
Abstract
Background
Physical inactivity is a leading risk factor for cardiovascular and other noncommunicable diseases in high-, low- and middle-income countries. Nepal, a low-income country in South Asia, is undergoing an epidemiological transition. Although the reported national prevalence of physical inactivity is relatively low, studies in urban and peri-urban localities have always shown higher prevalence. Therefore, this study aimed to measure physical activity in three domains—work, travel and leisure—in a peri-urban community and assess its variations across different sociodemographic correlates.
Methods
Adult participants (n = 640) from six randomly selected wards of the Jhaukhel-Duwakot Health Demographic Surveillance Site (JD-HDSS) near Kathmandu responded to the Global Physical Activity Questionnaire. To determine total physical activity, we calculated the metabolic equivalent of task in minutes/week for each domain and combined the results. Respondents were categorized into high, moderate or low physical activity. We also calculated the odds ratio for low physical activity in various sociodemographic variables and self-reported cardiometabolic states.
Results
The urbanizing JD-HDSS community showed a high prevalence of low physical activity (43.3%; 95% CI 39.4–47.1). Work-related activity contributed most to total physical activity. Furthermore, women and housewives and older, more educated and self-or government-employed respondents showed a greater prevalence of physical inactivity. Respondents with hypertension, diabetes or overweight/obesity reported less physical activity than individuals without those conditions. Only 5% of respondents identified physical inactivity as a cardiovascular risk factor.
Conclusions
Our findings reveal a high burden of physical inactivity in a peri-urban community of Nepal. Improving the level of physical activity involves sensitizing people to its importance through appropriate multi-sector strategies that provide encouragement across all sociodemographic groups.
Similar content being viewed by others


Introduction
With an estimated prevalence of 31%, physical inactivity is the fourth leading cause of death worldwide [1], contributing to premature death (10%), coronary artery disease (6%) and type 2 diabetes mellitus (7%) [2]. In 1953, Jeremy Morris pioneered the epidemiology of physical inactivity by comparing the mortality rate for coronary heart disease (CHD) in bus drivers versus more active bus conductors [3]. Since the American Heart Association recognized physical inactivity as a risk factor for CHD in 1992 [4], longitudinal studies have further consolidated the protective role of physical activity against cardiovascular diseases (CVDs), including CHD and hypertension [5, 6]. Consequently, public health organizations have initiated global efforts to curtail and counteract physical inactivity [7, 8].
In general, physical inactivity occurs more commonly in high-income countries than low-income countries [9]. However, physical inactivity varies greatly between different regions of the World Health Organization (WHO), ranging from 17% in Southeast Asia to 43% in the Americas [9]. A recent review showed variation between countries in the Asia-Pacific region and even between studies in the same country [10]. Most notably, the prevalence of physical inactivity in Nepal ranges from a modest 8% to a staggering 82% [10].
The Nepal data [10] show how different measurement tools can yield varying results. Currently, standard tools include the Global Physical Activity Questionnaire (GPAQ) and the International Physical Activity Questionnaire (IPAQ). Mostly used in risk factor surveillance such as the WHO Stepwise Approach to Surveillance (STEPS) surveys [11], the GPAQ emerged as a compromise between the long and short versions of the IPAQ, which underwent several metamorphoses during the late 1990s [1, 12–14]. The concept of domain in physical activity has evolved over time, shifting from an initial focus on leisure-time activity alone to its current emphasis on total physical activity (TPA), which includes leisure-time, occupational, housework and transport-related activity [9]. Further, objective measurement of physical activity with motion sensors and data comparison with questionnaire methods is increasingly a topic of interest and debate [15–18].
Apart from attempts to use standardized questionnaires to measure physical activity in different populations, recent longitudinal and cross-sectional studies have focused on determinants (i.e., variables with causal association) and correlates (i.e., variables with statistical association only), respectively [19]. Many determinants involve demographic, psychosocial, behavioral and social factors that reveal the innate complexity of physical inactivity [19]. Environmental (e.g., walkability) and policy (e.g., cycling policy) correlates influence an individual’s physical activity behavior [19, 20].
Nepal, a small agrarian republic in South Asia with 26 million inhabitants, has conducted limited research on physical activity. However, earlier studies, including the nationwide WHO STEPs survey (2007–2008), did not investigate the sociodemographic correlates of physical inactivity [21–23]. In this regard, we previously highlighted the problem of increased CVD and risk factors in Nepal [24] and elaborated the impact of urbanization on changing lifestyle, including rising body mass index and declining levels of physical activity [25]. For example, although the current percentage of overweight in Nepal is not remarkably high (7%), it is definitely increasing [24]. Only 6% of urban males have CHD [26], but the prevalence of hypertension in Nepal’s peri-urban communities has tripled, from 6% to 18%, in 25 years [27]. Likewise, dyslipidemia and diabetes mellitus have been reported in 10% and 19% of urban Nepalese adults, respectively [28, 29]. We previously suggested that health promotion might improve heart-healthy behaviors, including physical activity, and provide a starting point for CVD control in a resource-challenged country like Nepal [30].
However, when targeting various population subsets for positive behavioral changes such as physical activity, it is important to first explore how different sociodemographic factors influence activity patterns. Therefore, the current study in a peri-urban community of the Kathmandu valley aimed to conduct a detailed analysis of physical activity. We also sought to determine the relationship between physical activity and other behavioral and biological risk factors for cardiometabolic diseases and how it correlates with various sociodemographic factors.
Methods
Study site and population
We conducted the present study in the Jhaukhel-Duwakot Health Demographic Surveillance Site (JD-HDSS) [31]. Located 13 kilometers from Kathmandu in the Bhaktapur district of the Kathmandu valley, the two adjacent villages of JD-HDSS are rapidly transforming into peri-urban settlements. According to our 2010 baseline census, JD-HDSS includes 2,712 households and 13,669 inhabitants [31].
