
Abstract
Background
Delirium is a sign of deterioration in the homeostasis and physical status of the patient. The objective of our study was to investigate the predisposing factors for delirium in a surgical intensive care unit (ICU) setting.
Method
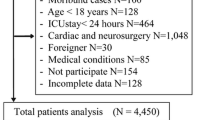
Between January 1996 and 1997, we screened prospectively 818 patients who were consecutive applicants to the general surgery service of Dicle-University Hospital and had been kept in the ICU for delirium. All patients were hospitalized either for elective or emergency services and were treated either with medication and/or surgery. Suspected cases of delirium were identified during daily interviews. The patients who had changes in the status of consciousness (n = 150) were consulted with an experienced consultation-liaison psychiatrist. The diagnosis of delirium was based on Diagnostic and Statistical Manual of Mental Disorders (revised third edition) criteria and established through psychiatric interviews. Patients were divided into two groups: the 'delirious group' (DG) (n = 90) and the 'non-delirious group' (NDG) (n = 728). During delirium, all abnormal findings related to physical conditions, laboratory features, and additional diseases were evaluated as probable risk factors of delirium.
Results
Of 818 patients, 386 (47.2%) were male and 432 (52.8%) were female. Delirium developed in 90 of 818 patients (11%). The cases of delirium in the DG were more frequent among male patients (63.3%) than female patients (36.7%) (χ2 = 10.5, P = 0.001). The mean age was 48.9 ± 18.1 and 38.5 ± 13.8 years in the DG and NDG, respectively (t = 6.4, P = 0.000). Frequency of delirium is higher in the patients admitted to the Emergency Department (χ2 = 43.6, P = 0.000). The rate of postoperative delirium was 10.9%, but there was no statistical difference related to operations between the DG and NDG (χ2 = 0.13, P = 0.71). The length of stay in the ICU was 10.7 ± 13.9 and 5.6 ± 2.9 days in the DG and NDG, respectively (t = 0.11, P = 0.000). The length of stay in hospital was 15.6 ± 16.5 and 8.1 ± 2.7 days in the DG and NDG, respectively (t = 11.08, P = 0.000). Logistic regression was used to explore the associations between probable risk factors and delirium. Delirium was not correlated with conditions such as hypertension, hypo/hyperpotassemia, hypernatremia, hypoalbuminemia, hypo/hyperglycemia, cardiac disease, emergency admission, age, length of stay in the ICU, length of stay in hospital, and gender. It was determined that conditions such as respiratory diseases (odds ratio [OR] = 30.6, 95% confidence interval [CI] = 9.5–98.4), infections (OR = 18.0, 95% CI = 3.5–90.8), fever (OR = 14.3, 95% CI = 4.1–49.3), anemia (OR = 5.4, 95% CI = 1.6–17.8), hypotension (OR = 19.8, 95% CI = 5.3–74.3), hypocalcemia (OR = 30.9, 95% CI = 5.8–163.2), hyponatremia (OR = 8.2, 95% CI = 2.5–26.4), azotemia (OR = 4.6, 95% CI = 1.4–15.6), elevated liver enzymes (OR = 6.3, 95% CI = 1.2–32.2), hyperamylasemia (OR = 43.4, 95% CI = 4.2–442.7), hyperbilirubinemia (OR = 8.7, 95% CI = 2.0–37.7) and metabolic acidosis (OR = 4.5, 95% CI = 1.1–17.7) were predicting factors for delirium.
Conclusion
We determined that conditions such as respiratory diseases, infections, fever, anemia, hypotension, hypocalcemia, hyponatremia, azotemia, elevated liver enzymes, hyperamylasemia, hyperbilirubinemia and metabolic acidosis were predicting factors for delirium.
Similar content being viewed by others


Introduction
Delirium is not a disease in itself, but a syndrome of acute cerebral inefficiency affecting the brain in various ways. It creates a deleterious effect on cognitive functions such as consciousness, orientation, perception, attention, short-term memory, judgment and abstract thinking [1,2]. Delirium is a temporary condition, which can occur suddenly or slowly over a period of hours or days. A single episode lasts up to 1 week. The symptoms may be so slight they go unnoticed or so serious they could be life threatening. The clinical signs of delirium are changeable all day, and are usually more serious during early morning or night. Temporary changes in clinical signs are important characteristics of delirium. While the patient may appear well and communicative during an observation, changes in orientation could occur a few minutes later [1,3]. Delirium is typically an indicator of a physical pathology and a worsening prognosis [1,4,5,6]. It is commonly unrecognized or misdiagnosed by physicians treating critically ill patients. The rate of misdiagnosis has been reported as 32–67% in various reviews [6,7]. Clinical evaluation is the most important criterion and electroencephalography is the most useful test for diagnosis.
