
Abstract
During the decade since the launch of Arthritis Research, the application of gene therapy to the rheumatic diseases has experienced the same vicissitudes as the field of gene therapy as a whole. There have been conceptual and technological advances and an increase in the number of clinical trials. However, funding has been unreliable and a small number of high-profile deaths in human trials, including one in an arthritis gene therapy trial, have provided ammunition to skeptics. Nevertheless, steady progress has been made in a number of applications, including rheumatoid arthritis and osteoarthritis, Sjögren syndrome, and lupus. Clinical trials in rheumatoid arthritis have progressed to phase II and have provided the first glimpses of possible efficacy. Two phase I protocols for osteoarthritis are under way. Proof of principle has been demonstrated in animal models of Sjögren syndrome and lupus. For certain indications, the major technological barriers to the development of genetic therapies seem to have been largely overcome. The translational research necessary to turn these advances into effective genetic medicines requires sustained funding and continuity of effort.
Similar content being viewed by others

Introduction
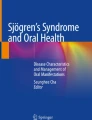
When Arthritis Research was launched, the field of gene therapy was going from strength to strength. The preceding decade had seen the number of human gene therapy trials grow, since the first properly authorized gene transfer to a human in 1989, to a total of 368 by 1998. Despite the worst predictions of the skeptics, there had been no serious adverse events and the field looked forward, like the economy that was fuelling much speculation in the area, to continued rapid growth. Optimists predicted that the first genetic medicines would be on the market within a few years. Rheumatoid arthritis (RA) had become an early target for gene therapy (Figure 1), capturing the optimism of the early 1990s and beginning clinical trials in 1996. The first International Meeting on the Gene Therapy of Arthritis and Related Disorders (GTARD) was held at the National Institutes of Health (NIH) (Bethesda, MD, USA) in 1998 [1] and attracted over 200 participants.

English language publications on arthritis gene therapy in the refereed literature. The data are based on a PubMed search using 'arthritis gene therapy' as the search term. The first paper on arthritis gene therapy was published in 1992 [27]. The first efficacy data for animal models of rheumatoid arthritis (RA) appeared in 1996 [103, 104], and the first efficacy data for animal models of osteoarthritis (OA) followed a year later [79]. The first human trial for RA began in 1996 [29]. Seven clinical trials for RA and OA have been initiated, one of them reaching phase II (Table 1). The first evidence of possible clinical responses to gene transfer was published this year [31]. Reprinted with permission [105].
Matters then changed abruptly. The 1999 death of Jesse Gelsinger [2] reopened safety concerns. This, in turn, made it more difficult to obtain funding from traditional sources, such as the NIH, as well as the biotechnology industry, which was also dealing with a rapidly slowing economy. Many rheumatic diseases, though serious, are not considered to be life-threatening, a factor that further reduced enthusiasm for gene therapy research in this area under these circumstances.
Although the first flush of enthusiasm is over, the past decade has seen steady progress in developing genetic therapies for several conditions, and the number of clinical trials worldwide is approaching 1,500. The first commercial gene therapeutic, Gendicin for cancer of the head and neck, has been launched in China [3], and gene therapy for familial lipoprotein lipase deficiency is available as an orphan drug in Europe and the US. Cures have been reported for X-linked severe combined immunodeficiency disease (SCID) [4], adenosine deaminase-SCID [5], and X-linked chronic granulomatous disease [6]. Striking success in treating Leber's congenital amaurosis has recently been reported by two independent groups [7, 8].
There has also been steady growth of research into developing gene therapies for the rheumatic diseases. Progress can be gauged, to some degree, by reading the summaries of the biennial GTARD meetings [1, 9, 10]. These, too, have reached their 10th anniversary and GTARD-5 was recently held in Seattle. As discussed below, there have been a number of clinical trials in the area of arthritis gene therapy, one of which has entered phase II, and some other areas are in an advanced preclinical stage of development.
Advances in technology
Central to any successful gene therapy is the ability to transfer genes efficiently and safely to the target cells. The same basic viral and nonviral vectors available now were available 10 years ago, but there have been developments in their engineering and application.
Viral vectors
Although oncoretroviruses, such as the Moloney murine leukemia virus, were the first to be used in clinical trials and dominated applications in human gene therapy for some years, they are less popular now. Pseudotyping the retroviral coat has overcome, to some degree, the problem of modest titers, but the inconvenience and expense of ex vivo gene transfer remain. Furthermore, the occurrence of insertional mutagenesis during human gene therapy trials [11] has generated a huge barrier to the use of oncoretroviruses in nonlethal nonmendelian diseases. The US Food and Drug Administration (FDA), for example, requires a 15-year follow-up on all clinical trials using integrating vectors.
Because lentivirus vectors are also integrating retroviruses, they are covered by the same restrictions. This is unfortunate because vesicular stomatitis virus-pseudotyped lentiviruses are extremely efficient and do not require host cell division; they transduce synovium very effectively after intra-articular injection [12, 13]. Although lentiviruses are being engineered to remain episomal, their human use in rheumatology seems unlikely within any reasonable time frame.
Adenovirus vectors have overtaken retroviruses as the most commonly used in human clinical trials. Indeed, the first commercially available gene therapeutic, Gendicine [3], which is available in China for cancer, uses adenovirus. Engineering adenovirus vectors has taken the direction of deleting larger and larger segments of the viral genome, leading to high-capacity 'gutted' vectors that lack all viral coding sequences [14]. This reduces the immunogenicity of transduced cells, but not that of the virions themselves. Although gutted adenovirus vectors have several advantages, including a theoretical carrying capacity of over 30 kb, they are difficult to produce and purify. Other modifications to adenovirus include mutating coat proteins to enhance transduction efficiency or to alter tropism. The inclusion of an arginine-glycine-aspartate sequence, for instance, greatly enhances the transduction of synovium [15].
Adeno-associated virus (AAV) has seen the greatest recent development. AAV was previously hampered by difficulties in manufacturing large amounts of clinical-grade vector and modest levels of transgene expression in many cell types. The latter reflects, in part, the single-stranded DNA genome of AAV, which requires the host cell to synthesize a complementary second strand; this process is inefficient in many cells.
The production problems have been eased by new technologies to facilitate the generation of recombinant AAV [16]. Most significantly, transgene expression has been made much higher, quicker, and more reliable by the development of self-complementary (sc) vectors containing positive- and negative-strand viral genomes linked at one terminal repeat [17]. The drawback is that the packaging capacity is reduced by half to about 2 kb. Nevertheless, many of the cytokines and other modulatory molecules of interest in rheumatic diseases have cDNAs that are small enough to fit into this space. Recent data confirm the superiority of scAAV as a means of transferring genes to joints and expressing them intra-articularly [18].
There has been a rapid increase in the number of different recombinant AAV serotypes [19]. Some of these offer altered tropisms and enhanced transduction efficiencies. AAV1, for instance, has a much greater ability to transduce skeletal muscle than the prototypical AAV2 serotype [20]. It is unclear which, if any, of these new serotypes will find applications in rheumatology, although this is an active area of research (see next section).
Until recently, little attention was paid to the immune reaction to AAV given its perceived low immunogenicity. This rapidly changed when data from a clinical trial using AAV to treat hemophilia noted a neutralizing immune reaction [21] involving the generation of cytotoxic T lymphocytes [22]. This led to transient transaminitis and curtailed transgene expression. In light of these sorts of findings, the immune response to AAV is undergoing reevaluation.
The perceived safety of AAV vectors has also contributed to their increased popularity. As noted, vector-related deaths have occurred in trials using recombinant retrovirus and adenovirus. Although a fatality occurred last year in an arthritis trial using recombinant AAV [23], the FDA determined that the vector was not to blame and allowed the trial to continue. The number of human trials using AAV has risen to over 50, most of these being approved in the last few years. Two large phase III trials for prostate cancer using AAV are under way. As noted earlier, orphan drug status has been granted for AAV-mediated gene therapy for familial lipoprotein lipase deficiency, and eyesight has been restored to patients with Leber's congentital amaurosis using AAV vectors [7, 8].
Although a number of other viral vectors have been used in clinical trials, they are less relevant to rheumatic diseases. Herpes simplex virus, for instance, is still troubled by cytotoxicity and its use is increasingly restricted to the nervous system, where it has a natural latency. Viral vectors are reviewed in reference [24].