The terrain in JD-HDSS slopes from north to south. Although roadways connect the villages to the newly expanded six-lane Kathmandu-Bhaktapur highway, interior sections are connected only by narrow walking trails that increasingly are used for bicycles and motorbikes. Because cars and public vehicles are rare in JD-HDSS, young people, especially males, usually travel on motorbikes. Previously inhabited mostly by farmers, the agro-base of JD-HDSS is declining as more people shift to non-agrarian jobs. The three major ethnic groups are Brahmin, Chhetri and Newar. Common morbidities include respiratory diseases, resulting mainly from the high rate of tobacco smoking and brick factory smoke, and cardiometabolic disorders such as hypertension and diabetes mellitus [31].
Data collection
After randomly selecting three wards (i.e., administrative units) from both Duwakot and Jhaukhel, we used our 2010 census data to prepare a list of all adults aged 25–59 years in all six wards. We selected one respondent from each household and applied the Kish technique [32] when a household contained more than one eligible candidate.
Twelve trained enumerators visited households in the selected wards between September and November 2011, conducting face-to-face interviews and recording physical measurements and blood pressures. The enumerators used a Microlife BR-9201 weighing machine (Microlife AG Swiss Corporation, Widnau, Switzerland) for weight measurement and non-stretchable tapes (Jonson Tapes Ltd, New Delhi, India) to determine height, waist and hip circumference. Blood pressure was measured digitally three times at 5-minute intervals, using Microlife BP 3AP1-3E (Microlife AG Swiss Corporation, Widnau, Switzerland). The final blood pressure measurement was an average of the three readings. In accordance with cutoffs established by the Joint National Committee–VII, we defined hypertension to include individuals with a known history of hypertension and also those diagnosed with hypertension during the survey (systolic blood pressure ≥ 140 mm Hg or diastolic blood pressure ≥ 90 mm Hg) [33]. Four public health graduates supervised the enumerators and a field coordinator and PhD student oversaw all data collection.
We used GPAQ version 2 to elicit information about three domains of physical activity: work (including housework), travel to and from places and leisure time [34]. Enumerators asked respondents how many days/week and the time/day they spent doing vigorous (e.g., lifting heavy loads) and moderate (e.g., carrying light loads) activities at work. They also asked respondents if they walked or cycled continuously for at least 10 minutes during their commute to work, market, etc. Questions about leisure-time physical activity included vigorous (e.g., intense sports) and moderate activity (e.g., swimming). In accordance with the GPAQ Analysis Guide, we converted the responses to metabolic equivalent to task (MET)–minutes/week [34]. Further, we categorized respondents’ physical activity as high, moderate or low depending on their total MET–minutes/week or other combination criteria [34]. This paper presents the prevalence of low physical activity (LPA) as an indicator of insufficient physical activity. In addition, we sorted respondents according to the WHO-recommended minimum of 150 minutes of moderate or 75 minutes of vigorous aerobic physical activity throughout the week [35].
We categorized sociodemographic variables in accordance with the WHO STEPS manual [11] and the classifications of the Central Bureau of Statistics, Nepal [36]. Our definition of primary and secondary education included respondents who studied up to grades 4 (usually aged 10 years) and 10 (usually aged 16 years), respectively. We based our categorization of smoking and alcohol consumption on the WHO STEPS manual [11], defining respondents who replied “yes” to “Do you smoke?” as current smokers and smokers who replied “yes” to “Did you ever smoke in the past?” as past smokers. Current drinkers had consumed alcohol within the previous month.
Data analysis
Data entry operators recorded data in Epidata version 2.1 and we analyzed the data using SPSS version 17.0 (IBM, Armonk, New York, USA) and STATA version 10.0 (StataCorp, Texas, USA). Our results present categorical values as percentages and the continuous variable as median. We conducted correlation analysis and calculated Spearman’s correlation coefficient for continuous variables. Our results report the unadjusted and adjusted odds ratios (OR) for LPA compared to moderate-to-vigorous physical activity, a single category created by combining the moderately and vigorously active groups. ORs were calculated for the various sociodemographic and cardiovascular risk factor correlates.
Ethical considerations
Our study was approved by the Nepal Health Research Council and the Institutional Review Board of Kathmandu Medical College. After briefing respondents about the purpose of the study, enumerators requested informed consent. Respondents were free to end the survey or skip any question or section. We maintained interview confidentiality by conducting surveys either indoors or in isolation. Hard copies of the data were stored securely in the JD-HDSS office in Jhaukhel. Newly diagnosed hypertensives and respondents who needed urgent health care were referred to Kathmandu Medical College or Nepal Medical College Community Hospital, where they were entitled to subsidized service charges.
Results
Among 840 households visited in 6 randomly selected wards, 789 individuals consented to participate in the study (93.9%). Among those, we obtained complete information on demographic variables from 777 respondents. We excluded respondents for which information on height, weight or blood pressure measurements was incomplete. Thus, final analyses were based on 640 individuals.
Demographic background and risk factors status
Table 1 shows the sociodemographic composition of the study population. Females were unintentionally oversampled (72.7%) and the three major ethnic groups (i.e., Brahmin, Chhetri and Newar) were represented proportionally. One fifth of respondents smoked tobacco (males, 33%; females, 15%) or currently drank alcohol (males, 35%; females, 13%). One fifth of the respondents had high blood pressure (males, 22%; females, 21%). Female respondents had more generalized (11% vs. 5% in males) and abdominal (56% vs. 21% in males) obesity.
Domains of physical activity
We investigated physical activity level in three domains (i.e., work, travel and leisure) and combined the results to assess TPA (Table 1). Work-related activities contributed most to TPA, particularly in females, housewives, Newars, ethnic minorities and those with informal education (>90% of TPA). In general, travel and leisure-time physical activity (LTPA) contributed less to TPA. Travel-related activities were particularly less common among government employees, housewives and those involved in agricultural work. LTPA in males, Brahmins and employed individuals (governmental, nongovernmental or self-employed) accounted for around one quarter of TPA.
