
Abstract
Background
Active transportation to school is an important contributor to the total physical activity of children and adolescents. However, active school travel has declined over time, and interventions are needed to reverse this trend. The purpose of this paper is to review intervention studies related to active school transportation to guide future intervention research.
Methods
A systematic review was conducted to identify intervention studies of active transportation to school published in the scientific literature through January 2010. Five electronic databases and a manual search were conducted. Detailed information was extracted, including a quantitative assessment comparing the effect sizes, and a qualitative assessment using an established evaluation tool.
Results
We identified 14 interventions that focused on active transportation to school. These interventions mainly focused on primary school children in the United States, Australia, and the United Kingdom. Almost all the interventions used quasi-experimental designs (10/14), and most of the interventions reported a small effect size on active transportation (6/14).
Conclusion
More research with higher quality study designs and measures should be conducted to further evaluate interventions and to determine the most successful strategies for increasing active transportation to school.
Similar content being viewed by others


Introduction
Currently, there is evidence that daily activities, including active transportation to school (defined as the use of active means, such as walking and bicycling to and from school), may have important health implications for young people. Active travel has been positively associated with higher daily levels of physical activity [1, 2] and higher cardiorespiratory fitness [3, 4]; but rates of active transportation to school have declined dramatically over the past 30 years [5]. Initiatives such as Safe Routes to School (SRTS), the Walking School Bus (WSB), or the Walk to School (WTS) program have been implemented to increase children's walking and bicycling to school with some success.
The earliest peer-reviewed intervention study targeting walking and bicycling to and from school was published in 2003, and since then the field has progressed in the design and development of interventions. Research in this area has grown in recent years, and literature reviews have been conducted on patterns of commuting to school and relationships with physical activity and other health outcomes [6–14]. However, a comprehensive review of methodology and outcomes of interventions is lacking. Therefore, in our systematic review of active transportation to school interventions published in the scientific literature, we extracted the key components and methodology for each study and assessed its quality and effectiveness to highlight both the approaches that were most successful and issues that should be addressed in future research.
Methods
Search strategy
A literature search was conducted using five electronic databases: MEDLINE (PubMed), Web of Science (SCI and SSCI), SPORT Discus, Cochrane library, and the National Transportation Library. Three categories of search terms were identified: school-age children, active transportation, and interventions. Specific terms used in the search were obtained from active transportation to school review studies [6, 7], from the subject headings (MeSH list) within PubMed, and from the librarian's and researchers' expertise, and then adapted for each database (see additional File 1 for more detail). In addition to these electronic databases, reference lists in review papers [6–14] and our own archives of published documents were also reviewed. All English language publications through January 2010 were included.
Selection and review process
Once the list of potentially relevant studies was compiled, titles and abstracts were reviewed to determine if the articles met the following four inclusion criteria: 1) focus on children and adolescents (6-18 y); 2) address active transportation to school; 3) contain an intervention; and 4) include at least one outcome or indicator of active transportation or physical activity. Any disagreements in the inclusion process were resolved through discussion among authors. Data were then extracted from the articles, including descriptive information, indicators of study quality, intervention strategies employed, and effectiveness. All the data extracted were checked by two researchers; if no agreement was reached, a third author adjudicated.
Quality assessment
The quality assessment was conducted using a standardized evaluation framework, the Evaluation of Public Health Practice Projects (EPHPP) [15]. EPHPP assesses six methodological dimensions: selection bias, study design, confounders, blinding, data collection methods, and withdrawals and dropouts, all of which feed into the calculation of a global rating. Each dimension is rated on a three-point scale: strong, moderate, or weak. Two additional methodological dimensions provided by the tool, but not involved in the global rating, are intervention integrity and analyses. The EPHPP tool was created primarily for individual level observational and clinical studies based on populations; consequently, rating criteria for some items were modified by authors to improve the suitability of the tool for the interventions included in this review. These criteria are attached in additional File 2.
Intervention strategy framework
The intervention design for each study was examined using a standardized intervention framework: the Active Living by Design (ALBD) Community Action Model [16]. The Community Action Model is an ecologic framework with multi-level strategies to increase physical activity and has been successfully applied in studies of active transportation to school [17]. This framework outlines five strategies: Preparation, time deliberately taken to plan and develop strategy for an initiative; Promotions, educating and encouraging targeted individuals; Programs, organized activities that engage individuals in physical activity; Policies, written and unwritten rules or standards that affect physical activity; and Physical, projects to create opportunities and remove barriers for physical activity. The 5 P's of the Community Action Model were abstracted from intervention strategies explicitly mentioned in the text of each study, as applying to active transportation to school.
