
Abstract
Objective
To assess effectiveness and safety of a generic fixed-dose combination of tenofovir (TDF)/emtricitabine (FTC)/efavirenz (EFV) among HIV-1-infected patients in Western India.
Methods
Antiretroviral (ARV)-naive and experienced (thymidine analog nucleoside reverse transcriptase inhibitor [tNRTI] replaced by TDF) patients were started on a regimen of 1 TDF/FTC/EFV pill once a day. They were followed clinically on a periodic basis, and viral loads and CD4 counts were measured at 6 and 12 months. Creatinine clearance was calculated at baseline and at 6 months and/or as clinically indicated. Effectiveness was defined as not having to discontinue the regimen due to failure or toxicity.
Results
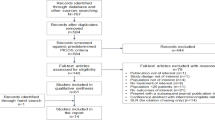
One hundred forty-one patients who started TDF/FTC/EFV before 1 June 2007 were eligible. Of these, 130 (92.2%) and 44 (31.2%) had 6- and 12-months follow-up, respectively. Thirty-five percent of the patients were ARV-naive. Eleven patients discontinued treatment (4 for virologic failure, 1 for grade 3–4 central nervous system disturbances, 4 for grade 3–4 renal toxicity, and 2 for cost). Ninety-six percent of patients were virologically suppressed at 6 months. Frequency of TDF-associated grade 3–4 renal toxicity was 2.8%; however, 3 of these patients had comorbid conditions associated with renal dysfunction.
Conclusion
A fixed-dose combination of generic TDF/FTC/EFV is effective in ARV-naive and experienced patients. Although frequency of severe renal toxicity was higher than has been reported in the literature, it was safe in patients with no comorbid renal conditions.
Similar content being viewed by others


Introduction
Antiretroviral therapy (ART) has significantly improved clinical outcomes of HIV-infected individuals in the developed and developing world.[1, 2] Generic fixed-dose thymidine analog nucleoside reverse transcriptase inhibitor (tNRTI)-based combinations have been effective in achieving virologic, immunologic, and clinical success in the developing world.[3, 4] However, reports are emerging about the long-term complications associated with tNRTIs, particularly those mediated by mitochondrial toxicity, including lipodystrophy, dyslipidemia, hyperlactatemia, and peripheral neuropathy.[5] Due to the concern of long-term toxicity associated with tNRTIs, particularly stavudine, ART guidelines around the world have recommended using these drugs sparingly. Nucleos(t)ide backbonesusing nonthymidine NRTIs (including tenofovir [TDF] and abacavir) have been found to be effective and safe over the long-term. In most of the developed world, these drugs are the preferred option to begin ART in naive HIV-infected individuals.[6]
Adherence has a major effect on treatment outcomes. Pill burden and scheduling are 2 of the factors associated with suboptimal adherence. A fixed-dose combination of TDF/emtricitabine (FTC)/efavirenz (EFV) combines the benefit of low pill burden (1 pill) with the simplest scheduling (once daily). A generic combination of these drugs has been available in India since September 2006 (Viraday; Cipla; Mumbai). However, there are no data on the effectiveness and safety of this combination. We assessed virologic, immunologic, and clinical benefits and safety of this combination in HIV-infected Indian patients.
Methods
Setting
This observational study was conducted at a private tertiary referral HIV care center in Pune, Western India. Patients paid for their own drugs and laboratory investigations. The study was approved by an independent ethics committee.
Patients
From September 2006 to June 2007, HIV-1 infected adult patients initiating a fixed-dose combination of TDF/FTC/EFV were consecutively recruited into the study. Only patients who could afford the combination were started on this regimen. Patients with a minimum of 6-months follow-up were eligible for analysis. Patients were divided into antiretroviral (ARV)-naive and antiretroviral-experienced (substituting TDF for tNRTI because of toxicity, convenience, or proactive change) groups. Before substitution, virologic suppression (plasma viral load [PVL] <400 copies/mL) was confirmed if the patient had been on the previous regimen for more than 6 months.
Drugs
A generic combination of TDF/FTC/EFV was approved for use in HIV-infected patients in India in September 2006. The dose regimen was 1 pill once a day, and patients were asked to take the pill preferably on an empty stomach at night. Patients were assessed for readiness to begin treatment before starting the regimen and were warned about the adverse events (particularly central nervous system [CNS] disturbances) associated with EFV use.