Burden of physical inactivity
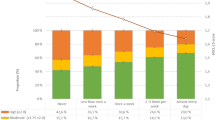
Based on the WHO guideline [35], 82.1% of males and 78.1% of females achieved the recommended weekly levels of minimal physical activity (Table 2). The proportion was highest among males working in agriculture (95.8%) and lowest among self-employed females (Table 2). However, the GPAQ classification showed that a larger proportion of our study population (i.e., 38.3% of males and 45.1% of females) had LPA. LPA was highest among ethnic minority males (71.4%) and lowest among males who had studied up to grade 4 (23.3%) (Table 2). Correspondingly, 50.8% of respondents demonstrated moderate or high physical activity (50.8% and 5.9%, respectively).
Sociodemographic correlates of physical activity
We also analyzed whether physical activity associates with sociodemographic factors such as gender, age, ethnicity, education and occupation (Table 1). Although males had higher total MET–minutes/week than females, women reported a higher rate of work-related physical activity (Table 1). Nonetheless, female respondents were 1.75 times more likely than males to have an inadequate level of physical activity as defined by the GPAQ (Table 1). LPA was greatest among the oldest age group, especially females, in all domains (adjusted OR = 1.67 [95% CI 1.08–2.58]) (Table 1). Our results show a negative correlation between age and physical activity during work, travel, leisure and TPA (Spearman’s correlation coefficient: -0.096, -0.053, -0.019 and -0.078, respectively).
Ethnic variations were evident. Newars reported more work-related activity and higher TPA, whereas Brahmins reported more physical activity during leisure time (Table 1). Ethnic minorities showed less physical inactivity. Compared with informal education, physical inactivity was three times higher in individuals educated up to high school or more (Table 1). Respondents who worked in agro-based jobs had the highest TPA (Table 1). In terms of TPA, inadequate physical activity was more likely in government employees, self-employed individuals and housewives (Table 1).
Association of physical activity with cardiovascular risk factors
Compared to individuals with no risk factors for CVD, respondents diagnosed with hypertension, diabetes mellitus or overweight/obesity showed a higher prevalence and increased odds for LPA (Table 1 and Table 2).
Discussion
Insufficient physical activity in Nepal typical of a low-income nation
The prevalence of LPA in our peri-urban study population is consistent with the findings of smaller studies in urban Nepal [22, 23] but less compared to studies in the neighboring capital city of Kathmandu (82%) [21]. However, this prevalence far exceeds the national average (5.5% [95% CI 3.4–7.7]) reported by the WHO STEPs survey using GPAQ [21] or the 8% estimated by the World Health Survey using IPAQ [37].
A comparison of Nepal to other countries clearly demonstrates worldwide variations in the prevalence of physical inactivity [2, 9]. Generally, the prevalence of physical activity associates positively with the national economy, ranging from around 5% in Bangladesh (another low-income nation) to around 15% in middle-income countries such as India and Viet Nam and greater prevalence in high-income countries such as Australia (38%), the United States of America (40%) and the United Kingdom (63%) [9, 38]. In addition, studies from other Asian HDSSs, including Vietnam (e.g., 13% in the rural Chililab HDSS and 58% in the urban Filabavi HDSS) show rural–urban disparities in physical inactivity levels [39]. Similarly, the current burden of physical inactivity in Nepal clusters around urban and urbanizing populations [40].
Contrasting physical activity in different domains
Despite rapidly declining levels of physical activity worldwide [41], emerging evidence suggests that different domains, particularly leisure time, play an important role in CHD reduction [42, 43]. Active transportation methods (e.g., cycling and walking) associate with decreased levels of all-cause mortality [9]. Further, some studies have explored the interrelationship between different domains of physical activity. For example, we found a positive correlation between occupational physical activity and LTPA, results that concur with a study in the United States [44]. However, our study did not investigate other occupation-related factors that inversely associate with leisure activity (e.g., job strain, working hours and overtime) [19].
Our finding of less physical activity during leisure time concurs with results from other urban [45] and HDSS studies in Asia [39]. In the context of traditionally urban Nepal, leisure-time activities (e.g., sports and exercise, including jogging) associate more frequently with youth or modern culture. Most Nepalese spend their leisure time watching television, socializing, gossiping or playing cards. Moreover, physical activity levels in Nepal vary seasonally and physiologically [46, 47].
Like many low-income countries, most physical activity in Nepal associates with work or occupation-related activities [19]. In contrast, high-income countries exhibit lower work-related physical activity, thus encouraging physical activities during transportation (e.g., cycling in Denmark) and leisure (e.g., Sweden, Canada, England and Spain) [9].
Sociodemographic variations in physical activity levels
In the present study, women did more household chores than men, reflecting an almost universal pattern in the traditionally patriarchal society in Nepal and other Asian countries [39, 45]. Nonetheless, our female respondents were more likely to have low overall physical activity. Male sex is a positive determinant of greater physical activity in children aged 4–9 years but not thereafter [19]. Further, risk reduction for CHD through regular physical activity is more pronounced in women than men (40% and 30%, respectively) [20]. In terms of age, the inverse relationship between age and physical activity is an almost global phenomenon, with some notable exceptions (i.e., New Zealand, Australia, China and some East Asian countries) [20, 48, 49]. Importantly, physical activity reduces cardiovascular risk even in old age [20].
In the present study, ethnic minorities showed less physical inactivity, a result that concurs with other findings [48, 50, 51] including those by studies that conducted objective measurements in children of different ethnic background [52]. Earlier studies attribute this disparity to fewer facilities for outdoor physical activity and a greater number of fast-food outlets in ethnic neighborhoods [53]. This discrepancy persists even after adjusting for possible sociodemographic variables, health-related factors and health-belief variations [54]. Further, physical activity preference differs according to ethnicity [55]. Indeed, protection against CVD through physical activity is apparent across not only gender and age but also ethnicity [20].
Studies in developed countries report that education level correlates positively with physical activity [19, 48], but our results revealed a step-wise inverse relationship. Other Asian HDSSs report similar findings [39], suggesting the probability of a contrasting trend of physical activity across the educational strata in low- and high-income countries. Our finding of highest TPA but lowest LTPA among agricultural workers concurs with findings from India [56], China [57], Finland [58] and elsewhere [19].
