
Abstract
Previously, a dominant role of the adaptive immune system in the pathogenesis of Sjögren's syndrome was suspected. Recent advances, however, have revealed a major role of the type I IFN pathway, documented by an increased circulating type I IFN activity and an IFN 'signature' in peripheral blood mononuclear cells and minor salivary gland biopsies from the patients. Polymorphisms in the genes IRF5 and STAT4 leading to increased IFN activation are associated with disease susceptibility. In the pathogenesis of Sjögren's syndrome, the activation of salivary gland epithelial cells appears to be the initial event. Once intrinsically activated, they express costimulatory and Toll-like receptors (TLRs) and MHC class I and II molecules, can present autoantigens and produce proinflammatory cytokines. The subsequent activation of plasmacytoid dendritic cells induces the production of high levels of proinflammatory cytokines in individuals with the risk alleles of the susceptibility genes IRF5 and STAT4. Under the influence of the high IFN concentration in the glands and through TLR ligation, B-cell activating factor is produced by epithelial cells and, together with autoantigen presentation on salivary gland epithelial cells, stimulates the adaptive immune system. In view of the central role of IFNalpha in at least the initiation of the pathogenesis of Sjögren's syndrome, blockade of this cytokine may be a rational therapeutic approach.
Similar content being viewed by others

Introduction
Sjögren's syndrome (SS) is an autoimmune disorder affecting the lachrymal and salivary glands and leads to dry eyes and dry mouth. Due to the presence of lymphocytic infiltrates in the glands and the presence of auto-antibodies (rheumatoid factors and antibodies against SS-A, SS-B, muscarinic receptors and alpha-fodrin), SS has been regarded as a disorder that is caused by aberrations in the adaptive immune system. Recent evidence reviewed here, however, points to a major contribution of the innate immune system, at least in the initiation of the pathogenesis of SS.
Genetic susceptibility factors of Sjögren's syndrome
The etiology of SS is still unclear. Since there is a familial aggregation of primary SS, however, genetic susceptibility factors have been suspected for a long time. Initially, HLA haplotypes were shown to be associated with primary SS. Later on, however, it became clear that they are primarily associated only with the subset of patients with SS-A (HLA-DRB1*15) or SS-A and SS-B antibodies (HLA-DRB1*03), but not with all subsets of SS. Currently, genome-wide association studies are being performed to identify the susceptibility genes of SS. So far, the genes IRF5 (Interferon regulatory factor-5) and STAT4 (Signal transducer and activator of transcription 4) have been convincingly identified and replicated in several studies as susceptibility factors of primary SS independent of the presence of autoantibodies.
Interferon regulatory factor-5
IRF5 is a transcription factor that mediates virus- and IFN-induced signaling pathways. Infection of cells with various viruses can activate Toll-like receptors (TLRs) and, further downstream, IRF5 to induce IFNalpha and the transcription of numerous inflammatory proteins [1]. IRF5-/- mice are highly vulnerable to both DNA and RNA viruses and infection of them was accompanied by low IFNalpha concentrations in the sera [2].
Three studies have confirmed an association between a polymorphism in the IRF5 gene and primary SS. In a French study [3], the IRF5 SNP rs2004640 GT or TT genotype was identified in 87% of primary SS patients but in only 77% of controls (odds ratio (OR) 1.93). The IRF5 rs2004640 T allele was found on 59% of chromosomes from primary SS patients compared with 52% of chromosomes from controls (OR 1.36). In a study of patients from Sweden and Norway [4], a 5-bp CGGGG indel in the promoter of IRF5 that is adjacent to rs2004640 was associated with primary SS (OR 1.63). In another French study [5], the 5-bp CGGGG indel in the promoter of the IRF5 allele was confirmed to transmit an increased risk of primary SS in two cohorts (odds ratio 2.0).
The CGGGG indel polymorphism of IRF5 is also associated with other autoimmune disorders, such as systemic lupus erythematosus (SLE) [6, 7], rheumatoid arthritis [8], and inflammatory bowel disease [9], suggesting common pathways in the induction of autoimmune disorders.
In functional studies, the presence of the risk allele was correlated with a high level of IRF5 mRNA in both peripheral blood mononuclear cells (PBMCs) and salivary gland epithelial cells (SGECs) and with increased levels of mRNA transcripts of the IFN-induced genes MX1 and IFITM1 [5]. As further evidence for the functional impact of the risk allele, increased expression of IRF5 mRNA from a promoter containing that allele was found using a minigene reporter. Increased expression of IRF5 protein was also observed in PBMCs from SLE patients carrying the risk allele of the CGGGG indel [6].
Signal transducer and activator of transcription 4
The STAT4 transcription factor plays a key role in signaling via the IFNalpha receptor by being activated and translocated to the nucleus after receptor ligation [10]. Besides its role in type I IFN signaling, STAT4 is also induced by IL-12 and IL-23 production by macrophages and dendritic cells, and is responsible for the IL-12-dependent activation of natural killer (NK) cells, polarization of naïve CD4+ T cells to IFNgamma- producing Th1 cells and the IL-23 -dependent expansion of Th17 cells. Thus, STAT4 has many stimulatory effects on the immune system and may contribute to autoimmune responses by affecting the functions of both innate and adaptive immune cells.
