
Abstract
Introduction
The objective of this prospective study was to assess short- and long-term efficacy of exercise training (ET) as add-on to medical therapy in patients with connective tissue disease-associated pulmonary arterial hypertension (CTD-APAH).
Methods
Patients with invasively confirmed CTD-APAH received ET in-hospital for 3 weeks and continued at home for 12 weeks. Efficacy parameters have been evaluated at baseline and after 15 weeks by blinded-observers. Survival rate has been evaluated in a follow-up period of 2.9 ± 1.9 years.
Results
Twenty-one consecutive patients were included and assessed at baseline, and after 3 weeks, 14 after 15 weeks. Patients significantly improved the mean distance walked in 6 minutes compared to baseline by 67 ± 52 meters after 3 weeks (p < 0.001) and by 71 ± 35 meters after 15 weeks (p = 0.003), scores of quality of life (p < 0.05), heart rate at rest, peak oxygen consumption, oxygen saturation and maximal workload. Systolic pulmonary artery pressure and diastolic systemic blood pressure improved significantly after 3 weeks of ET. The 1- and 2-year overall-survival rates were 100%, the 3-year survival 73%. In one patient lung transplantation was performed 6 months after ET.
Conclusion
ET as add-on to medical therapy is highly effective in patients with CTD-APAH to improve work capacity, quality of life and further prognostic relevant parameters and possibly improves the 1-, 2- and 3-year survival rate. Further randomized controlled studies are needed to confirm these results.
Trial registration
ClinicalTrials.gov: NCT00491309.
Similar content being viewed by others


Introduction
Pulmonary arterial hypertension (PAH) is characterized by increased pulmonary arterial pressure and pulmonary vascular resistance [1] and can be associated with connective tissue disease (CTD) such as systemic sclerosis (SSc) [2] systemic lupus erythematosus (SLE) [3, 4] and mixed connective tissue diseases (MCTD) [5]. Associated PAH (APAH) accounts for approximately half of all patients with PAH [6] and has identical histological findings as idiopathic PAH (IPAH). However, patients with CTD-APAH seem to have a more severely affected clinical phenotype than patients with IPAH. In the American Registry to Evaluate Early and long Term PAH Disease Management (REVEAL Registry), patients with CTD-APAH had a significantly lower 6-minute walking distance (6MWD), higher B-type natriuretic peptide levels, lower diffusing capacity of carbon monoxide and a lower 1-year survival rate than patients with IPAH [7]. Despite advances in PAH treatment, CTD-APAH continues to be progressive, with a 1-year on-treatment mortality of approximately 12.5 to 17.0% compared to 5.0 to 10.0% in IPAH [7, 8]. In comparison to other forms of APAH, patients with SSc-APAH demonstrated the worst 1-, 2- and 3-year survival rates of 78.0%, 58.0% and 47.0%, respectively [9]. Patients with CTD-APAH showed a significantly reduced time to hospitalization, had a higher mean age at diagnosis and higher incidence of comorbidities such as renal insufficiency and Raynaud's phenomenon [7, 10]. Furthermore, randomized controlled studies reveal reduced efficacy of PAH-targeted medication in this subgroup. For example, in the BREATHE-1 study, bosentan therapy improved baseline 6MWD by 46 meters in 102 patients with IPAH, but only by 3 meters in the 33 patients with SSc-APAH [11]. In addition, therapy with ambrisentan resulted in significant improvement in the 6MWD among patients with IPAH but not with CTD-APAH [12]. Thus, patients with CTD-APAH in particular, may have a high need for additional therapeutic tools to address their exercise capacity, quality of life (QoL) and survival.
Exercise training (ET) has shown beneficial effects on exercise capacity and QoL in patients with PAH [13–15], SLE [16] and in SSc [17–19]. ET also improved peak oxygen consumption and World Health Organization functional class (WHO-FC) in patients with pulmonary hypertension [13], and possibly clinical outcomes, with 1- and 2-year survival rates of 100 and 95%, respectively [14]. Up to now there has been no study focusing on the effect of exercise training in patients with CTD-APAH. The aim of this study was to prospectively assess the effects of ET on prognostic relevant factors such as 6MWD and QoL, and to analyze the survival rate in a cohort of patients with CTD-APAH.
