
Abstract
The Fc gamma receptors have been shown to play important roles in the initiation and regulation of many immunological and inflammatory processes and to amplify and refine the immune response to an infection. We have investigated the hypothesis that polymorphism within the FCGR genetic locus is associated with giant cell arteritis (GCA). Biallelic polymorphisms in FCGR2A, FCGR3A, FCGR3B and FCGR2B were examined for association with biopsy-proven GCA (n = 85) and healthy ethnically matched controls (n = 132) in a well-characterised cohort from Lugo, Spain. Haplotype frequencies and linkage disequilibrium (D') were estimated across the FCGR locus and a model-free analysis performed to determine association with GCA. There was a significant association between FCGR2A-131RR homozygosity (odds ratio (OR) 2.10, 95% confidence interval (CI) 1.12 to 3.77, P = 0.02, compared with all others) and carriage of FCGR3A-158F (OR 3.09, 95% CI 1.10 to 8.64, P = 0.03, compared with non-carriers) with susceptibility to GCA. FCGR haplotypes were examined to refine the extent of the association. The haplotype showing the strongest association with GCA susceptibility was the FCGR2A-FCGR3A 131R-158F haplotype (OR 2.84, P = 0.01 for homozygotes compared with all others). There was evidence of a multiplicative joint effect between homozygosity for FCGR2A-131R and HLA-DRB1*04 positivity, consistent with both of these two genetic factors contributing to the risk of disease. The risk of GCA in HLA-DRB1*04 positive individuals homozygous for the FCGR2A-131R allele is increased almost six-fold compared with those with other FCGR2A genotypes who are HLA-DRB1*04 negative. We have demonstrated that FCGR2A may contribute to the 'susceptibility' of GCA in this Spanish population. The increased association observed with a FCGR2A-FCGR3A haplotype suggests the presence of additional genetic polymorphisms in linkage disequilibrium with this haplotype that may contribute to disease susceptibility. These findings may ultimately provide new insights into disease pathogenesis.
Similar content being viewed by others

Introduction
Giant cell arteritis (GCA) is a common chronic granulomatous vasculitis that is restricted to the over-50 population and thus serves as a paradigm for ageing-related immunopathology. Permanent ischaemic lesions, predominantly irreversible blindness, occur in 15% of patients due to hyperplasia of the intimal layer of involved arteries and non-thrombotic luminal occlusion. Some patients present acutely with blindness, secondary to anterior ischaemic optic neuropathy or central retinal artery occlusion, whereas others present with a systemic inflammatory syndrome [1]. High-dose steroids are conventionally used to prevent these ischaemic complications, but in an elderly population this leads to a high incidence of adverse events [2].
There is some evidence that GCA is an antigen-driven, autoimmune disease. One of the earliest changes within the vessel wall is the accumulation of dendritic cells within the adventitia, which are believed to initiate and maintain antigen-specific adaptive immune responses, following an as yet unknown vascular insult [3]. The familial clustering of GCA supports a genetic component, and there is a strong association with HLA-DRB1*04 in many different populations [4]. Within cohorts of biopsy-proven GCA, HLA-DRB1*04 is associated with systemic signs and symptoms [5], visual manifestations [6] and corticosteroid resistance [7]. Many other studies have examined genetic variants in key components of immune and inflammatory pathways known to be activated in this disease. Associations with polymorphisms in genes encoding tumour necrosis factor [8], interleukin-4 [9], intracellular adhesion molecule-1 [10], vascular endothelial growth factor [11, 12] and endothelial nitric oxide synthase have been reported in some cohorts [13, 14], although many are awaiting replication in a second population. Variant alleles of mannose-binding lectin, which result in low levels of mannose-binding lectin protein, are also associated with GCA, perhaps through modulation of phagocytic function [15].
