
Abstract
Scleroderma (systemic sclerosis; SSc) is characterised by fibrosis of the skin and internal organs in the context of autoimmunity and vascular perturbation. Overproduction of extracellular matrix components and loss of specialised epithelial structures are analogous to the process of scar formation after tissue injury. Fibroblasts are the resident cells of connective tissue that become activated at sites of damage and are likely to be important effector cells in SSc. Differentiation into myofibroblasts is a hallmark process, although the mechanisms and cellular origins of this important fibroblastic cell are still unclear. This article reviews fibroblast biology in the context of SSc and highlights the potentially important place of fibroblast effector cells in fibrosis. Moreover, the heterogeneity of fibroblast properties, multiplicity of regulatory pathways and diversity of origin for myofibroblasts may underpin clinical diversity in SSc, and provide novel avenues for targeted therapy.
Similar content being viewed by others


Diversity of clinical phenotype in scleroderma
Scleroderma (also termed systemic sclerosis; SSc) is an autoimmune rheumatic disease of unknown aetiology that is characterised by pathological remodelling of connective tissues. Although often regarded as a prototypic fibrotic disease, SSc is as much characterised by vasculopathy and by atrophic changes as well as scarring and fibrosis, although the latter is a universal feature of organ-based pathology. The most visible manifestation of SSc is pathological changes in the skin; however, many of the visceral organs may be affected [1]. Clinically, SSc is heterogeneous and is grouped based on the pattern and extent of skin involvement. In limited cutaneous SSc, fibrosis is mainly present in the hands, arms and face, whereas in diffuse cutaneous SSc (dcSSc), the disease progresses more rapidly and affects the trunk and extremities [2]. Studies suggest that the extent and pattern of change in skin sclerosis, especially in dcSSc, reflects the severity and frequency of significant internal organ complications and impacts on survival and other important long-term disease outcomes. However, the relationship is complex and underscores the clinical heterogeneity of SSc [3]. Auto-antibodies are important diagnostic tools that also provide information about clinical risks of specific complications, such as lung fibrosis or SSc renal crisis [4]. Some reports support a functional role of anti-nuclear antibodies (ANAs) in the pathological development of SSc, including recent data suggesting antibodies against vascular receptors specific for endothelin or angiotensin II may associate with more progressive forms of SSc [3]. Intriguingly the agonist effects of auto-anti-platelet-derived growth factor receptor antibodies in modulating fibroblast intracellular signalling have been reported [5], although these studies have not been consistently repeated [6].
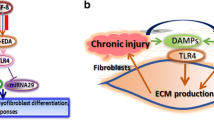
The pathophysiology of SSc includes vascular injury and inflammation, and culminates in fibrosis. The disruption of the affected tissue's architecture due to fibrosis is orchestrated by the fibroblasts' excessive synthesis and deposition of extracellular matrix (ECM) proteins, including collagen type I [7]. Central to the development and progression of fibrosis is the activation of resident fibroblasts. Fibrosis, like wound healing, is instigated by fibroblast activation, proliferation and migration of these cells into the site of trauma and deposition of matrix proteins such as fibronectin and collagen [8]. In wounds, the activated fibroblasts or myofibroblasts are lost, although the mechanism(s) by which these cells are cleared from the site of trauma remain contentious and may include apoptosis as well as de-activation. In fibrotic pathologies like SSc, however, these cells persist and promote a pro-fibrotic micro environment rich in ECM and growth factors, such as fibroblast growth factor (FGF) and connective tissue growth factor (CTGF; CCN2).
Fibroblast biology and scleroderma
The connective tissue confers a structural scaffold that facilitates organ function. Composed of ECM, the most common cell found in the connective tissues are spindle-shaped cells termed 'fibroblasts'. These cells, which express vimentin but not desmin or alpha smooth muscle actin (α-SMA), are found in the majority of organs and are essential for connective tissue homeostasis [5]. An imbalance in the deposition of ECM proteins, including collagen type I and III, leads to the pathological changes observed in SSc. Fibroblasts are highly active cells and each cell synthesises approximately 3.5 million pro-collagen molecules per day [6]. Fibroblasts regulate matrix turnover through the expression of matrix metalloproteinases (MMPs), which degrade ECM, and their inhibitors, tissue inhibitors of metalloproteinases (TIMPs). Consistent with increased ECM deposition in SSc patients, serum levels of TIMPs in dcSSc and limited cutaneous SSc are significantly raised compared to healthy controls. This supports the hypothesis that fibroblast-regulated matrix accumulation occurs through an imbalance in turnover of the ECM and this plays a pivotal role in SSc [9].
Fibroblasts are the key contributors to fibrosis in patients with SSc. In healthy individuals fibroblasts are protected from stress by the surrounding ECM, but during connective tissue diseases the damaged fibroblasts are no longer protected, causing the fibroblasts to attach to the ECM [10]. Upon tissue injury, fibroblasts migrate towards the wound and due to the presence of growth factors released by immune and blood cells differentiate into secretory myofibroblasts that are involved in repair during wound healing.