Materials and methods
Study population and design
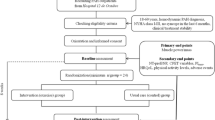
This prospective study investigated patients with CTD-APAH who received exercise and respiratory training as an add-on to disease-targeted medication, between October 2007 and July 2011. Further inclusion criteria were that patients must be aged between 18 and 80 years and classified as WHO-FC II to IV. Patients had to be under optimized medical therapy for PAH (endothelin-antagonists, inhaled or parenteral prostanoids, phosphodiesterase-5-inhibitors, anticoagulants, diuretics, and supplemental oxygen) and for the underlying rheumatologic disease (prednisone, methotrexate) for at least 2 months before entering the study. The diagnosis of CTD-APAH was established at the participating pulmonary hypertension (PH) centers according to current guidelines [1, 15]. The rheumatologic diagnosis of each patient had been confirmed by specialized rheumatologic centers. Patients with severe interstitial lung disease were excluded from the study. All patients underwent a detailed clinical work up including right heart catheterization, and all gave written informed consent for this study, which was approved by the Ethics Committee of the University of Heidelberg.
Outcome measures
Efficacy parameters of ET were prospectively assessed at baseline, week 3, and week 15 as described previously [13, 14]. The 6MWD was carried out under standardized conditions [20]. Cardiopulmonary exercise testing and stress Doppler echocardiography were performed during supine bicycle exercise as described previously [13]. Systolic pulmonary artery pressure (sPAP), systolic (RRsys) and diastolic (RRdiast) systemic blood pressure, workload, heart rate, ventilation, oxygen uptake (VO2), oxygen pulse (VO2/heart rate), oxygen saturation and carbon dioxide output (VCO2) were evaluated continuously. The anaerobic threshold (AT) was detected with the V-slope method. Gas exchange, Borg dyspnea index (with 6 representing no exertion and 20 maximal exertion) [21] and changes in WHO-FC were analyzed after 3 and 15 weeks. Health-related QoL assessment was measured by the Short Form Health Survey questionnaire (SF-36) [22]; the baseline scores were compared to the results after 15 weeks. The 6MWD and analysis of the SF-36 questionnaire were performed by investigators who were blinded to the patients' clinical data, so that the investigators did not know the values at any time point.
Exercise training program
We performed a program especially developed for patients with PH, that comprised at least 1.5 h/day ET as described previously [13, 14]. The program was started for the first 3 weeks in the Rehabilitation Clinic, Koenigstuhl, Heidelberg. It consisted of interval bicycle ergometer training at low workloads, mental gait training, dumbbell-training of single muscle groups using low weights (500 to 1000 g) and respiratory therapy 5 days/week. The training was continued at home with at least 30 minutes/day at 5 days/week for the following 12 weeks. Patients were asked to continue with ET at home after the 15-weeks-visit. In addition to physical training patients received psychological support and performed mental training to improve their perception of individual physical abilities and limits. Physicians specialized in rehabilitation medicine and PH experts closely supervised the training program as described before [13, 14]. Adverse events were recorded whenever they occurred. Oxygen saturation and heart rate were monitored continuously throughout the training and used to adjust the training intensity. When patients' oxygen saturation fell below 90% during exercise they received supplemental oxygen (3 to 10 L/min) throughout the training. At discharge from hospital after 3 weeks, patients received an individualized training manual and ordered a bicycle ergometer for use at home. All patients were asked to keep close contact with the physicians involved in the training program, and with their general practitioners and the specialized center.
Follow-up assessment
In 2011 all participating patients were interviewed by telephone using a half-structured questionnaire. The patients were asked about their current symptoms for WHO-FC, if and how they pursued ET at home, whether they had any adverse events from ET, any further cardiac events that might have occurred since the last observation and current medication. Patients who did not attend the last 15-week follow-up visit were the reason for missing the examination. If the patient was deceased, date of death was recorded and their relatives and/or treating physicians were asked for the cause and circumstances of death.
