
Abstract
Purpose
The objective of this systematic literature review was to report the results and complications of recent remnant preservation techniques in posterior cruciate ligament (PCL) reconstruction.
Methods
A systematic review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Two independent reviewers searched the PubMed, Scopus, Embase, and Cochrane Library databases using the terms “posterior cruciate ligament” or “PCL” and “remnant preserving.” The outcome measures extracted from the studies were the Lysholm score, the International Knee Documentation Committee’s (IKDC) subjective and objective scores, Tegner scores, Orthopädische Arbeitsgruppe Knie (OAK) rate of return to sports, and rate of complications. Data were also extracted from studies that used stress radiographs to perform a quantitative assessment of the preoperative and postoperative anteroposterior stability.
Results
The systematic review included 13 studies. The patient cohort of consisted of 643 participants (544 [84.6%] men and 99 [15.4%] women) with a mean age of 32.9 ± 4.0 years. The mean postoperative follow-up was 34.5 ± 10.9 months (range: 24–96 months), while the mean time from injury to surgery was 14.4 ± 9.9 months (range: 0–240 months). All studies reported clinically significant improvement at final follow-up, as evident from the measured subjective and objective IKDC scores, Lysholm score, Tegner score, and OAK rate. Only three studies reported return to sports activity, with a mean percentage of 90.8% (99/109). All studies showed a significant improvement in posterior translation, from 11.5 ± 1.2 mm to 3.3 ± 1.1 mm, using radiography (side-to-side difference). This systematic review revealed 13 (2.0%) failures and 33 (5.1%) minor complications: 10 (1.6%) cases of stiffness, 21 (4.9%) screws removal, 1 (0.2%) injury of the peroneal nerve, and 1 (0.2%) fibular fracture.
Conclusions
With the currently available data, all studies included in the review on posterior cruciate ligament reconstruction with remnant preservation demonstrated satisfactory outcomes at mid-term follow-up (> 24 months), despite varying surgical techniques and graft types, and intervals from injury to surgery. For clinical relevance, standard PCL reconstruction is a highly effective operation in terms of improvement in functional status, knee stability, quality of life, and cost effectiveness. The remnant preservation technique requires more comprehensive diagnostic assessments of the PCL remnant patterns and more complicated surgical procedures. Given the absence so far of high quality studies with long-term follow-up, the remnant-preserving techniques should be recommended only by experienced knee arthroscopic surgeons.
Level of evidence
Level IV.
Study registration
reviewregistry1376—www.researchregistry.com.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Introduction
Isolated lesions of the posterior cruciate ligament (PCL) are rare and are linked in most cases to a traffic or sporting accident [18, 35], and they represent only 1% of traumatised knee lesions [21, 26]. PCL is known for its ability to heal properly, and both conservative and surgical treatment provide good functional results for minimal to moderate instability [8, 29]. Nevertheless, long-term studies have shown an increase in the incidence of osteoarthritic lesions and a deterioration in the function of the traumatised knee if treated non-surgically, thus rendering reconstruction of the posterior cruciate ligament more acceptable, given the evolution of surgical techniques [6, 7].
In conventional PCL reconstruction techniques, the remaining fibres of the PCL are generally resected to obtain a good visualisation of the PCL insertion zone and facilitate the passage of the graft [30, 31]. More recently, several researchers have introduced the concept of preservation of the remaining fibres of the PCL; however, the advantages of such preservation are less clear. To our knowledge, there is no recent systematic review on the subject which discusses the interest in performing this technique of preserving PCL fibres. Therefore, the objective of this systematic literature review was to report the results and complications of recent remnant preservation techniques in PCL reconstruction.
It was hypothesised that isolated PCL reconstruction with remnant preservation surgery could provide encouraging clinical outcomes and good recovery of the proprioceptive function.
Materials and methods
The current systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and is registered in the Research Registry (reviewregistry1376 – www.researchregistry.com) [24, 28].
Eligibility criteria
The literature reviewed in this study was selected based on the following criteria.