Nonviral vectors
Nonviral vectors continue to be of interest because they are simpler, safer, and less expensive than viruses and offer very large carrying capacities. The simplest vectors are plasmids. Transfection efficiency can be increased by associating the DNA with a carrier, such as a liposome or a polymer, or through the use of a physical stimulus, such as an electric pulse (electroporation). Although a very large number of formulations exist, nonviral gene delivery (transfection) remains much less efficient than viral gene delivery (transduction) and this remains a barrier to its wider use. Despite this, nonviral vectors remain of interest because of persistent reports in the refereed literature of success when using them to treat animal models of rheumatic disease (discussed in the next sections). Nonviral vectors are reviewed in reference [25].
Applications in rheumatic diseases
Rheumatoid arthritis
Local therapy
Interest in applying gene therapy to the treatment of rheumatic diseases began in the early 1990s with attempts to deliver cDNAs to the synovial linings of joints [26, 27]. The basic premise is quite simple (Figure 2). The sustained intra-articular expression of a cDNA encoding a secreted anti-arthritic product will treat the joint locally without the need for readministration and avoid the peaks and troughs of traditional routes of drug delivery. No competing technology is able to do this. If gene transfer is sufficiently efficient, cDNAs encoding nonsecreted products are also possible. Treating individual diseased joints rather than the entire patient reduces costs and lowers opportunities for adverse systemic side effects. A number of different types of transgene have been suggested for this purpose, including those encoding cytokine antagonists, immunomodulators, antiangiogenic factors, apoptotic agents, antioxidants, inhibitors of mitosis, as well as molecules that modulate cell signalling and the activities of transcription factors (reviewed in [28]).

By the time the first issue of Arthritis Research appeared, a phase I clinical trial was under way (Figure 1 and Table 1). This used a retrovirus (MFG-IRAP) to deliver the human interleukin-1 receptor antagonist (IL-1Ra) cDNA by an ex vivo protocol to the metacarpophalangeal (MCP) joints of patients with advanced RA [29]. Among the strict safety requirements of this study was the need to recruit subjects who needed MCP joint replacement surgery, so that the genetically modified cells could be surgically removed 1 week after injection.
This study confirmed that genes could be safely transferred to human rheumatoid joints and expressed within them, at least for 1 week [30]. Although several subjects reported symptomatic improvement, the study was not designed to measure efficacy. A small similar German study, involving just two subjects, is thus of interest because it included preliminary outcome measures based on pain and swelling, using a joint that did not receive the IL-1Ra cDNA as an intrapatient control. Both subjects responded to gene transfer, one of them dramatically so, and the clinical improvement lasted for the entire 4 weeks of the study, despite one subject experiencing flares in nontreated joints [31].
The occurrence of leukemia in humans as a result of insertional mutagenesis using retrovirus vectors, coupled to the high cost of ex vivo gene therapy using passaged autologous cells, has curtailed future trials of this kind. Instead, investigators are concentrating on in vivo gene delivery to joints. Based upon promising preclinical data in rabbits [32], Roessler and colleagues treated one subject with plasmid DNA encoding herpes simplex virusthymidine kinase and followed this with administration of ganciclovir to effect a genetic synovectomy. Although there were no adverse events associated with this procedure, the trial overlapped with the death of Jesse Gelsinger in 1999, which hindered recruitment, and the study was terminated. Since then, the emphasis for in vivo delivery to joints has shifted to AAV for the reasons described in the previous section.
There have been two clinical trials using AAV, both sponsored by Targeted Genetics Corporation (Seattle, WA, USA). The vector (tgAAC94) comprises AAV2 with a single-stranded DNA genome encoding etanercept. Expression is driven by a human cytomegalovirus immediate early promoter. The trials have been discussed in detail [23]. In the first phase I study, 14 subjects with RA and 1 with ankylosing spondylitis were administered vector [33]. Fourteen knee joints and one ankle were injected with 1010 or 1011 virus particles per milliliter; knee joints received 5 mL and the ankle received 2 mL. A subsequent phase I/II study enrolled 127 subjects with a dose escalation of 1011, 1012, or 1013 virions per milliliter to be injected into symptomatic knee, ankle, wrist, MCP, or elbow joints. The protocol allowed subjects to receive a second injection of tgAAC94.
The phase I/II trial attracted considerable attention last year when a subject died soon after receiving a second injection of vector into her knee joint [23]. The case aroused controversy because, in addition to receiving cDNA encoding etanercept, the subject was on adalimumab, having previously taken etanercept until this was discontinued because of a flare. The subject died from histoplasmosis, a known risk factor with anti-tumor necrosis factors (anti-TNFs), in conjunction with a massive retroperitoneal hematoma. After a lengthy investigation by the FDA and the Recombinant DNA Advisory Committee of the NIH, the trial was allowed to proceed in a slightly modified fashion. Preliminary efficacy data suggest that some subjects had symptomatic improvement in response to the gene treatment [34].
A number of groups are now interested in using AAV to deliver genes to joints. Research is focusing on the choice of serotype and the host immune response to the vectors. Serotypes 1, 2, 5, and 8 have attracted the most scrutiny. According to Apparailly and colleagues [35], AAV5 is superior to AAV1 or 2 in the knee joints of mice. This was confirmed in rats, and AAV2 and 5 were shown to have equal efficiency in transducing cultures of human synovial fibroblasts [36]. Another study indicates the following order of preference: AAV2 > 1 > 5 > 8 [37]. However, when human synovial fluids were screened for pre-existing immunity to AAV, neutralizing antibodies to serotypes 1 and 2 were more common than antibodies to serotype 5, suggesting to Boissier and colleagues [37] that AAV5 may be more useful in humans, despite lower transduction efficiency. Humoral reactions to AAV2 were noted in the trial of tgAAC94, mentioned above, but possible cell-mediated immunity was not measured. Studies of AAV2-mediated gene delivery to the knee joints of rabbits confirm a neutralizing immune reaction that prevents redosing [18]. AAV has been used to express soluble TNF receptors [38], beta interferon (IFN-β) [39], angiostatin [40], dominant negative Iκκβ (inhibitor of kappa B kinase β) [41], and IL-1Ra [18] in the joints of experimental animals, with an associated antiarthritic effect.
In most species, conventional AAV vectors containing a single-stranded DNA genome have only a modest ability to transduce articular tissues. Transduction efficiency can be enhanced by irradiation, a process that provokes second-strand synthesis [42]. The need for the latter can be obviated with the use of scAAV, and recent findings confirm the superiority of these vectors in the rabbit knee joint [18]. According to data from the same study, only 10% to 20% of AAV genomes that enter synovial fibroblasts appear in the nucleus. This identifies a second constraint to transduction efficiency that helps to account for the relatively high number of AAV virions (104 to 105 particles per cell) needed for useful levels of transgene expression. Proteosome inhibitors improve the nuclear uptake of AAV genomes in human synovial cells, leading to greatly enhanced transgene expression [43]. In agreement with this, mutations to the AAV coat protein that prevent ubiquitination also increase transduction efficiency [44]. According to Traister and colleagues [45], transgene expression from AAV vectors is increased in human synovial fibroblasts in the presence of inflammatory cytokines. A similar effect was reported some years ago by Pan and colleagues [46, 47] in rat knee joints but this has been difficult to reproduce [18].
For intra-articular gene therapy to be a clinical success, there is a need for extended periods of transgene expression. This has proved difficult in animal models. Recent work by Gouze and colleagues [48] identified immune reactions to non-homologous proteins as the major barrier to prolonged transgene expression. Using the rat knee joint as a model system, they showed that cDNA encoding a rat protein delivered by an immunologically silent vector can be expressed in a stable prolonged fashion. Of interest, long-term transgene expression does not require an integrating vector and is independent of the promoter. Instead, it relies on the presence of long-lived nonmitotic cells within certain dense collagenous tissues in and around the joint (Figure 3).

Fibroblasts resident in fibrous articular tissues support stable expression of exogenous transgenes. Following intra-articular injection of lentivirus-GFP or Ad.GFP into the knees of nude rats, groups of animals were sacrificed at days 5 and 168. The knee joints and surrounding tissues were harvested intact, decalcified, and processed for histology. For each joint, the approximate positions of fluorescent cells identified in serial, sagittal whole-knee sections were tabulated in green on knee joint diagrams similar to those shown on the left. The diagrams shown are representative of the results observed with both viruses at the respective times. On the right, images characteristic of the appearance of the GFP+ cells in tissue sections at the different times are shown (×20 magnification). Lines indicate the approximate regions represented by the tissue sections. The numbers of GFP+ cells in the synovium and subsynovium were reduced dramatically at day 168. The density and distribution of GFP+ cells in the tendon, ligament, and fibrous synovium were largely unchanged over the duration of the experiment. No fluorescent cells were seen in the articular cartilage with either virus at any time point. B, bone; GFP, green fluorescent protein; M, muscle; P, patella. Reprinted with permission [48].