Although delirium can be experienced in all age groups, it has an increased frequency at more advanced ages [2,3]. Risk factors determined for the syndrome include: age [7,8,9,10,11,12], imbalance of electrolyte [5,7,10], hypotension [1,7], hyperglycemia [1,7,8], azotemia [7,12], fever/hypothermia and infections [5,7,10,11,12,13,14,15], use of multiple drugs and withdrawal of alcohol [7,8,10,11,12,13,14,15,16], male sex [7,10], severe diseases such as cancer, cerebrovasculary or cardiopulmonary disease, malnutrition and burn [1,5,7,8,15,16,17,18], patients who have been operated on and kept in ICUs [4,10,11,12,13,14,15,16,19], and psychosocial environment [1,3,5,20]. Furthermore, subclinical cerebral damage, increased adenylate cyclase in the central nervous system, and nutritional status identified by albumin level are predisposing factors for postoperative delirium [1]. Interleukin-2, monoclonal antibodies and ifosfamide have also been suspected recently as factors [15]. The aim of the present study was to confirm and/or determine predisposing factors for delirium.
Materials and methods
Between January 1996 and 1997, we screened prospectively for delirium 818 consecutive general surgery patients at the Dicle-University Hospital. All patients, whether hospitalized for elective or emergency services, or whether treated with medication or surgery, were kept for a period of time in our ICU. Ten nurses, four physicians and four staff work daily in the ICU department. The ICU has 24 beds with continuous non-invasive monitoring and ventilators. There are windows in the bed areas of the ICU. Trained clinician-researchers carried out daily structured interviewers with the patients from admission until hospital discharge. Suspected cases of delirium were identified during the daily interview. Patients with changes in their status of consciousness (n = 150) were consulted by an experienced consultation-liaison psychiatrist (SÖ).
Delirium was defined as an organic mental disorder involving a confusional state with attention deficit, disorganized thinking and a fluctuating course and acute development. The diagnosis of delirium was based on the criteria from the Diagnostic and Statistical Manual of Mental Disorders (revised third edition) and established through a psychiatric interview (Table 1). Patients who had history of severe dementia or had abused psychoactive drugs and alcohol were excluded from our study. Delirium was diagnosed in 90 patients. Patients were divided into two groups: the DG (n = 90) and the NDG (n = 728). Analysis of whole blood count, arterial blood gases, biochemistry and urine, culture antibiograms of blood, urine or other secretions, and radiological examinations, such as chest X-ray, were performed on all delirious and non-delirious patients. All abnormal findings during delirium, related to physical conditions, laboratory features, and additional diseases, were evaluated as probable risk factors for delirium. Findings for risk factors included respiratory disease (chronic obstructive pulmonary disease, cor pulmonale, pneumothorax, hemothorax, etc.), symptomatic infection, fever (>38°C), hypotension (symptomatic, or systolic blood pressure <80 mmHg), anemia (<25% htc), hypertension (>90/160 mmHg), hypo/hyperpotassemia (<3 or >6 mEq/l), hypocalcemia (<8 mg/dl), hypo/hypernatremia (<130 and >150 mmol/l), elevated level of serum urea nitrogen (>100 mg/dl), elevated level of hepatic enzymes (high alanine aminotransferase, high aspartate aminotranferase), hyperamy-lasemia (>300 U/l), hyperbilirubinemia (>10 mg/dl total bilirubin), metabolic acidosis, hypoalbuminemia (<3 g/dl), hypo/hyperglycemia (<60 or >300 mg/dl), cardiac disease (symptomatic coronary heart disease and arrhythmias, heart failure, etc.), emergency admission status, age, length of stay in the ICU (LSICU), length of stay in hospital (LSH), and gender. Patients were grouped according to their diagnosis. The groupings included hepatobiliopancreatic diseases (HBP), fistulas, traumas, acute abdominal diseases, malignancies, ileus, and others. The patients who had delirium were treated initially for etiological diseases, but when the treatment was insufficient medication with diazepam or haloperidole was added.