Myofibroblasts
In response to tissue injury, mesenchymal cells of fibroblastic lineage accumulate at the wound site and deposit and remodel new ECM and contract the wound site. The main fibroblastic cells responsible for this process are termed myofibroblasts and exhibit specific markers and phenotypic properties that are suited to this role. Normally as wounds repair and resolve myofibroblasts are lost from the site of injury, whereas in fibrotic pathologies such as SSc they remain [11, 12]. The persistence and accumulation of a large number of myofibroblasts in connective tissues is responsible for the exaggerated and uncontrolled production of ECM during the development and progression of fibrotic pathologies such as SSc [5, 12]. Myofibroblasts can arise from resident fibroblasts in a process termed fibroblast to myofibroblast transition. Unlike fibroblasts, myofibroblasts express the contractile protein α-SMA [5]. More recently, it has become recognised that myofibroblasts can arise from different cellular sources, including pericytes and smooth muscle and epithelial cells (Figure 1), via a number of biological processes that we address elsewhere in this review.

The cellular origins of pathogenic 'activated' fibroblasts in scleroderma. Scleroderma (SSc) fibrosis is characterised by the excessive accumulation of extracellular matrix (ECM) proteins, including type I and type III collagen, by 'activated fibroblasts' or myofibroblasts and leads to the development of pathological scaring and loss of organ function. These cells arise from a differentiation of resident and recruited circulating progenitor cells and collectively are likely to contribute the myofibroblast population. Myofibroblasts have been shown to arise from a number of cellular sources through the differentiation and activation of tissue-resident cells: epithelial to mesenchymal transition; endothelial to mesenchymal transition; fibroblast to myofibroblast transition; pericyte to mesenchymal transition; smooth muscle cell differentiation. In addition the recruitment and differentiation of circulating bone marrow-derived cells (BMDC) and fibrocytes can contribute to the myofibroblast population. SSc fibroblasts also promote a pro-fibrotic microenvironment, secreting growth factors, chemokines and cytokines that can in turn act on resident and infiltrating cells in an autocrine and paracrine manner to expand the reservoir of pro-fibrotic fibroblasts present in SSc fibrotic lesions.
Histological analysis of SSc skin has shown an abundance of myofibroblasts involved in lesional skin and fibrotic areas of the visceral organs from SSc patients [5, 13]. Consistent with the presence of myofibroblasts in SSc and wounding, gene expression profiling studies demonstrate a number of genes differentially regulated in wound healing fibroblasts and those derived from fibrotic regions of SSc patients [14]. Comprehensive transcriptional analysis of skin biopsies has demonstrated systematic differences in the gene expression profile of dermal fibroblasts from SSc patients into subsets including inflammatory and transforming growth factor (TGF)-β gene signatures [15, 16]. The different gene expression profiles exhibited by fibroblasts from SSc patients may reflect the diverse origins of the cells that contribute to the formation of myofibroblasts. It remains unclear if SSc fibroblasts arising from these diverse cellular pools will respond to similar therapeutic interventions, and future studies will be needed to explore the relevance to the pathological development of fibrosis in SSc patients.
Positional identity of fibroblasts - relevance to SSc
Fibroblasts isolated from different tissues display similar morphology but exhibit diverse functional properties. For example, the capacity of fibroblasts from different anatomical sites to migrate or express extracellular matrix proteins varies [17]. These differences are consistent with the wide variety of biological and physical environments these cells are found in. The 'positional memory' of fibroblasts was elegantly highlighted by Chang and colleagues [18] in gene expression profiling studies of fibroblasts from a variety of anatomical sites in the adult and foetus. A striking feature in this study was the distinct and characteristic transcriptional patterns displayed by fibroblasts, including genes associated with lipid metabolism, the TGFβ and Wnt cell signaling pathways, and fate determination [18]. This study high-lighted the context-dependent activity of fibroblasts to generate appropriate extracellular microenvironments. For example, foetal lung and skin fibroblasts expressed high levels of the basement membrane protein type IV collagen in the skin and lung alveoli. In contrast, skin but not lung fibroblasts expressed significant levels of type I and V collagen, which confers the tensile strength in the dermis [18]. Consistent with the different anatomical environ mental requirements of organs, fibroblasts exhibit distinct immune-modulatory effects on leukocytes, including recruitment [17]. The mechanism(s) by which fibroblasts acquire their positional identity remain unclear; however, it is likely epigenetic mechanisms play a significant role. It remains to be investigated if SSc fibroblasts lose their positional identity and this in turn promotes the development of a pro-fibrotic environment. It is plausible that location-specific signatures for fibro blasts and other cell types explain the diverse patterns of fibrosis between and within different subsets of SSc.
Origin of fibroblasts in SSc: resident cells, trans-differentiation, and circulating fibrocytes
The origin of activated fibroblasts or myofibroblasts in fibrotic tissues was until comparatively recently believed to result from the expansion and activation of resident fibroblasts. However, recent studies have highlighted the potential for other tissue-resident and blood-borne cells to contribute to the pool of myofibroblasts (Figure 1) that arise in fibrotic tissues [19–21]. A number of tissue-resident cells, including endothelial, epithelial and smooth muscle cells, can differentiate into fibroblastic-like cells [19, 20, 22, 23]. In addition to tissue-resident cells, blood-borne cells such as fibrocytes also contribute to the heterogeneity of these myofibroblasts [24].
