
Abstract
Introduction
This study sought to assess whether the use of thoraco-pelvic supports during prone positioning in patients with acute lung injury/acute respiratory distress syndrome (ALI/ARDS) improves, deteriorates or leaves unmodified gas exchange, hemodynamics and respiratory mechanics.
Methods
We studied 11 patients with ALI/ARDS, sedated and paralyzed, mechanically ventilated in volume control ventilation. Prone positioning with or without thoraco-pelvic supports was applied in a random sequence and maintained for a 1-hour period without changing the ventilation setting. In four healthy subjects the pressures between the body and the contact surface were measured with and without thoraco-pelvic supports. Oxygenation variables (arterial and central venous), physiologic dead space, end-expiratory lung volume (helium dilution technique) and respiratory mechanics (partitioned between lung and chest wall) were measured after 60 minutes in each condition.
Results
With thoraco-pelvic supports, the contact pressures almost doubled in comparison with those measured without supports (19.1 ± 15.2 versus 10.8 ± 7.0 cmH2O, p ≤ 0.05; means ± SD). The oxygenation-related variables were not different in the prone position, with or without thoraco-pelvic supports; neither were the CO2-related variables. The lung volumes were similar in the prone position with and without thoraco-pelvic supports. The use of thoraco-pelvic supports, however, did lead to a significant decrease in chest wall compliance from 158.1 ± 77.8 to 102.5 ± 38.0 ml/cmH2O and a significantly increased pleural pressure from 4.3 ± 1.9 to 6.1 ± 1.8 cmH2O, in comparison with the prone position without supports. Moreover, when thoraco-pelvic supports were added, heart rate increased significantly from 82.1 ± 17.9 to 86.7 ± 16.7 beats/minute and stroke volume index decreased significantly from 37.8 ± 6.8 to 34.9 ± 5.4 ml/m2. The increase in pleural pressure change was associated with a significant increase in heart rate (p = 0.0003) and decrease in stroke volume index (p = 0.0241).
Conclusion
The application of thoraco-pelvic supports decreases chest wall compliance, increases pleural pressure and slightly deteriorates hemodynamics without any advantage in gas exchange. Consequently, we stopped their use in clinical practice.
Similar content being viewed by others

Introduction
Prone positioning is used and recommended as a rescue maneuver to improve arterial oxygenation in adult patients with acute lung injury (ALI), acute respiratory distress syndrome (ARDS) [1, 2] or chronic obstructive pulmonary disease [3], although its benefits with regard to outcome are not proven [4, 5].
Improved oxygenation implies, by definition, improvement of the ventilation/perfusion ratio. This can be achieved through different mechanisms, not mutually exclusive, each documented in the literature: (1) a more uniform distribution of alveolar inflation/ventilation, due to the lower gradient of transpulmonary pressure resulting from the changes in chest wall mechanics, with perfusion being less affected [6–9]; (2) a greater recruitment of the dorsal lung regions in comparison with the derecruitment of the ventral lung regions when changing from the supine to the prone position [10]; (3) an overall increase in end-expiratory lung volume (EELV) as a result of the more favorable position of the diaphragm [11].
Douglas and colleagues [12] used supports under the ribcage and the pelvis of patients with respiratory failure, to prevent their abdomen from bearing the entire weight of the torso. Indeed, some authors have advocated the use of thoraco-pelvic supports to avoid an increase in intra-abdominal pressure, which could limit diaphragm excursion and, consequently, alveolar ventilation in the most dependent lung regions [13, 14]. A survey study, in 29 intensive care units, found that thoraco-pelvic supports were routinely applied in 18 of them [15].
However, the use of thoraco-pelvic supports in the prone position has potential drawbacks, such as the possibility of developing pressure sores at the contact surfaces [16]. Because the effectiveness of this intervention is debated, in the present study we set out to investigate whether the use of thoraco-pelvic supports on patients with ALI/ARDS improves, worsens, or has no effect on respiratory mechanics, gas exchange, and hemodynamics.