An ability to achieve long-term transgene expression opens the way for regulated expression. Two approaches have been investigated. One makes use of endogenous cues to ensure that the level of expression tracks disease activity within the joint. These strategies use inducible promoters based upon upstream regulatory sequences that control the expression of acute-phase proteins and inflammatory cytokines, such as IL-1 and IL-6 [38, 49, 50]. A related method uses a sequence containing multiple nuclear factor-kappa-B (NF-κB)-binding sites [38]. A second approach to regulated transgene expression uses exogenous molecules, such as doxycyline, to manipulate the level of production [51–53]. The latter approach provides greater insurance against inappropriate transgene expression as might occur during an infection. Though not strictly gene therapy, a related clinical trial injects decoy oligonucleotides that inhibit the activity of the transcription factor NF-κB into rheumatoid joints [54]. So far, there have been no adverse events and some evidence of a clinical response in certain subjects (Tetsuya Tomita, personal communication).
Systemic therapy
In a polyarticular condition such as RA, an intra-articular gene therapy might require the injection of large numbers of joints. Moreover, a local gene therapy might not address systemic extra-articular manifestations of the disease. Thus, there is interest in a more general approach to therapy in which a transgene is introduced into a site where a secreted gene product will have access to the systemic circulation (Figure 2). Proof of principle has been established using intramuscular, intravenous, intraperitoneal, and subcutaneous routes of delivery by in vivo and ex vivo methods (reviewed in [28]). Although this approach has obvious attractions, it provides only an incremental advance over what is already achieved by traditional methods of protein delivery and is accompanied by increased risk of adverse events. For these reasons, it has not achieved widespread popularity. One interesting possible exception, however, is the parenteral administration of naked DNA.
There are several reports in the refereed literature ascribing potent antiarthritic properties to plasmid DNA when delivered by intramuscular, intraperitoneal, intravenous, and intranasal routes [55–61]. Because levels of transgene expression are low when DNA is administered in these ways, an alternative explanation for their efficacy in animal models of RA is needed. One possibility is the uptake of DNA by antigen-presenting cells (APCs) which then travel to sites of antigen presentation where sufficient transgene is expressed to modulate immune reactivity locally. This is an example of facilitated local therapy, described in the next section.
DNA can also be used to vaccinate. There are several examples using animal models of RA in which DNA vaccines that express arthritogenic antigens, such as heat-shock proteins [62], or mediators of arthritis, such as TNF [63], are protective. It is also possible to induce tolerance by DNA immunization in the absence of adjuvant [64]. Though effective in animal models, such strategies may be risky in humans.
Facilitated local therapy
The ability to target multiple diseased joints selectively by a single parenteral injection is known as facilitated local therapy (Figure 2). This was first noted as a contralateral therapeutic effect in the knee joints of rabbits with bilateral antigen-induced arthritis [65]. It occurs with both in vivo and ex vivo [66] gene delivery and is thought to reflect immune modulation via APCs that are exposed to appropriate transgene products as they present arthritogenic antigens to T lymphocytes (Figure 4).

A model based upon trafficking of antigen-presenting cells (APCs) to explain the contralateral effect. Introduction of a suitable vector, in this example one encoding viral interleukin-10 (vIL-10), into an inflamed joint transduces synovium and APCs. Lymphocytes are very difficult to transduce, as reflected in the figure. Intra-articular antigen presentation thus occurs in the presence of a high local concentration of vIL-10 produced by the synovium, the APC, or both. Under these conditions, the immune response deviates toward a therapeutic Th2 response. Lymphocytes and APCs then traffic to other joints via the blood stream or lymphatics, where they suppress disease. Reprinted with permission [28].
Studies using the murine delayed-type hypersensitivity reaction as a model [67] showed that genetically modified dendritic cells and macrophages could migrate to sites of inflammation and inhibit immune-driven pathology in an antigen-specific manner. In subsequent studies, dendritic cells expressing IL-4 were shown to migrate to the paws of MHC-matched mice with collagen-induced arthritis and quell disease activity, even in established disease [68]. The anti-arthritic effect was stronger than when the same adenovirus vector was used to deliver IL-4 systemically. A variety of additional transgenes, including IL-10, indoleamine 2,3-dioxy-genase, and IκB (inhibitor of kappa-B), are effective in this manner.
A related strategy produces selective ablation of autoreactive T lymphocytes by modifying APCs to express inducers of apoptosis on their cell surfaces. When the APC expresses an arthritogenic antigen to reactive T lymphocytes, the latter undergo apoptosis. Although this has been shown in murine models using Fas ligand [69, 70] as the transgene, TRAIL (tumor necrosis factor-related apoptosis-inducing ligand) is a better candidate because its receptor has more limited distribution, thus reducing opportunities for unwanted side effects. Impressive proof of principle has been demonstrated in murine collagen-induced arthritis using dendritic cells that express TRAIL [71]. The therapeutic effect was improved by pulsing the dendritic cells with type II collagen before injection. The equivalent manipulation in RA will be complicated because the inciting antigens are not known, although a regulatory bystander effect could be achieved. The response to TRAIL gene transfer is enhanced when RNA interference is used to knock down expression of its decoy receptor, DcR2 [72].
T lymphocytes also home to sites of inflammation and immune reactivity. Like APCs, they may be genetically modified and used to target multiple sites of disease by parenteral administration, although lymphocytes are more difficult to transduce than APCs. However, proof of principle has been shown in several animal experiments using IL-4, IL-10, IL-12 p40, and anti-TNF single-chain antibody as transgenes [73, 74]. In most animal models, the arthritogenic antigen is known and T lymphocytes with the appropriate T-cell receptor can be used to maximize the effect. In RA, however, the inciting antigen is not known and enrichment is difficult. As one response to this limitation, Annenkov and Chernajovsky [75] engineered a T-cell receptor whose extracellular domain contains a type II collagen-binding motif.
Isis Pharmaceuticals (Carlsbad, CA, USA) sponsored phase I, IIa, and II clinical trials in which anti-sense RNA directed against TNF was injected intravenously and subcutaneously into subjects with RA. Anti-sense RNA was shown to traffic to the synovium of diseased joints, suggesting facilitated local delivery. The phase II study involved 157 subjects with RA who received 200 mg of anti-sense RNA twice a week, once a week, or once a fortnight. Subjects in the two highest dosing groups showed improvement in ACR20 (American College of Rheumatology 20% improvement criteria) scores. These studies were reported on the company's website [76] but were never published in the peer-reviewed literature. The company is no longer pursuing this project.
The recent emergence of RNA interference provides the ability to knock down cytokine synthesis in a highly specific fashion. Khoury and colleagues [77] have delivered short interfering RNA molecules targeted to IL-1, IL-6, and IL-18 in murine collagen-induced arthritis [77]. Knockdown of each cytokine was effective in reducing the incidence and severity of disease, but a dramatic therapeutic effect was observed when all three were inhibited together.
Osteoarthritis
Osteoarthritis (OA) is highly prevalent, incurable, and difficult to treat, imposing an enormous socioeconomic burden. Because it affects a limited number of joints and has no known systemic components, OA is well suited to local gene therapy [78]. Several preclinical studies confirm the efficacy of local gene delivery in the treatment of experimental models of OA [79–82]. Nearly all of these have used IL-1Ra as the transgene product, reflecting the importance of IL-1 as a mediator in the osteoarthritic joint. The equine study of Frisbie and colleagues [83] is of interest because, in addition to using the conventional histological outcome measures, they noted a reduction in lameness in response to gene therapy. This is an encouraging result for a disease in which pain is the overriding presenting clinical symptom. OA is common in horses, dogs, and other companion animals, suggesting a role for gene therapy in veterinary medicine.