Statistical methods
The analyses were performed by a statistician (CF). The within-group comparisons of baseline and weeks 3 and 15 for 6MWD, workload, Borg dyspnea index, parameters of gas exchange, systolic pulmonary arterial pressure (sPAP), systemic blood pressures, heart rate as well as summation and sub-scores of the SF-36 were compared by the Wilcoxon rank test. Comparison of WHO-FC at different time points was performed by the McNemar-Bowden test. All tests were two sided and P-values < 0.05 were considered statistically significant. Bonferroni adjustment for multiple comparisons was performed for the primary endpoints, 6MWD and QoL parameters; P-values < 0.005 were considered significant. All analyses were carried out using IBM SPSS V19 (IBM Corp. Armonk, NY, USA). We describe in detail, the patients who did not attend the 15-week measurement. To access the consequences for the main efficacy parameter, 6MWD, we performed multiple imputations of 6MWD at 15 weeks within SPSS using the predictive mean matching model, with age, peak oxygen consumption, oxygen consumption at the AT, oxygen saturation at maximal workload, systolic blood pressure at maximal workload at baseline, 6MWD at baseline and 3 weeks, and pain subscale of the SF-36 at baseline as explanatory variables. Kaplan-Meier estimates were used for survival analysis with the 95% two-sided confidence interval (CI) calculated using Greenwood's formula. All treated patients were included in the survival analysis. Patients who died or underwent organ transplantation were counted as endpoints; survivors were regarded as censored.
Results
Study population
We included 22 consecutive patients (Table 1). One patient had to be excluded because she could not perform the examinations after week 3 and week 15, due to upper airway infection. Thus, the final study group consisted of 21 patients: 9 patients (43%) with SSc-APAH, 7 (33%) with SLE-APAH, 2 (10%) with MCTD and 3 (14%) with other CTDs such as Jo-1 syndrome and Sjöegren's syndrome. Demographic data, diagnosis, functional class, hemodynamic values, lung function and medical therapy in the full study population are summarized in Table 1. At baseline 9 patients (43%) were in WHO-FC II, 7 (33%) were classified as WHO-FC III and 5 (24%) as WHO-FC IV. Combination therapies, including two to three PAH-targeted agents, were used in 62% of patients (Table 1).
Assessment of training effects
ET significantly improved the 6MWD from 386 ± 121 (mean ± standard deviation (SD)) meters by 64 ± 47 meters after 3 weeks (P < 0.001) and by 71 ± 35 meters after 15 weeks (P < 0.003) (Figure 1). All patients except one improved their 6MWD (Figure 1). In the patient with no increase in 6MWD the test was limited by her hip joint osteoarthritis. However, in this patient other parameters of physical exercise capacity improved during the ET.

Individual changes in six-minute-walking distance (6MWD) after 3 and 15 weeks exercise training. Using the Wilcoxon rank test, P < 0.001 was obtained for the comparisons with baseline at week 3 (n = 21) and P = 0.003 for comparison to week 15 (n = 11). The dashed line indicates the mean change from baseline in 6MWD (67 ± 52 meters and 72 ± 35 meters).
Nine patients (43%) referred from PH-centers other than Heidelberg did not attend the visit after 15 weeks, mainly due to the long traveling distance. Results remained significant after multiple imputation of missing values for the 6MWD at 15 weeks using the explanatory variables as described in Methods. The improvement in 6MWD ranged from 71 to 79 meters in the imputation replications. Patients who did not attend the assessment after 15 weeks had a significantly higher peak oxygen consumption at the AT (716 ± 139 vs. 543 ± 161 ml/min; P = 0.038) and a higher improvement in 6MWD (79 ± 62 vs. 50 ± 24 meters; P = 0.156) after 3 weeks. They did not differ significantly in other parameters such as demographics or parameters of right heart catheterization. After Bonferroni adjustment, improvement in 6MWD remained statistically significant.
ET also significantly improved QoL parameters indicated by the SF-36 subscale scores for physical functioning (P = 0.025), general health perception (P = 0.049), social functioning (P = 0.008), mental health (P = 0.033) and vitality (P = 0.021) (Figure 2, Table 2).

Mean short-form Health Survey Questionnaire (SF-36) scores for quality of life subscales before and after exercise training. At baseline (straight line), mean SF-36 scores were significantly reduced in comparison to respective values from a normal population (dotted line). After 15 weeks (dashed line), 5 scales of the SF-36 questionnaire improved significantly: physical functioning, general health perception, social functioning, mental health and vitality. P-values are indicated vs. baseline. No significant improvement was found for role emotional (ROLEM), role physical (ROLPH) and bodily pain (PAIN) after training. With Bonferroni adjustment, values of P < 0.005 were considered statistically significant. Data were available and were included in the analyses for 21 patients studied at baseline and for 18 patients studied at 15 weeks.