Materials and methods
Study population
Eleven consecutive intubated patients with ALI/ARDS, defined in accordance with standard criteria [17], were included in the study. None of them had a history of chronic obstructive pulmonary disease, heart failure or severe head trauma. Their main clinical characteristics are summarized in Table 1. After completing the study and analyzing the data we realized the possible importance of the contact pressures. We therefore measured the contact pressures directly in four healthy volunteers with or without the thoraco-pelvic supports.
The study was approved by the Institutional Review Board of our hospital. Informed consent, because the patients were incompetent, was obtained in accordance with Italian national regulations (waived consent).
Study design
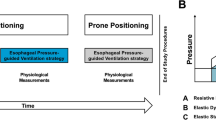
The patients were first studied in the supine position (1-hour baseline). Subsequently, they were studied in the prone position for 2 hours, for 1 hour with supports and for 1 hour without, in a randomized manner (see flow diagram in Figure 1) for a total duration of 3 hours study time.

Flow chart of the study protocol.
The patients were lying on air-cushioned beds (Total Care®; Hill Rom Services Inc., Batesville, IN, USA). In the supine position and in the prone position without supports, the body of each patient was in direct contact with the mattress. In prone position with supports, a roll was placed under the cranial part of the ribcage and a pillow under the pelvic region, so that most of the body weight rested on them. The thoraco-pelvic supports were placed so as to allow free abdominal movements (see Figure 2 and Table 2).

Patients' positions and contact pressures. Patients' positions used in the study: supine (top), prone without supports (center) and prone with thoraco-pelvic supports (bottom). The mean contact pressures (measured with pressure transducers in four healthy volunteers) are also indicated by white arrows. Table 2 shows detailed contact pressures at different sites and global values.
The patients were studied while sedated with fentanyl (1.5 to 5.5 μg/kg per hour) and midazolam (4 to 8 mg/hour), paralyzed with pancuronium bromide (0.05 to 0.1 mg/kg per hour) and ventilated in volume-control mode with a Servo Ventilator 300 C (Siemens, Solna, Sweden). Mechanical ventilation was set by the attending physician on a clinical basis and remained unchanged throughout the study periods. The baseline mean tidal volume was 565.3 ± 160.5 ml (7.2 ± 1.4 ml/kgIBW, where IBW stands for ideal body weight; means ± SD), respiratory rate was 17.1 ± 3.5 breaths/minute, inspiratory oxygen fraction was 0.43 ± 0.04, positive end-expiratory pressure (PEEP) was 10.8 ± 1.8 cmH2O, and plateau pressure was 22.4 ± 4.3 cmH2O.
Fluids, drug infusions and ventilator settings remained unchanged throughout the whole study period.
Measurements
Contact pressures
The pressures between the air-cushioned beds or thoraco-pelvic supports and the body (namely, the contact pressures) were measured in four healthy volunteers (age 28.7 ± 4.9 years, weight 66.2 ± 11.8 kg, body mass index 22.1 ± 2.0 kg/m2), in the same three conditions and body positions in which the patients were studied. A plastic bag with a volume of 250 ml containing 100 ml of water and equipped with a pressure transducer (Transpec IV L974; Abbott Ireland, Sligo, Ireland) was used. The zero of the pressure transducer was at the level of the plastic bag. In the supine position, pressure transducers were placed under the shoulders, the lumbar spine, and the sacrum. In the prone position, with and without the thoraco-pelvic supports, pressure transducers were placed in the corresponding positions, under the upper chest, the mesogastrium, and the pelvic region (Figure 2).
Gas exchanges and hemodynamics
All variables were recorded at the end of each study period. Blood gas tensions in the arterial and central venous blood were analysed with a blood gas analyzer (IL-1312 Blood Gas Manager; Instrumentation Laboratory, Milan, Italy). Minute metabolic carbon dioxide production, partial pressure of CO2 in mixed expired air, and end-tidal concentration of carbon dioxide were measured with a respiratory function monitor (CO2SMO™; Novametrix Medical Systems Inc., Wallingford, CT, USA). The venous admixture (estimated from the central venous blood values), the physiological dead space, and the alveolar dead space were computed from standard formulae.