Assessments
Patients were followed up 1 month after treatment initiation and quarterly thereafter. At each follow-up visit, patients were assessed for complications, such as the immune reconstitution inflammatory syndrome (IRIS) and acute toxicity. Adherence was determined by self-report and the patient's ability to keep the follow-up appointments. CD4 counts (FACSCount; Becton Dickinson; Franklin Lakes, New Jersey) and PVLs (Cobas Amplicor, Roche version 1.5) were determined every 6 months (PVLs were determined only in patients who could afford to pay for assays). Urinalysis and measurement of serum creatinine levels were done at baseline and every 6 months or as clinically indicated. Creatinine clearance (CrCl) was calculated using the Cockroft-Gault formula. Virologic failure was defined as inability to achieve or maintain an undetectable PVL (<400 copies/mL) at or after 6 months of initiation of TDF/FTC/EFV, or rebound of viral loads to above detectable limits (excluding blips) after suppression.
Immunologic failure was defined as a decline >50% from on-treatment peak CD4 values or a return to, or a fall below, pretherapy baseline levels after 6 months of therapy and persistent CD4 cells below 100/mm3 after 6 months of treatment.
Clinical failure was defined as new or recurrent WHO stage 4 HIV/AIDS 6 months after initiation of the regimen.
Virologic and immunologic failures were reconfirmed 2 to 4 weeks later by repeated determinations of PVL and CD4 counts, respectively.
IRIS was defined as occurrence of a new or paradoxical worsening of an existing clinical condition (infectious or noninfectious) within 6 months of initiation of ART.
Toxicity was graded according the system mentioned in the WHO ART scale-up guidelines (modified from the grading system of Division of AIDS, National Institute of Allergic and Infectious diseases, USA). The regimen was discontinued (substituted with nonoffending ARV drugs) in cases of grade 3–4 toxicity.
Statistical Analysis
The proportion of patients who discontinued treatment (because of failure or toxicity) was determined. Median CD4 counts before and after initiation of the regimen were determined at 6 and 12 months of follow-up. Univariate analysis was used to determine the risk for grade 3–4 renal toxicity with age, gender, pretherapy CD4 counts and CrCl, body mass index, background risk factors for renal disease, duration of HIV infection since diagnosis, WHO clinical stage at baseline, ART-naive or experienced, and duration on TDF/FTC/EFV. Multivariate analysis was not done because of the small number of grade 3–4 TDF nephrotoxicity events. All analyses reported are for the"as-treated" population.
Results
Patients and Follow-up
One hundred forty-one patients enrolled before 1 June 2007 were included in the final analysis. Of these, 49 (34.7%) patients were ARV-naive and 92 (65.3%) patients were ARV-experienced (TDF substituted for reasons mentioned in Table 1). The total follow-up time for all patients was 1285 months, 130 (92.2%) and 44 (31.2%) patients had at least 6- and 12-months follow-up, respectively. Eight patients (5.6%) were lost to follow-up (defined as not having been seen in the clinic for more than 6 months after the last visit). Table 1 summarizes the pretherapy characteristics of patients. The median duration of ARV exposure before initiation of TDF/FTC/EFV in the ARV-experienced group was 12 months (range, 1 to 81 months).
Treatment Effectiveness
Median self-reported adherence was 96.6%. Four patients needed to change ART because of ARV failure (Table 2). At 6 months, 96% of patients had PVL <400 copies/mL (data on PVL available on 102 of 130 patients at 6 months, as treated analysis). Table 2 summarizes the reasons for treatment discontinuations in patients initiating TDF/FTC/EFV.
The median change in CD4 counts at 6 and 12 months among ARV-naive patients was +168 cells/microliter (mcL) and +368 cells/mcL, respectively. The median change in CD4 counts at 6 and 12 months among ARV-experienced patients was +114 cells/mcL and +176 cells/mcL, respectively. None of the patients receiving the regimen had immunologic or clinical failure.
Thirteen patients (11 ARV-naive and 2 ARV-experienced) developed IRIS on TDF/FTC/EFV (8 cases of tuberculosis, 1 of cytomegalovirus vitreitis, 1 of hepatitis B virus, 1 of Pneumocystis jiroveci pneumonia, 1 of herpes zoster, and 1 of cryptococcal meningitis). One patient with life-threatening tuberculous IRIS temporarily discontinued the regimen.