Study design
This review included randomised controlled trials (RCTs) and controlled (non-randomised) clinical trials (CCTs), prospective and retrospective comparative cohort studies, case–control studies, and case series with more than 20 patients and two-year follow-up. Case reports and case series that did not report data on clinical and functional results were excluded.
Participants
Studies conducted on skeletally mature patients who underwent PCL reconstruction with the remnant-preserving technique and evaluation through a minimum of two years of follow-up were eligible for the review.
Interventions
Studies that reported data on clinical, functional, and radiological outcomes following PCL reconstruction with remnant preservation to treat knee laxity, isolated or associated with other knee ligamentous injuries, were considered eligible for the current study.
Types of outcome measures
The outcome measures extracted from the studies were the Lysholm score, the International Knee Documentation Committee’s (IKDC) subjective and objective scores, Tegner scores, the Orthopädische Arbeitsgruppe Knie (OAK) rate of return to sports, and the rate of complications. Data were also extracted from studies that used stress radiographs to perform a quantitative assessment of the preoperative and postoperative anteroposterior stability.
Information sources and search
A systematic search for relevant literature was performed on the PubMed (MEDLINE), Scopus, EMBASE, and Cochrane Library databases. The publication date was not considered an inclusion criterion. The search was carried out in May 2022. Two independent reviewers (RD and AH) assisted in conducting and validating the search. The following search terms were entered in the title, abstract, and keywords fields: “posterior cruciate ligament” or “PCL” and “remnant preserving.” Only papers published in English were included.
Data collection and analysis
Study selection
The retrieved articles were first screened according to their titles. If an article was found relevant, it was screened further by reading the abstract. After excluding studies that did not meet the eligibility criteria, the entire content of the remaining articles was evaluated for eligibility. To minimise the risk of bias, the authors reviewed and discussed all the selected articles and references, as well as the articles excluded from the study. In the event of any disagreement between the reviewers, the senior investigator made the final decision. At the end of the process, further studies that might have been missed were manually searched by going through the reference lists of the included studies and relevant systematic reviews.
Data collection process
The first two authors (RD and AH) collected the data from the selected articles using a computerised tool created with Microsoft Access (Version 2010; Microsoft Corp, Redmond, Washington). Every article was validated again by RD before analysis. For each study, the data collected included information regarding the patients (age, gender, duration between injury and surgery, and follow-up evaluation), their injuries (type, aetiology, and associated injuries), the surgery technique (type of graft used, number of bundles, fixation technique, number of femoral and tibial tunnels, and tensioning protocol), rehabilitation protocol, postoperative outcomes (Lysholm, IKDC, OAK, and Tegner scores, and radiographs), rate of complications, and the rate of return to sports. Rerupture has been defined as repeated PCL revision resulting from trauma [30, 31], graft rupture with persistent subjective instability [6, 7], catastrophic failure [6, 7], or reasons not reported because the revision procedure was performed elsewhere [20]. Scheduled repeated revision resulting from traumatic injury or graft rupture [4] was also considered.
Level of evidence
The Oxford Levels of Evidence set by the Oxford Centre for Evidence-Based Medicine were used to categorise the levels of evidence [25].
Evaluation of the quality of studies
The quality of the selected studies was evaluated using the Methodological Index for Nonrandomised Studies (MINORS) score [22]. The checklist includes12 items, of which the last four are specific to comparative studies. Each item was given a score of 0–2 points. The ideal score was 16 points for non-comparative studies and 24 for comparative studies.
Statistical analysis
The extracted quantitative parameters (age, follow-up time, and results of the PROMs) were given as mean ± standard deviation (SD), when provided in the articles. Otherwise, alternative values like median or range were extracted. Due to the high statistical and methodological heterogeneity of the included studies, a meta-analysis comparing the results between patients with and without concomitant surgeries was not possible. Instead, a narrative description and comparison of the clinical results was performed.
Results
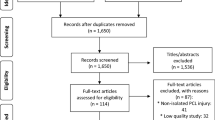
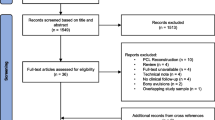
The electronic search yielded 125 studies. After removing 80 duplicates, 45 studies remained, of which 21 were excluded after reviewing the abstracts, thus bringing down the number of studies eligible for review to 24. An additional 11 articles were excluded based on the inclusion and exclusion criteria.