Because destruction of the articular cartilage is the most obvious pathological lesion in the affected joints of individuals with OA, studies on the treatment of OA overlap with those on cartilage regeneration. Discussion of gene transfer approaches to cartilage regeneration lies beyond the scope of this article, but reference [84] provides a good recent review. Collectively, cDNAs encoding insulin-like growth factor-1, fibroblast growth factor-2, bone morphogenetic protein (BMP)-2, BMP-4, BMP-7, TGF-β, and sonic hedgehog have shown promise in cartilage repair. Clinical trials are under way in Korea and the US using a retrovirally transduced, human chondrocyte cell line as a vehicle for the ex vivo delivery of TGF-β1 to joints with OA (Table 1). This protocol is based upon preclinical data showing a surprising restorative effect in animal models of cartilage damage when TGF-β1 is delivered in an ex vivo fashion using allograft or even xenograft cells [85]. In the human trial, the cells are irradiated prior to injection to prevent cell division and thus eliminate the risk of cancer from these aneuploid retrovirally transduced cells. So far, 16 subjects have been treated in this fashion without incident. Elevation of TGF-β1 levels has not been observed in serum, but two subjects have presented with synovial effusion. Eight patients have demonstrated symptomatic improvement, and evaluation via magnetic resonance imaging has found evidence of cartilage regeneration.
Gout
When urate crystals are injected into subcutaneous air pouches on mice, they induce inflammatory responses of the type seen in human gout. Ex vivo delivery of prostaglandin D synthetase has a strong anti-inflammatory effect, suggesting that this could serve as the basis of a gene treatment for crystal induced arthropathy [86]. A small clinical study indicates that recombinant IL-1Ra (Kineret®) has a beneficial effect in human gout [87]. This suggests an additional clinical target for the genetic therapies, discussed above, that presently use IL-1Ra cDNA to treat RA and OA.
Other rheumatic diseases
Sjögren syndrome
Like diarthrodial joints, salivary glands are discrete isolated structures that lend themselves to local gene transfer. Vectors can be introduced through a cannulated duct and reach the luminal surfaces of the epithelial cells. Because the salivary gland is well encapsulated, there is little risk of vector escaping to nontarget organs. Many of the principles described above in the context of RA also apply to Sjögren syndrome [88].
Although adenovirus vectors transfer genes to the salivary glands very efficiently, AAV is proving to be the vector of choice because it is safe and noninflammatory. Serotypes 2 and 5 show promise, and efficacy has been demonstrated in animal models using IL-10 [89] and vasoactive intestinal peptide [90] as the transgene products. Because the salivary gland has an exocrine function, it can also be used as a site of gene transfer for systemic delivery purposes [91]. Gene therapy for Sjögren syndrome is reviewed in references [88].
Lupus
Several of the strategies we have already discussed in the context of RA have also been applied to lupus. Unlike RA therapy, lupus therapy has not benefitted in a dramatic fashion from the introduction of biologics. Moreover, because lupus is accompanied by a large increase in mortality, the risk-to-benefit ratio is more favorable toward gene therapy. Lupus is thought to involve excess production of type 2 cytokines, so a number of investigators have introduced type 1 cytokines, such as IL-2 and IL-12. Encouraging results followed the intramuscular injection of plasmids encoding these cytokines in murine models [92, 93]. Injection of plasmids encoding an IFN-γ receptor: Fc construct has also shown promise [94]. In some experiments, the efficiency of transfection has been increased by electroporation, leading to efficacy with a cDNA encoding a dominant negative mutation of monocyte chemoattractant protein-1 [95]. The DNA vaccination approach has also worked using a cDNA encoding a consensus peptide from anti-DNA immunoglobulins.
Other investigators have used adenovirus to deliver the immunoinhibitory receptor PD-L1, TACI (transmembrane activator and CAML [calcium modulator and cyclophilin ligand] interactor, an inhibitor of B-lymphocyte stimulator [BLyS]), CTLA4, and a soluble form of the TGF receptor II [96–99]. CTLA4 and CD40Ig have also been delivered in animal models using AAV8 [100, 101]. Data from animal models thus provide numerous examples of successful gene therapy in murine models of lupus. The challenge is to translate these into clinically useful human protocols. Gene therapy for lupus is reviewed in reference [101].
Antiphospholipid syndrome
DNA vaccination has been used to generate antibodies to TNF with associated improvement in an animal model of antiphospholipid syndrome [102].
Summary and future directions
During the decade under review, the application of gene therapy in rheumatic diseases has undergone several mood swings. Nevertheless, a small group of investigators in this area has maintained a remarkably steady output of research papers (Figure 1), leading to several phase I clinical trials and one phase II trial in RA. There is evidence of a clinical response in certain subjects, suggesting that additional trials to establish efficacy are merited. Their implementation is not aided by the high cost of clinical trials. Moreover, there are widespread concerns about safety, and many question the use of gene therapy to treat nongenetic nonlethal diseases. These concerns are amplified by the clinical and commercial success of protein-based therapies for RA. Nevertheless, conventional biologics are very expensive, and an effective intra-articular gene therapy administered only rarely is likely to be far less costly.
OA, in contrast, responds poorly to conventional treatments and is a leading and growing cause of morbidity. The pressing need for better ways to control this common, debilitating, and expensive condition could be met by responsible gene therapy protocols using safe vectors. Two clinical trials exploring the use of gene therapy in OA are under way and another is in the pipeline. If successful, they could lead to wide human and veterinary application and pave the way for additional protocols in other arthritides.
Proof of principle has been established in animal models of Sjögren syndrome and lupus, pointing to the need for translational research to develop clinical trials. Because these diseases, unlike RA, do not respond well to present biologics, alternative approaches, such as gene therapy, seem worthwhile. Their success could encourage further investigations in serious, intractable, rheumatic diseases, such as scleroderma. The technology of gene transfer has developed to the point where it is no longer the rate-limiting step for many purposes. Instead, there is a need for considerable funding, persistence, and continuity of effort to bring gene therapy into rheumatologic clinical practice.
Note
The Scientific Basis of Rheumatology: A Decade of Progress
This article is part of a special collection of reviews, The Scientific Basis of Rheumatology: A Decade of Progress, published to mark Arthritis Research & Therapy's 10th anniversary.
Other articles in this series can be found at: http://arthritis-research.com/sbr
Abbreviations
- AAV:
-
adeno-associated virus
- APC:
-
antigen-presenting cell
- BMP:
-
bone morphogenetic protein
- FDA:
-
US Food and Drug Administration
- GTARD:
-
Gene Therapy of Arthritis and Related Disorders
- IFN:
-
interferon
- IL:
-
interleukin
- IL-1Ra:
-
interleukin-1 receptor antagonist
- MCP:
-
metacarpophalangeal
- NF-κB:
-
nuclear factor-kappa-B
- NIH:
-
National Institutes of Health
- OA:
-
osteoarthritis
- RA:
-
rheumatoid arthritis
- sc:
-
self-complementary
- SCID:
-
severe combined immunodeficiency disease
- TGF:
-
transforming growth factor
- TNF:
-
tumor necrosis factor
- TRAIL:
-
tumor necrosis factor-related apoptosis-inducing ligand.
References
Evans CH, Rediske JJ, Abramson SB, Robbins PD: Joint efforts: tackling arthritis using gene therapy. First International Meeting on the Gene Therapy of Arthritis and Related Disorders. Bethesda, MD, USA, 2–3 December 1998. Molecular Medicine Today. 1999, 5: 148-151. 10.1016/S1357-4310(99)01452-5.
Raper SE, Chirmule N, Lee FS, Wivel NA, Bagg A, Gao GP, Wilson JM, Batshaw ML: Fatal systemic inflammatory response syndrome in a ornithine transcarbamylase deficient patient following adenoviral gene transfer. Mol Genet Metab. 2003, 80: 148-158. 10.1016/j.ymgme.2003.08.016.
Wilson JM: Gendicine: the first commercial gene therapy product. Hum Gene Ther. 2005, 16: 1014-1015. 10.1089/hum.2005.16.1014.
Cavazzana-Calvo M, Hacein-Bey S, de Saint Basile G, Gross F, Yvon E, Nusbaum P, Selz F, Hue C, Certain S, Casanova JL, Bousso P, Deist FL, Fischer A: Gene therapy of human severe combined immunodeficiency (SCID)-X1 disease. Science. 2000, 288: 669-672. 10.1126/science.288.5466.669.