The differentiation of resident cells has been proposed as an important mechanism contributing to the development of tissue fibrosis in SSc (Figure 1). For example, endothelial to mesenchymal transition (EndoMT) was thought to be a rare phenomenon confined to embryonic development; however, Arciniegas and colleagues [20] elegantly demonstrated the capacity of adult endothelial cells to lose vascular markers such as E-cadherin and acquire myofibroblast markers, including α-SMA and type I collagen. Consistent with a putative pathological role of EndoMT in SSc, lung capillary endothelial cells can contribute to the pool of myofibroblasts/fibroblasts present in the bleomycin model of pulmonary SSc [19]. Like EndoMT, epithelial cells in a process termed epithelial to mesenchymal transition (EMT) are induced by TGF-β to take on fibroblast-like features [19].
EMT has been linked to cellular differentiation and tumour invasion for a number of years [14]. More recently, EMT has become strongly associated with renal and pulmonary fibrosis in pre-clinical models [25]; however, the contribution of EMT in the development of fibrotic pathologies, including SSc, remains contentious. During EMT, epithelial cells down-regulate epithelial markers such as E-cadherin and acquire mesenchymal/myofibroblast markers, including α-SMA [5, 21]. EMT, like EndoMT, is likely to lead to a significant loss of the functional capacity of these cells to act as biological barriers and contribute further to the development of fibrosis. The importance of barrier loss in the development and progression of SSc, as well as the therapeutic benefit of restoring barrier function, remain to be explored. EMT can be induced by a number of secreted factors, including TGF-β, CTGF and FGF-2, all of which have been implicated in SSc [26]. Studies from our own group have further highlighted a cellular link between microvascular damage and fibrosis via pericyte trans-differentiating into myofibroblasts (pericyte to mesenchymal transition (PeMT)) [27, 28]. The presence of activated pericytes in dcSSc skin and the capability of these cells to transition into myofibroblasts when activated further support their likely contribution to dermal fibrosis in SSc. Interestingly, elegant genetic ablation studies targeting ADAM12 support a role of PeMT during tissue injury. These studies demonstrated that the loss of perivascular ADAM12-positive cells led to a marked loss of pro-fibrotic collagen-producing cells during injury. Work from our own group has shown ADAM12 to be elevated in lung fibroblasts from SSc patients, supporting the possible contribution of PeMT in the development of SSc [29].
In addition to local precursors, circulating cells are also able to contribute to the myofibroblasts that populate fibrotic tissues (Figure 1). Fibrocytes were initially described in the early 1990s as blood-borne collagen-producing cells with antigen-presenting capability [30]. Since then, they have been associated with a broad range of fibrosing disorders, including SSc, sickle cell lung disease, asthma, pulmonary hypertension and atherosclerosis [31–35]. Although the cell surface markers that identify fibrocytes remains ambiguous, it is widely accepted that these cells share immune and mesenchymal cell surface markers [36] and migrate to sites of tissue injury [37]. The pre-clinical bleomycin insult model, which serves as a model of SSc fibrosis, exhibits enhanced fibrocyte recruitment in the dermis and lung, supporting the notion that fibrocytes play a key role in SSc [25, 32]. Previous studies have demonstrated that mice dosed with adenosine A2A antagonists were protected from developing bleomycin-induced lung fibrosis [38]. The use of these A2A antagonists also halted lung fibrocyte recruitment, suggesting that these receptors must be involved in fibrocyte recruitment and supporting the contribution of fibrocytes in the development of pulmonary fibrosis [32]. Consistent with fibrocyte recruitment to sites of tissue injury, these cells express a number of chemokine receptors, including chemokine receptor type 4 (CXCR4). Analysis of SSc patients demonstrated the presence of CXCR4+/collagen type I+ cells only in SSc interstitial lung disease patients. Further, the expression of CXCR4 and its ligand, stromal cell-derived factor 1 (CXCL12), was also highly upregulated in SSc lung compared to healthy controls [27]. The SSc lungs that overexpress CXCR4 also lack caveolin 1, and show enhanced monocyte migration compared to controls. In the bleomycin-induced fibrosis model, the use of caveolin scaffolding domain (CSD) diminishes fibrocyte accumulation in the lung and may represent a novel therapy in SSc [34].
The cellular origin of the mesenchymal cells that contribute to the excessive accumulation of ECM and loss of tissue architecture in SSc fibrosis remains unclear. Indeed, the reported contributions through the cellular processes that give rise to these cells, including expansion of resident tissue fibroblasts, EMT, fibroblast to myofibroblast transition and accumulation of bone marrow-derived and circulating fibrocytes, may vary in an organ-specific manner (Figure 1). Future studies will be required to assess the relative contribution and therapeutic relevance in SSc.
Fibroblast-dependent dysregulated connective tissue repair - unification of the pathogenic pathway in SSc
There are a number of established pre-clinical models of SSc and these continue to be the models of choice in SSc research (Table 1). Established models include the bleomycin-induced fibrotic model and tight skin mouse (tsk). More recently, transgenic models (Table 1) have facilitated research into fibroblastic mechanisms that drive fibrosis. An example of such a transgenic model is the TβRICA; Cre-ER transgenic mouse expressing constitutively active TβRI in fibroblasts. Postnatal expression of this activated receptor in mice leads to many of the clinical, histological and biochemical features seen in SSc patients. In the TβRICA; Cre-ER mouse, fibrosis of the dermis, thinner epidermis, loss of hair follicles and fibrotic thickening of small blood vessels in the lung and kidney are all evident [39]. Further, fibro blasts isolated from the skin exhibit increased expression of downstream TGF-β target genes and resemble that seen in SSc patients. These fibroblasts also showed increased expression of plasminogen activator, elevated Smad2/3 phosphorylation and enhanced myofibroblast differentiation [39]. This model of SSc is an example of the advantage of transgenic models and would be suitable for therapies aimed at alleviating enhanced TGF-β signalling in SSc and fibrosis.
