Arthrosc 9:364–368
Gokeler A, Benjaminse A, Hewett TE, Lephart SM, Engebretsen L, Ageberg E et al (2012) Proprioceptive deficits after ACL injury: are they clinically relevant? Br J Sports Med 46:180–192
Hong L, Li X, Zhang H, Liu X, Zhang J, Shen JW et al (2012) Anterior cruciate ligament reconstruction with remnant preservation: a prospective, randomized controlled study. Am J Sports Med 40:2747–2755
Hu J, Qu J, Xu D, Zhang T, Zhou J, Lu H (2014) Clinical outcomes of remnant preserving augmentation in anterior cruciate ligament reconstruction: a systematic review. Knee Surg Sports Traumatol Arthrosc 22:1976–1985
Junkin DM Jr, Johnson DL (2008) ACL tibial remnant, to save or not? Orthopedics 31:154–159
Kim HJ, Lee JH, Lee DH (2017) Proprioception in patients with anterior cruciate ligament tears: a meta-analysis comparing injured and uninjured limbs. Am J Sports Med 45:2916–2922
Kim SH, Chun CH, Chun KC, Jo HJ, Kim KM (2012) Histological assessment of mechanoreceptors in Achilles allografts after anterior cruciate ligament reconstruction. Am J Sports Med 40:2061–2065
Kondo E, Yasuda K, Onodera J, Kawaguchi Y, Kitamura N (2015) Effects of remnant tissue preservation on clinical and arthroscopic results after anatomic double-bundle anterior cruciate ligament reconstruction. Am J Sports Med 43:1882–1892
Kosy JD, Mandalia VI (2018) Anterior cruciate ligament mechanoreceptors and their potential importance in remnant-preserving reconstruction: a review of basic science and clinical findings. J Knee Surg 31:736–746
Laskowski ER, Newcomer-Aney K, Smith J (2000) Proprioception. Phys Med Rehabil Clin N Am 11(323–340):vi
Law M, Stewart D, Pollock N, Letts L, Bosch J, Westmorland M (1998) Critical review form for quantitative studies. https://srs-mcmaster.ca/wp-content/uploads/2015/04/Critical-Review-Form-Quantitative-Studies-English.pdf. Published
Lee BI, Kim CH, Jang BW, Hong YC, Kwon SW (2020) Preservation of the tibial remnant in anterior cruciate ligament reconstruction may improve postoperative proprioceptive function. Orthopedics 43:e231–e236
Lee BI, Kwon SW, Kim JB, Choi HS, Min KD (2008) Comparison of clinical results according to amount of preserved remnant in arthroscopic anterior cruciate ligament reconstruction using quadrupled hamstring graft. Arthroscopy 24:560–568
Lee BI, Min KD, Choi HS, Kim JB, Kim ST (2006) Arthroscopic anterior cruciate ligament reconstruction with the tibial-remnant preserving technique using a hamstring graft. Arthroscopy 22:340.e341-340.e347
Lee SH, Cho HG, Song JS, Chun KC, Chun CH (2020) Quantitative assessment of neural elements in a rat model using nerve growth factor after remnant-preserving anterior cruciate ligament reconstruction: a histological and immunofluorescence pilot study. J Orthop Surg Res 15:277
Lephart SM, Pincivero DM, Giraldo JL, Fu FH (1997) The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med 25:130–137
Ma T, Zeng C, Pan J, Zhao C, Fang H, Cai D (2017) Remnant preservation in anterior cruciate ligament reconstruction versus standard techniques: a meta-analysis of randomized controlled trials. J Sports Med Phys Fitness 57:1014–1022
Muneta T, Koga H (2017) Anterior cruciate ligament remnant and its values for preservation. Asia Pac J Sports Med Arthrosc Rehabil Technol 7:1–9
Muneta T, Koga H, Ju YJ, Horie M, Nakamura T, Sekiya I (2013) Remnant volume of anterior cruciate ligament correlates preoperative patients’ status and postoperative outcome. Knee Surg Sports Traumatol Arthrosc 21:906–913
Musahl V, Karlsson J (2019) Anterior cruciate ligament tear. N Engl J Med 380:2341–2348
Nagai T, Schilaty ND, Strauss JD, Crowley EM, Hewett TE (2018) Analysis of lower extremity proprioception for anterior cruciate ligament injury prevention: current opinion. Sports Med 48:1303–1309
Nakayama H, Kambara S, Iseki T, Kanto R, Kurosaka K, Yoshiya S (2017) Double-bundle anterior cruciate ligament reconstruction with and without remnant preservation—comparison of early postoperative outcomes and complications. Knee 24:1039–1046