Biostatistical evaluation was carried out on an IBM-compatible personal computer using SPSS 10.1 software. The Student t test for continuing variables and the chi-square test for categoric variables were used. To identify factors independently related to the development of delirium, we also performed forward stepwise (conditional) logistic regression. P < 0.05 was considered statistically significant.
Results
Of 818 patients, 386 (47.2%) were male and 432 (52.8%) were female. Delirium developed in 90 of 818 patients (11%). The cases of delirium in the DG were more frequent among male patients (63.3%) than female patients (36.7%) (χ2 = 10.5, P = 0.001). The mean age was 48.9 ± 18.1 and 38.5 ± 13.8 years in the DG and NDG consecutively (t = 6.4, P = 0.000). While 81.1% of delirious patients were admitted in an emergency state, the remaining 18.9% was admitted in elective states. Frequency of delirium was higher in the patients admitted through the Emergency Department (χ2 = 43.6, P = 0.000). The rate of postoperative delirium was 10.9%, but there were no statistical differences related to operation between the DG and NDG (χ2 = 0.13, P = 0.71) (Table 2). The LSICU was 10.7 ± 13.9 and 5.6 ± 2.9 days in the DG and NDG, respectively (t = 0.11, P = 0.000). The LSH was 15.6 ± 16.5 and 8.1 ± 2.7 days in the DG and NDG, respectively (t = 11.08, P = 0.000). Delirium was diagnosed in 12.9% of patients with HBP, in 50% of those with fistulas, in 20.8% of those exposed to trauma, in 8.2% of those with acute abdominal diseases, in 9.3% of those with malignancies, and in 18.4% of patients with ileus (Table 3). Psychomotor activity increased in 56.78% of delirious patients and decreased in 43.3%. Of delirious patients, 31.1% were treated with diazepam and 13.3% were treated with haloperidole.
Table 4 shows that the following factors were all associated with an increased risk of strongly developing delirium: respiratory diseases (OR = 30.6, 95% CI = 9.5–98.4), infections (OR = 18.0, 95% CI = 3.5–90.8), fever (OR = 14.3, 95% CI = 4.1–49.3), anemia (OR = 5.4, 95% CI = 1.6–17.8), hypotension (OR = 19.8, 95% CI = 5.3–74.3), hypocalcemia (OR = 30.9, 95% CI = 5.8–163.2), hyponatremia (OR = 8.2, 95% CI = 2.5–26.4), azotemia (OR = 4.6, 95% CI = 1.4–15.6), elevated liver enzymes (OR = 6.3, 95% CI = 1.2–32.2), hyperamylasemia (OR = 43.4, 95% CI = 4.2–442.7), hyperbilirubine-mia (OR = 8.7, 95% CI = 2.0–37.7) and metabolic acidosis (OR = 4.5, 95% CI = 1.1–17.7). Delirium was not correlated with conditions such as hypertension, hypo/hyperpotassemia, hypernatremia, hypoalbuminemia, hypo/hyperglycemia, cardiac disease, emergency admission, age, LSICU, LSH, and gender.
Discussion
Delirium, a syndrome associated with long hospital stays and high rates of morbidity and mortality [10], is a sign of deterioration in the homeostasis and physical status of the patient [17]. Approximately 10–15% of patients on general surgical wards and 15–25% of patients on general medical wards experience delirium during their hospital stay. Approximately 30% of patients in surgical ICUs and cardiac ICUs, and 40–50% of patients who are recovering from hip fractures have an episode of delirium [1,22]. The delirium rate is 10–40% in cancer patients [23], but increases to 85% in patients with advanced malignancies [15]. Delirium is seen in 18% of the patients when the ICU facility has windows, but rises to 40% of the cases when the ICU facility has no windows [11]. It has been determined that preoperative risk factors for delirium were older age [24,25,26], prior cognitive impairment [24,25], pre-existing cerebrovascular or other brain diseases, history of prior delirium [25], preoperative abnormal sodium [24], vision or hearing impairment [24,26] and regular use of psychotropic drugs before admission [24]. In this series, 11% of our patients had delirium; 34.4% (n = 31) of these were older than 60 years. The youngest patient was 15 years old, and the eldest was 91 years old. All of our patients, most of whom were younger than 60 years old, were kept in an ICU with windows. This may be responsible for the low frequency of delirium in this series. Although the age of delirious patients were higher than that of the NDG (t = 6.4, P = 0.000), age was not determined as a predicting factor for delirium (P > 0.05, in the logistic regression test) in our study. The rate of delirium has a predominance in males [10,27]. We found that the number of delirious male patients was significantly higher than female patients (χ2 = 10.5, P = 0.001), although gender was not a predictive factor for delirium (P > 0.05, in the logistic regression).