Another example of a transgenic mouse model is the TβRIIΔk-fib model. This model possesses a kinase deficient TβRII gene in fibroblasts leading to receptor expression-dependent balanced upregulation of TGF-β signalling. The mechanism of this model is validated in the human disease Loeys-Dietz syndrome where patients have mutations in the TβRII gene leading to increased expression of both collagen and CTGF, as well as increased pSmad2 in the nuclei, which indicates increased TGF-β signalling [40]. There is an increase in latent TGF-β in the ECM and they all have a fibrotic phenotype with dermal fibrosis. Twenty-five percent of these mice spontaneously develop lung fibrosis, which again recapitulates the disease of SSc. The intratracheal administration of bleomycin to these transgenic mice resulted in an increase in fibroblast proliferation, an increase in myofibro blasts and an increase in type II alveolar epithelial cell apoptosis [41]. In the TβRIIΔk-fib model the transgenic fibroblasts are shown to proliferate more rapidly than wild-type cells, and exhibit an increase in TGF-β markers, including CTGF [42]. Interestingly, the mice also develop vasculopathy, which is a key feature in SSc that can lead to important clinical complications, including SSc renal crisis and pulmonary arterial hypertension [43]. The development of diverse relevant pathology together with altered tissue injury response in multiple cell types provides strong support for a central role of fibroblasts in determining susceptibility to organ-based complications in SSc. This is consistent with a working hypothesis of 'fibroblast-dependent dysregulated connective tissue repair' as a unifying feature of SSc. As well as providing insight into potential pathogenic mechanisms in human disease, the studies outlined above also support fibroblastic cells as logical targets for disease-modifying therapy in SSc.
Recent studies by Wei and colleagues [44] demonstrated elevated Wnt-10b expression in the skin of SSc patients. Consistent with a role for the wnt signalling path way in fibrosis, this study demonstrated that Wnt-10b overexpression in transgenic animals led to enhanced Wnt signalling, skin thickening and expression of pro-fibrotic genes, including those encoding type I collagen and CTGF. Interestingly, these animals did not exhibit activation of the canonical TGF-β signalling pathway involving Smad2, suggesting the fibrogenic effects of this model are not directly mediated through induction of endogenous TGF-β [44]. However, the interplay between TGF-β and Wnt-regulated pathways may be complex as other studies in human fibroblast cultures have suggested that TGF-β signalling can activate canonical Wnt signalling and a broader potential role for morphogens in SSc pathogenesis is possible, as discussed below [45]. Collectively, the transgenic models of SSc highlighted in Table 1 suggest that alterations in a number of pathways can ultimately lead to the development of SSclike tissue fibrosis. Understanding the contribution of these pathways in promoting the forma tion of activated fibroblasts in SSc from different cellular pools that give rise to activated fibroblasts remains a key issue and will be of significant importance for future therapies.
Shifting the paradigm - novel fibroblast-activated signalling pathways
Recent integration of novel in vitro and in vivo approaches have led to the emergence of a number of novel molecules and signalling pathways in SSc, which has helped to elucidate the complex cellular and molecular mechanisms implicated in this fibrotic disease. For example, the family of transcription factor activator protein 1 (AP-1) has also been shown to be activated in SSc; recent studies have shown members of this family of transcription factors to be up-regulated in SSc, including c-jun and c-fos in skin and dermal fibroblasts of SSc [46], and Fra-2 [47]. Further studies have implicated the hedgehog morphogen, first discovered in the 1980s [48]. Sonic hedgehog (SHH), one of the three hedgehog proteins, was shown to be elevated in skin fibroblasts, endothelial cells and keratinocytes in SSc patients. It was also shown to induce myofibroblast differentiation, suggesting that excessive activation of this pathway in SSc promotes a pro-fibrotic cascade [49]. Inhibition of the hedgehog pathway exhibited potent anti-fibrotic effects in a model of SSc [50], suggesting that targeting this pathway could provide a novel therapeutic strategy in SSc. The Wnt signalling pathway has also become an area of interest in SSc and recent genome studies have shown an increase in expression of the Wnt receptor FZD2 and decreased expression of the Wnt antagonists DKK2 and WIF1 in skin from dcSSc patients. Activation of this pathway also stimulated an increase in fibroblast migration and proliferation, suggesting it plays an important role in SSc [51].
Conclusion
Significant advances in recent years have led to an appreciation that cells from a variety of origins can assume fibroblastic characteristics under pathological situations [19–22]. The default plasticity of cells to become fibroblasts and thus contribute to the reservoir of disease-causing myofibroblasts in SSc may in part explain the apparent heterogeneity in the disease. The capacity of SSc fibroblasts to promote the recruitment and differentiation of these cells to become pathological is actively being investigated. A key question, however, is whether SSc fibroblasts derived from different cellular origins affect the progression of fibrosis in SSc or leads to differences in the disease mediators that future therapeutics will seek to target. Future studies to define the interplay of fibroblast populations derived from different cellular origins in SSc will be crucial in our understanding of how best to develop and treat SSc. In conclusion, emerging data further support a key role for pathways that are central to normal growth and development in regulating abnormal fibroblast properties in acquired disease and fibrosis. These pathways, of the fibroblasts themselves, may ultimately provide therapeutic strategies for SSc that have a more direct anti-fibrotic effect than current treatments that target vasculopathy or the immune system.