Mean peak oxygen consumption, peak oxygen consumption/kg body weight, oxygen consumption at the anaerobic threshold, and oxygen saturation at maximal workload during cardiopulmonary exercise testing increased significantly from baseline to 3 weeks and to 15 weeks (Table 2). Heart rate at rest significantly decreased after 3 and 15 weeks. After 15 weeks patients achieved significantly higher workloads with an increase of maximal heart rate during cardiopulmonary exercise testing and maximal systolic blood pressure. The Borg scale remained unchanged although significantly higher workloads and higher heart rates during exercise were attained (Table 2 Figure 3). After 3 weeks of ET, mean diastolic blood pressure and sPAP at rest were significantly reduced (Table 2). C-reactive protein reduced in trend, but not significantly, after 3 and 15 weeks, whereas N-terminal prohormone of brain natriuretic peptide (NT-proBNP) plasma-levels remained unchanged. Seven patients improved their WHO-FC after 15 weeks; five of them were reclassified as WHO-FC IV. Nevertheless, the change in WHO-FC after 3 weeks and after 15 weeks compared to baseline was not significant (P = 0.058 and P = 0.096, respectively), possibly due to the small sample size.

Workload compared to the Borg scale. The figure shows a significant increase in workload after 3 and 15 weeks (P = 0.007 and P = 0.008). The Borg scale remained unchanged (P = 0.171 and P = 0.105, respectively) although significantly higher workloads and higher heart rates during exercise were attained. Values are indicated as the mean, and the bars represent standard deviation. The columns represent workload (measured in Watt) and the dotted line the Borg Scale.
Adverse events
During the 3-week in-hospital training, three patients had adverse events as follows: gastrointestinal infection with diarrhea (n = 1) and respiratory infections (n = 2). In all three patients the infection was treated successfully so that they were able to continue the training program after one or two weeks. All other patients (81%) tolerated the ET well. There were no signs of clinical worsening or right heart failure during the in-hospital program.
Follow-up and survival
Follow-up data were obtained after 2.9 ± 1.9 years (Figure 4). One patient had been listed for lung transplantation before starting the rehabilitation program. She improved her walking distance by about 88 meters after 3 weeks, but did not perform the examination after 15 weeks due to the long traveling distance. However, she required lung transplantation 6 months later. Between 2.8 and 5.0 years after in-hospital rehabilitation, two patients died due to PAH and right heart failure, and one patient died due to cancer of unknown primary origin. The Kaplan-Meier PAH-survival rate was 100% after 1 and 2 years, and 80% after 3 years (Figure 4). The overall survival rate was 100% after 1 and 2 years, and 73% after 3 years. The transplantation-free survival rate was 95% after 1 and 2 years (Figure 4).

Survival by Kaplan-Meier analysis. Within a follow-up period of 2.9 ± 1.9 years (25 ± 13 months), two patients died due to pulmonary hypertension (PH), one died due to carcinoma, and one patient underwent lung transplantation. The dashed line indicates mortality due to connective tissue disease-associated pulmonary arterial hypertension (CTD-APAH), the straight line indicates overall survival, and the dotted line indicates transplantation-free survival. The Kaplan-Meier PAH-survival rate was 100% after 1, and 2 years, and 80% after 3 years. The overall survival rate was 100% after 1, and 2 years, and 73% after 3 years. The transplantation-free survival rate was 95% after 1 and 2 years.
ET was continued over 3 years by 11 patients (61%). They reported a mean ET-duration of 29 ± 18 minutes at 4 ± 2 days/week. Among the 11 patients, 44% continued bicycle ergometer training, 17% dumbbell-training, 33% walking and 22% alternative training, such as gymnastics. Four patients (22%) combined two training items and three patients (17%) combined three items. Six patients (33%) stopped exercise training for the following reasons: pain, presyncopes, no permanent instruction and confidence with general state of health.