There is some epidemiological evidence, such as clustering of cases in space and time, that infection may act as a trigger for both GCA and polymyalgia rheumatica [16]. Organisms proposed include parvovirus B19 and Chlamydia pneumoniae, but the evidence remains inconclusive [17]. Infections may lead to vasculitis through various mechanisms: for example, interactions between microbial ligands and endogenous molecules, impairment of pathogen clearance, molecular mimicry, modification of self epitopes into 'neo-antigens', or failure to down-regulate the alloimmune response [18]. The ageing process itself leads to a functional decline in adaptive and innate immune responses, known as immunosenescence, in association with an increased susceptibility to infections, malignancies and autoimmune/inflammatory disorders. Although GCA-specific autoantibodies have not been described, antibodies against a broad range of human autoantigens have been observed in both types of GCA [19]. Anticardiolipin antibodies have been reported, particularly in biopsy-positive GCA [20], and often disappear with steroid treatment [21]. Furthermore, the pathogenicity of anti-endothelial antibodies, which have been demonstrated in up to 50% of GCA patients, remains to be elucidated, but such antibodies have the potential to mediate Fc gamma receptor (FcγR) cross-linking and trigger downstream effector functions [22].
The FcγRs, which bind IgG containing immune complexes/IgG autoantibodies, have been shown to play important roles in the initiation and regulation of many immunological and inflammatory processes and to amplify and refine the immune response to an infection. Activating FcγRs (FcγRI, FcγRIIa, FcγRIIIa, FcγRIIIb) potentiate phagocytosis in response to IgG-containing immune complexes/opsonised micro-organisms and trigger the oxidative burst, degranulation, maturation and release of cytokines, including tumour necrosis factor-α [23–25]. FcγR-mediated endocytosis by antigen presenting cells, such as dendritic cells, results in efficient MHC class I and II presentation [26]. FcγRIIIa cross-linking additionally stimulates antigen-dependent cellular cytotoxicity by natural killer cells and macrophages. Conversely, FcγRIIb contains an inhibitory motif in the cytoplasmic tail that abrogates cellular activation and down-regulates the antibody response, thus acting as a negative feedback mechanism [23–25]. Polymorphic variants that increase the expression or affinity of these IgG receptors, or enhance their ability to bind specific IgG isotypes, may, therefore, play an important role in determining both the inflammation mediated by IgG (auto)antibodies and IgG-containing immune complexes and/or the susceptibility to specific infections that may be associated with triggering vascular/inflammatory disease.
We have examined the hypothesis that the FCGR genetic locus is associated with susceptibility to GCA in a previously well-characterised GCA cohort from north-western Spain.
Materials and methods
Giant cell arteritis patients and controls
This was an allelic association study where FCGR2A, FCGR3A, FCGR3B and FCGR2B alleles and pairwise haplotypes were examined in a well-characterised GCA cohort from Lugo, Spain [6, 27]. Briefly, all patients and controls were of local Spanish descent and originated from the area surrounding Lugo, Galicia, in north-western Spain. They comprised 217 individuals (132 healthy controls and 85 GCA patients). All patients were recruited from Xeral-Calde Hospital (Lugo) and all patients fulfilled the 1990 American College of Rheumatology criteria for the classification of GCA and had a positive temporal artery biopsy [28]. All controls were healthy volunteers, who could trace their ancestry in the region for at least three generations. Ethical approval was obtained from the respective Local Research Ethics Committees.
FCGRgenotyping
Genotyping at the FCGR locus is complex in view of the high level of structural homology between the three class II (FCGR2A, FCGR2B and FCGR2C) and two class III (FCGR3A and FCGR3B) receptors. Gene duplication at this locus is believed to have occurred as a result of an unequal crossover event [29] with subsequent divergence of biological functions. The functional FCGR2A-131H/R, FCGR3A-158F/V and FCGR3B-NA1/NA2 polymorphisms and 3' untranslated region FCGR2B-1206G/A single nucleotide polymorphism were genotyped using assays that have previously been validated in our laboratory [30, 31]. FCGR2A genotyping was performed by direct sequencing for >80% of samples. The FCGR gene order from centromere to telomere at chromosome 1q23 is FCGR2A, FCGR3A, FCGR2C, FCGR3B, FCGR2B [31, 32].
Statistical analyses
Statistical analyses were performed using the Stata statistical software (Stata Corporation 2005, Stata Statistical Software: Release 9.0, College Station, Texas, USA) unless otherwise stated. The power calculations for this study were based on the FCGR allele frequencies observed in the UK population [31]. A cohort of 85 GCA cases and 130 controls provides 80% power to detect an odds ratio (OR) of 2.5 or 2.9 for a dominant and recessive mode of inheritance, respectively, assuming an allele frequency of 0.35 (5% significance level); for an allele frequency of 0.5 the corresponding ORs are 3.2 and 2.5). Hardy-Weinberg equilibrium was investigated in each control population using an exact test. Allele and genotype frequencies were compared using 2 × 2 and 3 × 2 contingency tables, respectively. Two-sided P values below 0.05 were considered statistically significant throughout.