Abbreviations
- α-SMA:
-
alpha smooth muscle actin
- CTGF:
-
connective tissue growth factor
- dcSSc:
-
diffuse cutaneous SSc
- ECM:
-
extracellular matrix
- EMT:
-
epithelial to mesenchymal transition
- EndoMT:
-
endothelial to mesenchymal transition
- FGF:
-
fibroblast growth factor
- PeMT:
-
pericyte to mesenchymal transition
- SSc:
-
systemic sclerosis (scleroderma).
References
Gabrielli A, Svegliati S, Moroncini G, Amico D: New insights into the role of oxidative stress in scleroderma fibrosis. Open Rheumatol J. 2012, 6: 87-95. 10.2174/1874312901206010087.
Gabrielli A, Avvedimento EV, Krieg T: Scleroderma. N Engl J Med. 2009, 360: 1989-2003. 10.1056/NEJMra0806188.
Riemekasten G, Philippe A, Näther M, Slowinski T, Müller DN, Heidecke H, Matucci-Cerinic M, Czirják L, Lukitsch I, Becker M, Kill A, van Laar JM, Catar R, Luft FC, Burmester GR, Hegner B, Dragun D: Involvement of functional autoantibodies against vascular receptors in systemic sclerosis. Ann Rheum Dis. 2011, 70: 530-536. 10.1136/ard.2010.135772.
Cepeda EJ, Reveille JD: Autoantibodies in systemic sclerosis and fibrosing syndromes: clinical indications and relevance. Curr Opin Rheumatol. 2004, 16: 723-732. 10.1097/01.bor.0000144760.37777.fa.
Hinz B, Phan SH, Thannickal VJ, Galli A, Bochaton-Piallat ML, Gabbiani G: The myofibroblast: one function, multiple origins. Am J Pathol. 2007, 170: 1807-1816. 10.2353/ajpath.2007.070112.
McAnulty RJ, Campa JS, Cambrey AD, Laurent GJ: The effect of transforming growth factor beta on rates of procollagen synthesis and degradation in vitro. Biochim Biophys Acta. 1991, 1091: 231-235. 10.1016/0167-4889(91)90066-7.
Denton CP, Black CM, Abraham DJ: Mechanisms and consequences of fibrosis in systemic sclerosis. Nat Clin Practice Rheumatol. 2006, 2: 134-144.
Leask A, Abraham DJ: TGFβ signaling and the fibrotic response. FASEB J. 2004, 18: 816-827. 10.1096/fj.03-1273rev.
Young-Min SA, Beeton C, Laughton R, Plumpton T, Bartram S, Murphy G, Black C, Cawston TE: Serum TIMP-1, TIMP-2, and MMP-1 in patients with systemic sclerosis, primary Raynaud's phenomenon, and in normal controls. Ann Rheum Dis. 2001, 60: 846-851.
Leask A: Getting out of a sticky situation: targeting the myofibroblast in scleroderma. Open Rheumatol J. 2012, 6: 163-169. 10.2174/1874312901206010163.
Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C, Brown RA: Myofibroblasts and mechano-regulation of connective tissue remodelling. Nat Rev Mol Cell Biol. 2002, 3: 349-363. 10.1038/nrm809.
Shi-Wen X, Thompson K, Khan K, Liu S, Murphy-Marshman H, Baron M, Denton CP, Leask A, Abraham DJ: Focal adhesion kinase and reactive oxygen species contribute to the persistent fibrotic phenotype of lesional scleroderma fibroblasts. Rheumatology. 2012, 51: 2146-2154. 10.1093/rheumatology/kes234.
Chen Y, Shi-Wen X, van Beek J, Kennedy L, McLeod M, Renzoni EA, Bou-Gharios G, Wilcox-Adelman S, Goetinck PF, Eastwood M, Black CM, Abraham DJ, Leask A: Matrix contraction by dermal fibroblasts requires transforming growth factor-beta/activin-linked kinase 5, heparan sulfate-containing proteoglycans, and MEK/ERK: insights into pathological scarring in chronic fibrotic disease. Am J Pathol. 2005, 167: 1699-1711. 10.1016/S0002-9440(10)61252-7.
Whitfield ML, Finlay DR, Murray JI, Troyanskaya OG, Chi JT, Pergamenschikov A, McCalmont TH, Brown PO, Botstein D, Connolly MK: Systemic and cell type-specific gene expression patterns in scleroderma skin. Proc Natl Acad Sci USA. 2003, 100: 12319-12324. 10.1073/pnas.1635114100.
Sargent JL, Milano A, Bhattacharyya S, Varga J, Connolly MK, Chang HY, Whitfield ML: A TGFbeta-responsive gene signature is associated with a subset of diffuse scleroderma with increased disease severity. J Invest Dermatol. 2010, 130: 694-705. 10.1038/jid.2009.318.
Greenblatt MB, Sargent JL, Farina G, Tsang K, Lafyatis R, Glimcher LH, Whitfield ML, Aliprantis AO: Interspecies comparison of human and murine scleroderma reveals IL-13 and CCL2 as disease subset-specific targets. Am J Pathol. 2012, 180: 1080-1094. 10.1016/j.ajpath.2011.11.024.