Safety
The major toxicity associated with TDF/FTC/EFV was EFV-induced CNS neuropsychiatric manifestations. Sixteen patients had grade 1–2 self-limiting events, but 1 patient had grade 4 CNS disturbances necessitating treatment discontinuation.
Four patients (2.8%) discontinued the regimen because of grade 3–4 renal toxicity. The median duration to development of nephrotoxicity was 2 months (1 to 12 months). Three patients had a comorbid condition potentially associated with renal disturbance (1 patient had a single kidney, but normal CrCl at baseline; 1 patient had hypertension; and chronic urinary tract infection, and 1 had dehydration). Of 17 patients with such conditions, 3 patients developed grade 3–4 renal toxicity. At 6 months, median serum creatinine and CrCl were 1 mg/dL (range, 0.4 to 8.1) and 86.22 mL/minute (min) (range, 9.92 to 153.75), a change of 0.36 mL/min from baseline. Only the above-mentioned 4 patients and 1 other patient (who died of thrombotic thrombocytopenic purpura) had a CrCl<50 mL/min on follow-up. On univariate analysis, only CrCl at baseline was associated with grade 3–4 nephrotoxicity, with a relative risk ratio of 0.89 (95% CI, 0.83 to 0.96, P =.004).
Discussion
We have demonstrated the short-term effectiveness and safety of a generic fixed-dose combination of TDF/FTC/EFV. This 1-pill/once-a-day regimen was associated with high levels of adherence and with minimal treatment-limiting toxicity. Antiretroviral scale-up programs may consider this regimen a better option than those provided currently to enhance adherence, improve treatment success, and limit tNRTItoxicity.
There are numerous advantages of using fixed-dose combinations for treatment of HIV infection, and they are widely recommended to be used in both the developed and developing world.[7] Fixed-dose combinations reduce pill burden, thus improving adherence; are cheaper than separate drugs; ensure that all the drugs in the combination are taken; lead to fewer prescription errors; and simplify program management. Disadvantages, while few, include difficulty in adjusting the dose, such as in cases of renal failure, and the need to discontinue the entire formulation if 1 component of the combination causes a treatment-limiting adverse event. An additional concern with the once-daily regimen is the potential for less "forgiveness" in the event of missed doses.
A fixed-dose combination of TDF/FTC/EFV was found to be bioequivalent to the individual formulations.[8] Generic fixed-dose combinations have been found to be of good quality, and many have been prequalified by World Health Organization and United States Food and Drug Administration for use in ART scale-up programs.
There are advantages in starting with a TDF-based regimen. In randomized, controlled trials, a combination of TDF/FTC/EFV was found to be superior to zidovudine (ZDV)/lamivudine (3TC)/EFV and d4T/3TC/EFV.[9, 10] Treatment discontinuation rates among the comparison groups were higher in these studies than have been reported by others. In the Gilead 934 trial,[9] CD4 improvements were greater in the TDF/FTC/EFV group than in the ZDV/3TC/EFV group, possibly related to ZDV bone-marrow suppression. Finally, a systematic overview of clinical trials found that TDF/3TC or FTC combined with EFV achieved better virologic responses than did other nucleoside backbones.[11] In our study, we have been able to show robust immunologic and virologic responses, with 96% of patients (on as-treated analysis) achieving undetectable viral loads at 6 months on therapy.
There have been reports that treatment-limiting toxicity associated with currently recommended first-line regimens in the developing world is common. Most toxicity is associated with use of tNRTIs. A significant proportion of patients develop morphologic and metabolic complications with use of d4T; these complications are also reported with long-term use of ZDV at a lesser frequency.[5] Many patients cannot tolerate d4T or ZDV; for these patients, changing to TDF or abacavir is the only option. Substituting one of these drugs has been shown to sustain treatment effectiveness and mitigate some tNRTI toxicity.[12] In India, abacavir is more expensive than TDF, is not currently produced as a fixed-dose combination with 3TC, and is not available as a once-daily pill in combination with EFV. Additionally, the prevalence of HLA-B*5701 associated with the abacavir hypersensitivity syndrome is unknown. For these reasons, it is better to change to TDF/FTC/EFV for patients experiencing NRTI toxicities or even to proactively prevent development of some of the long-term toxicities. In our study, we demonstrated continued virologic suppression and immunologic benefit in patients who, for these reasons, changed to the TDF/FTC/EFV regimen.