ORs and their 95% confidence intervals (CI) were calculated to quantify the magnitude of all significant associations, as an approximation of the relative risk. Haplotype frequencies were estimated pairwise across the FCGR locus using the Estimating Haplotypes PLUS (EHPLUS) program [33], which also calculates the empirical significance (P value) of overall linkage disequilibrium. The standardised disequilibrium coefficient (D') was calculated for each pair of FCGRs, utilizing the gene order derived from our electronic contig. The heterogeneity test within the Permutation and Model-free analysis program was used to test for association with disease. A permutation procedure implemented in this program enabled 1,000 permutations to be performed [33].
Association of FCGR haplotypes with GCA was investigated further using the haplotype trend regression approach proposed by Zaykin and colleagues [34] for dealing with uncertain phase. In this method, logistic regression can be used to relate disease status to an individual's haplotypes; where these are not known with certainty all haplotypes consistent with the genotypes are included as predictors, weighted by their probabilities (based on the estimated haplotype frequencies). This approach estimates the effect on risk of each haplotype assuming the effect of the two haplotypes is independent. Stepwise regression analyses were also used to investigate a possible interaction with HLA-DRB1*04 [35].
Results
Association of FCGR2A, FCGR3A, FCGR3B and FCGR2Bwith giant cell arteritis
There was no evidence of departure from Hardy-Weinberg equilibrium in the control group for any genotyped polymorphism.
There was weak evidence of a difference in the distribution of FCGR2A-131H/R alleles (P = 0.05) and genotypes (P = 0.06) between cases and controls (Table 1). The data supported a recessive model and individuals homozygous for the FCGR2A-131R allele had an increased risk of GCA (OR 2.10, 95% CI 1.12 to 3.77, P = 0.02, compared with all others). There was also a trend towards an increase in the FCGR3A-158F/V allele (P = 0.06) and genotype (P = 0.08) frequencies in GCA patients compared to controls (Table 1). The data were consistent with a dominant model and carriage of the FCGR3A-158F allele was associated with GCA (OR 3.09, 95% CI 1.10 to 8.64, P = 0.03). There were no significant differences in FCGR3B or FCGR2B allele or genotype frequencies between GCA subjects and controls.
Linkage disequilibrium at the FCGRgenetic locus
Significant linkage disequilibrium was observed between FCGR2A and FCGR3A (D' = 0.31, P = 0.01) and FCGR3A and FCGR3B (D' = -0.64, P = 0.0001) in the control population. The negative D' values indicate linkage disequilibrium between the commonest allele of one gene and the least common allele of the second gene (Table 2).
Association of FCGRhaplotypes with giant cell arteritis
The distributions of two-locus FCGR haplotypes were compared between the GCA and control populations, with a difference approaching statistical significance for FCGR2A-FCGR3A (Table 3). Compared with the control frequency of 36%, the FCGR2A-FCGR3A 131R-158F haplotype was found at increased frequency in GCA patients (50%).
From the haplotype trend regression analysis of FCGR2A-FCGR3A haplotypes, the 131R-158F haplotype was found to have a significant effect on the risk of GCA (OR 1.72, 95% CI 1.02 to 2.89, P = 0.04), compared to the H-V haplotype as baseline. These are maximum likelihood estimates of the effect of each haplotype assuming a log-additive combined effect of an individual's two haplotypes. Further analysis treating the number of copies of this haplotype as a factor shows that the effect of the haplotype is largely confined to those with two copies (data not shown). FCGR2A-FCGR3A haplotypes were analysed under a recessive model, where homozygosity for this haplotype was observed in 12% healthy controls compared with 27% GCA population giving an OR of 2.84, 95% CI 1.33 to 6.06 (P = 0.01) when homozygotes were compared with all others.
