
Abstract
Introduction
The assessment of volume responsiveness and the decision to administer a fluid bolus is a common dilemma facing physicians caring for critically ill patients. Static markers of cardiac preload are poor predictors of volume responsiveness, and dynamic markers are often limited by the presence of spontaneous respirations or cardiac arrhythmias. Passive leg raising (PLR) represents an endogenous volume challenge that can be used to predict fluid responsiveness.
Methods
Medical intensive care unit (ICU) patients requiring volume expansion were eligible for enrollment. Non-invasive measurements of stroke volume (SV) were obtained before and during PLR using a transthoracic Doppler ultrasound device prior to volume expansion. Measurements were then repeated following volume challenge to classify patients as either volume responders or non-responders based on their hemodynamic response to volume expansion. The change in SV from baseline during PLR was then compared with the change in SV with volume expansion to determine the ability of PLR in conjunction with SV measurement to predict volume responsiveness.
Results
A total of 102 fluid challenges in 89 patients were evaluated. In 47 of the 102 fluid challenges (46.1%), SV increased by ≥15% after volume infusion (responders). A SV increase induced by PLR of ≥15% predicted volume responsiveness with a sensitivity of 81%, specificity of 93%, positive predictive value of 91% and negative predictive value of 85%.
Conclusions
Non-invasive SV measurement and PLR can predict fluid responsiveness in a broad population of medical ICU patients. Less than 50% of ICU patients given fluid boluses were volume responsive.
Similar content being viewed by others

Introduction
Circulatory insufficiency is a common clinical problem faced by physicians caring for critically ill patients. The decision to employ volume expansion (VE) in these patients is complicated [1]. If a patient is preload responsive, then VE improves cardiac output (CO). Early resuscitation protocols that include fluid therapy can be life saving early in the course of sepsis [2, 3]. However, in a preload unresponsive patient, volume administration has no hemodynamic benefit. Liberal volume resuscitation can exacerbate pulmonary edema, precipitate respiratory failure, prolong mechanical ventilation times, and contribute to the development of intra-abdominal hypertension [4–6]. Prior studies have shown positive fluid balance to correlate with reduced survival [7–9]. In addition, prospective studies have shown that less than 50% of critically ill patients respond to the fluid boluses that are deemed necessary by treating clinicians [10–14]. A simple, non-invasive bedside test to determine volume responsiveness that would assist clinicians in facing this daily dilemma would have significant utility.
Passive leg raising (PLR) is a simple maneuver used for generations as an initial intervention for patients in shock. This procedure rapidly returns 150 to 200 ml of blood from the veins of the lower extremities to the central circulation [15]. As a result of increased ventricular preload, the CO is augmented according to the degree of preload reserve, and rapidly reversed when the legs are returned to a horizontal position. PLR therefore constitutes a reversible volume challenge during which hemodynamic changes can be measured [16].
The aim of our study was to determine if noninvasive stroke volume (SV) measurement could be used in conjunction with PLR to predict the hemodynamic response to VE.
Materials and methods
Patients
This study was conducted at Barnes-Jewish Hospital, a university-affiliated, urban teaching hospital. The study was approved by the Washington University School of Medicine Human Studies Committee. As the protocol was considered part of routine practice, informed consent was waived. Patients were informed that they participated in this study. Patients were enrolled from the medical intensive care unit (ICU), and any patient requiring VE as determined by the ICU attending physician was eligible for enrollment. No specific criteria for circulatory insufficiency were required for study entry. However, the decision of the ICU attending to administer fluid was based on clinical signs of inadequate tissue perfusion (e.g. escalating vasopressor requirement, decreasing urine output, etc.) and his/her clinical impression that the patient should be given a trial of volume expansion. Exclusion criteria included known aortic or pulmonary valve disease, known ascending aortic aneurysm, or contraindication to PLR for any reason.
Data collection
Stroke volume measurements were taken using a non-invasive, transthoracic Doppler ultrasound device (USCOM®; Uscom Ltd., Sydney, Australia). All measurements were performed by a single investigator (ST) following training on the device. Each study measurement was taken in accordance with a previously described protocol designed to optimize accuracy and reliability [17]. The device used directly measures the blood flow through either the aortic or pulmonary valves. For each patient studied, both positions were attempted and the location that resulted in the best signal was used.