Parsonage G, Filer AD, Haworth O, Nash GB, Rainger GE, Salmon M, Buckley CD: A stromal address code defined by fibroblasts. Trends Immunol. 2005, 26: 150-156. 10.1016/j.it.2004.11.014.
Chang HY, Chi JT, Dudoit S, Bondre C, van de Rijn M, Botstein D, Brown PO: Diversity, topographic differentiation, and positional memory in human fibroblasts. Proc Natl Acad Sci USA. 2002, 99: 12877-12882. 10.1073/pnas.162488599.
Hashimoto N, Phan SH, Imaizumi K, Matsuo M, Nakashima H, Kawabe T, Shimokata K, Hasegawa Y: Endothelial-mesenchymal transition in bleomycin-induced pulmonary fibrosis. Am J Respir Cell Mol Biol. 2010, 43: 161-172. 10.1165/rcmb.2009-0031OC.
Arciniegas E, Neves CY, Carrillo LM, Zambrano EA, Ramirez R: Endothelial-mesenchymal transition occurs during embryonic pulmonary artery development. Endothelium. 2005, 12: 193-200. 10.1080/10623320500227283.
Willis BC, Borok Z: TGF-beta-induced EMT: mechanisms and implications for fibrotic lung disease. Am J Physiol Lung Cell Mol Physiol. 2007, 293: L525-534. 10.1152/ajplung.00163.2007.
Frid MG, Kale VA, Stenmark KR: Mature vascular endothelium can give rise to smooth muscle cells via endothelial-mesenchymal transdifferentiation: in vitro analysis. Circ Res. 2002, 90: 1189-1196. 10.1161/01.RES.0000021432.70309.28.
Kalluri R: EMT: when epithelial cells decide to become mesenchymal-like cells. J Clin Invest. 2009, 119: 1417-1419. 10.1172/JCI39675.
Phillips RJ, Burdick MD, Hong K, Lutz MA, Murray LA, Xue YY, Belperio JA, Keane MP, Strieter RM: Circulating fibrocytes traffic to the lungs in response to CXCL12 and mediate fibrosis. J Clin Invest. 2004, 114: 438-446.
Hoyles RK, Derrett-Smith EC, Khan K, Shiwen X, Howat SL, Wells AU, Abraham DJ, Denton CP: An essential role for resident fibroblasts in experimental lung fibrosis is defined by lineage-specific deletion of high-affinity type II transforming growth factor beta receptor. Am J Respir Crit Care Med. 2011, 183: 249-261. 10.1164/rccm.201002-0279OC.
Budd DC, Holmes AM: Targeting TGFbeta superfamily ligand accessory proteins as novel therapeutics for chronic lung disorders. Pharmacol Ther. 2012, 135: 279-291. 10.1016/j.pharmthera.2012.06.001.
Rajkumar VS, Howell K, Csiszar K, Denton CP, Black CM, Abraham DJ: Shared expression of phenotypic markers in systemic sclerosis indicates a convergence of pericytes and fibroblasts to a myofibroblast lineage in fibrosis. Arthritis Res Ther. 2005, 7: R1113-1123. 10.1186/ar1790.
Dulauroy S, Di Carlo SE, Langa F, Eberl G, Peduto L: Lineage tracing and genetic ablation of ADAM12(+) perivascular cells identify a major source of profibrotic cells during acute tissue injury. Nat Med. 2012,
Shi-Wen X, Renzoni EA, Kennedy L, Howat S, Chen Y, Pearson JD, Bou-Gharios G, Dashwood MR, du Bois RM, Black CM, Denton CP, Abraham DJ, Leask A: Endogenous endothelin-1 signaling contributes to type I collagen and CCN2 overexpression in fibrotic fibroblasts. Matrix Biol. 2007, 26: 625-632. 10.1016/j.matbio.2007.06.003.
Chesney J, Bucala R: Peripheral blood fibrocytes: novel fibroblast-like cells that present antigen and mediate tissue repair. Biochem Soc Trans. 1997, 25: 520-524.
Yeager ME, Nguyen CM, Belchenko DD, Colvin KL, Takatsuki S, Ivy DD, Stenmark KR: Circulating fibrocytes are increased in children and young adults with pulmonary hypertension. Eur Respir J. 2012, 39: 104-111. 10.1183/09031936.00072311.
Katebi M, Fernandez P, Chan ES, Cronstein BN: Adenosine A2A receptor blockade or deletion diminishes fibrocyte accumulation in the skin in a murine model of scleroderma, bleomycin-induced fibrosis. Inflammation. 2008, 31: 299-303. 10.1007/s10753-008-9078-y.
Field JJ, Burdick MD, DeBaun MR, Strieter BA, Liu L, Mehrad B, Rose CE, Linden J, Strieter RM: The role of fibrocytes in sickle cell lung disease. PloS One. 2012, 7: e33702-10.1371/journal.pone.0033702.
Tourkina E, Bonner M, Oates J, Hofbauer A, Richard M, Znoyko S, Visconti RP, Zhang J, Hatfield CM, Silver RM, Hoffman S: Altered monocyte and fibrocyte phenotype and function in scleroderma interstitial lung disease: reversal by caveolin-1 scaffolding domain peptide. Fibrogenesis Tissue Repair. 2011, 4: 15-10.1186/1755-1536-4-15.