Contribution of FCGR2A genotype and HLA-DRB1*04 alleles in giant cell arteritis susceptibility
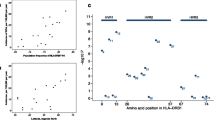
There was evidence of a multiplicative joint effect between homozygosity for FCGR2A-131R and HLA-DRB1*04 positivity, consistent with both of these two genetic factors contributing to the risk of disease (OR 2.23, 95% CI 1.09 to 4.58 and OR 2.61, 95% CI 1.30 to 5.22, respectively, from a model including both predictors). Thus, the risk of GCA in HLA-DRB1*04 positive individuals homozygous for the FCGR2A-131R allele is increased almost six-fold compared with those with other FCGR2A genotypes who are HLA-DRB1*04 negative. There is no evidence of an interaction between these two genetic loci (P = 0.19 from a likelihood ratio test).
Discussion
We have demonstrated a significant association between FCGR2A-131RR (OR 2.1, P = 0.02) and FCGR3A-158F (OR 3.09, P = 0.03) with susceptibility to GCA. Haplotype analyses can be more informative in their ability to identify disease predisposing genes. They may also provide additional evidence for the presence of unidentified polymorphic variants that are in linkage disequilibrium with the haplotype and are the true disease-susceptibility variants [36]. Accordingly, homozygosity for the FCGR2A-FCGR3A 131R-158F haplotype was associated with an almost three-fold increased risk of GCA (OR 2.84, P = 0.01).
The FcγRs play important roles in the initiation and propagation of many different immunological and inflammatory processes. The two alloforms (FCGR2A-131R and FCGR3A-158F) contained within the GCA-susceptibility haplotype encode low affinity variants (FcγRIIa-131R and FcγRIIIa-158F). FcγRIIa is the major phagocytic FcγR in humans and has two co-dominantly expressed alleles, 131H and 131R. The 131H isoform is the only FcγR that can bind IgG2, an antibody subclass that is also a poor activator of the classical complement pathway. FCGR2A-131H is, therefore, essential for handling IgG2 immune complexes: individuals homozygous for the 131R-allele have been shown to have an increased susceptibility to various encapsulated bacterial infections, such as Neisseria meningitides, Haemophilus influenzae and Streptococcus pneumoniae [37–39]. FcγRIIIa is expressed on natural killer cells, macrophages, γδ T-cells and a subset of monocytes. Consequently, they may act as susceptibility factors for GCA through a variety of mechanisms, such as an inability to bind IgG2 haplotypes (FcγRIIa-131R) on a background of impaired FcγR-mediated phagocytosis (FcγRIIa-131R and FcγRIIIa-158F) and impaired antigen-dependent cellular cytotoxicity of IgG-opsonised cells (FcγRIIIa-158F). Alternatively, FcγR polymorphisms may modulate endothelial leukocyte ingress, dendritic cell endocytosis and antigen presentation [26], or macrophage/natural killer cell effector functions to IgG containing immune complexes, each of which could separately influence the pathogenesis of GCA.
The same polymorphic variants have also been demonstrated to be associated with susceptibility to a variety of autoimmune diseases. For example, systemic lupus erythematosus is associated with the same FCGRIIA-131R, FCGRIIIA-158F and FCGRIIIB-NA2 alleles, whereas relapses in Wegener's granulomatosis are associated with FCGRIIA-131R and FCGRIIIA-158F alleles [40]. Flares in both systemic lupus erythematosus and Wegener's may be triggered by infection, particularly chronic nasal carriage of Staphylococcus aureus in the latter, but the picture is also complicated by impaired FcγR-mediated clearance of pathogenic autoantibodies and immune complexes.
Conclusion
Genetic polymorphism within the FCGR genetic locus may contribute to the development of GCA. The immunological consequences of these subtle defects in the innate immune system may be enhanced in the presence of immunosenescence, and the increased susceptibility to infection may potentially allow triggering of the inflammatory process in GCA. Additional studies from other ethnic groups will be required to confirm these genetic associations.
Abbreviations
- CI:
-
= confidence interval
- FcγR:
-
= Fc gamma receptor
- GCA:
-
= giant cell arteritis
- NA:
-
= neutrophil antigen
- OR:
-
= odds ratio.