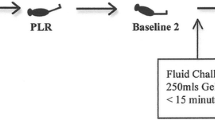
Study measurements were taken in four stages (Figure 1). In stage one the patient was placed in a semi-recumbent position with the head elevated at 45 degrees. In stage two, the patient was positioned supine with the legs straight and elevated at 45 degrees for two minutes. Stage three readings were taken two minutes after the patient was returned to the baseline position, and stage four immediately following VE. Calibrated automatic bed elevation (using standard ICU beds) was used to move the patient between stages.

Patient positioning during the four stages of measurement. After each change in position, two minutes elapsed before readings were recorded. The angle of elevation of the head or legs was 45 degrees. The patient's position was not changed between stages three and four.
Products for VE varied according to the order of the attending physician and included normal saline, Ringer's lactate and hetastarch. The volume administered in each case was at least 500 ml, and was given as a pressurized rapid infusion.
Vasopressor doses and ventilator settings were not changed at any time while a patient was being studied. Lower extremity compression devices were removed prior to the initial readings. Study measurements were recorded before, during, and after PLR and after VE throughout the stages described above.
Definition of volume responsiveness
Patients were classified according to their hemodynamic response to VE. Responders had a SV increment of at least 15% in response to VE (an increase in SV from stage one to stage four), while non-responders had a SV increase of less than 15%. Cutoff values of 10% to 15% have been previously used as representing a significant change in SV and cardiac index in similar studies [1, 16, 18–20], and a 15% change was reported as a significant difference between two measures of CO by thermodilution [21].
Statistical analysis
Continuous data are expressed as mean ± standard deviation. The Student's t-test was used for comparisons made between parametric data, and nonparametric data were analyzed with the Mann-Whitney U test. For categorical variables, chi-squared or Fisher's exact tests were used to test for differences between groups. The areas under receiver operating characteristic (ROC) curves are expressed as the area ± standard error, and were compared using the Hanley-McNeil method [22]. All tests were two-tailed, and a P value of less than 0.05 was pre-determined to be statistically significant. Where applicable, the Bonferroni multiplicity adjustment to the P value considered statistically significant is given [23, 24]. Analyses were performed using the SPSS© version 11.0.1 software package (SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
A total of 102 volume challenges in 89 consecutive patients were evaluated. One patient had three studies performed, while the remaining patients with more than one study had two studies each. Repeat studies performed on the same patient were separated in time by at least 24 hours. Thirteen additional patients were examined, although either they were unable to tolerate the procedure (three patients), unable to cooperate due to confusion or delirium (six patients), or satisfactory Doppler signals could not be obtained (four patients).
Stroke volume increased by 15% or more in 47 (46.1%) instances (responders), and by less than 15% in 55 (53.9%) instances (non-responders). For the purposes of data analysis, each volume challenge was considered an independent observation regardless of whether it was part of multiple studies performed on the same patient.
The resulting pool of volume challenges were performed on patients who were aged 59.4 ± 15.1 years, with 58 (56.9%) men and 44 (43.1%) women. Fifty-nine (57.8%) patients were receiving vasopressor support, 67 (65.7%) were mechanically ventilated, with 14 (20.9%) of those fully accommodated to the ventilator, and their Acute Physiology and Chronic Health Evaluation II score was 18.5 ± 6.1. The time elapsed between ICU admission and study entry was 61.7 ± 106.2 hours. Cardiac arrhythmias were present in 18 (17.5%) patients (atrial fibrillation in eight, premature ventricular beats in six, and premature atrial beats in four). The patient characteristics are summarized in Table 1.