Association studies of SNPs in the STAT4 gene revealed that the T allele of rs7574865 was more common in primary SS patients (on 29.6% of chromosomes) than in controls (on 22.3% of chromosomes) [11]. The findings were confirmed in a cohort from Colombia and Germany, in which the T allele was again associated with primary SS (OR 1.40) [12]. The C allele of the SNP rs7582694 of the STAT4 gene, which is in complete linkage disequilibrium with SNP rs7574865, was associated with primary SS in a French cohort (OR 1.57) [13].
Polymorphism of STAT4 has also been associated with other autoimmune disorders. The haplotype marked by the SNP rs7574865 was more common in SLE patients of European ancestry (OR 1.55) [14], in SLE patients from the US and Sweden (OR 1.57) [15] and in a Chinese Han population (OR 1.51) [16].
The T allele of SNP rs7574865 was also found to be associated with rheumatoid arthritis [14, 17], with ORs comparable to those observed in SLE, and, in a Spanish study, with susceptibility to limited cutaneous systemic sclerosis (OR 1.61), but not with diffuse cutaneous systemic sclerosis [18]. These data have been confirmed in a combined meta-analysis of the Spanish cohort and five independent cohorts of European ancestry [18].
There was no significant association of any of the STAT4 genotypes with mRNA levels of STAT4α and STAT4β among 30 primary SS patients [13]. There was, however, a weak correlation of STAT4 rs7574865 and rs7582694 polymorphisms, which are in complete linkage disequilibrium, with STAT4α mRNA levels in PBMCs from healthy donors [19]. In addition, the presence of the SNP correlated with increased expression of the risk allele of STAT4β in primary cells of mesenchymal origin (osteoblasts) [20].
Those patients who carry all of the IRF5 and STAT4 risk alleles have an increased risk (OR = 6.78) for primary SS [4]. The association of both STAT4 and IRF5 polymorphisms with many autoimmune diseases that are type 1 IFN driven suggests that STAT4 and IRF5 can contribute to a general loss of tolerance and that IFN is also a major player in the induction of primary SS.
TREX-1
Recently, mutations in the TREX-1 gene (which encodes the most abundant 3'-5' DNA exonuclease in cells [21]) have been found to be tightly linked with the development of autoimmune diseases, including primary SS. Loss of function mutations of the human TREX-1 gene cause Aicardi-Goutieres syndrome [22], which presents as severe encephalitis in infants, a disorder resembling a congenitally acquired viral infection. Patients with Aicardi-Goutieres syndrome have elevated levels of type I IFN in the cerebrospinal fluid. Mutations in the TREX-1 gene have also been associated with monogenic chilblain lupus [23] and later with SLE [24]. Most of the cases we contributed to the latter analysis were patients who had suffered from SLE and secondary SS, and subsequent careful examination of relatives of these index subjects revealed that several family members carrying the TREX-1 mutations also suffered from primary SS (un-published observations).
It has been suggested that TREX-1 mutations result in defective clearance of intracellular DNA, in particular from endogenous retroelements, which in the absence of functional TREX-1 induces the production of type I IFN and thus autoimmunity [25]. Trex-1 knockout mice die from inflammatory myocarditis at an early age [26], and in Trex-1-deficient mice single-stranded DNA fragments derived from endogenous retroelements have been shown to accumulate in the heart and induce myocarditis [25]. The accumulation of single-stranded DNA in the absence of Trex-1 induces the production of type I IFN and a double knockout of Trex-1 and the type I IFN receptor protected mice from developing the myocarditis observed in the Trex-1 single knockout [23], suggesting that IFN has a crucial role in this model of autoimmunity. Taken together, the observations from recent genetic studies point to a major influence of the type I IFN pathway, and thus innate immunity, on the pathogenesis of primary SS.
IFN signature in primary Sjögren's syndrome
As described above, the function of the susceptibility genes of SS suggest an important role of type I IFN in its pathogenesis. Indeed, two transcriptome studies documented an IFN signature in the salivary glands of patients with primary SS [27, 28]. Using a complementary DNA microarray to compare gene expression profiles in minor salivary glands obtained from ten patients with primary SS and ten control subjects, there was an upregulation of numerous type I IFN-induced genes in primary SS [27]. Furthermore, global gene expression profiling of minor salivary gland cells revealed that the expression of 23 genes in the IFN pathway, including two encoding TLRs (TLR8 and TLR9), was significantly different between patients with primary SS and controls [28]. In addition, mRNA obtained from peripheral blood of patients with primary SS revealed a pattern of overexpression of IFN-induced genes [29]. Approximately 50% of the over-expressed genes in PBMCs from the peripheral blood of patients with primary SS were found to be IFN inducible.
It has been difficult to detect elevated concentrations of IFN itself in the blood of patients with SS, most likely due to technical challenges with the commercially available ELISA kits. However, it was recently shown that serum and plasma from patients with primary SS can induce IFN-regulated genes in PBMCs from control donors [30]. In addition, higher concentrations of IFNalpha and IFNbeta in the serum of patients with primary SS were found when cell reporter assays were used, which are more sensitive than ELISAs [31].