References
Gonzalez-Gay MA, Barros S, Lopez-Diaz MJ, Garcia-Porrua C, Sanchez-Andrade A, Llorca J: Giant cell arteritis: disease patterns of clinical presentation in a series of 240 patients. Medicine (Baltimore). 2005, 84: 269-276. 10.1097/01.md.0000180042.42156.d1.
Nesher G, Sonnenblick M, Friedlander Y: Analysis of steroid related complications and mortality in temporal arteritis: a 15-year survey of 43 patients. J Rheumatol. 1994, 21: 1283-1286.
Ma-Krupa W, Jeon M-S, Spoerl S, Tedder TF, Goronzy JJ, Weyand CM: Activation of arterial wall dendritic cells and breakdown of self-tolerance in giant cell arteritis. J Exp Med. 2004, 199: 173-183. 10.1084/jem.20030850.
Gonzalez-Gay MA, Amoli MM, Garcia-Porrua C, Ollier WE: Genetic markers of disease susceptibility and severity in giant cell arteritis and polymyalgia rheumatica. Semin Arthritis Rheum. 2003, 33: 38-48. 10.1053/sarh.2002.50025.
Salvarani C, Boiardi L, Mantovani V, Ranzi A, Cantini F, Olivieri I, Bragliani M, Collina E, Macchioni P: HLA-DRB1 alleles associated with polymyalgia rheumatica in northern Italy: correlation with disease severity. Ann Rheum Dis. 1999, 58: 303-308.
Gonzalez-Gay MA, Garcia-Porrua C, Llorca J, Hajeer AH, Branas F, Dababneh A, Gonzalez-Louzao C, Rodriguez-Gil E, Rodriguez-Ledo P, Ollier WE: Visual manifestations of giant cell arteritis. Trends and clinical spectrum in 161 patients. Medicine (Baltimore). 2000, 79: 283-292.
Rauzy O, Fort M, Nourhashemi F, Alric L, Juchet H, Ecoiffier M, Abbal M, Adoue D: Relation between HLA DRB1 alleles and corticosteroid resistance in giant cell arteritis. Ann Rheum Dis. 1998, 57: 380-382.
Mattey DL, Hajeer AH, Dababneh A, Thomson W, Gonzalez-Gay MA, Garcia-Porrua C, Ollier WE: Association of giant cell arteritis and polymyalgia rheumatica with different tumor necrosis factor microsatellite polymorphisms. Arthritis Rheum. 2000, 43: 1749-1755. 10.1002/1529-0131(200008)43:8<1749::AID-ANR11>3.0.CO;2-K.
Amoli MM, Gonzalez-Gay MA, Zeggini E, Salway F, Garcia-Porrua C, Ollier WE: Epistatic interactions between HLA-DRB1 and interleukin 4, but not interferon-gamma, increase susceptibility to giant cell arteritis. J Rheumatol. 2004, 31: 2413-2417.
Salvarani C, Casali B, Boiardi L, Ranzi A, Macchioni P, Nicoli D, Farnetti E, Brini M, Portioli I: Intercellular adhesion molecule 1 gene polymorphisms in polymyalgia rheumatica/giant cell arteritis: association with disease risk and severity. J Rheumatol. 2000, 27: 1215-1221.
Boiardi L, Casali B, Nicoli D, Farnetti E, Chen Q, Macchioni P, Catanoso MG, Pulsatelli L, Meliconi R, Salvarani C: Vascular endothelial growth factor gene polymorphisms in giant cell arteritis. J Rheumatol. 2003, 30: 2160-2164.
Rueda B, Lopez-Nevot MA, Lopez-Diaz MJ, Garcia-Porrua C, Martin J, Gonzalez-Gay MA: A functional variant of vascular endothelial growth factor is associated with severe ischemic complications in giant cell arteritis. J Rheumatol. 2005, 32: 1737-1741.
Salvarani C, Casali B, Nicoli D, Farnetti E, Macchioni P, Catanoso MG, Chen Q, Bajocchi G, Boiardi L: Endothelial nitric oxide synthase gene polymorphisms in giant cell arteritis. Arthritis Rheum. 2003, 48: 3219-3223. 10.1002/art.11307.
Amoli MM, Garcia-Porrua C, Llorca J, Ollier WE, Gonzalez-Gay MA: Endothelial nitric oxide synthase haplotype associations in biopsy-proven giant cell arteritis. J Rheumatol. 2003, 30: 2019-2022.