Effects of PLR and volume expansion
The initial hemodynamic measurements are summarized in Table 2. The responders had a significantly lower initial SV (68 ± 25 ml vs. 87 ± 30 ml, P<0.001 compared with the non-responders, although the CO (6.8 ± 2.5 L/min vs. 8.0 ± 2.9 L/min, P = 0.03), corrected flow time (FTc; 363 ± 70 ms vs. 398 ± 66 ms, P = 0.01), mean arterial pressure (MAP; 68 ± 13 mmHg vs. 74 ± 14 mmHg, P = 0.03), and heart rate (101 ± 20 beats/min vs. 93 ± 20 beats/min, P = 0.06) were not different between the groups (Bonferroni adjusted level of significance for all comparisons 0.01).
The hemodynamic readings taken throughout the four stages of measurements are summarized in Table 3. For the responders, PLR induced a significant increase in SV (68 ± 25 ml vs. 82 ± 30 ml, P = 0.001), but the CO (6.8 ± 2.5 L/min vs. 8.0 ± 2.8 L/min, P = 0.03), FTc (363 ± 70 ms vs. 380 ± 68 ms, P = 0.22), MAP (68 ± 13 mmHg vs. 72 ± 11 mmHg, P = 0.11), heart rate (101 ± 20 beats/min vs. 99 ± 21 beats/min, P = 0.64), and pulse pressure (42 ± 14 mmHg vs. 45 ± 14 mmHg, P = 0.23) were unchanged (Bonferroni adjusted level of significance for all comparisons 0.01). The increase in SV was completely reversed when the patient was returned to the semi-recumbent position.
In the non-responders, PLR did not induce a significant change in any of the hemodynamic values measured. The SV (87 ± 30 ml vs. 91 ± 33 ml, P = 0.58), CO (8.0 ± 2.9 L/min vs. 8.4 ± 3.5 L/min, P = 0.46), FTc (398 ± 66 ms vs. 404 ± 78 ms, P = 0.66), MAP (74 ± 14 mmHg vs. 74 ± 16 mmHg, P = 0.95), heart rate (93 ± 20 beats/min vs. 94 ± 21 beats/min, P = 0.84), and pulse pressure (48 ± 15 mmHg vs. 49 ± 17 mmHg, P = 0.97) remained unchanged during PLR.
The changes in SV compared with stage one induced by both PLR and VE were significantly higher in the responders compared with the non-responders. The SV increased in response to PLR in the responders and non-responders by 21.0% ± 12.5% and 3.2% ± 10.4%, respectively (P<0.001, Bonferroni adjusted level of significance 0.01; Figure 2). The SV increased in response to VE in the responders and non-responders by 26.3% ± 14.2% and 3.5% ± 8.6%, respectively (P < 0.001, Bonferroni adjusted level of significance 0.01). The PLR-induced increase in SV was reversed once the patient was taken out of the PLR position (Table 3).

Stroke volume change by stage for responders and non-responders. Each measurement is represented as a percent change from the measurement taken during stage one (* P < 0.001, Bonferonni adjusted level of significance 0.01). SV = stroke volume.
Central venous pressure
The initial central venous pressure (CVP) was not different between the groups of responders and non-responders (7.8 ± 4.9 mmHg vs. 8.1 ± 4.8 mmHg, P = 0.80; Table 2). Additionally, the change in CVP between stages one and four was not different between the responders and non-responders (2.1 ± 3.0 mmHg vs. 3.2 ± 2.3 mmHg, P = 0.13).
Prediction of volume response
A SV increase induced by PLR of 15% or more predicted volume response with a sensitivity of 81%, specificity of 93%, positive predictive value of 91%, and a negative predictive value of 85% (Figure 3).

Individual percent change in stroke volume during passive leg raise for responders and non-responders. The dashed line represents the cutoff value of 15%. The squares represent the means with SD of the two groups (* P < 0.001, Bonferonni adjusted level of significance 0.01). PLR = passive leg raise; SV = stroke volume.