Plasmacytoid dendritic cells (PDCs) are the most potent producers of IFNalpha, producing up to 1,000 times more type I IFN than other cells. Circulating PDCs express higher levels of the activation marker CD40 in patients with primary SS. The number of PDCs in the blood of primary SS patients is reduced, but in immunohisto-chemistry studies these IFN-producing cells were detected in the salivary glands of all patients with primary SS but not in controls [28]. These results imply an influx of PDCs from the blood into the inflamed tissues in primary SS.
Salivary gland epithelial cells
Immunohistochemistry revealed that the lymphocytic infiltrates in SS form around epithelial structures of affected organs - for example, around the glandular epithelium of the exocrine glands [32]. Therefore, the term 'autoimmune epithelitis' was suggested for primary SS [33] and research has focused on the role of epithelial cells such as the SGECs.
Evidence for the activation of SGECs has been provided by immunohistochemical analyses showing that they express MHC class I and II molecules, the costimulatory molecules CD80 and CD86, the adhesion receptors intercellular adhesion molecule (ICAM)-1 and vascular cell adhesion molecule, and the local production of various chemokines and cytokines (IL1, IL6, TNF family member B cell-activating factor (BAFF)). In addition, conjunctival epithelial cells have been found to present the autoantigen SS-B (La) [34]. SGECs may thus promote the formation of lymphoid follicles by attracting and activating both B and T cells.
These findings were able to be replicated in vitro after techniques had been developed for long-term culture of SGECs. Cultured SGECs produce high amounts of BAFF and express several TLRs [35]. In addition, SGECs have been found to be prone to apoptosis. They produce exosomes, which are of endosomal origin and derive from the fusion of endosomes/lysosomes with the plasma membrane. Exosomes contain various proteins, including MHC class I and II and costimulatory molecules, cytoskeletal proteins and chaperones, and play a role in the exchange of cellular material and in the transfer of antigens to dendritic cells. SGECs have been shown to contain SS-A and SS-B [36], and therefore may initiate the typical autoantibody response in primary SS.
It is not clear yet what factors are responsible for the activation of SGECs in primary SS. Intriguingly, the signs of activation of SGECs, such as upregulation of MHC class I molecules, costimulatory molecules, TLRs and BAFF, remain stable even after long-term culture, demonstrating that these cells are intrinsically activated. Whether or not the activating stimulus is a virus remains unknown so far. SGECs appear to be the initially activated cells in the pathogenesis of SS and other cell types, such as PDCs, or components of the adaptive immune system are activated subsequently via the presentation of autoantigens or transfer of exosomes.
Pattern recognition receptors
The cellular part of the immune system consists of natural killer cells, monocytes, macrophages, granulocytes, dendritic cells and mast cells. The innate immune system responds to antigens in an HLA class II-independent manner. According to the danger model [37], an inflammatory response is initiated by conserved molecular patterns that may be associated with both foreign antigens and cellular components released by damaged cells. In order to recognize the molecular patterns, cells of the innate immune system express receptors able to detect highly conserved pathogen-associated molecular patterns (PAMPs), endogenous components released from damaged cells (danger associated molecular patterns (DAMPs)), also referred to as alarmins [38], and the loss of MHC class I molecules. The receptors recognizing DAMPs and PAMPs are termed pattern recognition receptors (PRRs). So far, several PRRs have been characterized, in particular TLRs, retinoic acid inducible gene (RIG) I-like receptors and NOD-like receptors. TLRs primarily bind to PAMPs in the extracellular space and in endosomes: for example, TLR3 to viral double-stranded RNA, TLR4 to lipopolysaccharide, TLR7 to single-stranded RNA and TLR9 to unmethylated DNA. RIG-1 is an intracellular receptor that binds to nucleic acids, and NOD1 and NOD2 are activated by bacterial peptidoglycans.
According to the danger model, tissue stress (for example, cell necrosis, hypoxia, low pH), and not only exogenous pathogens, can produce danger signals. The activation of antigen-presenting cells via PRRs leads to the upregulation of MHC class I and II and costimulatory molecules and to the secretion of proinflammatory cytokines, such as type I IFN, by PDCs. These factors activate the adaptive immune system, which in turn may produce autoantibodies. In SS, antibodies against SS-A, which is complexed to hYRNA, form immune complexes that can bind and stimulate TLRs. Thus, a vicious cycle may be initiated in which the innate and adaptive immune systems stimulate each other to give a perpetuating autoimmune response.
Genetic studies on the role of PRRs have revealed that SNPs of NOD2 are associated with Crohn's disease [39, 40] and Blau syndrome [41]. With regard to SS, there is so far evidence for a role of TLRs expressed by SGECs, which does not exclude a major role for other PRRs.
Role of Toll-like receptors in primary Sjögren's syndrome
SGECs express TLR3 and other TLRs. In comparison to other cells types, TLR3 is expressed at particularly high levels. In addition, RT-PCR analysis and functional studies revealed transcriptional activation of TLR2, TLR3 and TLR4 in cultured SGECs of patients with primary SS [35]. TLR3 binds double-stranded RNA of viral origin and its synthetic analogue poly(I:C). TLR3 ligation induces the production of proinflammatory cytokines and upregulates BAFF production in SGECs.