Lower level of physical activity in people with cardiovascular risk factors
Our respondents showed a similar prevalence of smoking, and current alcohol consumption was lower than the national average [21]. The prevalence of hypertension was similar to the national percentage [21]. Obesity was double the national average [21] and similar to that in nearby urban Kathmandu [21], hinting that the effect of urbanization is spilling from the urban area into nearby rural communities, a phenomenon already demonstrated in India [59]. In our study, the probability of inadequate physical activity was higher among individuals with diagnosed hypertension, diabetes mellitus or overweight/obesity. Due to the cross-sectional nature of our study, we cannot comment on physical inactivity as a cause or consequence of these cardiometabolic conditions. Nonetheless, earlier studies report decreased levels of physical activity following diagnosis with a chronic condition such as diabetes [60] or hypertension [61], mainly due to co-morbidities (e.g., arthritis) or social demands [62]. This phenomenon has been observed worldwide, particularly in low-income countries [63]. In addition, the relationship between overweight/obesity and physical inactivity can create a vicious cycle where in various psychosocial factors (e.g., fear of being teased or bullied, fear of negative judgments and lack of social or peer support) limit physical activity in overweight/obese people in [64].
Physical activity as an outcome of urbanization and changing lifestyle in Nepal
In our study population, high prevalence of physical inactivity reflects a side effect of development and urbanization in a low-income country like Nepal. For example, farming, which is a physically demanding occupation, decreased from 94% to 65% during the last 30 years [65]. This reduction corresponds with a similar decrease (from 60% to 33%) in agriculture’s share of GDP [65] and an escalating utilization of local land for new construction [66]. Further, although most farm equipment in Nepal is still powered by animals (41%) or humans (36%), mechanized equipment is gradually increasing (23%) [67]. Increased availability of motorized vehicles [68] and improved water supplies [69] have drastically decreased tradesmen’s demand for business-related mobility and women’s need to walk long distances for basic requirements (e.g., water). Modern technical gadgets that promote sedentary behavior frequently replace leisure activities (e.g., games and cultural rituals) [70], especially in the children and young adults.
Our results show that occupational activities comprise a major portion of total physical activity in JD-HDSS, raising concern for public health. Economic growth increases urbanization and reduces physical activity [1, 71]. Earlier trends for physical activity transition [72] in western countries [73, 74] and, more recently, in rapidly changing economies (e.g., China) [75] suggest that sedentary jobs will increase in Nepal. Lacking attempts to counteract this inevitable development by increasing physical activity in other domains (i.e., transport and leisure), overall physical activity likely will decline. Therefore, Nepal should not delay initiating interventions that improve physical activity through community-based strategies that incorporate informational, behavioral, social, policy and environmental approaches [76–78].
Lack of physical activity-friendly environment in urban Nepal
Although built environments influence physical activity [79, 80], our study did not explore this issue. Nepal’s roads are generally considered the most dangerous in the world for pedestrians [81–83], largely due to nonexistent pavement or cycling lanes, muddy and dilapidated roads, escalating traffic and congestion, negligent drivers who violate traffic rules, air pollution from dust and vehicular emissions and encroachment by street vendors. Many of these factors, including walkability [84], have a significant association with physical activity [85]. Further, Nepal’s urbanization is completely unplanned and settlements are haphazard. Parks and playgrounds, which associate positively with leisure-time physical activity in other settings [86, 87] are uncommon in urban areas of Nepal. When governments do not prioritize aesthetic appeal and green space, people are less likely to engage in physical activity, especially during commuting and leisure time [19]. Contextually, the built environment has a complex relationship with psychosocial and sociocultural aspects of physical activity [79]. To identify targets for possible interventions to increase physical activity, future research should address these areas.
Strengths and limitations of the study
Our study is the first detailed report on physical activity in an urbanizing population of Nepal. Earlier studies on the epidemiology of physical activity were conducted in high-income countries [9], but our timely study bridges this knowledge gap in a low-income setting. Similar to other HDSS studies [88], JD-HDSS provides a good platform for understanding the patterns of physical activity patterns in a peri-urban population. In addition, the longitudinal nature of an HDSS offers the advantage of systematic follow-up to examine trends and the effectiveness of interventions [89]. Moreover, our analysis demonstrates and reinforces the importance of ethnicity in cardiometabolic risk assessment [90–92]. However, our study did not explore in detail the social and environmental correlates of physical activity.
We adapted international data collection tools (including self-reported physical activity) to the local Nepali context [12, 34]. Although self-reported questionnaires provide inadequate validity compared to objectively-measured physical activity tools such as accelerometers [15, 93–95], such tools were too sophisticated, logistically impractical and expensive for successful use in our study setting. Additionally, objective tools carry their own limitations [9].
Despite the application of Kish technique during the selection of respondents at the household level, we previously reported unintentional oversampling of women [96]. We addressed this deficit by stratifying our results according to gender. Further, we excluded 137 of 777 respondents during analysis due to incomplete information regarding blood pressure or anthropometric measurements. Although including only respondents with complete information (i.e., three readings for each measurement) improved the validity of the study, the process also resulted in an 18% reduction in the study sample.
Conclusions
This study investigated different domains of physical activity among adults in a peri-urban community of Nepal and explored their associations with various socioeconomic variables. Our respondents (especially government employees, self-employed individuals and housewives) showed a high prevalence of LPA. We also investigated the changing trend of physical activity in a low-income country and the effect of urbanization (e.g., decreased energy expenditure during work and travel and technology-driven leisure-time activities). Improving the level of physical activity in Nepal will require a multi-sector approach.
Abbreviations
- CHD:
-
Coronary heart disease
- CVD:
-
Cardiovascular disease
- GPAQ:
-
Global Physical Activity Questionnaire
- IPAQ:
-
International Physical Activity Questionnaire
- JD-HDSS:
-
Jhaukhel-Duwakot Health Demographic Surveillance Site
- LPA:
-
Low physical activity
- LTPA:
-
Leisure-time physical activity
- MET:
-
Metabolic equivalent to task
- NCD:
-
Noncommunicable disease
- TPA:
-
Total physical activity
- WHO:
-
World Health Organization
- WHO STEPS:
-
WHO STEPwise approach to Surveillance.