The area under the ROC curve for the percent change in SV during PLR predicting a response to VE was 0.89 ± 0.04. Other than the SV, no hemodynamic index significantly changed during PLR. However, several other indices were different, although not statistically significant, at baseline between the responders and non-responders. ROC curves for these initial measures predicting volume response were also constructed. Compared with the SV change during PLR these indices were inferior at differentiating the responders from the non-responders, and included the stage one SV (ROC curve area 0.70 ± 0.05, P = 0.001), CO (0.62 ± 0.06, P < 0.001), CVP (0.52 ± 0.08, P < 0.001), MAP (0.63 ± 0.06, P < 0.001), and FTc (0.65 ± 0.06, P < 0.001). The ROC curves for SV change with PLR and initial CVP and SV are shown in Figure 4.

Receiver operating characteristic curves for predicting response to volume expansion. The dashed line represents the percent change in stroke volume (SV) during passive leg raise (PLR), the dotted line the stage one SV, and the solid line the stage one central venous pressure (CVP).
Repeatability of measurements
A repeatability analysis was performed using the paired readings for stages one and three from each patient. The hemodynamic effects of PLR are transient and reversible, and vasoactive agents were not changed between these measurements. Therefore, it is expected that the readings from these stages would not be different and can be used to validate the use of a 15% change in SV as being significant. Using the method described by Bland and Altman [25] the upper and lower limits of agreement between stages one and three were 13.9% (95% confidence interval (CI) = 13.2% to 14.6%) and -10.9% (95% CI = -11.6% to -10.2%), respectively. The corresponding plot of the log-transformed SV difference against mean is shown in Figure 5.

Bland-Altman plot of log-transformed difference against mean for paired stroke volume measurements from stages one and three. The dashed lines represent the log-transformed upper and lower limits of agreement (95% confidence interval for repeated measurements). SV = stroke volume.
Discussion
Our study demonstrates that a completely non-invasive SV measurement in conjunction with PLR can predict the hemodynamic response to VE. In our relatively unselected population of medical ICU patients, the change in SV with PLR was the only hemodynamic index with significant predictive ability. The initial CVP was not different between the groups of responders and non-responders, and the change in CVP did not correlate with the change in SV following VE. A repeatability analysis revealed that a cutoff of 15% representing a significant change in SV is reasonable.
The ultrasound device used in this study has been previously evaluated for accuracy and reliability. Knobloch and colleagues studied 36 patients undergoing coronary revascularization with 180 paired CO and SV measurements using the USCOM® and a pulmonary artery catheter (PAC) [26]. Good correlation was found for both CO and SV (correlation index 0.79, P < 0.01 and 0.95, P < 0.01, respectively), and a Bland-Altman analysis demonstrated a bias of 0.23 ± 1.01 L/min for the CO measurements. Chand and colleagues studied 50 patients following coronary artery bypass surgery and compared SV measurements obtained with the USCOM® and the PAC [27]. The SV measurements demonstrated a bias of 1.0 ml (limits of agreement -1.5 ml to 3.5 ml) for aortic measurements and 1.6 ml (limits of agreement -0.21 ml to 3.4 ml) for pulmonary readings. Tan and colleagues examined 24 mechanically ventilated patients following cardiac surgery and compared 40 paired CO readings obtained by the USCOM ® and the PAC [28]. The resulting bias between the two methods was 0.18 L/min with limits of agreement of -1.43 L/min to 1.78 L/min. Finally, Dey and Sprivulis developed and tested a protocol to optimize inter-assessor reliability with the USCOM® device [29]. Two trained physicians performed blinded assessments on 21 emergency department patients. The inter-assessor correlation coefficient for CO measurements was 0.91 (95% CI = 0.85 to 0.95, P < 0.001), and the average difference between paired readings was 0.2 ± 0.2 L/min.
In the largest similar study to date, Monnet and colleagues studied 71 mechanically ventilated patients with an esophageal Doppler monitor in place [18]. An increase in aortic blood flow of 10% or more during PLR was found to predict volume response with a sensitivity of 97% and specificity of 94%. Boulain and colleagues studied 39 patients with a PAC and radial arterial line in place, and found that the change in pulse pressure and SV were significantly correlated both during PLR and following VE [30]. Lafanechère and colleagues examined 22 intubated and fully sedated patients with an esophageal Doppler monitor in place [31]. An increase in aortic blood flow of more than 8% during PLR predicted volume response with a sensitivity of 90% and specificity of 83%. Finally, Monnet and colleagues studied 34 mechanically ventilated patients with arterial lines in place who were not necessarily fully accommodated to the ventilator [32]. Changes in arterial pulse pressure and pulse contour-derived cardiac index during end-expiratory occlusion of the ventilator as well as changes in cardiac index during PLR were examined. An increase in cardiac index of 10% or more during PLR predicted an increase in cardiac index following VE of 15% or more with a sensitivity of 91% and a specificity of 100%. Changes in pulse pressure and cardiac index during end-expiratory occlusion had similar predictive value.