Blood pressures (central and arterial) were measured with disposable pressure transducers (Transpec IV L974) positioned at the mid-axillary line. Cardiac output was measured with the thermo-dilution method, using a Swan–Ganz Oximetry Paceport Thermo-dilution Catheter (Edwards Lifesciences, Irvine, CA, USA) in five patients, and by pulse contour analysis (PiCCO System™ version 4.1; Pulsion Medical System, Munich, Germany) in four. In the five patients with a Swan–Ganz catheter, pulmonary artery and wedge pressures were also recorded. The stroke volume index was computed as the stroke volume divided by the body surface area (BSA). The BSA was obtained with the formula BSA [m2] = 0.20247 × height [m]0.725 × weight [kg]0.425 [18].
End-expiratory lung volume and respiratory mechanics
EELVs at PEEP were measured with a simplified closed-circuit helium-dilution method, during an end-expiratory pause [19]. An anesthesia bag, filled with 1.5 liters of a known gas mixture (13% helium in oxygen) was connected to the airway opening previously clamped at end-expiration to maintain the PEEP level. Ten manual breaths were subsequently performed. The helium concentration in the bag was then measured with a helium analyzer (PK Morgan Ltd, Chatham, UK) and EELV was computed from the formula EELV = (Vi × [He]i/[He]f) - Vi, where Vi is the initial gas volume in the anesthesia bag and [He]i and [He]f are the initial and final concentrations of helium in the bag, respectively.
Airway pressures were measured proximally to the endotracheal tube with a dedicated pressure transducer (MPX 2010 DP; Motorola, Phoenix, AZ, USA). Mean airway pressures were calculated as the area under the airway pressure–time trace, divided by the duration of each breath. Esophageal and gastric pressures were measured with two radio-opaque balloons inflated with 0.5 to 1.0 ml of air (SmartCath; Bicore, Irvine, CA, USA) connected to a pressure transducer (Bentley Trantec; Bentley Laboratories, Irvine, USA). The esophageal and gastric balloons were both positioned in the stomach with the use of an endotracheal tube inserted through the mouth as a guide through the pharynx. The esophageal balloon was then retracted until it reached the upper third of the esophagus. In addition, to ensure the correct position of the catheters, an inspiratory occlusion was made, so that a check for concordant changes in airway, esophageal, and gastric pressures could be made.
Respiratory flow rates were measured with a heated pneumotachograph (Fleisch no. 2; Fleisch, Lausanne, Switzerland) inserted between the proximal tip of the endotracheal tube and the Y-piece of the breathing circuit. Flow and pressure signals were recorded on a personal computer for subsequent analysis with dedicated software (Colligo; Elekton, Milan, Italy). Tidal volumes were obtained by mathematical integration of the measured flow signal. The static compliance of each component of the respiratory system – respiratory system, chest wall, and lung – was calculated as a chord compliance, using standard formulae, with the rapid occlusion method [20]. The end-inspiratory pause button of the ventilator was actioned until airway, esophageal, and gastric pressures decreased from their maximum value to an apparent plateau. Similarly, end-expiratory airway, esophageal, and gastric pressures were recorded after an end-expiratory hold maneuver.
Transpulmonary pressure was computed as the difference between airway pressure and esophageal pressure, and the transdiaphragmatic pressure as the difference between esophageal pressure and gastric pressure. Pleural pressure change, gastric pressure change, and transpulmonary pressure change were calculated as the differences between end-inspiratory and end-expiratory esophageal pressure, gastric pressure, and transpulmonary pressure, respectively.
Intra-abdominal pressure was estimated by measuring the bladder pressure by the method of Cheatham and Safcsak [21].
Statistical analysis
Data are shown as means ± SD. All data were analyzed with SAS software (version 8.2; SAS Institute, Cary, NC, USA).
The study design included a baseline condition (supine) and two treatments (prone without supports and prone with supports). The treatments were administered to each patient in a randomized order, in accordance with a crossover design.
The effect of the two treatments and of the sequence of their administration was evaluated with an analysis of variance for repeated measures, performed with the SAS MIXED procedure. In addition, each study treatment (prone with and without supports) was compared with baseline (supine) by using paired t tests.