The role of TLRs in the pathogenesis of SS has also been addressed by studies in mice. The injection of poly(I:C), a TLR3 agonist, stimulates the production of type I IFN. The treatment rapidly induces a temporal hypofunction of the salivary glands of most mice strains, which recover after termination of the poly(I:C) treatment. Mice deficient in IFNalpha-receptor1 are partially protected. In NZB/W F1 mice, however, which are prone to the development of a lupus-like disease, TLR3 stimulation induces severe sialadenitis [42]. The loss of saliva production precedes lymphocyte infiltration [42]. Four months after the discontinuation of the innate immunity stimulation, a lymphocytic infiltrate developed with formation of lymphoid aggregates in the salivary glands. This animal model of primary SS illustrates the initial sequential activation of innate immunity and the subsequent activation of adaptive immunity.
Stimulation of the adaptive immune system by components of innate immunity
Type I and II IFNs are the main inducers of the production of BAFF. Transgenic mice that overexpress BAFF develop polyarthritis and hallmarks of both SLE and SS, including infiltrates in the salivary glands and reduced saliva production [43]. The concentration of BAFF was found to be increased in the sera of patients with active SS [44], as well as in the salivary glands [45] and the saliva. Increased BAFF production was detected in T cells and monocytes as well as in salivary gland duct cells. Epithelial cells, therefore, are not only a target for the autoimmune response in primary SS, but also important in perpetuating the disease since they can present autoantigens and produce proinflammatory cytokines, including BAFF.
Possible triggers of the IFN signature in primary Sjögren's syndrome
So far, the initial inducer of IFN overproduction and the pathogenesis of SS has remained unclear. The type I IFN signature would be well in line with a viral trigger of the disease. For example, chronic sialadenitis is associated with hepatitis C virus and HIV infection. Epstein-Barr virus, retroviruses, enteroviruses and coxsackievirus have been suggested to induce SS [46], even though there is still no definitive proof of their contribution to the disease.
On the other hand, the female predominance of SS suggests a role of hormones in its pathogenesis. In particular, a role for estrogen deprivation has been suspected, as the disease often starts after menopause. Estrogen-deficient mice develop a disease similar to primary SS [47]. Estrogen deficiency induces aberrant class II MHC expression in exocrine glands via interactions between epithelial cells and PDCs. The expression of MHC class II molecules is increased in the exocrine glands of ovariectomized C57BL/6 (B6) mice compared to control B6 mice. The salivary gland dendritic cells adjacent to the apoptotic epithelial cells become activated. Estrogen deficiency also induces the overexpression of the transcription factor retinoblastoma-associated protein 48 (RbAP48). Mice with transgenic overexpression of RbAp48 develop autoimmune exocrinopathy resembling SS, with ocular and oral dryness, a lymphocytic infiltrate in the salivary and lachrymal glands, and production of autoantibodies typical for SS (anti-SS-A, anti-SS-B, and anti-fodrin). RbAP48 overexpression leads to activation and apoptosis of epithelial cells that express MHC class II molecules and the costimulatory molecules CD80, CD86 and ICAM [48].
Conclusion: current model of the pathophysiology of primary Sjögren's syndrome
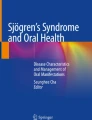
SS appears to be triggered by environmental factors such as viral infection or hypoestrogenism. In patients carrying susceptibility genes predisposing to enhanced reaction of the innate immune system via IFN pathway proteins, epithelial cells become activated and may also produce IFN and other cytokines (Figure 1). Subsequently, autoantigen presentation by the epithelial cells and BAFF overproduction induced by IFN stimulates B- and T-cell activation. Finally, autoantibodies against SS-A/SS-B, alpha-fodrin and muscarinic receptors develop as a sign of the involvement of the adaptive immune system.

Current model of the initiation of the pathogenesis of Sjögren's syndrome. (1) The disease is triggered by either a virus or hypoestrogenism. (2) Salivary gland epithelial cells (SGECs) become activated and start to express MHC class II molecules. (3) The subsequent activation of plasmacytoid dendritic cells (PDCs) induces a high production of proinflammatory cytokines, including IFNalpha, in individuals with the risk alleles of the susceptibility genes IRF5 and STAT4. (4) Under the influence of the high IFN concentration in the glands, TNF family member B cell-activating factor (BAFF) is produced and, together with the autoantigen presentation on SGECs, stimulates the adaptive immune system.
In conclusion, there is increasing evidence that innate immunity, in particular the production of IFNs and the activation of epithelial cells via TLRs, plays a major role in the initiation of the pathophysiology of SS. These findings are encouraging for future trials using anti-IFN antibodies as new biologicals in the treatment of primary SS.