Our specificity is comparable with these studies, but our sensitivity is somewhat lower. This may be the result of a less selected patient population and the inclusion of patients regardless of underlying diagnoses that may diminish the effect of PLR. Included in our study was one patient with lower extremity contractures, two patients with extensive bilateral lower extremity deep venous thrombosis, two chronically bed-bound quadriplegic patients, two patients with unilateral below the knee amputation, one patient with massive ascites, and one patient with abdominal compartment syndrome. Additionally, the use of a less invasive technique may have contributed to our lower sensitivity. Non-invasive measures of cardiac function have been previously studied in conjunction with PLR, and also demonstrated lower sensitivity for predicting the response to VE. For example, Lamia and colleagues and Maizel and colleagues studied 24 and 34 patients, respectively, with transthoracic echocardiography in conjunction with PLR [19, 20]. Changes in CO and SV were predictive of volume response, but the sensitivities were somewhat lower at 77% and 69%, respectively.
The dilemma of which patients to subject to VE is encountered daily in the ICU. One of the principal uses for the PAC was to differentiate between various etiologies of hypotension and thereby guide therapy to optimize a patients' hemodynamic status [33]. However, with numerous clinical trials showing no benefit, concerns about safety, and rampant misinterpretation of data, the PAC is being used infrequently now in North American ICUs. This is likely to be contributing to a situation of probable under-monitoring of many critically ill patients [34–39]. Many intensivists now base most of their VE decisions on the CVP [2, 40]. However, the CVP is a poor predictor of volume responsiveness and should not be used to make clinical decisions regarding fluid management [10, 41]. This underscores the need for alternative fluid management strategies.
This study has some limitations. First, there were 13 additional patients that were to be enrolled, but were either unable to perform PLR or an adequate Doppler signal could not be obtained. However, analgesia or sedation may have facilitated successful measurements in many of these patients. Second, the majority of patients enrolled in our study had sepsis or hypovolemia as the etiology of their circulatory insufficiency. This may limit somewhat the applicability of this technique. Third, there was a significant difference in the presence of arrhythmias between the groups of responders and non-responders. This clouds the issue of whether or not this technique can be employed in patients with arrhythmia. However, the SV change with PLR predicted the correct SV response to VE in 16 of the 18 patients with arrhythmia.
Finally, the use of repeat studies on the same patient as independent observations may have impacted the results of the analysis. It is possible that sequential measurements taken on the same patient were correlated, which could alter the error term for any given analysis. However, the patients enrolled in this study were being actively treated in the ICU, and repeat studies on the same patient were separated in time by at least 24 hours. Hemodynamic interventions performed in that time would presumably impact the results of subsequent studies, minimizing any correlation that may exist between the two studies. In support of this assertion, a limited analysis was repeated using only the first challenge on each patient, with results similar to those for the complete data set. The SV increased in response to PLR in the responders and non-responders by 21.7 ± 12.7% and 3.2 ± 12.0%, respectively (P < 0.001). The SV increased in response to VE in the responders and non-responders by 26.3 ± 13.3% and 2.0 ± 8.5%, respectively (P < 0.001). A SV increase induced by PLR of 15% or more predicted volume response with a sensitivity of 79%, specificity of 91%, positive predictive value of 90%, and a negative predictive value of 82%. The upper and lower limits of agreement in the repeatability analysis were 14.4% and -11.2%, respectively.