The prevalence of delirium in the Emergency Department was 9.6% [28]. In this series, the rate of delirium was 18.5% in emergency admissions, similar to Kishi's series (16%) [29], but emergency admission was not considered a factor for delirium.
The etiology of delirium is complex and usually consists of multiple factors. In 80–95% of delirious patients, the etiology is secondary to organic factors, but it is difficult to interpret further details [5,6,7]. Imbalances of electrolytes, metabolic changes, intoxication or absence of drugs, trauma of head and postoperative state are the most common etiological factors. Other less common factors are infections, intracranial lesions, coma, fever, cardiovasculary diseases, poisons, polymedication and deficiencies of vitamins [4,5,26,28,30]. Anti-cholinergic drugs are also commonly accused agents [5]. Surgical stress and infectious fever are common factors in geriatric patients [14]. Francis et al [12] reported that abnormal sodium levels, fever/hypothermia and azotemia were independent predictors for delirium in elderly patients. Foreman [31] determined that hypernatremia, hypokalemia, hyperglycemia, azotemia, hypotension and polymedication were predictors for delirium in a prospective study. Some predisposing factors determined in our study were respiratory disease (14.1%), hypotension (17%), anemia (16.4%), hyponatremia (11.7%), azotemia (10.8%), and metabolic acidosis (7.6%). The major neurotransmitter hypothesized as involved in delirium is acetylcholine, and the major neuro-anatomical area is the reticular formation [2]. Electrolyte imbalance and azotemia may be responsible for the decrease in acetylcholine activity in the brain.
Symptomatic infection and fever were other independent predictors of delirium. Delirium has been reported in infectious diseases such as diverticulitis [32], pneumonia [33] and typhoid fever [34]. Certainly, fever is concomitant with many infections and experimental data have supported a casual relation between fever and delirium. Fever and infection correlated with delirium in our study as independent predictors in the multivariate logistic regression. Cytokines and/or bacterial toxins and cerebral metabolic changes may be causes of the mental changes associated with infection.
To perform specific treatment, it is important to determine the etiological factor. Arterial blood gases and current and past vital signs should be checked to establish whether cerebral hypoxemia or hypertensive encephalopathy is present. The patient with hypoglycemic-induced delirium virtually always has a history of insulin-dependent diabetes mellitus. Hypoglycemic delirium is also hyperadrenergic. Hypotension can result from multiple etiologies, such as decreased cardiac output from a myocardial infarction, cardiac failure or arrhythmias, and anemia. All medical conditions that cause hypotension can lead to a decrease in brain oxygenation [1]. In this study, we predicted that respiratory diseases, anemia, and hypotension were effective in delirium by decreasing brain oxygenation.
Research into patients who developed hepatic failure suggests that the gamma-aminobutyric acid system is important in the development of hepatic encephalopathy (i.e. hypoactive delirium caused by liver dysfunction). Specifically, endogenous benzodiazepine-like substances may play a role in delirium associated with hepatic failure [1]. In our study, delirium was seen in 12.9% of HBP. The abnormalities, such as elevated level of hepatic enzymes, hyperbilirubinemia, hypocalcemia and hyperamylasemia associated with HBP, were strongly predictive factors for delirium. This condition showed that early intervention was important in HBP cases.
The existence of hyperactive, hypoactive, or mixed clinical subtypes of delirium is widely accepted. The hyperactive subtype was more frequent (46.5%) than the unspecified (27.3%) and hypoactive subtypes (26.2%) [35]. In a series consisting of cancer patients, it was observed that the hyperactive type (which has a shorter duration) is the most commonly seen subtype of delirium, with a rate of 71% [36]. In our study, 56.7% of delirious patients had hyperactive subtype.