No additional studies were found upon manually checking the reference lists of the selected articles. Thus, 13 studies were included in the analysis [1, 5, 10, 11, 13,14,15,16,17, 19, 32,33,34]. Of the 13 included articles, one was level II [32], five were level III [1, 11, 17, 33, 34], and seven were level IV [5, 10, 13,14,15,16, 19].
Figure 1 is a flowchart depicting the process of selection of the studies. The studies analysed had a mean MINORS score of 13.8 (range: 9–21), which confirmed the acceptable methodological quality of the reviewed literature (Table 1).

A flowchart of the literature screening performed in this study
Patients’ and study characteristics
Table 1 shows the characteristics of the cohorts involved in the 13 selected studies, and a summary of their data. The patients cohort consisted of 643 participants (544 [84.6%] men and 99 [15.4%] women) with a mean age of 32.9 ± 4.0 years (range: 14–66). The mean postoperative follow-up was 34.5 ± 10.9 months (range: 24–96 months), while the mean time from injury to surgery was 14.4 ± 9.9 months (range: 0–240 months). Concomitant injuries involved 50 (7.8%) chondral injuries, 109 (17.0%) meniscus injuries, 24 (3.7%) medial collateral ligament (MCL) lesions, 113 (17.6%) posterolateral rotatory instability, and seven (1.1%) ACL tears (Fig. 2).

Coronal Magnetic Resonance of the knee showing the remnant of the posterior cruciate ligament (blue lines)
Surgical protocol
The data regarding the surgical technique followed in each of the examined studies are displayed in Table 2. The type of graft used in the various studies was as follows: six studies reported the use of Achilles allograft [1, 11, 13, 32,33,34], five studies autologous hamstrings [1, 5, 10, 16, 17], and three studies tibialis allografts (anterior or posterior) [14, 15, 19]. The femoral graft-fixation construct was performed in 10 studies with a screw [1, 5, 10, 11, 13, 16, 17, 32,33,34], and with the RigidFix System in three studies [14, 15, 17], while the Endobutton System was employed in one study only [19].
Furthermore, all studies reported conducting the tibial fixation with a screw (with or without adding a staple) [1, 5, 10, 11, 13,14,15,16,17, 32,33,34], except for one that used the Biointrafix System [19]. Additionally, all studies except one [32] performed a single-bundle reconstruction [1, 5, 10, 11, 13,14,15,16,17, 33, 34]. The tensioning of the PCL reconstruction was performed at 90° in seven studies [13, 15, 17, 19, 32,33,34], at a range from 70° to 90° in three studies [10, 16, 17], and at 70° and 60° in one study [5, 11]. The use of a postoperative brace was suggested in all studies [1, 10, 11, 13,14,15,16,17, 19, 32,33,34] except one [5]. Moreover, weight-bearing was allowed from day zero in six studies [5, 10, 11, 14,15,16], while it was allowed from 3–7 weeks post operation in other studies [13, 17, 19, 32,33,34].
Preservation technique
Six studies reported the use of the transtibial technique [10, 11, 14, 15, 17, 34], three studies used the anteromedial portal technique [5, 32, 33], and one study employed the anterolateral portal technique [13]. An outside-in technique was performed in one study [1], and an inlay technique was followed in two studies [16, 17], while an all-anterior approach was used in one study [19]. Different levels of preservation were reported; in this regard, as much fibre of PCL as possible was preserved in nine studies [1, 11, 13,14,15, 19, 32,33,34], and in another study, as many fibres as possible and synovium were preserved [10]. Furthermore, only posteromedial fibres were preserved in one study [5], while only anterolateral fibres were preserved in two other studies [16, 17]; on the other hand, a tensioning of the remaining fibres plus anterolateral bundle reconstruction were performed in one study [17].