Gaspar HB, Bjorkegren E, Parsley K, Gilmour KC, King D, Sinclair J, Zhang F, Giannakopoulos A, Adams S, Fairbanks LD, Gaspar J, Henderson L, Xu-Bayford JH, Davies EG, Veys PA, Kinnon C, Thrasher AJ: Successful reconstitution of immunity in ADA-SCID by stem cell gene therapy following cessation of PEG-ADA and use of mild preconditioning. Mol Ther. 2006, 14: 505-513. 10.1016/j.ymthe.2006.06.007.
Ott MG, Schmidt M, Schwarzwaelder K, Stein S, Siler U, Koehl U, Glimm H, Kuhlcke K, Schilz A, Kunkel H, Naundorf S, Brinkmann A, Deichmann A, Fischer M, Ball C, Pilz I, Dunbar C, Du Y, Jenkins NA, Copeland NG, Lüthi U, Hassan M, Thrasher AJ, Hoelzer D, von Kalle C, Seger R, Grez M: Correction of X-linked chronic granulomatous disease by gene therapy, augmented by insertional activation of MDS1-EVI1, PRDM16 or SETBP1. Nat Med. 2006, 12: 401-409. 10.1038/nm1393.
Bainbridge JW, Smith AJ, Barker SS, Robbie S, Henderson R, Balaggan K, Viswanathan A, Holder GE, Stockman A, Tyler N, Petersen-Jones S, Bhattacharya SS, Thrasher AJ, Fitzke FW, Carter BJ, Rubin GS, Moore AT, Ali RR: Effect of gene therapy on visual function in Leber's congenital amaurosis. N Engl J Med. 2008, 358: 2231-2239. 10.1056/NEJMoa0802268.
Maguire AM, Simonelli F, Pierce EA, Pugh EN, Mingozzi F, Bennicelli J, Banfi S, Marshall KA, Testa F, Surace EM, Rossi S, Lyubarsky A, Arruda VR, Konkle B, Stone E, Sun J, Jacobs J, Dell'Osso L, Hertle R, Ma JX, Redmond TM, Zhu X, Hauck B, Zelenaia O, Shindler KS, Maguire MG, Wright JF, Volpe NJ, McDonnell JW, Auricchio A, High KA, Bennett J: Safety and efficacy of gene transfer for Leber's congenital amaurosis. N Engl J Med. 2008, 358: 2240-2248. 10.1056/NEJMoa0802315.
Evans CH, Ghivizzani SC, Gouze E, Rediske JJ, Schwarz EM, Robbins PD: The 3rd International Meeting on Gene Therapy in Rheumatology and Orthopaedics. Arthritis Res Ther. 2005, 7: 273-278. 10.1186/ar1853.
Robbins PD, Evans CH, Jorgensen C: Gene therapy moves forward – the second international meeting on gene and cell therapies of arthritis and related disorders, 17–18 May 2001, Montpellier, France. Arthritis Res Ther. 2001, 3: 289-292.
Hacein-Bey-Abina S, von Kalle C, Schmidt M, Le Deist F, Wulffraat N, McIntyre E, Radford I, Villeval JL, Fraser CC, Cavazzana-Calvo M, Fischer A: A serious adverse event after successful gene therapy for X-linked severe combined immunodeficiency. N Engl J Med. 2003, 348: 255-256. 10.1056/NEJM200301163480314.
Gouze E, Pawliuk R, Gouze JN, Pilapil C, Fleet C, Palmer GD, Evans CH, Leboulch P, Ghivizzani SC: Lentiviral-mediated gene delivery to synovium: potent intra-articular expression with amplification by inflammation. Mol Ther. 2003, 7: 460-466. 10.1016/S1525-0016(03)00024-8.
Gouze E, Pawliuk R, Pilapil C, Gouze JN, Fleet C, Palmer GD, Evans CH, Leboulch P, Ghivizzani SC: In vivo gene delivery to synovium by lentiviral vectors. Mol Ther. 2002, 5: 397-404. 10.1006/mthe.2002.0562.
Imperiale MJ, Kochanek S: Adenovirus vectors: biology, design, and production. Curr Top Microbiol Immunol. 2004, 273: 335-357.
Toh ML, Hong SS, Loo van de F, Franqueville L, Lindholm L, Berg van den W, Boulanger P, Miossec P: Enhancement of aden-ovirus-mediated gene delivery to rheumatoid arthritis synoviocytes and synovium by fiber modifications: role of arginine-glycine-aspartic acid (RGD)- and non-RGD-binding integrins. J Immunol. 2005, 175: 7687-7698.
Grieger JC, Choi VW, Samulski RJ: Production and characterization of adeno-associated viral vectors. Nat Protoc. 2006, 1: 1412-1428. 10.1038/nprot.2006.207.
McCarty DM, Fu H, Monahan PE, Toulson CE, Naik P, Samulski RJ: Adeno-associated virus terminal repeat (TR) mutant generates self-complementary vectors to overcome the rate-limiting step to transduction in vivo. Gene Ther. 2003, 10: 2112-2118. 10.1038/sj.gt.3302134.
Kay JD, Gouze E, Oligino TJ, Gouze JN, Watson RS, Levings PP, Bush ML, Dacanay A, Robbins PD, Evans CH, Ghivizzani SC: Intra-articular gene delivery and expression of IL-1Ra mediated by self-complementary adeno-associated virus. J Gene Med. 2008
Wu Z, Asokan A, Samulski RJ: Adeno-associated virus serotypes: vector toolkit for human gene therapy. Mol Ther. 2006, 14: 316-327. 10.1016/j.ymthe.2006.05.009.
Louboutin JP, Wang L, Wilson JM: Gene transfer into skeletal muscle using novel AAV serotypes. J Gene Med. 2005, 7: 442-451. 10.1002/jgm.686.
Manno CS, Pierce GF, Arruda VR, Glader B, Ragni M, Rasko JJ, Ozelo MC, Hoots K, Blatt P, Konkle B, Dake M, Kaye R, Razavi M, Zajko A, Zehnder J, Rustagi PK, Nakai H, Chew A, Leonard D, Wright JF, Lessard RR, Sommer JM, Tigges M, Sabatino D, Luk A, Jiang H, Mingozzi F, Couto L, Ertl HC, High KA, Kay MA: Successful transduction of liver in hemophilia by AAV-Factor IX and limitations imposed by the host immune response. Nat Med. 2006, 12: 342-347. 10.1038/nm1358.
Mingozzi F, Maus MV, Hui DJ, Sabatino DE, Murphy SL, Rasko JE, Ragni MV, Manno CS, Sommer J, Jiang H, Pierce GF, Ertl HC, High KA: CD8(+) T-cell responses to adeno-associated virus capsid in humans. Nat Med. 2007, 13: 419-422. 10.1038/nm1549.
Evans CH, Ghivizzani SC, Robbins PD: Arthritis gene therapy's first death. Arthritis Res Ther. 2008, 10: 110-10.1186/ar2411.
Thomas CE, Ehrhardt A, Kay MA: Progress and problems with the use of viral vectors for gene therapy. Nat Rev Genet. 2003, 4: 346-358. 10.1038/nrg1066.
Conwell CC, Huang L: Recent advances in non-viral gene delivery. Adv Genet. 2005, 53: 3-18.
Bandara G, Mueller GM, Galea-Lauri J, Tindal MH, Georgescu HI, Suchanek MK, Hung GL, Glorioso JC, Robbins PD, Evans CH: Intraarticular expression of biologically active interleukin 1-receptor-antagonist protein by ex vivo gene transfer. Proc Natl Acad Sci USA. 1993, 90: 10764-10768. 10.1073/pnas.90.22.10764.
Bandara G, Robbins PD, Georgescu HI, Mueller GM, Glorioso JC, Evans CH: Gene transfer to synoviocytes: prospects for gene treatment of arthritis. DNA Cell Biol. 1992, 11: 227-231.
Evans CH, Ghivizzani SC, Robbins PD: Gene therapy for arthritis: what next?. Arthritis Rheum. 2006, 54: 1714-1729. 10.1002/art.21886.
Evans CH, Robbins PD, Ghivizzani SC, Herndon JH, Kang R, Bahnson AB, Barranger JA, Elders EM, Gay S, Tomaino MM, Wasko MC, Watkins SC, Whiteside TL, Glorioso JC, Lotze MT, Wright TM: Clinical trial to assess the safety, feasibility, and efficacy of transferring a potentially anti-arthritic cytokine gene to human joints with rheumatoid arthritis. Hum Gene Ther. 1996, 7: 1261-1280. 10.1089/hum.1996.7.10-1261.