Discussion
This is the first prospective clinical trial investigating short- and long-term effects of ET as an add-on to PAH-targeted medication in patients with severe CTD-APAH. The results of the study suggest that ET can significantly improve prognostic relevant parameters such as exercise capacity and QoL in this condition, and has an excellent long-term survival of 100% after 2 years and 80% after 3 years.
The results represent an important source of data on survival, exercise capacity and QoL in patients with CTD-APAH treated with ET. The 6MWD, QoL questionnaire (SF-36), peak oxygen consumption, oxygen consumption at the AT, maximal oxygen saturation and maximal workload increased significantly with ET after 3 and 15 weeks. RRdiast and sPAP significantly decreased after 3 weeks. This may be due to an improvement in endothelial dysfunction. Nevertheless, due to the limited number of patients we cannot exclude that these improvements occurred coincidentally. The Borg scale remained unchanged although significantly higher workloads and higher heart rates during exercise were attained. These results are in line with previous studies of ET in patients with other forms of PH/PAH [13–15]. There are few data on exercise training in CTD. In patients with SSc but not PAH, ET has improved QoL parameters (SF-36) and heart rate at rest [19], 6 MWD [18] and muscle strength [17]. Quality of life and peak VO2 have also been significantly ameliorated by training in patients with SLE without PAH [16].
Survival of patients with CTD-APAH after training
The Kaplan-Meier overall survival rate of 100% after 1 and 2 years and 73% (80% PH-related survival) after 3 years, using ET as add-on to optimized PAH-targeted medical treatment, can be considered a positive outcome in CTD-APAH. Despite optimized PAH-targeted therapy, the Reveal registry showed a 1-year survival in patients with SSC-APAH of only 82% vs. 84% in SLE-APAH, 88% in MCTD-APAH and 93% in IPAH [7]. In two trials of bosentan in CTD-APAH-patients, the Kaplan-Meier estimates of survival were 85.9% and 73.4% after 1 and 2 years, respectively [23]. The 3-year survival rate in SSc-APAH was 60% vs. 78% in IPAH [8]. Similar patterns have been seen in the UK registry [9] and the French registry [24, 25] and in several further studies [26]. These data indicate that patients with CTD-APAH represent a high-risk subgroup of patients with PAH. The CTD-APAH-cohort assessed in this study had been severely affected with a mean 6MWD of 386 ± 121 meters at baseline despite double or even triple PAH-targeted therapy in 62% of patients, and is therefore comparable to the cohorts described previously. We cannot exclude that we selected highly motivated and compliant patients with fewer outcome limitations. In addition, the number of patients in our study was quite small. Nevertheless, ET may have improved survival by ameliorating prognostic relevant factors such as QoL, exercise capacity and oxygen consumption. Since heart rate at rest, RRdiast and peak oxygen consumption significantly improved, ET possibly improved right ventricular reserve [14]. Similar effects of ET have been seen in patients with IPAH and CTEPH and right heart failure [14, 15].
Improvement in 6-minute-walking distance
The 6MWD has been used as primary endpoint in many randomized controlled clinical trials in PAH [1], and correlates with prognostic relevant clinical parameters such as WHO-FC in patients with SSc-PAH [6]. However, the test is not sufficiently validated in CTD-APAH and in patients with rheumatic diseases in particular, it is influenced by comorbidity and musculoskeletal limitations [6, 27]. This has been taken as explanation for the fact that 6MWD in patients with CTD-APAH is at best only minimally improved by PAH-targeted medication. In randomized controlled trials, sildenafil is the only drug to have been associated with a significant increase in 6MWD in patients with CTD-APAH (in many other trials no subgroup analysis for this disease has been performed). Therefore, a mean increase of almost 70 meters after 3 and 15 weeks ET is unexpectedly high. The absence of a non-trained placebo group may be considered a limitation of the study, with concern that some of the improvements were due to the so-called placebo effect, rather than efficacy of ET. However, previously reported placebo-controlled PAH studies of bosentan or other PAH-specific treatments have not shown any clinically relevant improvements in the placebo groups. In fact, they have consistently shown a continuous decline in 6MWD. Therefore, the results of this study suggest that, especially in CTD-APAH-patients with known high coincidence of musculoskeletal limitations, ET as an add-on to PAH-targeted medication may be useful, and possibly even more effective in improving exercise capacity than medical treatment. Further randomized trials are needed to clarify this question.