Ozenci AM, Inanmaz E, Ozcanli H, Soyuncu Y, Samanci N, Dagseven T et al (2007) Proprioceptive comparison of allograft and autograft anterior cruciate ligament reconstructions. Knee Surg Sports Traumatol Arthrosc 15:1432–1437
Płocki J, Pelikan P, Bejer A, Granek A, Krawczyk-Suszek M, Kotela I (2019) Comparison of results of ACL reconstruction using LARS method and autogenous ST/GR graft. Acta Bioeng Biomech 21:113–119
Relph N, Herrington L, Tyson S (2014) The effects of ACL injury on knee proprioception: a meta-analysis. Physiotherapy 100:187–195
Riemann BL, Lephart SM (2002) The sensorimotor system, part II: the role of proprioception in motor control and functional joint stability. J Athl Train 37:80–84
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 350:g7647
Smith TO, Davies L, Hing CB (2010) Early versus delayed surgery for anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 18:304–311
Takahashi T, Kondo E, Yasuda K, Miyatake S, Kawaguchi Y, Onodera J et al (2016) Effects of remnant tissue preservation on the tendon graft in anterior cruciate ligament reconstruction: a biomechanical and histological study. Am J Sports Med 44:1708–1716
Takazawa Y, Ikeda H, Kawasaki T, Ishijima M, Kubota M, Saita Y et al (2013) ACL reconstruction preserving the ACL remnant achieves good clinical outcomes and can reduce subsequent graft rupture. Orthop J Sports Med 1:2325967113505076
Wang H, Liu Z, Li Y, Peng Y, Xu W, Hu N et al (2019) Is remnant preservation in anterior cruciate ligament reconstruction superior to the standard technique? A systematic review and meta-analysis. Biomed Res Int 2019:1652901
Wang HD, Wang FS, Gao SJ, Zhang YZ (2018) Remnant preservation technique versus standard technique for anterior cruciate ligament reconstruction: a meta-analysis of randomized controlled trials. J Orthop Surg Res 13:231
Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD (2016) Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med 44:1861–1876
Won SH, Lee BI, Park SY, Min KD, Kim JB, Kwon SW et al (2020) Outcome differences of remnant—preserving versus non-preserving methods in arthroscopic anterior cruciate ligament reconstruction: a meta-analysis with subgroup analysis. Knee Surg Relat Res 32:7
Wright J, Swiontkowski M, Heckman J (2003) Introducing levels of evidence to the journal. J Bone Joint Surg Am 85:1–3
Xie GM, Huang Fu XQ, Zhao JZ (2012) The effect of remnant preservation on patterns of gene expression in a rabbit model of anterior cruciate ligament reconstruction. J Surg Res 176:510–516
Young SW, Valladares RD, Loi F, Dragoo JL (2016) Mechanoreceptor reinnervation of autografts versus allografts after anterior cruciate ligament reconstruction. Orthop J Sports Med 4:2325967116668782
Acknowledgements
None.
Funding
Funded by: (1) National Key Research and Development Program of China, grant nos. 2018YFC1106200 and 2018YFC1106202; (2) The Western Medicine Guidance Project of Science and Technology Commission of Shanghai Municipality, grant no. 17411966400.
Author information
Authors and Affiliations
Contributions
EC contributed to the search, review, and completion of this systemic review. JC contributed to the search, review, and completion of this systemic review. CX contributed to the review, and completion of this systemic review. JZ contributed to the completion and supervision of this systemic review. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of Shanghai Sixth People’s Hospital.
Consent for publication
Not applicable.
Competing interests
All authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cho, E., Chen, J., Xu, C. et al. Remnant preservation may improve proprioception after anterior cruciate ligament reconstruction. J Orthop Traumatol 23, 22 (2022). https://doi.org/10.1186/s10195-022-00641-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10195-022-00641-y