Jacobsen S, Baslund B, Madsen HO, Tvede N, Svejgaard A, Garred P: Mannose-binding lectin variant alleles and HLA-DR4 alleles are associated with giant cell arteritis. J Rheumatol. 2002, 29: 2148-2153.
Salvarani C, Gabriel SE, O'Fallon WM, Hunder GG: The incidence of giant cell arteritis in Olmsted County, Minnesota – apparent fluctuations in a cyclic pattern. Ann Intern Med. 1995, 123: 192-194.
Seo P, Stone JH: Large-vessel vasculitis. Arthritis Rheum. 2004, 51: 128-139. 10.1002/art.20083.
Hoffman G: Large-vessel vasculitis. Unresolved issues. Arthritis Rheum. 2003, 48: 2406-2414. 10.1002/art.11243.
Schmits R, Kubuschok B, Schuster S, Preuss K-D, Pfreudschuh M: Analysis of the B cell repertoire against autoantigens in patients with giant cell arteritis and polymyalgia rheumatica. Clin Exp Immunol. 2002, 127: 379-385. 10.1046/j.1365-2249.2002.01751.x.
Duhaut P, Berruyer M, Pinede L, Demolombe-Rague S, Loire R, Seydoux D, Dechavanne M, Ninet J, Pasquier J, for the Groupe de Recherche sur l'Artérite à Cellules Géantes: Anticardiolipin antibodies and giant cell arteritis. Arthritis Rheum. 1998, 41: 701-709. 10.1002/1529-0131(199804)41:4<701::AID-ART18>3.0.CO;2-P.
Manna R, Latteri M, Cristiano C, Todaro L, Scuderi F, Gasbarrini G: Anticardiolipin antibodies in giant cell arteritis and polymyalgia rheumatica: a study of 40 cases. Br J Rheumatol. 1998, 37: 208-210. 10.1093/rheumatology/37.2.208.
Praprotnik S, Blank M, Meroni PL, Rozman B, Eldor A, Shoenfeld Y: Classification of anti-endothelial cell antibodies into antibodies against microvascular and macrovascular endothelial cells: the pathogenic and diagnostic implications. Arthritis Rheum. 2001, 44: 1484-1494. 10.1002/1529-0131(200107)44:7<1484::AID-ART269>3.0.CO;2-Q.
Salmon JE, Pricop L: Human receptors for immunoglobulin G: key elements in the pathogenesis of rheumatic disease. Arthritis Rheum. 2001, 44: 739-750. 10.1002/1529-0131(200104)44:4<739::AID-ANR129>3.0.CO;2-O.
Ravetch JV, Bolland S: IgG Fc Receptors. Annu Rev Immunol. 2001, 19: 275-290. 10.1146/annurev.immunol.19.1.275.
Takai T: Roles of Fc receptors in autoimmunity. Nat Rev Immunol. 2002, 2: 580-592.
Regnault A, Lankar D, Lacabanne V, Rodriguez A, Théry C, Rescigno M, Saito T, Verbeek S, Bonnerot C, Ricciardi-Castagnoli P, et al: Fcg receptor-mediated induction of dendritic cell maturation and major histocompatibility complex class I-restricted antigen presentation after immune complex internalisation. J Exp Med. 1999, 189: 371-380. 10.1084/jem.189.2.371.
Gonzalez-Gay MA, Garcia-Porrua C, Vazquez-Caruncho M, Dababneh A, Hajeer A, Ollier WE: The spectrum of polymyalgia rheumatica in northwestern Spain: incidence and analysis of variables associated with relapse in a 10 year study. J Rheumatol. 1999, 26: 1326-1332.
Hunder GG, Bloch DA, Michel BA, Stevens MB, Arend WP, Calabrese LH, Edworth SM, Fauci AS, Leavitt RY, Lie JT, et al: The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum. 1990, 33: 1122-1128.
Warmerdam PA, Nabben NMJ, van de Graaf SA, van de Winkel JG, Capel PJ: The human low affinity immunoglobulin G Fc receptor IIC gene is a result of an unequal cross-over event. J Biol Chem. 1993, 268: 7346-7349.