Limitations
The results of this prospective study are promising and our data provide a good rationale for future studies of exercise training in patients with CTD-APAH. However, the positive results may also be influenced by the small sample size. Larger, randomized controlled and multicentric studies are needed to determine the effectiveness of exercise training in CTD-APAH. The effects of ET after 15 weeks may be biased due to the missing values of about 43% of patients who did not perform the last follow-up visit. A comparison between patients who completed the 15 week assessment and those who did not revealed that patients who dropped out had even better improvement in efficacy parameters after 3 weeks in-hospital rehabilitation. This suggests that they possibly did not attend because they felt better. Feedback from patients during follow-up visits supports this assumption.
It is a general issue of rehabilitation programs that the therapy cannot be performed in a blinded fashion and that a referral bias towards highly motivated patients with a better outcome may occur. Further studies are necessary to determine the effects of training programs on outcome in patients with PH.
Conclusion
This is the first trial investigating exercise training in CTD-APAH as an add-on to optimized medical therapy. The results indicate that ET is effective in CTD-APAH and may improve work capacity, QoL and further prognostic relevant parameters, and possibly improves the 1-, 2- and 3-year survival rate. Further randomized controlled studies are needed to confirm these results.
Abbreviations
- APAH:
-
associated pulmonary arterial hypertension
- AT:
-
anaerobic threshold
- CI:
-
confidence interval
- CTD:
-
connective tissue disease
- EqCO2:
-
ventilatory equivalent for carbon dioxide
- ET:
-
exercise training
- FEV1%VC:
-
forced expiratory volume in one second/vital capacity
- IPAH:
-
idiopathic pulmonary arterial hypertension
- MCTD:
-
mixed connective tissue disease
- 6MWD:
-
six minute walking distance
- NT-proBNP:
-
N-terminal prohormone of brain natriuretic peptide
- PAH:
-
pulmonary arterial hypertension
- PCWP:
-
pulmonary capillary wedge pressure
- PH:
-
pulmonary hypertension
- pO2:
-
partial oxygen pressure
- QoL:
-
quality of life
- REVEAL-Registry:
-
Registry to Evaluate Early and long Term PAH Disease Management
- RRdiast:
-
diastolic systemic blood pressure
- RRsys:
-
systolic systemic blood pressure
- SD:
-
standard deviation
- SF-36:
-
short form Health Survey Questionnaire
- SLE:
-
systemic lupus erythematosus
- sPAP:
-
systolic pulmonary arterial pressure
- SSc:
-
systemic sclerosis
- TLCO:
-
carbon monoxide transfer factor
- VCO2:
-
carbon dioxide output
- VE:
-
ventilation
- VO2/heart rate:
-
oxygen pulse
- VO2:
-
oxygen uptake
- WHO-FC:
-
World Health Organization functional class.
References
Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G, ESC Committee for Practice Guidelines (CPG): Guidelines for the diagnosis and treatment of pulmonary hypertension: The Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J. 2009, 30: 2493-537.
Mukerjee D, St George D, Coleiro B, Knight C, Denton CP, Davar J, Black CM, Coghlan JG: Prevalence and outcome in systemic sclerosis associated pulmonary arterial hypertension: application of a registry approach. Ann Rheum Dis. 2003, 62: 1088-93. 10.1136/ard.62.11.1088.
Li EK, Tam LS: Pulmonary hypertension in systemic lupus erythematosus: clinical association and survival in 18 patients. J Rheumatol. 1999, 26: 1923-29.
Chung SM, Lee CK, Lee EY, Yoo B, Lee SD, Moon HB: Clinical aspects of pulmonary hypertension in patients with systemic lupus erythematosus and in patients with idiopathic pulmonary arterial hypertension. Clin Rheumatol. 2006, 25: 866-72. 10.1007/s10067-006-0206-5.
Burdt MA, Hoffman RW, Deutscher SL, Wang GS, Johnson JC, Sharp GC: Long-term outcome in mixed connective tissue disease: longitudinal clinical and serologic findings. Arthritis Rheum. 1999, 42: 899-909. 10.1002/1529-0131(199905)42:5<899::AID-ANR8>3.0.CO;2-L.
Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaici A, Weitzenblum E, Cordier JF, Chabot F, Dromer C, Pison C, Reynaud-Gaubert M, Haloun A, Laurent M, Hachulla E, Simonneau G: Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006, 173: 1023-30. 10.1164/rccm.200510-1668OC.