Lee CG, Homer RJ, Cohn L, Link H, Jung S, Craft JE, Graham BS, Johnson TR, Elias JA: Transgenic overexpression of interleukin (IL)-10 in the lung causes mucus metaplasia, tissue inflammation, and airway remodeling via IL-13-dependent and -independent pathways. J Biol Chem. 2002, 277: 35466-35474. 10.1074/jbc.M206395200.
Andersson-Sjoland A, de Alba CG, Nihlberg K, Becerril C, Ramirez R, Pardo A, Westergren-Thorsson G, Selman M: Fibrocytes are a potential source of lung fibroblasts in idiopathic pulmonary fibrosis. Int J Biochem Cell Biol. 2008, 40: 2129-2140. 10.1016/j.biocel.2008.02.012.
Bucala R, Spiegel LA, Chesney J, Hogan M, Cerami A: Circulating fibrocytes define a new leukocyte subpopulation that mediates tissue repair. Mol Med. 1994, 1: 71-81.
Chan ES, Fernandez P, Merchant AA, Montesinos MC, Trzaska S, Desai A, Tung CF, Khoa DN, Pillinger MH, Reiss AB, Tomic-Canic M, Chen JF, Schwarzschild MA, Cronstein BN: Adenosine A2A receptors in diffuse dermal fibrosis: pathogenic role in human dermal fibroblasts and in a murine model of scleroderma. Arthritis Rheum. 2006, 54: 2632-2642. 10.1002/art.21974.
Sonnylal S, Denton CP, Zheng B, Keene DR, He R, Adams HP, Vanpelt CS, Geng YJ, Deng JM, Behringer RR, de Crombrugghe B: Postnatal induction of transforming growth factor beta signaling in fibroblasts of mice recapitulates clinical, histologic, and biochemical features of scleroderma. Arthritis Rheum. 2007, 56: 334-344. 10.1002/art.22328.
Loeys BL, Chen J, Neptune ER, Judge DP, Podowski M, Holm T, Meyers J, Leitch CC, Katsanis N, Sharifi N, Xu FL, Myers LA, Spevak PJ, Cameron DE, De Backer J, Hellemans J, Chen Y, Davis EC, Webb CL, Kress W, Coucke P, Rifkin DB, De Paepe AM, Dietz HC: A syndrome of altered cardiovascular, craniofacial, neurocognitive and skeletal development caused by mutations in TGFBR1 or TGFBR2. Nat Genet. 2005, 37: 275-281. 10.1038/ng1511.
Hoyles RK, Khan K, Shiwen X, Howat SL, Lindahl GE, Leoni P, du Bois RM, Wells AU, Black CM, Abraham DJ, Denton CP: Fibroblast-specific perturbation of transforming growth factor beta signaling provides insight into potential pathogenic mechanisms of scleroderma-associated lung fibrosis: exaggerated response to alveolar epithelial injury in a novel mouse model. Arthritis Rheum. 2008, 58: 1175-1188. 10.1002/art.23379.
Denton CP, Zheng B, Evans LA, Shi-wen X, Ong VH, Fisher I, Lazaridis K, Abraham DJ, Black CM, de Crombrugghe B: Fibroblast-specific expression of a kinase-deficient type II transforming growth factor beta (TGFbeta) receptor leads to paradoxical activation of TGFbeta signaling pathways with fibrosis in transgenic mice. J Biol Chem. 2003, 278: 25109-25119. 10.1074/jbc.M300636200.
Derrett-Smith EC, Dooley A, Khan K, Shi-wen X, Abraham D, Denton CP: Systemic vasculopathy with altered vasoreactivity in a transgenic mouse model of scleroderma. Arthritis Res Ther. 2010, 12: R69-10.1186/ar2986.
Wei J, Melichian D, Komura K, Hinchcliff M, Lam AP, Lafyatis R, Gottardi CJ, MacDougald OA, Varga J: Canonical Wnt signaling induces skin fibrosis and subcutaneous lipoatrophy: a novel mouse model for scleroderma?. Arthritis Rheum. 2011, 63: 1707-1717. 10.1002/art.30312.
Akhmetshina A, Palumbo K, Dees C, Bergmann C, Venalis P, Zerr P, Horn A, Kireva T, Beyer C, Zwerina J, Schneider H, Sadowski A, Riener MO, MacDougald OA, Distler O, Schett G, Distler JH: Activation of canonical Wnt signalling is required for TGF-beta-mediated fibrosis. Nat Commun. 2012, 3: 735-
Avouac J, Palumbo K, Tomcik M, Zerr P, Dees C, Horn A, Maurer B, Akhmetshina A, Beyer C, Sadowski A, Schneider H, Shiozawa S, Distler O, Schett G, Allanore Y, Distler JH: Inhibition of activator protein 1 signaling abrogates transforming growth factor beta-mediated activation of fibroblasts and prevents experimental fibrosis. Arthritis Rheum. 2012, 64: 1642-1652. 10.1002/art.33501.
Eferl R, Hasselblatt P, Rath M, Popper H, Zenz R, Komnenovic V, Idarraga MH, Kenner L, Wagner EF: Development of pulmonary fibrosis through a pathway involving the transcription factor Fra-2/AP-1. Proc Natl Acad Sci USA. 2008, 105: 10525-10530. 10.1073/pnas.0801414105.
Nusslein-Volhard C, Wieschaus E: Mutations affecting segment number and polarity in Drosophila. Nature. 1980, 287: 795-801. 10.1038/287795a0.