There has been a concern about renal toxicity associated with TDF, although most studies have demonstrated low frequencies.[13–15] In the Gilead 903 study,[10] no patients discontinued TDF for renal toxicity through 288 weeks on treatment. TDF renal toxicity usually occurs months after initiation of therapy (range, 5 to 26 months); however, it does occur within 8 weeks of initiation of treatment in a significant subset of patients.[16, 17] Greater decreases in renal function have been described when TDF is used along with a protease inhibitor-based regimen than when it is used with a nonnucleoside RTI (NNRTI).[18] In our patient population, the frequency of grade 3–4 renal complications were a little higher than those reported from other observational studies.[15] However, most patients with renal complications had comorbid renal conditions. All of these events occurred within 6 months of initiation. Monitoring for TDF nephrotoxicity is recommended, especially in patients with background renal disease and low CrCl at baseline. Measuring serum creatinine levels is inexpensive (approximately US$1) and hence can be made widely available for periodic monitoring of renal toxicity in ARV scale-up programs.
The frequency of adverse events associated with other drugs in the regimen (FTC, EFV) was similar to that described when these drugs were used in non-TDF-based regimens.[10] CNS disturbances due to EFV were the most common toxicity associated with this regimen. Treatment was discontinued in 1 patient due to severe EFV-induced CNS problems. We routinely warned the patients about this toxicity and assured them that the symptoms were self-limiting, and this may have contributed to underreporting. None of our patients reported hyperpigmentation associated with FTC.
Other advantages of initiating ART with a TDF/FTC/EFV is effectiveness in treating concomitant chronic hepatitis B virus infection, and a possible sequencing advantage even if failure is identified late. The frequency of the K65R resistance mutation associated with TDF is low.[19] Even in the presence of K65R, tNRTIs would be effective components of second-line regimens.[20] Failing of tNRTIs leads to accumulation of thymidine analog resistance mutations that can compromise the entire NRTI class.
There are a few limitations in using this regimen as first-line therapy in the developing world. TDF/FTC/EFV is the most expensive of the NNRTI-based regimens, and the generic version costs around US$1200 per year. All patients in our study belonged to a higher socioeconomic class and paid for their own treatment. However, it would be reasonable to assume that this regimen would become cheaper with time, particularly if demand increases. Another limitation is the teratogenic effect associated with EFV, which necessitates careful use or avoidance of this regimen in women who are pregnant or who may becomepregnant.
Although our study is observational and has limited follow-up, it does demonstrate the effectiveness of generically manufactured fixed-dose combination of TDF/FTC/EFV. Although grade 3–4 renal toxicity was common in the study, the regimen was safe in patients who did not have comorbid renal conditions. Further studies are needed to confirm these observations. Finally, the patients accessing care at our private clinic may differ from those who would access free programs, which limits generalizability of the conclusions. To our knowledge, this is the first report on the use of a fixed-dose combination of TDF/FTC/EFV in clinical practice, especially in the developing world. With the numerous advantages of this regimen, it is time to position it as first-line therapy for wider use in the developing world.
Authors and Disclosures
Sanjay Pujari, MD, AAHIVS, has disclosed no relevant financial relationships.
Ameet Dravid, MD, has disclosed no relevant financial relationships.
Nikhil Gupte, PhD, has disclosed no relevant financial relationships.
Kedar Joshi, MD, has disclosed no relevant financial relationships.
Vivek Bele, MD, has disclosed no relevant financial relationships.