Chung L, Liu J, Parsons L, Hassoun PM, McGoon M, Badesch DB, Miller DP, Nicolls MR, Zamanian RT: Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest. 2010, 138: 1383-94. 10.1378/chest.10-0260.
Clements PJ, Tan M, McLaughlin VV, Oudiz RJ, Tapson VF, Channick RN, Rubin LJ, Langer A, Pulmonary Arterial Hypertension Quality Enhancement Research Initiative (PAH-QuERI) Investigators: The pulmonary arterial hypertension quality enhancement research initiative: comparison of patients with idiopathic PAH to patients with systemic sclerosis-associated PAH. Ann Rheum Dis. 2012, 71: 249-52. 10.1136/annrheumdis-2011-200265.
Condliffe R, Kiely D, Peacock AJ, Corris PA, Gibbs JS, Vrapi F, Das C, Elliot CA, Johnson M, DeSoyza J, Torpy C, Goldsmith K, Hodgkins D, Hughes RJ, Pepke-Zaba J, Coghlan JG: Connective tissue disease-associated pulmonary arterial hypertension in the modern treatment era. Am J Respir Crit Care Med. 2009, 179: 91-92.
Goldberg A: Pulmonary Arterial Hypertension in Connective Tissue Diseases. Cardiol Rev. 2010, 18: 85-88. 10.1097/CRD.0b013e3181cbcde7.
Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, Pulido T, Frost A, Roux S, Leconte I, Landzberg M, Simonneau G: Bosentan therapy for pulmonary arterial hypertension. N Engl J Med. 2002, 346: 896-903. 10.1056/NEJMoa012212.
Galie N, Olschewski H, Oudiz RJ, Torres F, Frost A, Ghofrani HA, Badesch DB, McGoon MD, McLaughlin VV, Roecker EB, Gerber MJ, Dufton C, Wiens BL, Rubin LJ, Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy Studies (ARIES) Group: Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation. 2008, 117: 3010-19. 10.1161/CIRCULATIONAHA.107.742510.
Mereles D, Ehlken N, Kreuscher S, Ghofrani S, Hoeper MM, Halank M, Meyer FJ, Karger G, Buss J, Juenger J, Holzapfel N, Opitz C, Winkler J, Herth FF, Wilkens H, Katus HA, Olschewski H, Grünig E: Exercise and respiratory training improve exercise capacity and quality of life in patients with severe chronic pulmonary hypertension. Circulation. 2006, 114: 1482-89. 10.1161/CIRCULATIONAHA.106.618397.
Grünig E, Ehlken N, Ghofrani A, Staehler G, Meyer FJ, Juenger J, Opitz CF, Klose H, Wilkens H, Rosenkranz S, Olschewski H, Halank M: Effect of exercise and respiratory training on clinical progression and survival in patients with severe chronic pulmonary hypertension. Respiration. 2011, 81: 394-401. 10.1159/000322475.
Grünig E, Lichtblau M, Ehlken N, Ghofrani HA, Reichenberger F, Staehler G, Halank M, Fischer C, Seyfarth HJ, Klose H, Meyer A, Sorichter S, Wilkens H, Rosenkranz S, Opitz C, Leuchte H, Karger G, Speich R, Nagel C: Safety and efficacy of exercise training in various forms of pulmonary hypertension. Eur Respir J.
Carvalho MR, Sato EI, Tebexreni AS, Heidecher RT, Schenkman S, Neto TL: Effects of supervised cardiovascular training program on exercise tolerance, aerobic capacity, and quality of life in patients with systemic lupus erythematosus. Arthritis Rheum. 2005, 53: 838-44. 10.1002/art.21605.
Pinto ALS, Oliveira NC, Gualano B, Christmann RB, Painelli VS, Artioli GG, Prado DM, Lima FR: Efficacy and safety of concurrent training in systemic sclerosis. J Strength Cond Res. 2011, 25: 1423-28. 10.1519/JSC.0b013e3181d6858b.