Horn A, Palumbo K, Cordazzo C, Dees C, Akhmetshina A, Tomcik M, Zerr P, Avouac J, Gusinde J, Zwerina J, Roudaut H, Traiffort E, Ruat M, Distler O, Schett G, Distler JH: Hedgehog signaling controls fibroblast activation and tissue fibrosis in systemic sclerosis. Arthritis Rheum. 2012, 64: 2724-2733. 10.1002/art.34444.
Horn A, Kireva T, Palumbo-Zerr K, Dees C, Tomcik M, Cordazzo C, Zerr P, Akhmetshina A, Ruat M, Distler O, Beyer C, Schett G, Distler JH: Inhibition of hedgehog signalling prevents experimental fibrosis and induces regression of established fibrosis. Ann Rheum Dis. 2012, 71: 785-789. 10.1136/annrheumdis-2011-200883.
Wei J, Fang F, Lam AP, Sargent JL, Hamburg E, Hinchcliff ME, Gottardi CJ, Atit R, Whitfield ML, Varga J: Wnt/beta-catenin signaling is hyperactivated in systemic sclerosis and induces Smad-dependent fibrotic responses in mesenchymal cells. Arthritis Rheum. 2012, 64: 2734-2745. 10.1002/art.34424.
Thoua NM, Derrett-Smith EC, Khan K, Dooley A, Shi-Wen X, Denton CP: Gut fibrosis with altered colonic contractility in a mouse model of scleroderma. Rheumatology. 2012, 51: 1989-1998. 10.1093/rheumatology/kes191.
Sonnylal S, Denton CP, Zheng B, Keene DR, He R, Adams HP, Vanpelt CS, Geng YJ, Deng JM, Behringer RR, de Crombrugghe B: Postnatal induction of transforming growth factor beta signaling in fibroblasts of mice recapitulates clinical, histologic, and biochemical features of scleroderma. Arthritis Rheum. 2007, 56: 334-344. 10.1002/art.22328.
Sonnylal S, Shi-Wen X, Leoni P, Naff K, Van Pelt CS, Nakamura H, Leask A, Abraham D, Bou-Gharios G, de Crombrugghe B: Selective expression of connective tissue growth factor in fibroblasts in vivo promotes systemic tissue fibrosis. Arthritis Rheum. 2010, 62: 1523-1532. 10.1002/art.27382.
Venalis P, Distler O, Lundberg IE, Schett G, Distler JH: Heart involvement in patients with systemic sclerosis is mimicked by Fra-2 transgenic mice. Ann Rheum Dis. 2012, 71 (Suppl 1): A46-
Drab M, Verkade P, Elger M, Kasper M, Lohn M, Lauterbach B, Menne J, Lindschau C, Mende F, Luft FC, Schedl A, Haller H, Kurzchalia TV: Loss of caveolae, vascular dysfunction, and pulmonary defects in caveolin-1 gene-disrupted mice. Science. 2001, 293: 2449-2452. 10.1126/science.1062688.
Razani B, Engelman JA, Wang XB, Schubert W, Zhang XL, Marks CB, Macaluso F, Russell RG, Li M, Pestell RG, Di Vizio D, Hou H, Kneitz B, Lagaud G, Christ GJ, Edelmann W, Lisanti MP: Caveolin-1 null mice are viable but show evidence of hyperproliferative and vascular abnormalities. J Biol Chem. 2001, 276: 38121-38138.
Samuel CS, Zhao C, Yang Q, Wang H, Tian H, Tregear GW, Amento EP: The relaxin gene knockout mouse: a model of progressive scleroderma. J Invest Dermatol. 2005, 125: 692-699. 10.1111/j.0022-202X.2005.23880.x.
Saito E, Fujimoto M, Hasegawa M, Komura K, Hamaguchi Y, Kaburagi Y, Nagaoka T, Takehara K, Tedder TF, Sato S: CD19-dependent B lymphocyte signaling thresholds influence skin fibrosis and autoimmunity in the tight skin mouse. J Clin Invest. 2002, 109: 1453-1462.
Gentiletti J, McCloskey LJ, Artlett CM, Peters J, Jimenez SA, Christner PJ: Demonstration of autoimmunity in the tight skin-2 mouse: a model for scleroderma. J Immunol. 2005, 175: 2418-2426.
Yamamoto T, Takagawa S, Katayama I, Yamazaki K, Hamazaki Y, Shinkai H, Nishioka K: Animal model of sclerotic skin. I: Local injections of bleomycin induce sclerotic skin mimicking scleroderma. J Invest Dermatol. 1999, 112: 456-462. 10.1046/j.1523-1747.1999.00528.x.
Kavian N, Servettaz A, Mongaret C, Wang A, Nicco C, Chéreau C, Grange P, Vuiblet V, Birembaut P, Diebold MD, Weill B, Dupin N, Batteux F: Targeting ADAM-17/notch signaling abrogates the development of systemic sclerosis in a murine model. Arthritis Rheum. 2010, 62: 3477-3487. 10.1002/art.27626.
Acknowledgements
AJG, CPD and AMH acknowledge an educational grant from Novartis Institute of Biomedical Research, and Arthritis Research UK.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
About this article
Cite this article
Gilbane, A.J., Denton, C.P. & Holmes, A.M. Scleroderma pathogenesis: a pivotal role for fibroblasts as effector cells. Arthritis Res Ther 15, 215 (2013). https://doi.org/10.1186/ar4230
Published:
DOI: https://doi.org/10.1186/ar4230