Note
Autoimmune Basis of Rheumatic Diseases
This article is part of a series on Sjögren's syndrome, edited by Thomas Dörner, which can be found online at http://arthritis-research.com/series/Sjogrens
This series forms part of a special collection of reviews covering major autoimmune rheumatic diseases, available at: http://arthritis-research.com/series/abrd
Abbreviations
- bp:
-
base pair
- BAFF:
-
TNF family member B cell-activating factor
- DAMP:
-
danger associated molecular pattern
- ELISA:
-
enzyme-linked immunosorbent assay
- ICAM:
-
intercellular adhesion molecule
- IFN:
-
interferon
- IL:
-
interleukin
- IRF:
-
interferon regulatory factor
- MHC:
-
major histocompatibility complex
- OR:
-
odds ratio
- PAMP:
-
pathogen-associated molecular pattern
- PBMC:
-
peripheral blood mononuclear cell
- PDC:
-
plasmacytoid dendritic cell
- PRR:
-
pattern recognition receptor
- RbAP:
-
retinoblastoma-associated protein
- SGEC:
-
salivary gland epithelial cell
- SLE:
-
systemic lupus erythematosus
- SNP:
-
single nucleotide polymorphism
- SS:
-
Sjögren's syndrome
- STAT:
-
signal transducer and activator of transcription
- TLR:
-
Toll-like receptor
- TNF:
-
tumor necrosis factor.
References
Barnes BJ, Kellum MJ, Field AE, Pitha PM: Multiple regulatory domains of IRF-5 control activation, cellular localization, and induction of chemokines that mediate recruitment of T lymphocytes. Mol Cell Biol. 2002, 22: 5721-5740. 10.1128/MCB.22.16.5721-5740.2002.
Yanai H, Chen HM, Inuzuka T, Kondo S, Mak TW, Takaoka A, Honda K, Taniguchi T: Role of IFN regulatory factor 5 transcription factor in antiviral immunity and tumor suppression. Proc Natl Acad Sci USA. 2007, 104: 3402-3407. 10.1073/pnas.0611559104.
Miceli-Richard C, Comets E, Loiseau P, Puechal X, Hachulla E, Mariette X: Association of an IRF5 gene functional polymorphism with Sjögren's syndrome. Arthritis Rheum. 2007, 56: 3989-3994. 10.1002/art.23142.
Nordmark G, Kristjansdottir G, Theander E, Eriksson P, Brun JG, Wang C, Padyukov L, Truedsson L, Alm G, Eloranta ML, Jonsson R, Rönnblom L, Syvänen AC: Additive effects of the major risk alleles of IRF5 and STAT4 in primary Sjögren's syndrome. Genes Immun. 2009, 10: 68-76. 10.1038/gene.2008.94.
Miceli-Richard C, Gestermann N, Ittah M, Comets E, Loiseau P, Puechal X, Hachulla E, Gottenberg JE, Lebon P, Becquemont L, Mariette X: The CGGGG insertion/deletion polymorphism of the IRF5 promoter is a strong risk factor for primary Sjögren's syndrome. Arthritis Rheum. 2009, 60: 1991-1997. 10.1002/art.24662.
Sigurdsson S, Goring HHH, Kristjansdottir G, Milani L, Nordmark G, Sandling JK, Eloranta M-L, Feng D, Sangster-Guity N, Gunnarsson I, Svenungsson E, Sturfelt G, Jonsen A, Truedsson L, Barnes BJ, Alm G, Ronnblom L, Syvanen A-C: Comprehensive evaluation of the genetic variants of interferon regulatory growth factor 5 (IRF5) reveals a novel 5 bp length polymorphism as strong risk factor for systemic lupus erythematosus. Hum Mol Genet. 2008, 17: 872-881.
Sigurdsson S, Nordmark G, Goring HHH, Lindroos K, Wiman A-C, Sturfelt G, Jonsen A, Rantapaa-Dahlqvist S, Moller B, Kere J, Koskenmies S, Widen E, Eloranta M-L, Julkunen H, Kristjansdottir H, Steinsson K, Alm G, Ronnblom L, Syvanen A-C: Polymorphisms in the tyrosine kinase 2 and interferon regulatory factor 5 genes are associated with systemic lupus erythematosus. Am J Hum Genet. 2005, 76: 528-537. 10.1086/428480.
Sigurdsson S, Padyukov L, Kurreeman FAS, Liljedahl U, Wiman A-C, Alfredsson L, Toes R, Ronnelid J, Klareskog L, Huizinga TWJ, Alm G, Syvanen A-C, Ronnblom L: Association of a haplotype in the promoter region of the interferon regulatory factor 5 gene with rheumatoid arthritis. Arthritis Rheum. 2007, 56: 2202-2210. 10.1002/art.22704.
Dideberg V, Kristjansdottir G, Milani L, Libioulle C, Sigurdsson S, Louis E, Wiman A-C, Vermeire S, Rutgeerts P, Belaiche J, Franchimont D, Van Gossum A, Bours V, Syvanen A-C: An insertion-deletion polymorphism in the interferon regulatory factor 5 (IRF5) gene confers risk of inflammatory bowel diseases. Hum Mol Genet. 2007, 16: 3008-3016. 10.1093/hmg/ddm259.