To explore the possible association between pleural pressure change and several tested variables, we used the SAS MIXED procedure, building a mixed-effect linear model, in which each patient was treated as a random coefficient. This procedure yielded the parameters of a global regression model, as well as an indication (p value) of the significance of the association itself.
Results
Contact pressures
Contact pressures recorded in four healthy subjects in the supine and in the prone position with and without supports are summarized in Figure 2. As shown, in shifting the subjects from the supine to the prone position without thoraco-pelvic supports, the contact pressures at thorax and sacrum/pubis did not change significantly, whereas pressures recorded at the abdominal wall surface increased (11.0 ± 1.8 versus 5.8 ± 2.9 cmH2O for the supine position). After application of the thoraco-pelvic supports the contact pressures at thorax and pubis increased significantly compared with those in the prone position without supports (29.0 ± 6.5 versus 17.0 ± 7.4 cmH2O and 28.3 ± 8.9 versus 4.5 ± 4.2 cmH2O, respectively) whereas the contact pressure at the abdominal wall surface was zero because the abdomen remained suspended.
End-expiratory lung volume and respiratory mechanics
The EELVs and the mechanics of the respiratory system, partitioned into the chest wall and lung components, are summarized in Table 3. Shifting the patients from the supine to the prone position, without supports, led to a decreasing trend of chest wall compliance and to a significant increase in lung compliance. Adding the thoraco-pelvic supports in the prone position led to a further significant decrease in chest wall compliance and a significant increase in pleural pressure. We found no sequence effect (that is, prone after supine or supine after prone; see Figure 1) on lung volumes and respiratory mechanics variables.
Gas exchange
Table 4 summarizes the gas exchange variables in the supine and in the prone position with and without thoraco-pelvic supports. As shown, the oxygenation-related variables in the arterial and central venous blood improved significantly in shifting the patients from supine to prone without thoraco-pelvic supports. The application of thoraco-pelvic supports did not lead to any further significant change. No significant differences were observed in CO2-related variables between the supine and the prone position with or without thoraco-pelvic supports. We found no sequence effect on gas exchange variables.
Hemodynamics
The application of thoraco-pelvic supports caused a significant increase in heart rate and a decrease in stroke volume index and in pulmonary artery pressures, in comparison with the prone position without supports. The other hemodynamic variables (notably cardiac index and systemic vascular resistance) were not affected by the application of thoraco-pelvic supports. There was no sequence effect on hemodynamic variables. We observed a significant association between the level of pleural pressure change and heart rate (p = 0.0003) and between pleural pressure change and stroke volume index (p = 0.0241) (see Figure 3 and Table 5).

Intrathoracic pressure and hemodynamics. Top panel, association between pleural pressure change (delta Ppl) and heart rate (HR); bottom panel, association between pleural pressure change and stroke volume index (SVI). Each patient is represented with a different symbol and the values recorded in the three different conditions are all indicated, together with the regression line about these points for each individual patient. A regression line for the whole model of association is also depicted (thick line). Pleural pressure change is significantly associated with heart rate (p = 0.0003) and with stroke volume index (p = 0.0241).
Discussion
In the present study we found that the prone position with thoraco-pelvic supports, as compared with the prone position without supports, did not affect gas exchange and lung volume but decreased the chest wall compliance, increased the pleural pressure and slightly modified the hemodynamic pattern (heart rate and stroke volume index). In addition, we confirmed the positive effects of the prone position on oxygenation when shifting ALI/ARDS patients from the supine to the prone position, as largely documented in the literature [4, 5].
Mechanics of the respiratory system
When, in previous studies, we directly investigated chest wall displacements by optoelectronic plethysmography we found that both in spontaneously breathing subjects and in paralysed patients with ALI/ARDS in the supine position, the ribcage accounted for about 37% of the chest wall displacement and the abdomen for 63% (that is, the ribcage compliance and abdominal wall compliance were 37% and 63%, respectively, of the whole chest wall compliance) [22, 23]. When the subjects were moved to the prone position without pelvic supports, the ribcage accounted for 46.5% of the chest wall displacement, and the abdomen for 53.5% [23]. In experimental animals, too, with a computed tomography scan we found a more even distribution of chest wall displacement [24] when shifting from supine to prone.