Clinical and functional outcomes
All studies reported clinically significant improvement at final follow-up. The subjective IKDC scores observed in 11 studies [10, 11, 13,14,15,16,17, 19, 32,33,34] (only at the final follow-up in one study) were measured at 51.2 ± 6.5 at the preoperative stage and 80.2 ± 7.0 at the postoperative stage. On the other hand, eight studies [1, 5, 10, 11, 13, 16, 17, 32] reported the objective IKDC scores (only at the final follow-up in one study); in this regard, at the preoperative stage, the levels were measured as follows: A—0; B—8; C—130; D—143, whereas at the postoperative stage the levels were measured as follows: A—135; B—154; C—35; D—6 (Fig. 3).

A, B Sagittal Magnetic Resonance of the knee showing the remnant of the posterior cruciate ligament (blue lines) and the intact anterior cruciate ligament, highlighting difficulties in performing surgery due to limited space
Ten studies [1, 5, 11, 13,14,15, 19, 32,33,34] evaluated the Lysholm score (only at the final follow-up in one study), with mean results improving from 59.8 ± 4.8 preoperatively to 86.3 ± 5.9 postoperatively. Additionally, seven studies [11, 14, 15, 19, 32,33,34] (only at the final follow-up in one study) reported the Tegner score varying from 2.9 ± 0.9 preoperatively to 5.6 ± 1.0 postoperatively. Finally, three studies [10, 16, 17] reported OAK scores, with the mean results improving from 65.0 ± 3.5 at the preoperative stage to 88.0 ± 1.6 at the postoperative stage. It is noteworthy that only three studies [5, 11, 15] reported a return to sports activity, with a mean percentage of 90.8% (99/109). In particular, in the study by Deehan et al. the level of activity was evaluated as moderate to strenuous [5]; Kim reported that only eight patients returned to pre-injury activity, while the others were considered near-returns to activity [11], whereas in Lee’s study all patients returned to their pre-injury activity [15].
The results are presented in detail in Table 3.
Radiological outcomes
Eleven studies reported radiographic evidence of significant improvement at the final follow-up, regarding posterior translation [1, 10, 11, 13,14,15,16,17, 19, 33, 34]. In particular, the mean results of posterior translation improved from 11.5 ± 1.2 mm preoperatively to 3.3 ± 1.1 mm postoperatively. Eight studies reported comparative results, with regard to the contralateral side' [10, 13,14,15,16,17, 33, 34].
Moreover, nine (1.4%) patients reported osteoarthritis progression, while the gross appearance in MRI findings demonstrated grade I osteoarthritis in 29 patients (4.5%) and grade II in 14 patients (2.2%), with a mean signal intensity of 1.5. The results are detailed in Table 3.
Complications and failures
This systematic review revealed 13 (2.0%) failures and 33 minor complications (5.1%), including 10 cases of stiffness (1.6%), 21 (4.9%) screw removals, 1 (0.2%) injury of the peroneal nerve, and 1 (0.2%) fibular fracture.
The results are reported in detail in Table 3.
Discussion
The most important findings of the current study confirm that preservation of the remnants of the PCL reconstruction leads to good clinical results, regardless of the technique used. Regarding the clinical results, three types of grafts were used in the different studies, none of which stood out as having a clear benefit. Ahn et al. [1] arrived at the same conclusions when comparing the clinical results of arthroscopic PCL reconstruction using hamstrings or Achilles tendon allograft while preserving the remnant. Lee et al. [15] demonstrated that arthroscopic PCLR with remnant preservation had high return-to-sport rates and a high level of patient satisfaction. The average IKDC was 88.7 ± 14.1, and the average Lysholm score was 89.4 ± 12.3, with a minimum follow-up of two years.
Unlike for the anterior cruciate ligament (ACL), the extant literature on the posterior cruciate ligament (PCL) does not demonstrate the superiority of these techniques compared to conventional techniques [9, 12, 23], due to a lack of prospective, randomised studies, making it hard to decide whether preserving the remnant is advantageous or not. Nevertheless, some authors have described favourable results (IKDC rating of A or B in 97% to 100%) after chronic PCLR (> 6 months) ([1]. While these results are satisfactory, they are still not superior to those obtained using conventional techniques without preservation of the PCL stump, as shown by Kim et al. [11], with similar Lysholm scores, return-to-activity rate, and objective IKDC scores.