There is no specific drug used for management of delirium. The first step of treatment is trying to calm down the patient and to identify the underlying cause [1,3,13]. The second step is treating the causative factors, when determinable. If causative factors are undeterminable, then efforts should be directed to preventing permanent damage [1,3]. Butyrophenones (haloperidole, thiothixene and droperidole), and benzodiazepins (diazepam, oksazepam and lorazepam) are the recommended drugs for sedation and preventing agitation [16,37,38]. In this series, we treated the etiological factors in all patients and gave diazepam to 31.1% of the patients and haloperidole to 13.3% of the patients.
Both surgeons and anesthesiologists could reduce the incidence of delirium in the patients who are at high risk by carefully ordering and monitoring the dosages of drugs, and watching for signs of cardiac ischemia during the perioperative period [8,10].
The practice of polymedication should not be given up [8,30]. The goal in diagnosis is to discover reversible causes for delirium. In this study series, we determined that conditions such as disease or symptom variables (respiratory diseases, symptomatic infections, fever, anemia, hypotension) and laboratory variables (hypocalcemia, hyponatremia, azotemia, elevated liver enzymes, hyperamylasemia, hyperbilirubinemia, and metabolic acidosis) were predicting factors for delirium. Clinicians must identify specific etiologies when possible and apply appropriate treatment.
Abbreviations
- CI:
-
CI = confidence interval
- DG:
-
DG = delirious group
- HBP:
-
HBP = hepatobiliopancreatic diseases
- ICU:
-
ICU = intensive care unit
- LSH:
-
LSH = length of stay in hospital
- LSICU:
-
LSICU = length of stay in the ICU
- NDG:
-
NDG = non-delirious group
- OR:
-
OR = odds ratio.
References
Wise MG: Delirium. In American Psychiatric Press Textbook of Neuropsychiatry. Edited by Hales RE, Yudofsky SC. Washington, DC: American Psychiatric Press; 1987, 89-105.
Kaplan HI, Sadock BJ: Synopsis of Psychiatry, 8th edn. Baltimore, USA: Lippincott Williams & Wilkins; 1998.
Lipowski JZ: Delirium (Acute confusional states). JAMA 1987, 258: 1789-1792. 10.1001/jama.258.13.1789
Haller E, Binder R: Delirium, dementia, amnestic disorders. In:Review of General Psychiatry, 4th edn. Edited by Goldman HH. London:Appleton & Lange; 1992, 176-181.
Lipowski ZJ: Transient cognitive disorders (Delirium, acute confusional states) in the elderly. Am J Psychiatry 1983, 140: 1426-1436.
Dubos G, Gonthier R, Simeone I, Camus V, Schwed P, Cadec B, Diana MC, Burtin B, Melac M: Confusion syndromes in hospitalized aged patients: polymorphism of symptoms and course. Prospective study of 183 patients. Rev Med Interne 1996, 17: 979-986. 10.1016/S0248-8663(97)80841-7
Inouye SK: The dilemma of delirium: Clinical and research controversies regarding diagnosis and evaluation of delirium in hospitalized elderly medical patients. Am J Med 1994, 97: 278-288.
Marcantonio ER, Goldman L, Mangione CM, Ludwing LE, Muraca B, Haslauer CM, Donaldson MC, Whittemore AD, Sugarbaker DJ, Poss R: A clinical prediction rule for delirium after elective noncardiac surgery. JAMA 1994, 271: 134-139. 10.1001/jama.271.2.134
Radanov BP, Basetti C: Delirium: occurrence, diagnosis and therapy. Schweiz Rundsch Med Prax 1995, 84: 1335-1341.
Schor JD, Levkoff SE, Lipsitz LA, Reilly CH, Cleary PD, Rowe JW, Evans DA: Risk factors for delirium in hospitalized elderly. JAMA 1992, 267: 827-831. 10.1001/jama.267.6.827
Wilson LM: Intensive Care Delirium: The effect of outside deprivation in a windowless unit. Arch Intern Med 1972, 130: 225-226. 10.1001/archinte.130.2.225
Francis J, Martin D, Kapoor WN: A prospective study of delirium in hospitalized elderly. JAMA 1990, 263: 1097-1101. 10.1001/jama.263.8.1097
Hege SG: Postoperative transitory syndrome and delirium. Anesthetist 1989, 9: 443-451.
Lazaro L, Marcos T, Cirera E, Pujol J: Delirium in an elderly population admitted at a general hospital. Med Clin Barc 1995, 104: 329-333.