If we apply these figures to our actual patients we can estimate that in the supine position the ribcage compliance would have been 86.8 ± 56.3 ml/cmH2O and the abdominal wall compliance 148.4 ± 96.2 ml/cmH2O (total chest wall compliance 235.2 ± 152.5 ml/cmH2O), whereas in the prone position they would have been 73.5 ± 36.2 and 84.6 ± 41.6 ml/cmH2O, respectively (total chest wall compliance 158.1 ± 77.8 ml/cmH2O). This suggests that, in shifting from supine to prone without thoraco-pelvic supports, the decrease in abdominal wall compliance accounts for most of the decrease in chest wall compliance. If so, the use of thoraco-pelvic supports, which allows free movement of the abdominal wall, should be mostly indicated. In contrast, we found that applying the thoraco-pelvic supports led to a further decrease in chest wall compliance. Thus, at least in patients with ALI/ARDS, when using thoraco-pelvic supports, the possible improvement in abdominal chest wall compliance may be offset by the greater decrease of the ribcage compliance, possibly as a result of the increased contact pressures at the ribcage. In addition, the expected improvement in abdominal wall compliance with thoraco-pelvic supports could be lower than expected because of the greater baseline distension of the unsupported abdominal wall and the possible effects of pelvic supports on the lower abdominal mechanics.
Lung volumes, gas exchange and hemodynamics
In the present study, as shown previously [4, 5], the oxygenation variables increased significantly when the patients were shifted from supine to prone without thoraco-pelvic supports, but did not change when the supports were added. The average EELVs did not change in any position. However, the lung volume increased in some patients after being moved from the supine to the prone position, whereas in others it decreased, suggesting different individual interactions between the opposite effects of the prone position on recruitment (increased lung gas volume) and on increased pleural pressure (decreased transpulmonary pressure). We found that several hemodynamic variables changed significantly between the use and the non-use of supports in the prone position. Although we do not have direct evidence, we speculate that the independent variable that caused the hemodynamic changes is the increase in intrathoracic pressure associated with the use of thoraco-pelvic supports. The hemodynamic changes, in fact, are compatible with the homeostatic response to an initial decrease in effective circulating volume induced by an increase in pleural pressure. The correlation we found between the progressive increase in pleural pressure change and the decrease in stroke volume and increase in heart rate supports this hypothesis.
Clinical implications
One of the major complications related to the prone position are pressure sores, usually located at the weight-bearing sites such as the bony prominences where the contact pressures are the highest [4, 5, 25]. A relationship between pressure sores and the duration and magnitude of the contact pressure has been shown [26]. In patients in the prone position, a significantly higher number of new or worsening pressure sores has been found in comparison with the supine position [4, 5, 27]. The use of thoraco-pelvic supports, by increasing the contact pressures, because of a lower contact surface compared with lying with the body directly on the air-cushioned beds, could potentially increase skin-tissue damage.
Conclusion
This study suggests that the prone position primarily induces changes in pleural pressure, probably by modifying the geometry and mechanics of the chest wall. Adding the thoraco-pelvic supports does not provide any advantage in oxygenation but increases the pleural pressure. Moreover, although not investigated in this short-term study, increased contact pressures at the interface between the thoraco-pelvic supports and the body may increase, with time, the likelihood of pressure sores. Indeed, in clinical practice, we have stopped using thoraco-pelvic supports in the prone position.
Key messages
-
The prone position is a recognized rescue therapy for severe hypoxemia in ARDS.
-
Allowing free abdominal movement should improve lung mechanics and gas exchange on a theoretical basis.
-
This hypothesis was tested by studying respiratory mechanics (partitioned into lung and chest wall components), gas exchange and hemodynamics with and without thoraco-pelvic supports.
-
We could not show any benefit from using thoraco-pelvic supports.
-
Thoraco-pelvic supports are useless in ARDS patients in the prone position and merely increase the likelihood of pressure sores, as a result of increased contact pressures.
Abbreviations
- ALI:
-
= acute lung injury
- ARDS:
-
= acute respiratory distress syndrome
- BSA:
-
= body surface area
- EELV:
-
= end-expiratory lung volume
- PEEP:
-
= positive end-expiratory pressure.