Frucht DM, Aringer M, Galon J, Danning C, Brown M, Fan S, Centola M, Wu C-Y, Yamada N, Gabalaway HE, O'Shea JJ: Stat4 is expressed in activated peripheral blood monocytes, dendritic cells, and macrophages at sites of Th1-mediated inflammation. J Immunol. 2000, 164: 4659-4664.
Korman BD, Alba MI, Le JM, Alevizos I, Smith JA, Nikolov NP, Kastner DL, Remmers EF, Illei GG: Variant form of STAT4 is associated with primary Sjögren's syndrome. Genes Immun. 2008, 9: 267-270. 10.1038/gene.2008.1.
Palomino-Morales RJ, Diaz-Gallo LM, Witte T, Anaya JM, Martín J: Influence of STAT4 polymorphism in primary Sjögren's syndrome. J Rheumatol. 2010, 37: 1016-1019. 10.3899/jrheum.091007.
Gestermann N, Mekinian A, Comets E, Loiseau P, Puechal X, Hachulla E, Gottenberg JE, Mariette X, Miceli-Richard C: STAT4 is a confirmed genetic risk factor for Sjögren's syndrome and could be involved in type 1 interferon pathway signaling. Genes Immun. 2010, 11: 432-438. 10.1038/gene.2010.29.
Remmers EF, Plenge RM, Lee AT, Graham RR, Hom G, Behrens TW, de Bakker PI, Le JM, Lee HS, Batliwalla F, Li W, Masters SL, Booty MG, Carulli JP, Padyukov L, Alfredsson L, Klareskog L, Chen WV, Amos CI, Criswell LA, Seldin MF, Kastner DL, Gregersen PK: STAT4 and the risk of rheumatoid arthritis and systemic lupus erythematosus. N Engl J Med. 2007, 357: 977-986. 10.1056/NEJMoa073003.
Gateva V, Sandling JK, Hom G, Taylor KE, Chung SA, Sun X, Ortmann W, Kosoy R, Ferreira RC, Nordmark G, Gunnarsson I, Svenungsson E, Padyukov L, Sturfelt G, Jönsen A, Bengtsson AA, Rantapää-Dahlqvist S, Baechler EC, Brown EE, Alarcón GS, Edberg JC, Ramsey-Goldman R, McGwin G, Reveille JD, Vilá LM, Kimberly RP, Manzi S, Petri MA, Lee A, Gregersen PK, et al: A large-scale replication study identifies TNIP1, PRDM1, JAZF1, UHRF1BP1 and IL10 as risk loci for systemic lupus erythematosus. Nat Genet. 2009, 41: 1228-1233. 10.1038/ng.468.
Han JW, Zheng HF, Cui Y, Sun LD, Ye DQ, Hu Z, Xu JH, Cai ZM, Huang W, Zhao GP, Xie HF, Fang H, Lu QJ, Xu JH, Li XP, Pan YF, Deng DQ, Zeng FQ, Ye ZZ, Zhang XY, Wang QW, Hao F, Ma L, Zuo XB, Zhou FS, Du WH, Cheng YL, Yang JQ, Shen SK, Li J, et al: Genome-wide association study in a Chinese Han population identifies nine new susceptibility loci for systemic lupus erythematosus. Nat Genet. 2009, 41: 1234-1237. 10.1038/ng.472.
Martínez A, Varadé J, Márquez A, Cénit MC, Espino L, Perdigones N, Santiago JL, Fernández-Arquero M, de la Calle H, Arroyo R, Mendoza JL, Fernández-Gutiérrez B, de la Concha EG, Urcelay E: Association of the STAT4 gene with increased susceptibility for some immune-mediated diseases. Arthritis Rheum. 2008, 58: 2598-2602. 10.1002/art.23792.
Rueda B, Broen J, Simeon C, Hesselstrand R, Diaz B, Suárez H, Ortego-Centeno N, Riemekasten G, Fonollosa V, Vonk MC, van den Hoogen FH, Sanchez-Román J, Aguirre-Zamorano MA, García-Portales R, Pros A, Camps MT, Gonzalez-Gay MA, Coenen MJ, Airo P, Beretta L, Scorza R, van Laar J, Gonzalez-Escribano MF, Nelson JL, Radstake TR, Martin J: The STAT4 gene influences the genetic predisposition to systemic sclerosis phenotype. Hum Mol Genet. 2009, 18: 2071-2077. 10.1093/hmg/ddp119.
Abelson AK, Delgado-Vega AM, Kozyrev SV, Sánchez E, Velázquez-Cruz R, Eriksson N, Wojcik J, Linga Reddy MV, Lima G, D'Alfonso S, Migliaresi S, Baca V, Orozco L, Witte T, Ortego-Centeno N, AADEA group, Abderrahim H, Pons-Estel BA, Gutiérrez C, Suárez A, González-Escribano MF, Martin J, Alarcón-Riquelme ME: STAT4 associates with systemic lupus erythematosus through two independent effects that correlate with gene expression and act additively with IRF5 to increase risk. Ann Rheum Dis. 2009, 68: 1746-1753. 10.1136/ard.2008.097642.