Zimberg M, Berenson S: Delirium in patients with cancer: Nursing assessment and intervention. Oncol Nurs Forum 1990, 17: 529-538.
Fish DN: Treatment of delirium in the critically ill patient. Clin Pharm 1991, 10: 456-466.
Özkan S: Psychiatric Medicine: Consultation-Liaison Psychiatry [in Turkish], 1st edn. Istanbul: Roche Publications; 1993.
Stiefel F, Razavi D: Common psychiatric disorders in cancer patients. II. Anxiety and acute confusional states. Support Care Cancer 1994, 2: 233-237.
Hayashi H, Maeda Y, Morichika H, Miyama T, Suzuki T: Surgical stress and transient postoperative psychiatric disturbances in aged patients studied using the Yamaguchi University Mental Disorder Scale. Surg Today 1996, 26: 413-418.
Rabins PV: Psychosocial and management aspect of delirium. Int Psychogeriatr 1991, 3: 319-324.
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 3rd edn rev. Washington, DC: American Psychiatric Association; 1987, 97-124.
Dubin WR, Field NL, Gastfriend DR: Postcardiotomy delirium: a critical review. J Thorac Cardiovasc Surg 1979, 77: 5865-5894.
Massie MJ, Holland J, Glass E: Delirium in terminally ill cancer patients. Am J Psychiatry 1983, 140: 1048-1050.
Galanakis P, Bickel H, Gradinger R, Von Gumppenberg S, Forstl H: Acute confusional state in the elderly following hip surgery: incidence, risk factors and complications. Int J Geriatr Psychiatry 2001, 16: 349-355. 10.1002/gps.327
Litaker D, Locala J, Franco K, Bronson DL, Tannous Z: Preoperative risk factors for postoperative delirium. Gen Hosp Psychiatry 2001, 23: 84-89. 10.1016/S0163-8343(01)00117-7
Gallinat J, Moller H, Moser RL, Hegerl U: Postoperative delirium: risk factors, prophylaxis and treatment. Anaesthesist 1999, 48: 507-518. 10.1007/s001010050741
Millar HR: Psychiatric morbidity in elderly surgical patients. Br J Psychiatry 1981, 138: 17-20.
Elie M, Rousseau F, Cole M, Primeau F, McCusker J, Bellavance F: Prevalence and detection of delirium in elderly emergency department patients. CMAJ 2000, 163: 977-981.
Kishi Y, Iwasaki Y, Takezawa K, Kurosawa H, Endo S: Delirium in critical care unit patients admitted through an emergency room. Gen Hosp Psychiatry 1995, 17: 371-379. 10.1016/0163-8343(95)00056-W
Geary SM: Intensive care unit psychosis revisited: Understanding and managing delirium in the critical care setting. Crit Care Nurs Q 1994, 17: 51-63.
Foreman MD: Confusion in the hospitalized elderly: incidence, onset, and associated factors. Res Nurs Health 1989, 12: 21-29.
Normal DC, Yoshikawa TT: Intraabdominal infections in the elderly. J Am Geriatr Soc 1983, 31: 677-684.
Verghese A, Berk SL: Bacterial pneumonia in the elderly. Medicine 1983, 62: 271-285.
Verghese A: The "typhoid state" revisited. Am J Med 1985, 79: 370-372.
Camus V, Gonthier R, Dubos G, Schwed P, Simeone I: Etiologic and outcome profiles in hypoactive and hyperactive subtypes of delirium. J Geriatr Psychiatry Neurol 2000, 13: 38-42.
Olofsson SM, Weitzner MA, Walentine AD, Baile WF, Meyers CA: A retrospective study of the psychiatric management and outcome of delirium in the cancer patient. Support Care Cancer 1996, 4: 351-357.
Berger I, Waldhorn RE: Analgesia, sedation and paralysis in the intensive care unit. Am Family Physician 1995, 51: 166-172.
Seneff MG, Mathews RA: Use of haloperidole infusions to control delirium in critically ill adults. Ann Pharmacother 1995, 29: 690-693.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Rights and permissions
About this article
Cite this article
Aldemir, M., Özen, S., Kara, I.H. et al. Predisposing factors for delirium in the surgical intensive care unit. Crit Care 5, 265 (2001). https://doi.org/10.1186/cc1044
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc1044