Effectiveness assessment
The effectiveness assessment was conducted by calculating the effect size using Cohen's d. Effect size was calculated between experimental and control groups, or between baseline and follow-up for the experimental group. The calculations were individualized for each study, using standardized mean or proportion differences [18], t statistics, or P values [19–21]. This information is detailed in additional File 3. The Cohen's d was divided into five levels: trivial (Cohen's d ≤ 0.2), small (>0.2), moderate (>0.5), large (>0.8), and very large (>1.3) [22].
Results
Study selection
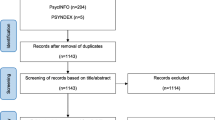
The electronic search strategy produced 6311 papers among the five databases: 949 from PubMed, 807 from Web of Science, 243 from Cochrane Library, 2802 from SPORT Discus, and 1510 from the National Transportation Library. After discarding 380 duplicates, 5931 papers remained.
From these 5931 papers, 15 papers were identified for consideration based on a review of titles and abstracts; and an additional 10 papers were located through a manual search process. These 25 were thoroughly read, and 11 were excluded in a second selection process because they failed to meet inclusion criteria. Thus, 14 intervention studies relating to active transportation to school were selected and included in this review. Because two papers from Boarnet, et al. [23, 24] reported on the same intervention study, results from these two papers were presented as one.
Study population
Characteristics of the different interventions about active transportation to school are presented in Table 1. The 14 studies took place on three continents (America, Oceania, and Europe). Eight studies were conducted in the United States (three in California, and one each in Nebraska, Utah, New Mexico, Washington, and Michigan) [23–31], three studies in Australia [32–34], and two studies in the United Kingdom [35, 36]. Most of the interventions discussed in the studies focused on urban settings.
All the studies focused on children (from age 5 to 12 y) and were set in elementary schools. However, one study also included adolescents from middle school to age 15 y [30]. The number of participants showed high variation across the intervention studies, from two studies that reported very small samples of 11 [29] and 22 [27] participants, to four studies that reported samples between 1300 to 2000 students [24, 30, 33, 36].
Quality assessment
The quality assessment of the interventions was conducted using the EPHPP tool. All studies were evaluated as weak in the global rating, and an analysis of the individual items is reported in Table 2. None of the studies included a sample representative of the school population, and only two (classified as moderate in selection bias) included a school sample somewhat likely to be representative of the population [25, 28]. Three studies were rated as strong, with randomized controlled trial study designs [29, 33, 36]. Most of the study designs were moderately rated, with quasi-experimental designs (two group pre + post [25, 26, 28, 35] or just one group pre + post [24, 30, 31, 34]). Three interventions were weak [23, 27, 32] because they had only post measures or were conducted as observational studies. Most of the interventions did not take into account confounders; the three studies that did include confounders were rated as moderate [28, 36] and strong [33]. Blinding or masking in most of the studies was assessed as moderate [23–26, 28–32, 36], and four studies were rated as weak [27, 33–35]. Mediators were not assessed in any of the examined interventions; similarly, the studies generally failed to describe their theoretical frameworks.
The assessment method for collecting data on the primary outcome (active transportation to school) was self-report by children [25, 28, 30, 34, 35], parents [23, 24, 26, 32, 36], or both children and parents [27, 33]. Mode and frequency of transportation to school were usually asked, but the form of the questions and the way of asking them differed for each study. Only three studies reported evidence of validity [25, 29] or reliability [25, 26, 29] for the measurement instruments, and were rated as either moderate [26] or strong [25, 29]. Regarding the withdrawals and dropout criteria, only those interventions that reported more than 60% of participants completing the study obtained a strong [29, 35, 36] or moderate [27] rating.