Sigurdsson S, Nordmark G, Garnier S, Grundberg E, Kwan T, Nilsson O, Eloranta ML, Gunnarsson I, Svenungsson E, Sturfelt G, Bengtsson AA, Jönsen A, Truedsson L, Rantapää-Dahlqvist S, Eriksson C, Alm G, Göring HH, Pastinen T, Syvänen AC, Rönnblom L: A risk haplotype of STAT4 for systemic lupus erythematosus is over-expressed, correlates with anti-dsDNA and shows additive effects with two risk alleles of IRF5. Hum Mol Genet. 2008, 17: 2868-2876. 10.1093/hmg/ddn184.
Höss M, Robins P, Naven TJ, Pappin DJ, Sgouros J, Lindahl T: A human DNA editing enzyme homologous to the Escherichia coli DnaQ/MutD protein. EMBO J. 1999, 18: 3868-3875. 10.1093/emboj/18.13.3868.
Crow YJ, Hayward BE, Parmar R, Robins P, Leitch A, Ali M, Black DN, van Bokhoven H, Brunner HG, Hamel BC, Corry PC, Cowan FM, Frints SG, Klepper J, Livingston JH, Lynch SA, Massey RF, Meritet JF, Michaud JL, Ponsot G, Voit T, Lebon P, Bonthron DT, Jackson AP, Barnes DE, Lindahl T: Mutations in the gene encoding the 3'-5' DNA exonuclease TREX1 cause Aicardi-Goutières syndrome at the AGS1 locus. Nat Genet. 2006, 38: 917-920. 10.1038/ng1845.
Lee-Kirsch MA, Chowdhury D, Harvey S, Gong M, Senenko L, Engel K, Pfeiffer C, Hollis T, Gahr M, Perrino FW, Lieberman J, Hubner N: A mutation in TREX1 that impairs susceptibility to granzyme A-mediated cell death underlies familial chilblain lupus. J Mol Med. 2007, 85: 531-537. 10.1007/s00109-007-0199-9.
Lee-Kirsch MA, Gong M, Chowdhury D, Senenko L, Engel K, Lee YA, de Silva U, Bailey SL, Witte T, Vyse TJ, Kere J, Pfeiffer C, Harvey S, Wong A, Koskenmies S, Hummel O, Rohde K, Schmidt RE, Dominiczak AF, Gahr M, Hollis T, Perrino FW, Lieberman J, Hübner N: Mutations in the gene encoding the 3'-5' DNA exonuclease TREX1 are associated with systemic lupus erythematosus. Nat Genet. 2007, 39: 1065-1067. 10.1038/ng2091.
Stetson DB, Ko JS, Heidmann T, Medzhitov R: Trex1 prevents cell-intrinsic initiation of autoimmunity. Cell. 2008, 134: 587-598. 10.1016/j.cell.2008.06.032.
Morita M, Stamp G, Robins P, Dulic A, Rosewell I, Hrivnak G, Daly G, Lindahl T, Barnes DE: Gene-targeted mice lacking the Trex1 (DNase III) 3'→5' DNA exonuclease develop inflammatory myocarditis. Mol Cell Biol. 2004, 24: 6719-6727. 10.1128/MCB.24.15.6719-6727.2004.
Hjelmervik TO, Petersen K, Jonassen I, Jonsson R, Bolstad AI: Gene expression profiling of minor salivary glands clearly distinguishes primary Sjögren's syndrome patients from healthy control subjects. Arthritis Rheum. 2005, 52: 1534-1544. 10.1002/art.21006.
Gottenberg JE, Cagnard N, Lucchesi C, Letourneur F, Mistou S, Lazure T, Jacques S, Ba N, Ittah M, Lepajolec C, Labetoulle M, Ardizzone M, Sibilia J, Fournier C, Chiocchia G, Mariette X: Activation of IFN pathways and plasmacytoid dendritic cell recruitment in target organs of primary Sjögren's syndrome. Proc Natl Acad Sci USA. 2006, 103: 2770-2775. 10.1073/pnas.0510837103.
Emamian ES, Leon JM, Lessard CJ, Grandits M, Baechler EC, Gaffney PM, Segal B, Rhodus NL, Moser KL: Peripheral blood gene expression profiling in Sjögren's syndrome. Genes Immun. 2009, 10: 285-296. 10.1038/gene.2009.20.
Båve U, Nordmark G, Lövgren T, Rönnelid J, Cajander S, Eloranta ML, Alm GV, Rönnblom L: Activation of the type I interferon system in primary Sjögren's syndrome: a possible etiopathogenic mechanism. Arthritis Rheum. 2005, 52: 1185-1195. 10.1002/art.20998.
Mavragani CP, Niewold TB, Moutsopoulos NM, Pillemer SR, Wahl SM, Crow MK: Augmented interferon-alpha pathway activation in patients with Sjögren's syndrome treated with etanercept. Arthritis Rheum. 2007, 56: 3995-4004. 10.1002/art.23062.
Manoussakis MN, Moutsopoulos HM: Sjögren's syndrome: autoimmune epithelitis. Baillieres Best Pract Res Clin Rheumatol. 2000, 14: 73-95. 10.1053/berh.1999.0078.
Skopouli FN, Moutsopoulos HM: Autoimmune epithelitis: Sjögren's syndrome. Clin Exp Rheumatol. 1994, 12 (Suppl 11): S9-11.