References
Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall JC, Parker MM, et al.: Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med 2004, 32: 858-873. 10.1097/01.CCM.0000117317.18092.E4
Slutsky AS: The acute respiratory distress syndrome, mechanical ventilation, and the prone position. N Engl J Med 2001, 345: 610-612. 10.1056/NEJM200108233450811
Mentzelopoulos SD, Zakynthinos SG, Roussos C, Tzoufi MJ, Michalopoulos AS: Prone position improves lung mechanical behavior and enhances gas exchange efficiency in mechanically ventilated chronic obstructive pulmonary disease patients. Anesth Analg 2003, 96: 1756-1767. 10.1213/01.ANE.0000064282.79068.1E
Gattinoni L, Tognoni G, Pesenti A, Taccone P, Mascheroni D, Labarta V, Malacrida R, Di Giulio P, Fumagalli R, Pelosi P, et al.: Effect of prone positioning on the survival of patients with acute respiratory failure. N Engl J Med 2001, 345: 568-573. 10.1056/NEJMoa010043
Guerin C, Gaillard S, Lemasson S, Ayzac L, Girard R, Beuret P, Palmier B, Le QV, Sirodot M, Rosselli S, et al.: Effects of systematic prone positioning in hypoxemic acute respiratory failure: a randomized controlled trial. JAMA 2004, 292: 2379-2387. 10.1001/jama.292.19.2379
Gattinoni L, Pelosi P, Vitale G, Pesenti A, D'Andrea L, Mascheroni D: Body position changes redistribute lung computed-tomographic density in patients with acute respiratory failure. Anesthesiology 1991, 74: 15-23.
Pelosi P, Tubiolo D, Mascheroni D, Vicardi P, Crotti S, Valenza F, Gattinoni L: Effects of the prone position on respiratory mechanics and gas exchange during acute lung injury. Am J Respir Crit Care Med 1998, 157: 387-393.
Mutoh T, Guest RJ, Lamm WJ, Albert RK: Prone position alters the effect of volume overload on regional pleural pressures and improves hypoxemia in pigs in vivo. Am Rev Respir Dis 1992, 146: 300-306.
Richter T, Bellani G, Scott HR, Vidal Melo MF, Winkler T, Venegas JG, Musch G: Effect of prone position on regional shunt, aeration, and perfusion in experimental acute lung injury. Am J Respir Crit Care Med 2005, 172: 480-487. 10.1164/rccm.200501-004OC
Gattinoni L, Pelosi P, Valenza F, Mascheroni D: Patient positioning in acute respiratory failure. In Principles and Practice of Mechanical Ventilation. Edited by: Tobin M. New York: McGraw-Hill; 1994:1067-1076.
Pelosi P, Bottino N, Chiumello D, Caironi P, Panigada M, Gamberoni C, Colombo G, Bigatello LM, Gattinoni L: Sigh in supine and prone position during acute respiratory distress syndrome. Am J Respir Crit Care Med 2003, 167: 521-527. 10.1164/rccm.200203-198OC
Douglas WW, Rehder K, Beynen FM, Sessler AD, Marsh HM: Improved oxygenation in patients with acute respiratory failure: the prone position. Am Rev Respir Dis 1977, 115: 559-566.
Pelosi P, Croci M, Calappi E, Cerisara M, Mulazzi D, Vicardi P, Gattinoni L: The prone positioning during general anesthesia minimally affects respiratory mechanics while improving functional residual capacity and increasing oxygen tension. Anesth Analg 1995, 80: 955-960. 10.1097/00000539-199505000-00017
Pelosi P, Croci M, Calappi E, Mulazzi D, Cerisara M, Vercesi P, Vicardi P, Gattinoni L: Prone positioning improves pulmonary function in obese patients during general anesthesia. Anesth Analg 1996, 83: 578-583. 10.1097/00000539-199609000-00025
Leonet S, Fontaine C, Moraine JJ, Vincent JL: Prone positioning in acute respiratory failure: survey of Belgian ICU nurses. Intensive Care Med 2002, 28: 576-580. 10.1007/s00134-002-1274-x
Messerole E, Peine P, Wittkopp S, Marini JJ, Albert RK: The pragmatics of prone positioning. Am J Respir Crit Care Med 2002, 165: 1359-1363. 10.1164/rccm.2107005
Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, LeGall JR, Morris A, Spragg R: Report of the American-European consensus conference on ARDS: definitions, mechanisms, relevant outcomes and clinical trial coordination. The Consensus Committee. Intensive Care Med 1994, 20: 225-232. 10.1007/BF01704707
Du Bois D, Du Bois EF: A formula to estimate the approximate surface area if height and weight be known. Arch Int Med 1916, 17: 863-871.