Evans CH, Robbins PD, Ghivizzani SC, Wasko MC, Tomaino MM, Kang R, Muzzonigro TA, Vogt M, Elder EM, Whiteside TL, Watkins SC, Herndon JH: Gene transfer to human joints: progress toward a gene therapy of arthritis. Proc Natl Acad Sci USA. 2005, 102: 8698-8703. 10.1073/pnas.0502854102.
Wehling P, Reinecke J, Baltzer AA, Granrath M, Schulitz KP, Schultz C, Krauspe R, Whiteside T, Elder E, Ghivizzani SC, Robbins PD, Evans CH: Clinical responses to gene therapy in joints of two subjects with rheumatoid arthritis. Hum Gene Ther. 2008
Sant SM, Suarez TM, Moalli MR, Wu BY, Blaivas M, Laing TJ, Roessler BJ: Molecular lysis of synovial lining cells by in vivo herpes simplex virusthymidine kinase gene transfer. Hum Gene Ther. 1998, 9: 2735-2743. 10.1089/hum.1998.9.18-2735.
Mease PJ, Hobbs K, Chalmers A, El-Gabalawy H, Bookman A, Keystone E, Furst DE, Anklesaria P, Heald AE: Local delivery of a recombinant adeno-associated vector containing a tumor necrosis factor-{alpha} antagonist gene in inflammatory arthritis: a phase 1 dose-escalation safety and tolerability study. Ann Rheum Dis. 2008
Mease P, Wei N, Fudman E, Kivitz A, Anklesaria P, Heald A: Local treatment for inflammatory arthritis: a phase 1/2 clinical study of intra-articular administration of a recombinant adeno-associated vector containing a TNF-a antagonist gene [abstract]. Arthritis Rheum. 2007, 56 (suppl 9): S793-
Apparailly F, Khoury M, Vervoordeldonk MJ, Adriaansen J, Gicquel E, Perez N, Riviere C, Louis-Plence P, Noel D, Danos O, Douar AM, Tak PP, Jorgensen C: Adeno-associated virus pseudotype 5 vector improves gene transfer in arthritic joints. Hum Gene Ther. 2005, 16: 426-434. 10.1089/hum.2005.16.426.
Adriaansen J, Tas SW, Klarenbeek PL, Bakker AC, Apparailly F, Firestein GS, Jorgensen C, Vervoordeldonk MJ, Tak PP: Enhanced gene transfer to arthritic joints using adeno-associated virus type 5: implications for intra-articular gene therapy. Ann Rheum Dis. 2005, 64: 1677-1684. 10.1136/ard.2004.035063.
Boissier MC, Lemeiter D, Clavel C, Valvason C, Laroche L, Begue T, Bessis N: Synoviocyte infection with adeno-associated virus (AAV) is neutralized by human synovial fluid from arthritis patients and depends on AAV serotype. Hum Gene Ther. 2007, 18: 525-535. 10.1089/hum.2006.174.
Adriaansen J, Khoury M, de Cortie CJ, Fallaux FJ, Bigey P, Scherman D, Gould DJ, Chernajovsky Y, Apparailly F, Jorgensen C, Vervoordeldonk MJ, Tak PP: Reduction of arthritis following intra-articular administration of an adeno-associated virus serotype 5 expressing a disease-inducible TNF-blocking agent. Ann Rheum Dis. 2007, 66: 1143-1150. 10.1136/ard.2006.064519.
Adriaansen J, Fallaux FJ, de Cortie CJ, Vervoordeldonk MJ, Tak PP: Local delivery of beta interferon using an adeno-associated virus type 5 effectively inhibits adjuvant arthritis in rats. J Gen Virol. 2007, 88: 1717-1721. 10.1099/vir.0.82603-0.
Takahashi H, Kato K, Miyake K, Hirai Y, Yoshino S, Shimada T: Adeno-associated virus vector-mediated anti-angiogenic gene therapy for collagen-induced arthritis in mice. Clin Exp Rheumatol. 2005, 23: 455-461.
Tas SW, Adriaansen J, Hajji N, Bakker AC, Firestein GS, Vervoordeldonk MJ, Tak PP: Amelioration of arthritis by intraarticular dominant negative Ikk beta gene therapy using adeno-associated virus type 5. Hum Gene Ther. 2006, 17: 821-832. 10.1089/hum.2006.17.821.
Ulrich-Vinther M, Duch MR, Soballe K, O'Keefe RJ, Schwarz EM, Pedersen FS: In vivo gene delivery to articular chondrocytes mediated by an adeno-associated virus vector. J Orthop Res. 2004, 22: 726-734. 10.1016/j.orthres.2003.12.003.
Jennings K, Miyamae T, Traister R, Marinov A, Katakura S, Sowders D, Trapnell B, Wilson JM, Gao G, Hirsch R: Proteasome inhibition enhances AAV-mediated transgene expression in human synoviocytes in vitro and in vivo. Mol Ther. 2005, 11: 600-607. 10.1016/j.ymthe.2004.10.020.
Zhong L, Li B, Mah CS, Govindasamy L, Agbandje-McKenna M, Cooper M, Herzog RW, Zolotukhin I, Warrington KH, Weigel-Van Aken KA, Hobbs JA, Zolotukhin S, Muzyczka N, Srivastava A: Next generation of adeno-associated virus 2 vectors: point mutations in tyrosines lead to high-efficiency transduction at lower doses. Proc Natl Acad Sci USA. 2008, 105: 7827-7832. 10.1073/pnas.0802866105.
Traister RS, Fabre S, Wang Z, Xiao X, Hirsch R: Inflammatory cytokine regulation of transgene expression in human fibroblast-like synoviocytes infected with adeno-associated virus. Arthritis Rheum. 2006, 54: 2119-2126. 10.1002/art.21940.
Pan RY, Chen SL, Xiao X, Liu DW, Peng HJ, Tsao YP: Therapy and prevention of arthritis by recombinant adeno-associated virus vector with delivery of interleukin-1 receptor antagonist. Arthritis Rheum. 2000, 43: 289-297. 10.1002/1529-0131(200002)43:2<289::AID-ANR8>3.0.CO;2-H.
Pan RY, Xiao X, Chen SL, Li J, Lin LC, Wang HJ, Tsao YP: Disease-inducible transgene expression from a recombinant adeno-associated virus vector in a rat arthritis model. J Virol. 1999, 73: 3410-3417.
Gouze E, Gouze JN, Palmer GD, Pilapil C, Evans CH, Ghivizzani SC: Transgene persistence and cell turnover in the diarthrodial joint: implications for gene therapy of chronic joint diseases. Mol Ther. 2007, 15: 1114-1120.
Miagkov AV, Varley AW, Munford RS, Makarov SS: Endogenous regulation of a therapeutic transgene restores homeostasis in arthritic joints. J Clin Invest. 2002, 109: 1223-1229.
Loo van de FA, de Hooge AS, Smeets RL, Bakker AC, Bennink MB, Arntz OJ, Joosten LA, van Beuningen HM, Kraan van der PK, Varley AW, Berg van den WB: An inflammation-inducible adenoviral expression system for local treatment of the arthritic joint. Gene Ther. 2004, 11: 581-590. 10.1038/sj.gt.3302182.
Apparailly F, Millet V, Noel D, Jacquet C, Sany J, Jorgensen C: Tetracycline-inducible interleukin-10 gene transfer mediated by an adeno-associated virus: application to experimental arthritis. Hum Gene Ther. 2002, 13: 1179-1188. 10.1089/104303402320138961.
Gould DJ, Berenstein M, Dreja H, Ledda F, Podhajcer OL, Chernajovsky Y: A novel doxycycline inducible autoregulatory plasmid which displays 'on'/'off' regulation suited to gene therapy applications. Gene Ther. 2000, 7: 2061-2070. 10.1038/sj.gt.3301354.
Zhang HG, Hyde K, Page GP, Brand JP, Zhou J, Yu S, Allison DB, Hsu HC, Mountz JD: Novel tumor necrosis factor alpha-regulated genes in rheumatoid arthritis. Arthritis Rheum. 2004, 50: 420-431. 10.1002/art.20037.
Tomita T, Takeuchi E, Tomita N, Morishita R, Kaneko M, Yamamoto K, Nakase T, Seki H, Kato K, Kaneda Y, Ochi T: Suppressed severity of collagen-induced arthritis by in vivo transfection of nuclear factor kappaB decoy oligodeoxynucheotides as a gene therapy. Arthritis Rheum. 1999, 42: 2532-2542. 10.1002/1529-0131(199912)42:12<2532::AID-ANR5>3.0.CO;2-2.