Yannopoulos DI, Roncin S, Lamour A, Pennec YL, Moutsopoulos HM, Youinou P: Conjunctival epithelial cells from patients with Sjögren's syndrome inappropriately express major histocompatibility complex molecules, La (SS-B) antigen, and heat-shock proteins. J Clin Immunol. 1992, 12: 259-265. 10.1007/BF00918149.
Deshmukh US, Nandula SR, Thimmalapura PR, Scindia YM, Bagavant H: Activation of innate immune responses through Toll-like receptor 3 causes a rapid loss of salivary gland function. J Oral Pathol Med. 2009, 38: 42-47.
Kapsogeorgou EK, Abu-Helu RF, Moutsopoulos HM, Manoussakis MN: Salivary gland epithelial cell exosomes: a source of autoantigenic ribonucleoproteins. Arthritis Rheum. 2005, 52: 1517-1521. 10.1002/art.21005.
Matzinger P: The danger model: a renewed sense of self. Science. 2002, 296: 301-305. 10.1126/science.1071059.
Oppenheim JJ, Yang D: Alarmins: chemotactic activators of immune responses. Curr Opin Immunol. 2005, 17: 359-365. 10.1016/j.coi.2005.06.002.
Ogura Y, Bonen DK, Inohara N, Nicolae DL, Chen FF, Ramos R, Britton H, Moran T, Karaliuskas R, Duerr RH, Achkar JP, Brant SR, Bayless TM, Kirschner BS, Hanauer SB, Nuñez G, Cho JH: A frameshift mutation in NOD2 associated with susceptibility to Crohn's disease. Nature. 2001, 411: 603-606. 10.1038/35079114.
Hugot JP, Chamaillard M, Zouali H, Lesage S, Cézard JP, Belaiche J, Almer S, Tysk C, O'Morain CA, Gassull M, Binder V, Finkel Y, Cortot A, Modigliani R, Laurent-Puig P, Gower-Rousseau C, Macry J, Colombel JF, Sahbatou M, Thomas G: Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn's disease. Nature. 2001, 411: 599-603. 10.1038/35079107.
Miceli-Richard C, Lesage S, Rybojad M, Prieur AM, Manouvrier-Hanu S, Häfner R, Chamaillard M, Zouali H, Thomas G, Hugot JP: CARD15 mutations in Blau syndrome. Nat Genet. 2001, 29: 19-20. 10.1038/ng720.
Spachidou MP, Bourazopoulou E, Maratheftis CI, Kapsogeorgou EK, Moutsopoulos HM, Tzioufas AG, Manoussakis MN: Expression of functional Toll-like receptors by salivary gland epithelial cells: increased mRNA expression in cells derived from patients with primary Sjögren's syndrome. Clin Exp Immunol. 2007, 147: 497-503. 10.1111/j.1365-2249.2006.03311.x.
Groom J, Kalled SL, Cutler AH, Olson C, Woodcock SA, Schneider P, Tschopp J, Cachero TG, Batten M, Wheway J, Mauri D, Cavill D, Gordon TP, Mackay CR, Mackay F: Association of BAFF/BLyS overexpression and altered B cell differentiation with Sjögren's syndrome. J Clin Invest. 2002, 109: 59-68.
Mariette X, Roux S, Zhang J, Bengoufa D, Lavie F, Zhou T, Kimberly R: The level of BLyS (BAFF) correlates with the titre of autoantibodies in human Sjogren's syndrome. Ann Rheum Dis. 2003, 62: 168-171. 10.1136/ard.62.2.168.
Daridon C, Devauchelle V, Hutin P, Le Berre R, Martins-Carvalho C, Bendaoud B, Dueymes M, Saraux A, Youinou P, Pers JO: Aberrant expression of BAFF by B lymphocytes infiltrating the salivary glands of patients with primary Sjogren's syndrome. Arthritis Rheum. 2007, 56: 1134-1144. 10.1002/art.22458.
Triantafyllopoulou A, Tapinos N, Moutsopoulos HM: Evidence for coxsackievirus infection in primary Sjogren's syndrome. Arthritis Rheum. 2004, 50: 2897-2902. 10.1002/art.20463.
Arakaki R, Nagaoka A, Ishimaru N, Yamada A, Yoshida S, Hayashi Y: Role of plasmacytoid dendritic cells for aberrant class II expression in exocrine glands from estrogen-deficient mice of healthy background. Am J Pathol. 2009, 174: 1715-1724. 10.2353/ajpath.2009.080695.
Ishimaru N, Arakaki R, Yoshida S, Yamada A, Noji S, Hayashi Y: Expression of the retinoblastoma protein RbAp48 in exocrine glands leads to Sjögren's syndrome-like autoimmune exocrinopathy. J Exp Med. 2008, 205: 2915-2927. 10.1084/jem.20080174.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
About this article
Cite this article
Low, H.Z., Witte, T. Aspects of innate immunity in Sjögren's syndrome. Arthritis Res Ther 13, 218 (2011). https://doi.org/10.1186/ar3318
Published:
DOI: https://doi.org/10.1186/ar3318