References
Palella FJ Jr, Delaney KM, Moorman AC, et al.: Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998, 338: 853–860. Abstract
Kumarasamy N, Solomon S, Chaguturu SK, et al.: The changing natural history of HIV disease: before and after the introduction of generic antiretroviral therapy in southern India. Clin Infect Dis 2005, 41: 1525–1528. Abstract
Laurent C, Kouanfack C, Koulla-Shiro S, et al.: Effectiveness and safety of a generic fixed-dose combination of nevirapine, stavudine, and lamivudine in HIV-1-infected adults in Cameroon: open-label multicentre trial. Lancet 2004, 364: 29–34. Abstract
Pujari S, Patel A, Eknath N, et al.: Effectiveness of generic fixed-dose combinations of highly active antiretroviral therapy for treatment of HIV infection in India. J Acquir Immune Defic Syndr 2004, 37: 1566–1569. Abstract
Pujari SN, Dravid A, Naik E, et al.: Lipodystrophy and dyslipidemia among patients taking first-line, World Health Organization-recommended highly active antiretroviral therapy regimens in Western India. J Acquir Immune Defic Syndr 2005, 39: 199–202. Abstract
Hammer SM, Saag MS, Schechter M, et al.: Treatment for adult HIV infection: 2006 recommendations of the International AIDS Society-USA panel. JAMA 2006, 296: 827–843. Abstract
World Health Organization: Antiretroviral therapy for HIV infection in adults and adolescents in resource limited settings: towards universal access. [http://www.who.int]
Mathaiss AA, Hinkle J, Menning M, et al.: Bioequivalence of efavirenz/emtricitabine/tenofovir disoproxil fumarate single tablet regimen. J Acquir Immune Defic Syndr 2007, in press.
Pozniak AL, Gallant JE, DeJesus E, et al.: Tenofovir disoproxil fumarate, emtricitabine, and efavirenz versus fixed-dose zidovudine/lamivudine and efavirenz in antiretroviral-naive patients: virologic, immunologic, and morphologic changes–a 96-week analysis. J Acquir Immune Defic Syndr 2006, 43: 535–540. Abstract
Gallant JE, Staszewski S, Pozniak A, et al.: Efficacy and safety of tenofovir DF vs stavudine in combination therapy in antiretroviral naive patients: a 3 year randomized trial. JAMA 2004, 292: 191–201. Abstract
Bartlett JA, Chen SS, Quinn JB: Comparative efficacy of nucleoside/nucleotide reverse transcriptase inhibitors in combination with efavirenz: results of a systematic overvirew. HIV Clin Trials 2007, 8: 221–226. Abstract
Milinkovic A, Martinez E, Lopez S, et al.: The impact of reducing stavudine dose versus switching to tenofovir on plasma lipids, body composition and mitochondrial function in HIV-infected patients. Antivir Ther 2007, 12: 407–415. Abstract
Cassetti I, Madruga JV, Suleiman JM, et al.: The safety and efficacy of tenofovir DF in combination with lamivudine and efavirenz through 6 years in antiretroviral-naive HIV-1-infected patients. HIV Clin Trials 2007, 8: 164–172. Abstract
Gallant JE, Parish MA, Keruly JC, et al.: Changes in renal function associated with tenofovir disoproxil fumarate treatment, compared with nucleoside reverse-transcriptase inhibitor treatment. Clin Infect Dis 2005, 40: 1194–1198. Abstract
Nelson MR, Katalama C, Montaner JS, et al.: The safety of tenofovir disoproxil fumarate for the treatment of HIV infection in adults: the first 4 years. AIDS 2007, 21: 1273–1281. Abstract
Patel SM, Zembower TR, Pallela F, et al.: Early onset of tenofovir induced renal failure: Case report and review of literature. Scientific World Journal 2007, 7: 1140–1148. Abstract
Malik A, Abraham P, Malin N: Acute renal failure and Fanconi syndrome in an AIDS patient on tenofovir treatment-case report and review of literature. J Infect 2005, 51: E61-E65. Abstract
Goicoechea M, Liu S, Best B, et al.: Greater tenofovir associated renal dysfunction decline with protease inhibitor based versus non-nucleoside reverse transcriptase inhibitor based therapy. J Infect Dis 2008, 197: 102–108.
Margot NA, Lu B, Cheng A, et al.: Resistance development over 144 weeks in treatment-naive patients receiving tenofovir disoproxil fumarate or stavudine with lamivudine and efavirenz in Study 903. HIV Med 2006, 7: 442–450. Abstract
Gallant JE: Drug resistance after failure of initial antiretroviral therapy in resource limited countries. Clin Infect Dis 2007, 44: 453–455. Abstract
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Pujari, S., Dravid, A., Gupte, N. et al. Effectiveness and Safety of Generic Fixed-Dose Combination of Tenofovir/Emtricitabine/Efavirenz in HIV-1-Infected Patients in Western India. JIAS 10, 196 (2008). https://doi.org/10.1186/1758-2652-10-8-196
Published:
DOI: https://doi.org/10.1186/1758-2652-10-8-196