In describing intervention integrity, three studies reported the percentage of participants receiving the allocated intervention [28, 32, 36]. Only four studies measured the consistency of the intervention [25, 28, 32, 36], and none of the studies reported contamination that might influence the results. The unit of intervention allocation in most of the studies was the school, except for two studies where it was the individual [27, 29]. The unit of analysis was the individual in nine studies, and it was the school in five others [24, 31, 33–35]. In two studies [30, 31], the active transportation measure did not include the same schools at multiple time points. Several studies did not account for school clustering or used inappropriate statistical methods for the study design [28, 31–33, 35, 36].
Intervention description
Two studies included all five strategies from the Community Action Model [26, 31]. Two other studies included either the four strategies of preparation, promotion, programs, and projects [30] or those of preparation, promotion, programs, and policy [34]. Half the selected studies included the strategies of preparation, promotion, and programs [27–29, 32, 33, 35, 36]. One study included only preparation and program [25], and two others included only projects [23, 24].
Interventions about active transportation to school involved three main elements: schools, parents, and communities. School involvement was the common element in all the interventions, except for Boarnet et al. [23, 24] which focused on infrastructure projects in the community. A majority of the interventions (n = 8) reported the involvement of the school, parents, and the community [26–28, 30, 32–34, 36], and two studies included only school and parental involvement [29, 35]. One study included both school and community involvement [31], and one study included only school involvement [25].
The economic investment in the interventions was reported in several studies. Six interventions reported that one or more people were paid for being leaders [25], staff [30], coordinators [27, 28], teachers [33], or researchers [34]; one study reported payment for the media [32], and another study reported large financial support from several sources for addressing active transportation in the overall community in addition to active travel to school [31]. Moreover, a number of interventions received special government funding (SRTS) for participating and implementing the program [37].
Effectiveness
Almost all the studies reported an increase in the percentage of active transportation to school following the interventions; however, the degree of change varied widely (3% to 64%). Two studies did not report significant improvements in active transportation to school [26, 36]. Two other studies reported improvements, but in other outcomes (increased physical activity levels [29] and longer average distances walked to school [35]).
Based on the calculated Cohen's d effect size (additional File 3), three studies produced trivial effect sizes [24, 32, 34], six reported a small effect [23, 25, 28, 30, 31, 36], two reported a large effect [33, 35], and one reported a very large effect [29]. Cohen's d was not calculated for two studies [26, 27] due to insufficient data. The two studies that measured physical activity [29] and the distance walked [35] both reported strong effect sizes.
Discussion
In this review, 14 interventions that promoted active transportation to school among children and adolescents were identified. These interventions were heterogeneous, varying in size, scope, and focus. Weaknesses in the quality of various study components were identified. The most common intervention strategies employed, based on the Community Action Model framework, were preparation, promotion, and programming. Although most interventions showed some improvement in use of active transportation to school, methods used to assess change and effect sizes varied, with only three interventions having a large or very large effect size.
The heterogeneity of the intervention studies, coupled with the overall weaknesses in the quality of the study protocols, limited our ability to draw clear conclusions about which intervention strategies might be most effective. From the cross-sectional literature, it is known that interventions must address a complex and varied array of factors that influence children's modes of travel to school, including the physical environment around the school, economic characteristics of the families, social networks of the children, and cultural norms [7]. However, the lessons learned from the literature need to be more consistently applied to intervention research, and the studies in this review highlight this lack of consistency.
Numerous studies have examined specifically how the physical environment affects active transportation. Cross-sectional studies have consistently shown that distance is the strongest predictor of active transportation to school among children, with longer distances associated with lower rates of active commuting [7, 10, 11]. However, few of the intervention studies account for distance in their study design or analyses. Distance could be considered as part of the inclusion criteria for intervention studies to target students living within a walkable distance to school. Only McKee [35] reported targeting the intervention towards children who lived within three miles from school and who were driven to school. Presumably, interventions using WSB [25, 27–29, 31, 34] or SRTS [23, 24, 30, 31] were conducted within walkable distances, but none of these studies mentioned distance to school as an inclusion criterion. Additionally, studies could take distance into account in their statistical analyses, especially if randomization has not occurred. Studies with these weaknesses could underestimate their results, since more than two or three miles from school is often considered a distance not typically walked for school [35].