Conclusions
We have demonstrated that a transthoracic Doppler ultrasound device can be used in conjunction with PLR to predict volume responsiveness in a variety of unselected medical ICU patients. Less than 50% of the patients subjected to fluid loading were volume responsive, underscoring the need for routine application of such methods when VE is considered. As with many non-invasive diagnostic maneuvers, results from this technique are likely best interpreted and clinically applied as one part of a larger clinical picture with the ultimate goal being a decrease in the amount of fluid loading that does not result in improved cardiac output.
Key messages
-
Non-invasive stroke volume measurement using transthoracic ultrasound can be utilized to determine fluid responsiveness in critically ill patients.
-
Stroke volume changes in response to PLR correlate well with fluid challenges as a predictor of fluid responsiveness in critically ill patients.
-
CVP measurements do not accurately reflect fluid responsiveness in critically ill patients.
-
Less than 50% of ICU patients given fluid boluses are volume responsive.
Abbreviations
- CI:
-
confidence interval
- CO:
-
cardiac output
- CVP:
-
central venous pressure
- FTc:
-
corrected flow time
- ICU:
-
intensive care unit
- MAP:
-
mean arterial pressure
- PAC:
-
pulmonary artery catheter
- PLR:
-
passive leg raise
- ROC:
-
receiver operating characteristic
- SV:
-
stroke volume
- VE:
-
volume expansion.
References
Michard F, Teboul JL: Predicting fluid responsiveness in ICU patients. Chest 2002, 121: 2000-2008. 10.1378/chest.121.6.2000
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M: Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001, 345: 1368-1377. 10.1056/NEJMoa010307
Micek ST, Roubinian N, Heuring T, Bode M, Williams J, Harrison C, Murphy T, Prentice D, Ruoff BE, Kollef MH: Before-after study of a standardized hospital order set for the management of septic shock. Crit Care Med 2006, 34: 2707-2713. 10.1097/01.CCM.0000241151.25426.D7
Brandstrup B, Tønnesen H, Beier-Holgersen R, Hjortsø E, Ørding H, Lindorff-Larsen K, Rasmussen MS, Lanng C, Wallin L, Iversen LH, Gramkow CS, Okholm M, Blemmer T, Svendsen PE, Rottensten HH, Thage B, Riis J, Jeppesen IS, Teilum D, Christensen AM, Graungaard B, Pott F: Effects of intravenous fluid restriction on postoperative complications: comparison of two perioperative fluid regimens. Annals of Surgery 2003, 238: 641-648. 10.1097/01.sla.0000094387.50865.23
Upadya A, Tilluckdharry L, Muralidharan V, Amoateng-Adjepong Y, Manthous CA: Fluid balance and weaning outcomes. Intensive Care Med 2005, 31: 1643-1647. 10.1007/s00134-005-2801-3
Malbrain ML, Chiumello D, Pelosi P, Bihari D, Innes R, Ranieri VM, Del Turco M, Wilmer A, Brienza N, Malcangi V, Cohen J, Japiassu A, De Keulenaer BL, Daelemans R, Jacquet L, Laterre PF, Frank G, de Souza P, Cesana B, Gattinoni L: Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: a multi-center epidemiological study. Crit Care Med 2005, 33: 315-322. 10.1097/01.CCM.0000153408.09806.1B
Vincent JL, Sakr Y, Sprung CL, Ranieri VM, Reinhart K, Gerlach H, Moreno R, Carlet J, Le Gall JR, Payen D: Sepsis in European intensive care units: Results of the SOAP study. Crit Care Med 2006, 34: 344-353. 10.1097/01.CCM.0000194725.48928.3A
Alsous F, Khamiees M, DeGirolamo A, Amoateng-Adjepong Y, Manthous CA: Negative fluid balance predicts survival in patients with septic shock. Chest 2000, 117: 1749-1754. 10.1378/chest.117.6.1749
Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AF Jr, Hite RD, Harabin AL: Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006, 354: 2564-2575. 10.1056/NEJMoa062200
Osman D, Ridel C, Ray P, Monnet X, Anguel N, Richard C, Teboul JL: Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge. Crit Care Med 2007, 35: 64-68. 10.1097/01.CCM.0000249851.94101.4F
Michard F, Boussat S, Chemla D, Anguel N, Mercat A, Lecarpentier Y, Richard C, Pinsky MR, Teboul JL: Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med 2000, 162: 134-138.