References
Kohl HW, Craig CL, Lambert EV, Inoue S, Alkandari JR, Leetongin G, Kahlmeier S: The pandemic of physical inactivity: global action for public health. Lancet. 2012, 380: 294-305. 10.1016/S0140-6736(12)60898-8.
Lee I, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT: Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012, 380: 219-229. 10.1016/S0140-6736(12)61031-9.
Morris JN, Heady JA, Raffle PA, Roberts CG, Parks JW: Coronary heart-disease and physical activity of work. Lancet. 1953, 265 (6795): 1053-1057.
Fletcher GF, Blair SN, Blumenthal J, Caspersen C, Chaitman B, Epstein S, Falls H, Froelicher ES, Froelicher VF, Pina IL: Statement on exercise. Benefits and recommendations for physical activity programs for all Americans. A statement for health professionals by the Committee on Exercise and Cardiac Rehabilitation of the Council on Clinical Cardiology, American Heart association. Circulation. 1992, 86 (1): 340-344. 10.1161/01.CIR.86.1.340.
Physical Activity Guidelines Advisory Committee: Physical activity guidelines advisory committee report. 2008, Washington, DC: US Department of Health and Human Services
Nocon M, Hiemann T, Müller-Riemenschneider F, Thalau F, Roll S, Willich SN: Association of physical activity with all-cause and cardiovascular mortality: a systematic review and meta-analysis. Eur J Cardiovasc Prev Rehabil. 2008, 15 (3): 239-246. 10.1097/HJR.0b013e3282f55e09.
World Health Organization: Global strategy on diet, physical activity and health. 2010, Geneva, Switzerland: WHO
Beaglehole R, Bonita R, Alleyne G, Horton R, Li L, Lincoln P, Mbanya J, McKee M, Moodie R, Nishtar S: for The Lancet NCD Action Group. UN high-level meeting on non-communicable diseases: addressing four questions. Lancet. 2011, 378: 449-455. 10.1016/S0140-6736(11)60879-9.
Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U: Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012, 380: 247-257. 10.1016/S0140-6736(12)60646-1.
Macniven R, Bauman A, Abouzeid M: A review of population-based prevalence studies of physical activity in adults in the Asia-Pacific region. BMC Public Health. 2012, 12 (1): 41-10.1186/1471-2458-12-41.
World Health Organization: The WHO STEPwise approach to chronic disease risk factor surveillance (STEPS). 2009, Retrieved April 13, 2011 from http://www.who.int/chp/steps/STEPS_Instrument_v2.1.pdf
Armstrong T, Bull F: Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health. 2006, 14 (2): 66-70. 10.1007/s10389-006-0024-x.
Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P: International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003, 195: 1381-1395.
Bull F, Maslin T: Final report on reliability and validity of the Global Physical Activity Questionnaire (GPAQ v1). 2006, Geneva: World Health Organization
Ainsworth BE: How do I measure physical activity in my patients? Questionnaires and objective methods. Br J Sports Med. 2009, 43 (1): 6-9.
Shephard R: Limits to the measurement of habitual physical activity by questionnaires. Br J Sports Med. 2003, 37 (3): 197-206.
Milton K, Bull F, Bauman A: Reliability and validity testing of a single-item physical activity measure. Br J Sports Med. 2011, 45 (3): 203-208. 10.1136/bjsm.2009.068395.
Wareham N, Jakes R, Rennie K, Schuit J, Mitchell J, Hennings S, Day N: Validity and repeatability of a simple index derived from the short physical activity questionnaire used in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Public Health Nutr. 2003, 6 (4): 407-414.
Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW: Correlates of physical activity: why are some people physically active and others not?. Lancet. 2012, 380: 258-271. 10.1016/S0140-6736(12)60735-1.
Shiroma EJ, Lee I: Physical Activity and Cardiovascular Health Lessons Learned From Epidemiological Studies Across Age, Gender, and Race/Ethnicity. Circulation. 2010, 122 (7): 743-752. 10.1161/CIRCULATIONAHA.109.914721.
Ministry of Health and Population Nepal: Nepal non-communicable diseases risk factor ssurvey 2007. 2008, Kathmandu: Ministry of Health and Population
Vaidya A, Pokharel PK, Nagesh S, Karki P, Kumar S, Majhi S: Association of obesity and physical activity in adult males of Dharan Nepal. Kathmandu Univ Med J. 2006, 4 (2): 192-197.
Sharma SK, Ghimire A, Radhakrishnan J, Thapa L, Shrestha NR, Paudel N, Gurung K, Budathoki A, Baral N, Brodie D: Prevalence of hypertension, obesity, diabetes, and metabolic syndrome in Nepal. Int J Hypertens. 2011, doi:10.4061/2011/821971
Vaidya A: Tackling cardiovascular health and disease in Nepal: epidemiology, strategies and implementation. Heart Asia. 2011, 3 (1): 87-91.
Vaidya A, Shakya S, Krettek A: Obesity prevalence in Nepal: public health challenges in a low-income nation during an alarming worldwide trend. Int J Environ Res Publ Health. 2010, 7 (6): 2726-2744. 10.3390/ijerph7062726.
Vaidya A, Pokharel PK, Nagesh S, Karki P, Kumar S, Majhi S: Prevalence of coronary heart disease in the urban adult males of eastern Nepal: A population-based analytical cross-sectional study. Indian Heart J. 2009, 61: 341-347.
Vaidya A, Pathak RP, Pandey MR: Prevalence of hypertension in Nepalese community triples in 25 years: a repeat cross-sectional study in rural Kathmandu. Indian Heart J. 2012, 64 (2): 128-131. 10.1016/S0019-4832(12)60045-5.