Dreja H, Annenkov A, Chernajovsky Y: Soluble complement receptor 1 (CD35) delivered by retrovirally infected syngeneic cells or by naked DNA injection prevents the progression of collagen-induced arthritis. Arthritis Rheum. 2000, 43: 1698-1709. 10.1002/1529-0131(200008)43:8<1698::AID-ANR5>3.0.CO;2-8.
Fellowes R, Etheridge CJ, Coade S, Cooper RG, Stewart L, Miller AD, Woo P: Amelioration of established collagen induced arthritis by systemic IL-10 gene delivery. Gene Ther. 2000, 7: 967-977. 10.1038/sj.gt.3301165.
Kim JM, Jeong JG, Ho SH, Hahn W, Park EJ, Kim S, Yu SS, Lee YW, Kim S: Protection against collagen-induced arthritis by intramuscular gene therapy with an expression plasmid for the interleukin-1 receptor antagonist. Gene Ther. 2003, 10: 1543-1550. 10.1038/sj.gt.3302042.
Kageyama Y, Koide Y, Uchijima M, Nagata T, Yoshida A, Taiki A, Miura T, Nagafusa T, Nagano A: Plasmid encoding interleukin-4 in the amelioration of murine collagen-induced arthritis. Arthritis Rheum. 2004, 50: 968-975. 10.1002/art.20107.
Miyata M, Sasajima T, Sato H, Saito A, Saito A, Iriswa A, Sato Y, Kasukawa R: Suppression of collagen induced arthritis in mice utilizing plasmid DNA encoding interleukin 10. J Rheumatol. 2000, 27: 1601-1605.
Song XY, Gu M, Jin WW, Klinman DM, Wahl SM: Plasmid DNA encoding transforming growth factor-beta1 suppresses chronic disease in a streptococcal cell wall-induced arthritis model. J Clin Invest. 1998, 101: 2615-2621. 10.1172/JCI2480.
Woods AM, Thompson SJ, Wooley PH, Panayi G, Klavinskis LS: Immune modulation of collagen-induced arthritis by intranasal cytokine gene delivery: a model for the therapy of rheumatoid arthritis. Arthritis Rheum. 2005, 52: 3761-3771. 10.1002/art.21473.
Quintana FJ, Carmi P, Mor F, Cohen IR: Inhibition of adjuvant arthritis by a DNA vaccine encoding human heat shock protein 60. J Immunol. 2002, 169: 3422-3428.
Dalum I, Butler DM, Jensen MR, Hindersson P, Steinaa L, Waterston AM, Grell SN, Feldmann M, Elsner HI, Mouritsen S: Therapeutic antibodies elicited by immunization against TNF-alpha. Nat Biotechnol. 1999, 17: 666-669. 10.1038/10878.
McDevitt H: Specific antigen vaccination to treat autoimmune disease. Proc Natl Acad Sci USA. 2004, 101 (Suppl 2): 14627-14630. 10.1073/pnas.0405235101.
Ghivizzani SC, Lechman ER, Kang R, Tio C, Kolls J, Evans CH, Robbins PD: Direct adenovirus-mediated gene transfer of interleukin 1 and tumor necrosis factor alpha soluble receptors to rabbit knees with experimental arthritis has local and distal anti-arthritic effects. Proc Natl Acad Sci USA. 1998, 95: 4613-4618. 10.1073/pnas.95.8.4613.
Kim SH, Lechman ER, Kim S, Nash J, Oligino TJ, Robbins PD: Ex vivo gene delivery of IL-1Ra and soluble TNF receptor confers a distal synergistic therapeutic effect in antigen-induced arthritis. Mol Ther. 2002, 6: 591-600. 10.1016/S1525-0016(02)90711-2.
Whalen JD, Thomson AW, Lu L, Robbins PD, Evans CH: Viral IL-10 gene transfer inhibits DTH responses to soluble antigens: evidence for involvement of genetically modified dendritic cells and macrophages. Mol Ther. 2001, 4: 543-550. 10.1006/mthe.2001.0492.
Kim SH, Kim S, Evans CH, Ghivizzani SC, Oligino T, Robbins PD: Effective treatment of established murine collagen-induced arthritis by systemic administration of dendritic cells genetically modified to express IL-4. J Immunol. 2001, 166: 3499-3505.
Kim SH, Kim S, Oligino TJ, Robbins PD: Effective treatment of established mouse collagen-induced arthritis by systemic administration of dendritic cells genetically modified to express FasL. Mol Ther. 2002, 6: 584-590. 10.1016/S1525-0016(02)90712-4.
Zhan HG, Mountz JD, Fleck M, Zhou T, Hsu HC: Specific deletion of autoreactive T cells by adenovirus-transfected, Fas ligand-producing antigen-presenting cells. Immunol Res. 2002, 26: 235-246. 10.1385/IR:26:1-3:235.
Liu Z, Xu X, Hsu HC, Tousson A, Yang PA, Wu Q, Liu C, Yu S, Zhang HG, Mountz JD: CII-DC-AdTRAIL cell gene therapy inhibits infiltration of CII-reactive T cells and CII-induced arthritis. J Clin Invest. 2003, 112: 1332-1341.
Terzioglu E, Bisgin A, Sanlioglu AD, Ulker M, Yazisiz V, Tuzuner S, Sanlioglu S: Concurrent gene therapy strategies effectively destroy synoviocytes of patients with rheumatoid arthritis. Rheumatology (Oxford). 2007, 46: 783-789. 10.1093/rheumatology/kel448.
Tarner IH, Slavin AJ, McBride J, Levicnik A, Smith R, Nolan GP, Contag CH, Fathman CG: Treatment of autoimmune disease by adoptive cellular gene therapy. Ann N Y Acad Sci. 2003, 998: 512-519. 10.1196/annals.1254.067.
Slavin AJ, Tarner IH, Nakajima A, Urbanek-Ruiz I, McBride J, Contag CH, Fathman CG: Adoptive cellular gene therapy of autoimmune disease. Autoimmun Rev. 2002, 1: 213-219. 10.1016/S1568-9972(02)00051-4.
Annenkov A, Chernajovsky Y: Engineering mouse T lymphocytes specific to type II collagen by transduction with a chimeric receptor consisting of a single chain Fv and TCR zeta. Gene Ther. 2000, 7: 714-722. 10.1038/sj.gt.3301149.
[http://ir.isispharm.com/releasedetail.cfm?ReleaseID=220333]
Khoury M, Escriou V, Courties G, Galy A, Yao R, Largeau C, Scherman D, Jorgensen C, Apparailly F: Efficient suppression of murine arthritis by combined anticytokine small interfering RNA lipoplexes. Arthritis Rheum. 2008, 58: 2356-2367. 10.1002/art.23660.
Evans CH, Gouze JN, Gouze E, Robbins PD, Ghivizzani SC: Osteoarthritis gene therapy. Gene Ther. 2004, 11: 379-389. 10.1038/sj.gt.3302196.
Pelletier JP, Caron JP, Evans C, Robbins PD, Georgescu HI, Jovanovic D, Fernandes JC, Martel-Pelletier J: In vivo suppression of early experimental osteoarthritis by interleukin-1 receptor antagonist using gene therapy. Arthritis Rheum. 1997, 40: 1012-1019. 10.1002/art.1780400604.
Fernandes J, Tardif G, Martel-Pelletier J, Lascau-Coman V, Dupuis M, Moldovan F, Sheppard M, Krishnan BR, Pelletier JP: In vivo transfer of interleukin-1 receptor antagonist gene in osteoarthritic rabbit knee joints: prevention of osteoarthritis progression. Am J Pathol. 1999, 154: 1159-1169.
Zhang X, Mao Z, Yu C: Suppression of early experimental osteoarthritis by gene transfer of interleukin-1 receptor antagonist and interleukin-10. J Orthop Res. 2004, 22: 742-750. 10.1016/j.orthres.2003.12.007.
Zhang X, Yu C, Xushi , Zhang C, Tang T, Dai K: Direct chitosan-mediated gene delivery to the rabbit knee joints in vitro and in vivo. Biochem Biophys Res Commun. 2006, 341: 202-208. 10.1016/j.bbrc.2005.12.171.