While the heterogeneity of the interventions in this review does not allow for clear recommendations about the most effective strategies, they do highlight the importance of getting the right groups involved and working towards a specific goal. National and international active school transportation initiatives like WTS and SRTS both emphasize the importance of identifying the goal and getting all the necessary people or groups involved; however, these aspects are not captured in the Community Action Model framework of strategies employed. The importance of this mixed involvement was highlighted in an evaluation of the United States National WTS program [38] which found that getting more groups involved was critical to expanding the program's reach and engagement. Acquiring buy-in from schools, parents, and community members can be challenging, but may be an essential component in the effectiveness and sustainability of the intervention. The interventions with the highest effectiveness [32–34] shared two common elements: a) a strong involvement of schools through principals and teachers working actively in the intervention, and b) parents receiving specific materials and being encouraged to walk. While teachers may be concerned about crowded curricula [32, 36], participating in one-day events that are unproductive or unsustainable[32], or taking on the extra responsibilities related to school travel [36], parents are often concerned about child and traffic safety [7, 39]. Regarding community involvement, a global intervention based on a partnership approach among the health sector, schools, and local government might be successful, because it has been shown to provide a plan of action and shared responsibilities about active transportation in the community [34]. The quality of parent, school, and community involvement, as well as interaction among these groups, such as regular meetings between school and community groups, may be among the more influential components of active transportation to school interventions.
In addition, interventions focused on active transportation to school may be more effective than those with a broader focus. For example, the Gold Medal Schools program [26] and Project U-Turn [31] both incorporated all five P's of the Community Action Model framework. The Gold Medal Schools program had broad objectives, including to promote better nutrition, regular physical activity, and tobacco prevention, and its results showed only a low, non-significant improvement in rates of active transportation to school. In comparison, Project U-Turn focused solely on active transportation, and showed an increase in rates of active transportation to school from 5% to 15% of students over four years. Of course, this comparison must be interpreted cautiously since the methodology and purposes of the two programs were different.
Active transportation to school is a relatively new research field, and intervention studies are early in their development. While interventions included in this review were hampered by many methodological flaws, as highlighted by their "weak" ratings on the quality assessment measures, the details of the individual component ratings provide insight into ways future studies can be strengthened. Based on the quality assessment instrument, only interventions using experimental designs were rated as high for their study design; however, only three of the intervention studies in this review were so rated [29, 33, 36]. Additionally, the school typically should be used as the unit of randomization, based on the intervention components, as was done in the studies of McKee et al. and Rowland et al. [35, 36] to avoid contamination between experimental and control participants. Another limitation of most studies was that measures used to assess active transportation to school were weak and often lacked evidence of validity or reliability. They differed with regard to the content of the question (e.g., they either assessed only walking or both walking and bicycling), collection methods used (e.g., interview, questionnaire), and time frames recalled (e.g., yesterday, last week). Similar measurement issues have arisen in the literature [10, 33], thus making inter-study comparisons difficult. Future studies should make use of valid and reliable tools for assessing active transportation to school. Moreover, high quality studies should assess mediators, base their interventions on a theoretical framework, and use appropriate statistical methods for their study designs.
Half of the identified interventions reported a small level of effectiveness, meaning that there was only a slight increase in active transportation to school following the intervention. However, an intervention's quality may be related positively to the produced effect size. Both studies with higher quality [29, 36] reported large or very large effect sizes. Another challenge in this review was the variety of methods used to report study effectiveness, making it difficult to compare across studies. Only six of the studies [25, 26, 28, 29, 35, 40] provided p-values used for determining effectiveness of their interventions. The calculation of effect size with the Cohen's d was an important contribution of this review. Therefore, future studies are encouraged to report critical data elements so that effect sizes can be calculated.
Limitations and strengths
This review is not without limitations. First, inter-study comparisons using effectiveness ratings must be considered with caution because different formulas were used for calculating the effect size from the data provided for each study, and only effectiveness ratings calculated with the same formula are completely comparable. A second limitation relates to inclusion criteria. Although experimental designs provide the strongest evidence, we also included non-experimental designs because of the limited number of interventions about active transportation to school. A third limitation concerns the relatively scarce information about details of the interventions, including study design, measurements, and implementation of the intervention (all of which may be due to space restrictions imposed by the journals in which they were published). Fourth, we found some gaps when assessing the quality of the interventions using the EPHPP tool, because this tool was designed primarily for individually-focused studies. Our study group adapted the tool in effort to make it most useful for this review.