Shrestha U, Singh D, Bhattarai M: The prevalence of hypertension and diabetes defined by fasting and 2-h plasma glucose criteria in urban Nepal. Diabetic Med. 2006, 23 (10): 1130-1135. 10.1111/j.1464-5491.2006.01953.x.
Limbu Y, Rai S, Ono K, Kurokawa M, Yanagida J, Rai G, Gurung N, Rai C: Lipid profile of adult Nepalese population. Nepal Med Coll J. 2008, 10 (1): 4-7.
Vaidya A, Krettek A: Is Health Promotion the Starting Point of Primary Cardiovascular Care in Low-and Middle-Income Countries Like Nepal?. Health Promot Pract. 2012, 13 (3): 412-415. 10.1177/1524839911423273.
Aryal UR, Vaidya A, Shakya-Vaidya S, Petzold M, Krettek A, Sinamangal N: Establishing a health demographic surveillance site in Bhaktapur district, Nepal: initial experiences and findings. BMC Res Notes. 2012, 5 (1): 489-10.1186/1756-0500-5-489.
Kish L: Sampling Organizations and Groups of Unequal Sizes. Am Sociol Rev. 1965, 30: 564-572. 10.2307/2091346.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT: Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003, 42 (6): 1206-1252. 10.1161/01.HYP.0000107251.49515.c2.
World Health Organization: Global Physical Activity Questionnaire (GPAQ) Analysis Guide. 2012, Geneva, Switzerland: WHO
World Health Organization: Global recommendations on physical activity for health. 2010, Geneva, Switzerland: WHO
Central Bureau of Statistics: National Population and Housing Census 2011. 2012, Kathmandu: National Planning Commission Secretariat
Guthold R, Ono T, Strong KL, Chatterji S, Morabia A: Worldwide variability in physical inactivity: a 51-country survey. Am J Prev Med. 2008, 34 (6): 486-494. 10.1016/j.amepre.2008.02.013.
World Health Organization: Global Health Observatory Data Repository. 2012, Retrieved December 13, 2013 from https://apps.who.int/infobase/Indicators.aspx
Ng N, Hakimi M, Van Minh H, Juvekar S, Razzaque A, Ashraf A, Ahmed SM, Kanungsukkasem U, Soonthornthada K, Bich TH: Prevalence of physical inactivity in nine rural INDEPTH Health and Demographic Surveillance Systems in five Asian countries. Global Health Action. 2009, 2: 44-53.
van de Vijver S, Oti S, Addo J, de Graft-Aikins A, Agyemang C: Review of community-based interventions for prevention of cardiovascular diseases in low-and middle-income countries. Ethn Health. 2012, 17 (6): 651-676. 10.1080/13557858.2012.754409.
Ng SW, Popkin B: Time use and physical activity: a shift away from movement across the globe. Obesity Reviews. 2012, 13 (8): 659-680. 10.1111/j.1467-789X.2011.00982.x.
Sofi F, Capalbo A, Cesari F, Abbate R, Gensini GF: Physical activity during leisure time and primary prevention of coronary heart disease: an updated meta-analysis of cohort studies. Eur J Cardiovasc Prev Rehabil. 2008, 15 (3): 247-257. 10.1097/HJR.0b013e3282f232ac.
Held C, Iqbal R, Lear SA, Rosengren A, Islam S, Mathew J, Yusuf S: Physical activity levels, ownership of goods promoting sedentary behaviour and risk of myocardial infarction: results of the INTERHEART study. Eur Heart J. 2012, 33 (4): 452-466. 10.1093/eurheartj/ehr432.
Wolin KY, Bennett GG: Interrelations of socioeconomic position and occupational and leisure-time physical activity in the National Health and Nutrition Examination Survey. J Phys Act health. 2008, 5 (2): 229.
Nang EEK, Khoo EY, Salim A, Tai ES, Lee J, Van Dam RM: Patterns of physical activity in different domains and implications for intervention in a multi-ethnic Asian population: a cross-sectional study. BMC Public Health. 2010, 10 (1): 644-10.1186/1471-2458-10-644.
Panter-Brick C, Lotstein DS, Ellison PT: Seasonality of reproductive function and weight loss in rural Nepali women. Hum Reprod. 1993, 8 (5): 684-690.
Panter-Brick C: The energy cost of common tasks in rural Nepal: levels of energy expenditure compatible with sustained physical activity. Eur J Appl Physiol Occup Physiol. 1992, 64 (5): 477-484. 10.1007/BF00625071.
Crespo CJ, Smit E, Andersen RE, Carter-Pokras O, Ainsworth BE: Race/ethnicity, social class and their relation to physical inactivity during leisure time: results from the Third National Health and Nutrition Examination Survey, 1988–1994. Am J Prev Med. 2000, 18: 46-53. 10.1016/S0749-3797(99)00105-1.
Bauman A, Bull F, Chey T, Craig CL, Ainsworth BE, Sallis JF, Bowles HR, Hagstromer M, Sjostrom M, Pratt M: The International Prevalence Study on Physical Activity: results from 20 countries. Int J Behav Nutr Phys Act. 2009, 6: 21-10.1186/1479-5868-6-21.
Bryan SN, Tremblay MS, Pérez CE, Ardern CI, Katzmarzyk PT: Physical activity and ethnicity: evidence from the Canadian Community Health Survey. Can J Public Health. 2006, 97 (4): 271-276.
Higgins V, Dale A: Ethnic differences in physical activity and obesity. Understanding Population Trends and Processes, Volume 3: Ethnicity and Integration. Edited by: Stillwell J, Finney N, van Ham M. 2010, Dordrecht, Netherlands: Springer
Eyre ELJ, Duncan MJ: The Impact of Ethnicity on Objectively Measured Physical Activity in Children. ISRN Obesity. 2013, doi:10.1155/2013/757431
Molaodi OR, Leyland AH, Ellaway A, Kearns A, Harding S: Neighbourhood food and physical activity environments in England, UK: does ethnic density matter?. Int J Behav Nutr Phys Act. 2012, 9 (1): 75-10.1186/1479-5868-9-75.