Frisbie DD, Ghivizzani SC, Robbins PD, Evans CH, McIlwraith CW: Treatment of experimental equine osteoarthritis by in vivo delivery of the equine interleukin-1 receptor antagonist gene. Gene Ther. 2002, 9: 12-20. 10.1038/sj.gt.3301608.
Cucchiarini M, Madry H: Gene therapy for cartilage defects. J Gene Med. 2005, 7: 1495-1509. 10.1002/jgm.824.
Lee KH, Song SU, Hwang TS, Yi Y, Oh IS, Lee JY, Choi KB, Choi MS, Kim SJ: Regeneration of hyaline cartilage by cell-mediated gene therapy using transforming growth factor beta 1-producing fibroblasts. Hum Gene Ther. 2001, 12: 1805-1813. 10.1089/104303401750476294.
Murakami Y, Akahoshi T, Hayashi I, Endo H, Hashimoto A, Kono S, Kondo H, Kawai S, Inoue M, Kitasato H: Inhibition of monosodium urate monohydrate crystal-induced acute inflammation by retrovirally transfected prostaglandin D synthase. Arthritis Rheum. 2003, 48: 2931-2941. 10.1002/art.11271.
So A, De Smedt T, Revaz S, Tschopp J: A pilot study of IL-1 inhibition by anakinra in acute gout. Arthritis Res Ther. 2007, 9: R28-10.1186/ar2143.
Kok MR, Baum BJ, Tak PP, Pillemer SR: Use of localised gene transfer to develop new treatment strategies for the salivary component of Sjögren's syndrome. Ann Rheum Dis. 2003, 62: 1038-1046. 10.1136/ard.62.11.1038.
Kok MR, Yamano S, Lodde BM, Wang J, Couwenhoven RI, Yakar S, Voutetakis A, Leroith D, Schmidt M, Afione S, Pillemer SR, Tsutsui MT, Tak PP, Chiorini JA, Baum BJ: Local adeno-associated virus-mediated interleukin 10 gene transfer has disease-modifying effects in a murine model of Sjögren's syndrome. Hum Gene Ther. 2003, 14: 1605-1618. 10.1089/104303403322542257.
Lodde BM, Mineshiba F, Wang J, Cotrim AP, Afione S, Tak PP, Baum BJ: Effect of human vasoactive intestinal peptide gene transfer in a murine model of Sjögren's syndrome. Ann Rheum Dis. 2006, 65: 195-200. 10.1136/ard.2005.038232.
Voutetakis A, Kok MR, Zheng C, Bossis I, Wang J, Cotrim AP, Marracino N, Goldsmith CM, Chiorini JA, Loh YP, Nieman LK, Baum BJ: Reengineered salivary glands are stable endogenous bioreactors for systemic gene therapeutics. Proc Natl Acad Sci USA. 2004, 101: 3053-3058. 10.1073/pnas.0400136101.
Raz E, Dudler J, Lotz M, Baird SM, Berry CC, Eisenberg RA, Carson DA: Modulation of disease activity in murine systemic lupus erythematosus by cytokine gene delivery. Lupus. 1995, 4: 286-292. 10.1177/096120339500400409.
Hagiwara E, Okubo T, Aoki I, Ohno S, Tsuji T, Ihata A, Ueda A, Shirai A, Okuda K, Miyazaki J, Ishigatsubo Y: IL-12-encoding plasmid has a beneficial effect on spontaneous autoimmune disease in MRL/MP-lpr/lpr mice. Cytokine. 2000, 12: 1035-1041. 10.1006/cyto.1999.0662.
Lawson BR, Prud'homme GJ, Chang Y, Gardner HA, Kuan J, Kono DH, Theofilopoulos AN: Treatment of murine lupus with cDNA encoding IFN-gammaR/Fc. J Clin Invest. 2000, 106: 207-215. 10.1172/JCI10167.
Shimizu S, Nakashima H, Masutani K, Inoue Y, Miyake K, Akahoshi M, Tanaka Y, Egashira K, Hirakata H, Otsuka T, Harada M: Antimonocyte chemoattractant protein-1 gene therapy attenuates nephritis in MRL/lpr mice. Rheumatology (Oxford). 2004, 43: 1121-1128. 10.1093/rheumatology/keh277.
Haviv YS, Takayama K, Nagi PA, Tousson A, Cook W, Wang M, Lam JT, Naito S, Lei X, Carey DE, Curiel DT: Modulation of renal glomerular disease using remote delivery of adenoviral-encoded solubletype II TGF-beta receptor fusion molecule. J Gene Med. 2003, 5: 839-851. 10.1002/jgm.428.
Takiguchi M, Murakami M, Nakagawa I, Saito I, Hashimoto A, Uede T: CTLA4IgG gene delivery prevents autoantibody production and lupus nephritis in MRL/lpr mice. Life Sci. 2000, 66: 991-1001. 10.1016/S0024-3205(99)00664-5.
Ding H, Wu X, Wu J, Yagita H, He Y, Zhang J, Ren J, Gao W: Delivering PD-1 inhibitory signal concomitant with blocking ICOS co-stimulation suppresses lupus-like syndrome in autoimmune BXSB mice. Clin Immunol. 2006, 118: 258-267. 10.1016/j.clim.2005.10.017.
Liu W, Szalai A, Zhao L, Liu D, Martin F, Kimberly RP, Zhou T, Carter RH: Control of spontaneous B lymphocyte autoimmunity with adenovirus-encoded soluble TACI. Arthritis Rheum. 2004, 50: 1884-1896. 10.1002/art.20290.
Ye X, Zhu T, Bastacky S, McHale T, Li J, Xiao X: Prevention and reversal of lupus in NZB/NZW mice by costimulatory blockade with adeno-associated virus-mediated gene transfer. Arthritis Rheum. 2005, 52: 3975-3986. 10.1002/art.21417.
Kyttaris VC, Sfikakis PP, Juang YT, Tsokos GC: Gene therapy in systemic lupus erythematosus. Curr Gene Ther. 2005, 5: 677-684. 10.2174/156652305774964703.
Blank M, Krause I, Wildbaum G, Karin N, Shoenfeld Y: TNFalpha DNA vaccination prevents clinical manifestations of experimental antiphospholipid syndrome. Lupus. 2003, 12: 546-549. 10.1191/0961203303lu399oa.
Otani K, Nita I, Macaulay W, Georgescu HI, Robbins PD, Evans CH: Suppression of antigen-induced arthritis in rabbits by ex vivo gene therapy. J Immunol. 1996, 156: 3558-3562.
Makarov SS, Olsen JC, Johnston WN, Anderle SK, Brown RR, Baldwin AS, Haskill JS, Schwab JH: Suppression of experimental arthritis by gene transfer of interleukin 1 receptor antagonist cDNA. Proc Natl Acad Sci USA. 1996, 93: 402-406. 10.1073/pnas.93.1.402.
Evans CH: Arthritis gene therapy at an inflection point. Future Rheumatol. 2008, 3: 207-210. 10.2217/17460816.3.3.207.
Evans CH, Ghivizzani SC, Kang R, Muzzonigro T, Wasko MC, Herndon JH, Robbins PD: Gene therapy for rheumatic diseases. Arthritis Rheum. 1999, 42: 1-16. 10.1002/1529-0131(199901)42:1<1::AID-ANR1>3.0.CO;2-4.
Acknowledgements
The authors' work in this area has been supported by NIH grants DK 446640, AR 43623, AR47353, AR050249, AR048566, and AR051085. GTARD-5 was supported, in part, by NIH grant R13 AR 055864.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
CHE and PDR are on the scientific advisory board of TissueGene Inc. (Rockville, MD, USA), for which they receive an honorarium but no stock. TissueGene Inc. is developing gene therapies for osteoarthritis. CHE is on the supervisory board of Orthogen AG (Düsseldorf, Germany), and PDR is on the scientific advisory board. Neither individual receives an honorarium, but CHE owns stock in the company. Orthogen AG is not developing gene therapies for arthritis. PDR and SCG are cofounders of Molecular Orthopaedics Incorporated (Chapel Hill, NC, USA), which is developing gene therapies for osteoarthritis. The authors are developing a clinical protocol using AAV to treat osteoarthritis by gene therapy.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
About this article
Cite this article
Evans, C.H., Ghivizzani, S.C. & Robbins, P.D. Gene therapy of the rheumatic diseases: 1998 to 2008. Arthritis Res Ther 11, 209 (2009). https://doi.org/10.1186/ar2563
Published:
DOI: https://doi.org/10.1186/ar2563