To our knowledge, this is the first systematic review of interventions designed to promote active transportation to school among young people. The search strategy used was based on the recommendations of Pai et al. [41] for systematic reviews. A second strength was calculating the effectiveness and examining the quality of the interventions, a methodology that provided detailed insight for future studies. Finally, the rigorous review process for selecting the studies and extracting the data, including both the effectiveness and quality assessments, is a strength.
Conclusion
A detailed discussion of interventions to promote active transportation to and from school among young people has been provided through this review. The main findings are:
-
1)
Existing interventions to promote active transportation to and from school are heterogeneous, due to the size, scope, and focus of the intervention and measurements.
-
2)
Interventions with appropriate school, parent, and community involvement and that work toward a specific goal (i.e., increasing active transportation) seemed to be more effective than interventions that were broader in focus.
-
3)
Intervention quality was often low as measured by the EPHPP tool.
-
4)
Interventions evidenced a small but promising effectiveness in increasing active transportation to school.
A range of methodological issues need to be considered in future interventions, including experimental study designs, valid and reliable data collection methods, and appropriate statistical analysis. Future studies should examine the effect of the parental, school, and community involvement, and address the complexity of multiple factors influencing active transportation to and from school. Long-term outcomes and sustainability of the active transportation to school interventions also should be examined.
References
Rosenberg DE, Sallis JF, Conway TL, Cain KL, McKenzie TL: Active transportation to school over 2 years in relation to weight status and physical activity. Obesity (Silver Spring). 2006, 14: 1771-1776. 10.1038/oby.2006.204.
Cooper AR, Wedderkopp N, Wang H, Andersen LB, Froberg K, Page AS: Active travel to school and cardiovascular fitness in Danish children and adolescents. Med Sci Sports Exerc. 2006, 38: 1724-1731. 10.1249/01.mss.0000229570.02037.1d.
Andersen LB, Lawlor DA, Cooper AR, Froberg K, Anderssen SA: Physical fitness in relation to transport to school in adolescents: the Danish youth and sports study. Scand J Med Sci Sports. 2009, 19: 406-411. 10.1111/j.1600-0838.2008.00803.x.
Voss C, Sandercock G: Aerobic fitness and mode of travel to school in English schoolchildren. Med Sci Sports Exerc. 2010, 42: 281-287.
McDonald NC: Active transportation to school: trends among U.S. schoolchildren, 1969-2001. Am J Prev Med. 2007, 32: 509-516. 10.1016/j.amepre.2007.02.022.
Ogilvie D, Egan M, Hamilton V, Petticrew M: Promoting walking and cycling as an alternative to using cars: systematic review. Br Med J. 2004, 329: 763-766B. 10.1136/bmj.38216.714560.55.
Pont K, Ziviani J, Wadley D, Bennett S, Abbott R: Environmental correlates of children's active transportation: a systematic literature review. Health Place. 2009, 15: 827-840. 10.1016/j.healthplace.2009.02.002.
Lee MC, Orenstein MR, Richardson MJ: Systematic review of active commuting to school and childrens physical activity and weight. J Phys Act Health. 2008, 5: 930-949.
Faulkner GE, Buliung RN, Flora PK, Fusco C: Active school transport, physical activity levels and body weight of children and youth: a systematic review. Prev Med. 2009, 48: 3-8. 10.1016/j.ypmed.2008.10.017.
Davison KK, Werder JL, Lawson CT: Children's active commuting to school: current knowledge and future directions. Prev Chronic Dis. 2008, 5: A100.
Panter JR, Jones AP, van Sluijs EM: Environmental determinants of active travel in youth: A review and framework for future research. Int J Behav Nutr Phys Act. 2008, 5: 34-10.1186/1479-5868-5-34.
McMillan TE: Urban Form and a Child's Trip to School: The Current Literature and a Framework for Future Research. Journal of Planning Literature. 2005, 19: 440-456. 10.1177/0885412204274173.
Tudor-Locke C, Ainsworth BE, Popkin BM: Active commuting to school - An overlooked source of childrens' physical activity?. Sports Med. 2001, 31: 309-313. 10.2165/00007256-200131050-00001.
Sirard JR, Slater ME: Walking and Bicycling to School: A Review. American Journal of Lifestyle Medicine. 2008, 2: 372-396. 10.1177/1559827608320127.