Mathieu RA, Powell-Wiley TM, Ayers CR, McGuire DK, Khera A, Das SR, Lakoski SG: Physical activity participation, health perceptions, and cardiovascular disease mortality in a multiethnic population: The Dallas Heart Study. Am Heart J. 2012, 163 (6): 1037-1040. 10.1016/j.ahj.2012.03.005.
Dogra S, Meisner BA, Ardern CI: Variation in mode of physical activity by ethnicity and time since immigration: a cross-sectional analysis. Int J Behav Nutr Phys Act. 2010, 7 (1): 75-10.1186/1479-5868-7-75.
Gupta R, Deedwania PC, Sharma K, Gupta A, Guptha S, Achari V, Asirvatham AJ, Bhansali A, Gupta B, Gupta S: Association of Educational, Occupational and Socioeconomic Status with Cardiovascular Risk Factors in Asian Indians: A Cross-Sectional Study. PLoS One. 2012, 7 (8): e44098-10.1371/journal.pone.0044098.
Ding D, Sallis JF, Hovell MF, Du J, Zheng M, He H, Owen N: Physical activity and sedentary behaviours among rural adults in suixi, china: a cross-sectional study. Int J Behav Nutr Phys Act. 2011, 8 (1): 37-10.1186/1479-5868-8-37.
Seiluri T, Lahti J, Rahkonen O, Lahelma E, Lallukka T: Changes in occupational class differences in leisure-time physical activity: a follow-up study. Int J Behav Nutr Phys Act. 2011, 8: 14-10.1186/1479-5868-8-14.
Sullivan R, Kinra S, Ekelund U, Bharathi A, Vaz M, Kurpad A, Collier T, Reddy KS, Prabhakaran D, Ben-Shlomo Y: Socio-demographic patterning of physical activity across migrant groups in India: results from the Indian migration study. PloS One. 2011, 6 (10): e24898-10.1371/journal.pone.0024898.
Thomas N, Alder E, Leese G: Barriers to physical activity in patients with diabetes. Postgrad Med J. 2004, 80 (943): 287-291. 10.1136/pgmj.2003.010553.
Steptoe A, McMunn A: Health behaviour patterns in relation to hypertension: the English Longitudinal Study of Ageing. J Hypertens. 2009, 27 (2): 224-230. 10.1097/HJH.0b013e3283193e6e.
Penn L, Moffatt SM, White M: Participants' perspective on maintaining behaviour change: a qualitative study within the European Diabetes Prevention Study. BMC Public Health. 2008, 8 (1): 235-10.1186/1471-2458-8-235.
Teo K, Lear S, Islam S, Mony P, Dehghan M, Li W, Rosengren A, Lopez-Jaramillo P, Diaz R, Oliveira G: Prevalence of a Healthy Lifestyle Among Individuals With Cardiovascular Disease in High-, Middle-and Low-Income Countries: The Prospective Urban Rural Epidemiology (PURE) Study Healthy Lifestyle and Cardiovascular Disease. JAMA. 2013, 309 (15): 1613-1621. 10.1001/jama.2013.3519.
Stankov I, Olds T, Cargo M: Overweight and obese adolescents: what turns them off physical activity?. Int J Behav Nutr Phys Act. 2012, 9 (1): 53-10.1186/1479-5868-9-53.
International Labour Organization: Labour and Social Trends in Nepal 2010. 2010, Geneva, Switzerland: ILO
ktm2day: Rapid urbanization takes its toll on valley land. Retrieved December 13, 2013 from http://www.ktm2day.com/2011/06/09/rapid-urbanization-takes-its-toll-on-valley-land/
Shrestha S: Status of Agricultural Mechanization in Nepal. 2012, New Delhi: United Nations Asian and Pacific Center for Agricultural Engineering and Machinery (UNAPCAEM)
Sharma KK: Status Paper on Road Safety in Nepal: The fourth meeting of the Working Group on the Asian Highway and Expert Group Meeting on Progress on Road Safety Improvement in Asia and the Pacific, 27–29 September 2011. 2011, Bangkok, Thailand: United Nations Economic and Social Commission for Asia and Pacific
Department of Water Supply and Sewerage: History of piped water supply system development in Nepal. 2013, Retrieved December 13, 2013 from http://www.dwss.gov.np/
Rana J: Bhaktapur, Nepal's Capital of Music and Dance. Kailash. 1990, 16 (1–2): 5-14.
Bosdriesz JR, Witvliet MI, Visscher TL, Kunst AE: The influence of the macro-environment on physical activity: a multilevel analysis of 38 countries worldwide. Int J Behav Nutr Phys Act. 2012, 9: 110-10.1186/1479-5868-9-110.
Katzmarzyk PT, Mason C: The physical activity transition. J Phys Act Health. 2009, 6 (3): 269-280.
Norman A, Bellocco R, Vaida F, Wolk A: Age and temporal trends of total physical activity in Swedish men. Med Sci Sports Exerc. 2003, 35 (4): 617-622. 10.1249/01.MSS.0000058357.23080.F4.
Orsini N, Bellocco R, Bottai M, Pagano M, Wolk A: Age and temporal trends of total physical activity among Swedish women. Med Sci Sports Exerc. 2006, 38 (2): 240-245. 10.1249/01.mss.0000185086.19220.b3.
Monda KL, Gordon-Larsen P, Stevens J, Popkin BM: China's transition: the effect of rapid urbanization on adult occupational physical activity. Soc Sci Med. 2007, 64 (4): 858-870. 10.1016/j.socscimed.2006.10.019.
Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, Montes F, Brownson RC: Evidence-based intervention in physical activity: lessons from around the world. The Lancet. 2012, 380: 272-281. 10.1016/S0140-6736(12)60816-2.
Lachat C, Otchere S, Roberfroid D, Abdulai A, Seret FMA, Milesevic J, Xuereb G, Candeias V, Kolsteren P: Diet and physical activity for the prevention of noncommunicable diseases in low-and middle-income countries: a systematic policy review. PLoS Med. 2013, 10 (6): e1001465-10.1371/journal.pmed.1001465.