Similarly, regarding radiological results, Kim et al. [11] found satisfactory but comparable long-term radiological results. There is no statistically significant difference in the results on long-term stability between patients who underwent PCLR with or without remnant preservation: the mean differences in posterior tibial translation were similar in the two groups (classic group: 4.4 ± 3.0 mm; 82.6 ± 11.0; A: 21.7% and B: 73.9%; and preservation group: 4.1 ± 3.4 mm; 84.1 ± 10.7; A: 26.7% and B: 83.3%; p = …/n.s.).
On the other hand, these techniques do not seem to be associated with high complication rates; therefore, they appear feasible without too much difficulty. In this regard, this systematic literature review found only 13 (3%) failures and 10 cases of stiffness (2.35%), which is comparable with other techniques [2, 3, 27].
Some doubts still exist regarding the time from injury to surgery and how it can affect graft maturation in remnant preservation; correlation analysis showed that the time from injury to surgery had a statistically significant correlation with the signal intensity score [19]. Multivariate stepwise logistic regression analyses also showed that time from injury to surgery was the significant covariate [19]. These results imply that the time from injury to surgery might be a risk factor for graft signal intensity. However, the correlations were weak. Similarly, Lee et al. found that chronic groups were significantly inferior to acute or subacute groups in terms of side-to-side laxity difference at follow-up and observed no or very weak PCL remnant in the patients of subacute or chronic groups [17].
This systematic literature review has several limitations. First, the selection of articles was very restrictive as only studies with a minimum follow-up of two years and at least two cases were retained. Moreover, this literature review was based on low quality studies: level II, III and IV studies were included in the analyses, but no level I study was found. These factors may have affected the study’s conclusions. Another limitation is that there was only a direct comparison between remnant-preserving PCLRs and standard PCLRs, although conclusions could be drawn from such a comparison. Furthermore, most of the articles focussed on a surgical technique and reported retrospective series criteria. Additionally, the included studies demonstrated some heterogeneity regarding the type of reconstruction, the type of graft, the type of fixation, and the interval between injury and surgical management. Despite these discrepancies, all studies on PCLR with remnant preservation have reported satisfactory results. Accordingly, this opens up the possibility of new randomised studies concerning the type of reconstruction with preservation of the remnant.
For clinical relevance, standard PCL reconstruction is a highly effective operation in terms of improvement in functional status, knee stability, quality of life, and cost effectiveness. The remnant preservation technique requires more comprehensive diagnostic assessments of the PCL remnant patterns and more complicated surgical procedures. Given the current absence of high quality studies with long-term follow-up, the remnant-preserving techniques should be recommended only by experienced knee arthroscopic surgeons.
Conclusions
With the currently limited available data, all studies included in the review on PCLR with remnant preservation demonstrated satisfactory outcomes at mid-term follow-up despite their using different surgical techniques and different graft types, and the varying intervals from injury to surgery. However, the review did not find substantial evidence to support the superiority of the new techniques over the traditional ones.