Morgan AW, Keyte VH, Babbage SJ, Robinson JI, Ponchel F, Barrett JH, Bhakta BB, Bingham SJ, Buch MH, Conaghan PG, et al: FcgRIIIA-158V and rheumatoid arthritis. A confirmation study. Rheumatology (Oxford). 2003, 42: 528-533. 10.1093/rheumatology/keg169.
Morgan AW, Barrett JH, Griffiths B, Subramanian D, Robinson JI, Keyte VH, Ali M, Jones EA, Old RW, Ponchel F, et al: Analysis of Fcg receptor haplotypes in rheumatoid arthritis. FCGR3A remains a major susceptibility gene at this locus with an additional contribution from FCGR3B. Arthritis Res Therapy. 2005, 8: R5-10.1186/ar1847.
Su K, Wu J, Edberg JC, McKenzie SE, Kimberly RP: Genomic organization of classical human low-affinity Fcgamma receptor genes. Genes Immun. 2002, 3 (Suppl 1): S51-S56. 10.1038/sj.gene.6363879.
Zhao JH, Curtis D, Sham PC: Model-free analysis and permutation tests for allelic associations. Hum Hered. 2000, 50: 133-139. 10.1159/000022901.
Zaykin DV, Westfall PH, Young SS, Karnoub MA, Wagner MJ, Ehm MG: Testing association of statistically inferred haplotypes with discrete and continuous traits in samples of unrelated individuals. Hum Hered. 2002, 53: 79-91. 10.1159/000057986.
Cordell HJ, Clayton DG: A unified stepwise regression procedure for evaluating the relative effects of polymorphisms within a gene using case/control or family data: application to HLA in Type 1 diabetes. Am J Hum Genet. 2002, 70: 124-141. 10.1086/338007.
Fallin D, Cohen A, Essioux L, Chumakov I, Blumenfeld M, Cohen D, Schork NJ: Genetic analysis of case/control data using estimated haplotype frequencies: application to APOE locus variation and Alzheimer's disease. Genome Res. 2001, 11: 143-151. 10.1101/gr.148401.
Fijen CAP, Bredius RGM, Kuijper EJ: Polymorphism of IgG Fc receptors in meningococcal disease. Ann Intern Med. 1993, 119: 636-
Musser JM, Kroll JS, Granoff DM, Moxon ER, Brodeur BR, Campos J, Dabernat H, Frederikson W, Hamel J, Hammond G, et al: Global genetic structure and molecular epidemiology of encapsulated Haemophilus influenzae. Rev Infect Dis. 1990, 12: 75-111.
Domingo P, Muñiz-Diaz E, Baraldès MA, Arilla M, Barquet N, Pericas R, Juárez C, Madoz P, Vázquez G: Associations between Fc gamma receptor IIA polymorphisms and the risk and prognosis of meningococcal disease. Am J Med. 2002, 112: 19-25. 10.1016/S0002-9343(01)01047-6.
Dijstelbloem HM, Scheepers RHM, Oost WW, Stegeman CA, van der Pol WL, Sluiter WJ, Kallenberg CGM, van de Winkel JGJ, Tervaert JWC: Fcg receptor polymorphisms in Wegener's granulomatosis: risk factors for disease relapse. Arthritis Rheum. 1999, 42: 1823-1827. 10.1002/1529-0131(199909)42:9<1823::AID-ANR5>3.0.CO;2-X.
Acknowledgements
This work was supported by a grant from The Health Foundation and Dr Ann Morgan is currently funded by the Arthritis Research Campaign, UK.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
AWM participated in the design of the study, oversaw all aspects of the laboratory work, analysed the data and prepared the manuscript. JIR, AW and SJB undertook the genotyping assays on DNA prepared in the laboratory of WERO and JHB provided additional statistical support. MAG-G and JM participated in the collection of clinical data and the recruitment of patients into this study. WERO and JDI participated in the design of the study, interpretation of the results and writing of the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Morgan, A.W., Robinson, J.I., Barrett, J.H. et al. Association of FCGR2A and FCGR2A-FCGR3Ahaplotypes with susceptibility to giant cell arteritis. Arthritis Res Ther 8, R109 (2006). https://doi.org/10.1186/ar1996
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/ar1996