Global Advocacy for Physical Activity (GAPA) the Advocacy Council of the International Society for Physical Activity and Health (ISPAH): NCD Prevention: Investments that Work for Physical Activity. Br J Sports Med. 2012, 46: 709-712.
Humphrey NP: Does the Built Environment Influence Physical Activity?. TR News. 2005, 237: 32.
Sallis JF, Floyd MF, Rodriguez DA, Saelens BE: Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation. 2012, 125 (5): 729-737. 10.1161/CIRCULATIONAHA.110.969022.
Poudel-Tandukar K, Nakahara S, Ichikawa M, Poudel KC, Jimba M: Risk perception, road behavior, and pedestrian injury among adolescent students in Kathmandu, Nepal. Inj Prev. 2007, 13 (4): 258-263. 10.1136/ip.2006.014662.
Ministry of Physical Planning, Works & Transport Management: Nepal Road Safety Action Plan (2013–2020). 2013, Kathmandu: Ministry of Physical Planning, Works & Transport Management
Sharma KK: Country Status Paper on Road Safety in Nepal. Retrieved on April 13, 2013 from http://www.unescap.org/ttdw/roadsafety/Reports2007/Nepal_RSpaper.pdf
Lovasi GS, Grady S, Rundle A: Steps forward: review and recommendations for research on walkability, physical activity and cardiovascular health. Public Health Rev. 2012, 33 (2): 484-506.
Van Holle V, Deforche B, Van Cauwenberg J, Goubert L, Maes L, Van de Weghe N, De Bourdeaudhuij I: Relationship between the physical environment and different domains of physical activity in European adults: a systematic review. BMC Public Health. 2012, 12 (1): 807-10.1186/1471-2458-12-807.
Inoue S, Ohya Y, Odagiri Y, Takamiya T, Ishii K, Kitabayashi M, Suijo K, Sallis JF, Shimomitsu T: Association between perceived neighborhood environment and walking among adults in 4 cities in Japan. J Epidemiol. 2010, 20 (4): 277-286. 10.2188/jea.JE20090120.
Sallis JF, Bowles HR, Bauman A, Ainsworth BE, Bull FC, Craig CL, Sjöström M, De Bourdeaudhuij I, Lefevre J, Matsudo V: Neighborhood environments and physical activity among adults in 11 countries. Am J Prev Med. 2009, 36 (6): 484-490. 10.1016/j.amepre.2009.01.031.
Bloomfield GS, Mwangi A, Chege P, Simiyu CJ, Aswa DF, Odhiambo D, Obala AA, Ayuo P, Khwa-Otsyula BO: Multiple cardiovascular risk factors in Kenya: evidence from a health and demographic surveillance system using the WHO STEPwise approach to chronic disease risk factor surveillance. Heart. 2013, 99 (18): 1323-1329. 10.1136/heartjnl-2013-303913.
Ng N, Van Minh H, Juvekar S, Razzaque A, Bich TH, Kanungsukkasem U, Ashraf A, Ahmed SM, Soonthornthada K: Using the INDEPTH HDSS to build capacity for chronic non-communicable disease risk factor surveillance in low and middle-income countries. Global Health Action. 2009, 2: doi:10.3402/gha.v2i0.1984
Anand SS: Using ethnicity as a classification variable in health research: perpetuating the myth of biological determinism, serving socio-political agendas, or making valuable contributions to medical sciences?. Ethn Health. 1999, 4 (4): 241-244. 10.1080/13557859998029.
Wells J: Ethnic variability in adiposity, thrifty phenotypes and cardiometabolic risk: addressing the full range of ethnicity, including those of mixed ethnicity. Obes Rev. 2012, 13 (S2): 14-29.
Zaman MJ, Bhopal RS: New answers to three questions on the epidemic of coronary mortality in south Asians: incidence or case fatality? Biology or environment? Will the next generation be affected?. Heart. 2013, 99 (3): 154-158. 10.1136/heartjnl-2012-302364.
Miranda A, Benjamin C, Gillian R, Valerie B: Reported frequency of physical activity in a large epidemiological study: relationship to specific activities and repeatability over time. BMC Med Res Methodol. 2011, 11: 97-10.1186/1471-2288-11-97.
Ford ES, Caspersen CJ: Sedentary behaviour and cardiovascular disease: a review of prospective studies. Int J Epidemiol. 2012, 41 (5): 1338-1353. 10.1093/ije/dys078.
Sternfeld B, Goldman-Rosas L: A systematic approach to selecting an appropriate measure of self-reported physical activity or sedentary behavior. J Phys Act health. 2012, 9: S19-S28.
Vaidya A, Aryal UR, Krettek A: Cardiovascular health knowledge, attitude and practice/behaviour in an urbanising community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot Health Demographic Surveillance Site. BMJ Open. 2013, 3 (10): e002976.
Acknowledgments
This study was supported by grants from the Wilhelm & Martina Lundgren’s Foundation (vet1- 367/2011 and vet1-379/2012) and the University of Gothenburg, Sweden through a “Global University” grant (A 11 0524/09). We are grateful to the study respondents for their valuable participation in the study. We acknowledge all enumerators. We thank the field coordinator, Prof. Dr. Muni Raj Chhetri, and field supervisors Chandra Shova Khaitu, Rachana Shrestha, Shova Poudel and Vishal Bhandari. We are grateful for Assistant Prof. Umesh Raj Aryal’s suggestions during statistical analysis. We thank scientific editor Karen Williams (Kwills Editing Services, Weymouth, MA, USA) for providing professional English-language editing of this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AV designed the study, performed statistical analysis, and drafted the manuscript. AK helped design the study and provided critical revision of the manuscript. Both authors have read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited.
About this article
Cite this article
Vaidya, A., Krettek, A. Physical activity level and its sociodemographic correlates in a peri-urban Nepalese population: a cross-sectional study from the Jhaukhel-Duwakot health demographic surveillance site. Int J Behav Nutr Phys Act 11, 39 (2014). https://doi.org/10.1186/1479-5868-11-39
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1479-5868-11-39