References
Ahn JH, Yoo JC, Wang JH (2005) Posterior cruciate ligament reconstruction: double-loop hamstring tendon autograft versus Achilles tendon allograft–clinical results of a minimum 2-year follow-up. Arthroscopy 21:965–969
Ahn S, Lee YS, Song YD, Chang CB, Kang SB, Choi YS (2016) Does surgical reconstruction produce better stability than conservative treatment in the isolated PCL injuries? Arch Orthop Trauma Surg 136:811–819
Ansari AS, Dennis BB, Horner NS, Zhu M, Brookes C, Khan M, Grant JA (2019) Influence of graft source on postoperative activity and joint laxity in posterior cruciate ligament reconstruction: a systematic review. Arthroscopy 35:262–274
Chen YJ, Yang CP, Ho CS, Weng CJ, Chen AC, Hsu WH, Hsu KY, Chan YS (2022) Midterm outcomes after revision posterior cruciate ligament reconstruction with a single-bundle transtibial autograft. Orthop J Sports Med 10:23259671221115424
Deehan DJ, Salmon LJ, Russell VJ, Pinczewski LA (2003) Endoscopic single-bundle posterior cruciate ligament reconstruction: results at minimum 2-year follow-up. Arthroscopy 19:955–962
Fanelli GC (2021) Posterior cruciate ligament-part 1. J Knee Surg 34:471
Fanelli GC (2021) Posterior cruciate ligament-part 2. J Knee Surg 34:581
Fanelli GC (2021) Posterior cruciate ligament. Sports Med Arthrosc Rev 28:1
Huang H, Nagao M, Nishio H, Kaneko H, Saita Y, Takazawa Y, Ikeda H, Kaneko K, Ishijima M (2021) Remnant preservation provides good clinical outcomes after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 29:3763–3772
Jung YB, Jung HJ, Song KS, Kim JY, Lee HJ, Lee JS (2010) Remnant posterior cruciate ligament-augmenting stent procedure for injuries in the acute or subacute stage. Arthroscopy 26:223–229
Kim SJ, Kim SH, Chun YM, Hwang BY, Choi DH, Yoon JY (2012) Clinical comparison of conventional and remnant-preserving transtibial single-bundle posterior cruciate ligament reconstruction combined with posterolateral corner reconstruction. Am J Sports Med 40:640–649
Kosy JD, Walmsley K, Gordon EA, Heddon SV, Anaspure R, Schranz PJ, Mandalia VI (2021) Remnant preservation does not affect accuracy of tibial tunnel positioning in single-bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 29:1157–1163
Lee DC, Shon OJ, Kwack BH, Lee SJ (2013) Proprioception and clinical results of anterolateral single-bundle posterior cruciate ligament reconstruction with remnant preservation. Knee Surg Relat Res 25:126–132
Lee DW, Jang HW, Lee YS, Oh SJ, Kim JY, Song HE, Kim JG (2014) Clinical, functional, and morphological evaluations of posterior cruciate ligament reconstruction with remnant preservation: minimum 2-year follow-up. Am J Sports Med 42:1822–1831
Lee DW, Kim JG, Yang SJ, Cho SI (2019) Return to sports and clinical outcomes after arthroscopic anatomic posterior cruciate ligament reconstruction with remnant preservation. Arthroscopy 35:2658-2668.e1
Lee KH, Jung YB, Jung HJ, Jang EC, Song KS, Kim JY, Lee SH (2011) Combined posterolateral corner reconstruction with remnant tensioning and augmentation in chronic posterior cruciate ligament injuries: minimum 2-year follow-up. Arthroscopy 27:507–515
Lee SH, Jung YB, Lee HJ, Jung HJ, Kim SH (2013) Remnant preservation is helpful to obtain good clinical results in posterior cruciate ligament reconstruction: comparison of clinical results of three techniques. Clin Orthop Surg 5:278–286
Liu CH, Chiu CH, Chang SS, Yeh WL, Chen AC, Hsu KY, Weng CJ, Chan YS (2022) Clinical and functional outcomes of isolated posterior cruciate ligament reconstruction in patients over the age of 40 years. BMC Musculoskelet Disord 23:210. https://doi.org/10.1186/s12891-022-05151-w
Liu S, Sun Y, Chen T, Tao H, Hu Y, Chen S, Chen J (2018) Time from injury to surgery affects graft maturation following posterior cruciate ligament reconstruction with remnant preservation: a magnetic resonance imaging-based study. Arthroscopy 34:2846–2854
Longo UG, Viganò M, Candela V, de Girolamo L, Cella E, Thiebat G, Salvatore G, Ciccozzi M, Denaro V (2021) Epidemiology of posterior cruciate ligament reconstructions in Italy: a 15-year study. J Clin Med 10:499. https://doi.org/10.3390/jcm10030499