Effective Public Health Practice Project: Quality assessment Tool for Quantitative Studies. [http://www.myhamilton.ca/NR/rdonlyres/6B3670AC-8134-4F76-A64C-9C39DBC0F768/0/QATool.pdf]
Bors P, Dessauer M, Bell R, Wilkerson R, Lee J, Strunk SL: The Active Living by Design national program: community initiatives and lessons learned. Am J Prev Med. 2009, 37: S313-321. 10.1016/j.amepre.2009.09.027.
Fesperman CE, Evenson KR, Rodriguez DA, Salvesen D: A comparative case study on active transport to and from school. Prev Chronic Dis. 2008, 5: A40.
Nakagawa S, Cuthill IC: Effect size, confidence interval and statistical significance: a practical guide for biologists. Biol Rev Camb Philos Soc. 2007, 82: 591-605. 10.1111/j.1469-185X.2007.00027.x.
Hunter J, Schmidt F: Methods of meta-analysis. 1991, Sage Publ
Meta-Analysis: Methods of Accumulating Results Across Research Domains. [http://www.lyonsmorris.com/MetaA/macalc/MApaper.pdf]
Abramowitz M, Stegun I: Handbook of mathematical functions with formulas, graphs, and mathematical tables. 1964, Dover publications
Cohen J: Statistical power analysis for the behavioral sciences, Hillsdale, NJ: L. Book Statistical power analysis for the behavioral sciences, Hillsdale, NJ: L. 1988, City: Erlbaum Associates, (Editor ed.^eds.)
Boarnet MG, Anderson CL, Day K, McMillan T, Alfonzo M: Evaluation of the California Safe Routes to School legislation: urban form changes and children's active transportation to school. Am J Prev Med. 2005, 28: 134-140. 10.1016/j.amepre.2004.10.026.
Boarnet MG, Day K, Anderson C, McMillan T, Alfonzo M: California's Safe Routes to School Program: Impacts on Walking, Bicycling, and Pedestrian Safety. J Am Plann Assoc. 2005, 71: 301-317. 10.1080/01944360508976700.
Heelan KA, Abbey BM, Donnelly JE, Mayo MS, Welk GJ: Evaluation of a walking school bus for promoting physical activity in youth. J Phys Act Health. 2009, 6: 560-567.
Jordan KC, Erickson ED, Cox R, Carlson EC, Heap E, Friedrichs M, Moyer-Mileur LJ, Shen SY, Mihalopoulos NL: Evaluation of the Gold Medal Schools Program. J Am Diet Assoc. 2008, 108: 1916-1920. 10.1016/j.jada.2008.08.002.
Kong AS, Sussman AL, Negrete S, Patterson N, Mittleman R, Hough R: Implementation of a walking school bus: lessons learned. J Sch Health. 2009, 79: 319-325. 10.1111/j.1746-1561.2009.00416.x. quiz 333-314
Mendoza JA, Levinger DD, Johnston BD: Pilot evaluation of a walking school bus program in a low-income, urban community. BMC Public Health. 2009, 9: 122-10.1186/1471-2458-9-122.
Sirard JR, Alhassan S, Spencer TR, Robinson TN: Changes in Physical Activity from Walking to School. Journal of nutrition education and behavior. 2008, 40: 324-326. 10.1016/j.jneb.2007.12.002.
Staunton CE, Hubsmith D, Kallins W: Promoting safe walking and biking to school: the Marin County success story. Am J Public Health. 2003, 93: 1431-1434. 10.2105/AJPH.93.9.1431.
TenBrink DS, McMunn R, Panken S: Project U-Turn: increasing active transportation in Jackson, Michigan. Am J Prev Med. 2009, 37: S329-335. 10.1016/j.amepre.2009.09.004.
Merom D, Rissel C, Mahmic A, Bauman A: Process evaluation of the New South Wales Walk Safely to School Day. Health Promot J Austr. 2005, 16: 100-106.
Wen LM, Fry D, Merom D, Rissel C, Dirkis H, Balafas A: Increasing active travel to school: are we on the right track? A cluster randomised controlled trial from Sydney, Australia. Prev Med. 2008, 47: 612-618. 10.1016/j.ypmed.2008.09.002.