Schouffoer AA, Ninaber MK, Beaart-van de Voorde LJ, van der Giesen FJ, de Jong Z, Stolk J, Voskuyl AE, Scherptong RW, van Laar JM, Schuerwegh AJ, Huizinga TW, Vlieland TP: Randomized comparison of a multidisciplinary team care program with usual care in patients with systemic sclerosis. Arthritis Care Res. 2011, 63: 909-17. 10.1002/acr.20448.
Antonioli CM, Bua G, Frigè A, Prandini K, Radici S, Scarsi M, Danieli E, Malvicini A, Airo P: An individualized rehabilitation program in patients with systemic sclerosis may improve quality of life and hand mobility. Clin Rheumatol. 2009, 28: 159-65. 10.1007/s10067-008-1006-x.
Guyatt GH, Pugsley SO, Sullivan MJ, Thompson PJ, Berman L, Jones NL, Fallen EL, Taylor DW: Effect of encouragement on walking test performance. Thorax. 1984, 39: 818-22. 10.1136/thx.39.11.818.
Borg G: Psychophysical bases of perceived exertion. Med Sci Sports Exerc. 1982, 14: 377-81.
Ware J, Sherbourne C: The MOS 36-Item Short-Form Health Survey (SF-36): I. conceptual framework and item selection. Medical Care. 1992, 30: 473-83. 10.1097/00005650-199206000-00002.
Denton CP, Pope JE, Peter HH, Gabrielli A, Boonstra A, van den Hoogen FH, Riemekasten G, De Vita S, Morganti A, Dölberg M, Berkani O, Guillevin L, TRacleer Use in PAH associated with Scleroderma and Connective Tissue Diseases (TRUST) Investigators: Long-term effects of bosentan on quality of life, survival, safety and tolerability in pulmonary arterial hypertension related to connective tissue diseases. Ann Rheum Dis. 2008, 67: 1222-28.
Hachulla E, Launay D, Yaici A, Berezne A, de Groote P, Sitbon O, Mouthon L, Guillevin L, Hatron PY, Simonneau G, Clerson P, Humbert M, French PAH-SSc Network: Pulmonary arterial hypertension associated with systemic sclerosis in patients with functional class II dyspnoea: mild symptoms but severe outcome. Rheumatology. 2010, 49: 940-944. 10.1093/rheumatology/kep449.
Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaïci A, Weitzenblum E, Cordier JF, Chabot F, Dromer C, Pison C, Reynaud-Gaubert M, Haloun A, Laurent M, Hachulla E, Cottin V, Degano B, Jaïs X, Montani D, Souza R, Simonneau G: Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010, 122: 156-63. 10.1161/CIRCULATIONAHA.109.911818.
Johnson SR, Granton JT: Pulmonary hypertension in systemic sclerosis and systemic lupus erythematosus. Eur Respir Rev. 2011, 20: 277-86. 10.1183/09059180.00003811.
Impens AJ, Wangkaew S, Seibold JR: The 6-minute walk test in scleroderma--how measuring everything measures nothing. Rheumatology. 2008, 47: 68-69. 10.1093/rheumatology/kem296.
Acknowledgements
We would like to thank all patients who participated, and the patient association, Pulmonale Hypertonie eV, especially Bruno Kopp, for their support. We are grateful for the support of the clinic director Karl-Heinz Markmann, Alexander Heinz, all physicians especially Robert Nechwatal, Gabriele Karger, Soeren Uiker, the psychologist Volker Weigand, the therapists, and physiotherapists of the Rehabilitation Clinic Koenigstuhl, Heidelberg, who took part in the rehabilitation program. The study was funded by a grant from the German Pulmonary Hypertension Association; Pulmonale Hypertonie eV, Rheinstetten, Germany.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
EG, CN and NE were responsible for designing the study, and conducting and analyzing the results and were directly involved in data collection. FM, FP and ML were directly involved in acquisition of data. CF was directly involved in analyzing and interpreting the results. NB, CF, FS, GS, FR, HT, MH, HJS and SW were principle investigators directly involved in data collection. All authors were involved in the writing of the manuscript and saw and approved the final version of the paper.
Ekkehard Grünig, Felicitas Maier, Simone Wagner and Christian Nagel contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Grünig, E., Maier, F., Ehlken, N. et al. Exercise training in pulmonary arterial hypertension associated with connective tissue diseases. Arthritis Res Ther 14, R148 (2012). https://doi.org/10.1186/ar3883
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/ar3883