Damia G, Mascheroni D, Croci M, Tarenzi L: Perioperative changes in functional residual capacity in morbidly obese patients. Br J Anaesth 1988, 60: 574-578.
Polese G, Rossi A, Appendini L, Brandi G, Bates JH, Brandolese R: Partitioning of respiratory mechanics in mechanically ventilated patients. J Appl Physiol 1991, 71: 2425-2433.
Cheatham ML, Safcsak K: Intraabdominal pressure: a revised method for measurement. J Am Coll Surg 1998, 186: 594-595. 10.1016/S1072-7515(98)00122-7
Aliverti A, Dellaca R, Pelosi P, Chiumello D, Pedotti A, Gattinoni L: Optoelectronic plethysmography in intensive care patients. Am J Respir Crit Care Med 2000, 161: 1546-1552.
Aliverti A, Dellaca R, Pelosi P, Chiumello D, Gatihnoni L, Pedoti A: Compartmental analysis of breathing in the supine and prone positions by optoelectronic plethysmography. Ann Biomed Eng 2001, 29: 60-70. 10.1114/1.1332084
Valenza F, Guglielmi M, Maffioletti M, Tedesco C, Maccagni P, Fossali T, Aletti G, Porro GA, Irace M, Carlesso E, et al.: Prone position delays the progression of ventilator-induced lung injury in rats: does lung strain distribution play a role? Crit Care Med 2005, 33: 361-367. 10.1097/01.CCM.0000150660.45376.7C
McLeod AG: Principles of alternating pressure surfaces. Adv Wound Care 1997, 10: 30-36.
Kosiak M: Etiology and pathology of ischemic ulcers. Arch Phys Med Rehabil 1959, 40: 62-69.
Johannigman JA, Davis K Jr, Miller SL, Campbell RS, Luchette FA, Frame SB, Branson RD: Prone positioning for acute respiratory distress syndrome in the surgical intensive care unit: who, when, and how long? Surgery 2000, 128: 708-716. 10.1067/msy.2000.108225
Acknowledgements
The authors thank all who participated in the study and in the care of the patients enrolled. Special thanks go to Angelo Colombo MD PhD, with a degree in statistics, of the Terapia Intensiva Neuroscienze (Fondazione Ospedale Maggiore Policlinico, Mangiagalli e Regina Elena) for statistical advice, and to the nursing staff of the general Intensive Care Unit of the Fondazione Ospedale Maggiore Policlinico, Mangiagalli e Regina Elena and to all the physicians, without whom this study would not have been possible. This study received financial support from Fondazione IRCCS 'Ospedale Maggiore Policlinico, Mangiagalli e Regina Elena di Milano'.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
LG is a member of the paid KCI Advisory Board. All other authors declare that they have no competing interests.
Authors' contributions
DC conceived the study, participated in its design and coordination, performed the measurements and wrote a first draft of the manuscript. MC participated in the study design and coordination and performed the measurements. MR participated in the study design and coordination and performed the measurements. LL participated in the study design and coordination and performed the measurements. GLB participated in the study design and coordination and performed the measurements. FP performed the statistical analysis and helped draft the manuscript. EC performed the statistical analysis and helped draft the manuscript. LG conceived the study, participated in its design and coordination, coordinated the final analysis of collected data, and revised the manuscript in writing its final version. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Chiumello, D., Cressoni, M., Racagni, M. et al. Effects of thoraco-pelvic supports during prone position in patients with acute lung injury/acute respiratory distress syndrome: a physiological study. Crit Care 10, R87 (2006). https://doi.org/10.1186/cc4933
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc4933