Mestriner MB, Cury RPL, Dos Santos NA, de Oliveira VM, de Camargo OPA, Belloti JC (2021) Double-bundle posterior cruciate ligament reconstruction: No differences between two types of autografts in isolated or combined lesions. Knee 27:140–150
Muka T, Glisic M, Milic J, Verhoog S, Bohlius J, Bramer W, Chowdhury R, Franco OH (2020) A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. Eur J Epidemiol 35:49–60
Okutan AE, Kalkışım M, Gürün E, Ayas MS, Aynacı O (2022) Tibial slope, remnant preservation, and graft size are the most important factors affecting graft healing after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 30:1584–1593
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Paras T, Sabzevari S, Solomon D, Smith C, McDonough C, Lin A (2022) Trends in level of evidence of systematic reviews in sports medicine, 2010–2020: a systematic review and meta-analysis. Orthop J Sports Med 10:23259671221121330
Schlumberger M, Schuster P, Eichinger M, Mayer P, Mayr R, Immendörfer M, Richter J (2020) Posterior cruciate ligament lesions are mainly present as combined lesions even in sports injuries. Knee Surg Sports Traumatol Arthrosc 28:2091–2098
Shin YS, Kim HJ, Lee DH (2017) No clinically important difference in knee scores or instability between transtibial and inlay techniques for PCL reconstruction: a systematic review. Clin Orthop Relat Res 475:1239–1248
Song E, Ang L, Park JY, Jun EY, Kim KH, Jun J, Park S, Lee MS (2021) A scoping review on biomedical journal peer review guides for reviewers. PLoS ONE 16:e0251440
Vermeijden HD, van der List JP, DiFelice GS (2020) Arthroscopic posterior cruciate ligament primary repair. Sports Med Arthrosc Rev 28:23–29
Winkler PW, Zsidai B, Wagala NN, Hughes JD, Horvath A, Senorski EH, Samuelsson K, Musahl V (2021) Evolving evidence in the treatment of primary and recurrent posterior cruciate ligament injuries, part 1: anatomy, biomechanics and diagnostics. Knee Surg Sports Traumatol Arthrosc 29:672–681
Winkler PW, Zsidai B, Wagala NN, Hughes JD, Horvath A, Senorski EH, Samuelsson K, Musahl V (2021) Evolving evidence in the treatment of primary and recurrent posterior cruciate ligament injuries, part 2: surgical techniques, outcomes and rehabilitation. Knee Surg Sports Traumatol Arthrosc 29:682–693
Yoon KH, Bae DK, Song SJ, Cho HJ, Lee JH (2011) A prospective randomized study comparing arthroscopic single-bundle and double-bundle posterior cruciate ligament reconstructions preserving remnant fibers. Am J Sports Med 39:474–480
Yoon KH, Kim JS, Park JY, Park SY, Kiat RYD, Kim SG (2021) Comparable clinical and radiologic outcomes between an anatomic tunnel and a low tibial tunnel in remnant-preserving posterior cruciate ligament reconstruction. Orthop J Sports Med 9:2325967120985153
Yoon KH, Kim JS, Park JY, Park SY, Kiat RYD, Kim SG (2021) Comparable clinical and radiological outcomes between anatomical and high femoral tunnels in posterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 29:1936–1943
Zsidai B, Horvath A, Winkler PW, Narup E, Kaarre J, Svantesson E, Musahl V, Hamrin Senorski E, Samuelsson K (2022) Different injury patterns exist among patients undergoing operative treatment of isolated PCL, combined PCL/ACL, and isolated ACL injuries: a study from the Swedish National Knee Ligament Registry. Knee Surg Sports Traumatol Arthrosc 30:3451–3460
Acknowledgements
This study was supported and funded by the Italian Ministry of Health—"Ricerca Corrente".
Funding
Open access funding provided by Università degli Studi di Milano within the CRUI-CARE Agreement. None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethical approval
Not needed.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
D’Ambrosi, R., Hallé, A. & Hardy, A. Good clinical and radiological results following remnant-preserving posterior cruciate ligament reconstruction: a systematic review. Knee Surg Sports Traumatol Arthrosc 31, 2418–2432 (2023). https://doi.org/10.1007/s00167-022-07192-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-022-07192-z