Sakka SG, Bredle DL, Reinhart K, Meier-Hellmann A: Comparison between intrathoracic blood volume and cardiac filling pressures in the early phase of hemodynamic instability of patients with sepsis or septic shock. J Crit Care 1999, 14: 78-83. 10.1016/S0883-9441(99)90018-7
Michard F, Alaya S, Zarka V, Bahloul M, Richard C, Teboul JL: Global end-diastolic volume as an indicator of cardiac preload in patients with septic shock. Chest 2003, 124: 1900-1908. 10.1378/chest.124.5.1900
Vieillard-Baron A, Chergui K, Rabiller A, Peyrouset O, Page B, Beauchet A, Jardin F: Superior vena caval collapsibility as a gauge of volume status in ventilated septic patients. Intensive Care Med 2004, 30: 1734-1739.
Rutlen DL, Wackers FJ, Zaret BL: Radionuclide assessment of peripheral intravascular capacity: a technique to measure intravascular volume changes in the capacitance circulation in man. Circulation 1981, 64: 146-152.
Monnet X, Teboul JL: Passive leg raising. Intensive Care Med 2008, 34: 659-663. 10.1007/s00134-008-0994-y
Dey I, Sprivulis P: Emergency physicians can reliably assess emergency department patient cardiac output using the USCOM continuous wave Doppler cardiac output monitor. Emerg Med Australas 2005, 17: 193-199.
Monnet X, Rienzo M, Osman D, Anguel N, Richard C, Pinsky MR, Teboul JL: Passive leg raising predicts fluid responsiveness in the critically ill. Crit Care Med 2006, 34: 1402-1407. 10.1097/01.CCM.0000215453.11735.06
Lamia B, Ochagavia A, Monnet X, Chemla D, Richard C, Teboul JL: Echocardiographic prediction of volume responsiveness in critically ill patients with spontaneous breathing activity. Intensive Care Med 2007, 33: 1125-1132. 10.1007/s00134-007-0646-7
Maizel J, Airapetian N, Lorne E, Tribouilloy C, Massy Z, Slama M: Diagnosis of central hypovolemia by using passive leg raising. Intensive Care Med 2007, 33: 1133-1138. 10.1007/s00134-007-0642-y
Stetz CW, Miller RG, Kelly GE, Raffin TA: Reliability of the thermodilution method in the determination of cardiac output in clinical practice. Am Rev Respir Dis 1982, 126: 1001-1004.
Hanley JA, McNeil BJ: A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983, 148: 839-843.
Sankoh AJ, Huque MF, Dubey SD: Some comments on frequently used multiple endpoint adjustment methods in clinical trials. Stat Med 1997, 16: 2529-2542. 10.1002/(SICI)1097-0258(19971130)16:22<2529::AID-SIM692>3.0.CO;2-J
Šidák Z: Rectangular confidence regions for the means of multivariate normal distributions. J Am Stat Assoc 1967, 62: 626-633. 10.2307/2283989
Bland JM, Altman DG: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1: 307-310. 10.1016/S0140-6736(86)91008-1
Knobloch K, Lichtenberg A, Winterhalter M, Rossner D, Pichlmaier M, Phillips R: Non-invasive cardiac output determination by two-dimensional independent Doppler during and after cardiac surgery. Ann Thorac Surg 2005, 80: 1479-1484. 10.1016/j.athoracsur.2004.12.034
Chand R, Mehta Y, Trehan N: Cardiac output estimation with a new Doppler device after off-pump coronary artery bypass surgery. J Cardiothorac Vasc Anesth 2006, 20: 315-319. 10.1053/j.jvca.2005.05.024
Tan HL, Pinder M, Parsons R, Roberts B, van Heerden PV: Clinical evaluation of USCOM ultrasonic cardiac output monitor in cardiac surgical patients in intensive care unit. Br J Anaesth 2005, 94: 287-291. 10.1093/bja/aei054
Dey I, Sprivulis P: Emergency physicians can reliably assess emergency department patient cardiac output using the USCOM continuous wave Doppler cardiac output monitor. Emerg Med Australas 2005, 17: 193-199.