Zaccari V, Dirkis H: Walking to school in inner Sydney. Health Promotion Journal of Australia. 2003, 14: 137-140.
McKee R, Mutrie N, Crawford F, Green B: Promoting walking to school: results of a quasi-experimental trial. J Epidemiol Community Health. 2007, 61: 818-823. 10.1136/jech.2006.048181.
Rowland D, DiGuiseppi C, Gross M, Afolabi E, Roberts I: Randomised controlled trial of site specific advice on school travel patterns. Arch Dis Child. 2003, 88: 8-11. 10.1136/adc.88.1.8.
Steiner RL, Bejleri I, Wheelock JL, Boles G, Cahill M, Perez BO: Understanding and Mapping Institutional Impediments to Walking and Bicycling to School A Case Study of Hillsborough County, Florida. Transportation Research Record. 2008, 3-11. 10.3141/2074-01.
Ward DS, Linnan L, Vaughn A, Neelon B, Martin SL, Fulton JE: Characteristics associated with US Walk to School programs. Int J Behav Nutr Phys Act. 2007, 4: 67-10.1186/1479-5868-4-67.
McDonald N, Aalborg A: Why Do Parents Take Kids to School? Implications for Safe Routes to School Programs. 2009, Transportation Research Board
Wen LM, Fry D, Rissel C, Dirkis H, Balafas A, Merom D: Factors associated with children being driven to school: implications for walk to school programs. Health Educ Res. 2008, 23: 325-334. 10.1093/her/cym043.
Pai M, McCulloch M, Gorman JD, Pai N, Enanoria W, Kennedy G, Tharyan P, Colford JM: Systematic reviews and meta-analyses: an illustrated, step-by-step guide. Natl Med J India. 2004, 17: 86-95.
Acknowledgements
We thank Dr. Derek Hales for his collaboration on the calculation of effect sizes and Dr. Richard B. Lawhon for reviewing the manuscript. Dr. Chillón was funded by a grant from the Spanish Ministry of Education (JC2009-00238). The work was done at the UNC Center for Health Promotion and Disease Prevention, a member of the Prevention Research Centers Program of the Center for Disease Control and Prevention (CDC) (#U48-DP000059) and extends previous work conducted for the National Evaluation of Walk to School (CDC, SIP 09-2002) and the North Carolina Physical Activity Policy Research Center (CDC, SIP 10-2007). The content is solely the responsibility of the authors and does not necessarily represent the official views of the CDC.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
PC, KE, AV and DW helped develop the literature search strategy, retrieved and reviewed studies, extracted data elements, and edited the manuscript. In addition, PC led the literature search strategy, compiled the studies, and developed the manuscript. All authors read and approved the final manuscript.
Electronic supplementary material
12966_2010_406_MOESM1_ESM.DOC
Additional file 1: Electronic search for the intervention studies including: database, number of references found, and terms included. The electronic search performed to identify the studies for this review is provided in detail. The terms used to search in the five different databases used (PubMed, Web of Science, Cochrane Library, SPORT Discus and the National Transportation Library) are included. Moreover, the number of final references found in each database was likewise mentioned. (DOC 34 KB)
12966_2010_406_MOESM2_ESM.DOC
Additional file 2: Adjusted criteria for the quality assessment tool for quantitative studies. This file included all the adjusted criteria performed to adapt the original tool called "Quality assessment Tool for quantitative studies from the Effective Public Health Practice Project-EPHPP-", into the identified studies in this review, since these studies were not experimental or clinical studies. Adjusted criteria were performed for selection bias, study design, confounders, blinding, data collection methods, withdrawals and drop-outs, intervention integrity, analysis and final scoring (DOC 38 KB)
12966_2010_406_MOESM3_ESM.DOC
Additional file 3: A summary of the calculation of effect size using Cohen's d. A detailed explanation of how was calculated the effect size using Cohen's d for every study identified in this review has been included. Conceptual data, numerical data and formulas are provided for every study that provided enough data to calculate effect size; moreover, studies where calculation was not possible were likewise mentioned. (DOC 66 KB)
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Chillón, P., Evenson, K.R., Vaughn, A. et al. A systematic review of interventions for promoting active transportation to school. Int J Behav Nutr Phys Act 8, 10 (2011). https://doi.org/10.1186/1479-5868-8-10
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1479-5868-8-10