Boulain T, Achard JM, Teboul JL, Richard C, Perrotin D, Ginies G: Changes in BP induced by passive leg raising predict response to fluid loading in critically ill patients. Chest 2002, 121: 1245-1252. 10.1378/chest.121.4.1245
Lafanechère A, Pène F, Goulenok C, Delahaye A, Mallet V, Choukroun G, Chiche JD, Mira JP, Cariou A: Changes in aortic blood flow induced by passive leg raising predict fluid responsiveness in critically ill patients. Critical Care 2006, 10: R132. 10.1186/cc5044
Monnet X, Osman D, Ridel C, Lamia B, Richard C, Teboul JL: Predicting volume responsiveness by using the end-expiratory occlusion in mechanically ventilated intensive care unit patients. Crit Care Med 2009, 37: 951-956. 10.1097/CCM.0b013e3181968fe1
Swan HJ, Ganz W, Forrester J, Marcus H, Diamond G, Chonette D: Catheterization of the heart in man with use of a flow directed balloon-tipped catheter. N Engl J Med 1970, 283: 447-451.
Connors AF Jr, Speroff T, Dawson NV, Thomas C, Harrell FE Jr, Wagner D, Desbiens N, Goldman L, Wu AW, Califf RM, Fulkerson WJ Jr, Vidaillet H, Broste S, Bellamy P, Lynn J, Knaus WA: The effectiveness of right heart catheterization in the initial care of critically ill patients. JAMA 1996, 276: 889-897. 10.1001/jama.276.11.889
Sandham JD, Hull RD, Brant RF, Knox L, Pineo GF, Doig CJ, Laporta DP, Viner S, Passerini L, Devitt H, Kirby A, Jacka M: A randomized, controlled trial of the use of pulmonary artery catheters in high-risk surgical patients. N Engl J Med 2003, 348: 5-14. 10.1056/NEJMoa021108
Binanay C, Califf RM, Hasselblad V, O'Connor CM, Shah MR, Sopko G, Stevenson LW, Francis GS, Leier CV, Miller LW: Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: the ESCAPE trial. JAMA 2005, 294: 1625-1633. 10.1001/jama.294.13.1625
Harvey S, Harrison DA, Singer M, Ashcroft J, Jones CM, Elbourne D, Brampton W, Williams D, Young D, Rowan K: Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man). Lancet 2005, 366: 472-477. 10.1016/S0140-6736(05)67061-4
Wheeler AP, Bernard GR, Thompson BT, Schoenfeld D, Wiedemann HP, deBoisblanc B, Connors AF Jr, Hite RD, Harabin AL: Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006, 354: 2213-2224. 10.1056/NEJMoa061895
Squara P, Bennett D, Perret C: Pulmonary artery catheter: does the problem lie in the users. Chest 2002, 121: 2009-2015. 10.1378/chest.121.6.2009
Boldt J, Lenz M, Kumle B, Papsdorf M: Volume replacement strategies on intensive care units: results from a postal survey. Intensive Care Med 1998, 24: 147-151. 10.1007/s001340050536
Marik PE, Baram M, Vahid B: Does central venous pressure predict fluid responsiveness? Chest 2008, 134: 172-178. 10.1378/chest.07-2331
Acknowledgements
This study received no financial support. The ultrasound device used was provided by Uscom, Ltd., although they had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
WI conceived and designed the study, participated in drafting the manuscript, and provided supervision. MK participated in the study design, provided critical revision of the manuscript, and provided supervision. ST performed data acquisition, participated in drafting the manuscript, and performed statistical analysis. WI had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Thiel, S.W., Kollef, M.H. & Isakow, W. Non-invasive stroke volume measurement and passive leg raising predict volume responsiveness in medical ICU patients: an observational cohort study. Crit Care 13, R111 (2009). https://doi.org/10.1186/cc7955
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc7955