
Abstract
Objective
Walking groups are increasingly being set up but little is known about their efficacy in promoting physical activity. The present study aims to assess the efficacy of interventions to promote walking in groups to promoting physical activity within adults, and to explore potential moderators of this efficacy.
Method
Systematic literature review searches were conducted using multiple databases. A random effect model was used for the meta-analysis, with sensitivity analysis.
Results
The effect of the interventions (19 studies, 4 572 participants) on physical activity was of medium size (d = 0.52), statistically significant (95%CI 0.32 to 0.71, p < 0.0001), and with large fail-safe of N = 753. Moderator analyses showed that lower quality studies had larger effect sizes than higher quality studies, studies reporting outcomes over six months had larger effect sizes than studies reporting outcomes up to six months, studies that targeted both genders had higher effect sizes than studies that targeted only women, studies that targeted older adults had larger effect sizes than studies that targeted younger adults. No significant differences were found between studies delivered by professionals and those delivered by lay people.
Conclusion
Interventions to promote walking in groups are efficacious at increasing physical activity. Despite low homogeneity of results, and limitations (e.g. small number of studies using objective measures of physical activity, publication bias), which might have influence the findings, the large fail-safe N suggests these findings are robust. Possible explanations for heterogeneity between studies are discussed, and the need for more investigation of this is highlighted.
Similar content being viewed by others

Background
The health benefits of physical activity are well documented [1, 2]. Governmental recommendations suggest that adults and older adults should participate in at least 150 minutes of moderate or vigorous activity per week, in order to promote and maintain health [3, 4]. However, most adults do not currently achieve this [5, 6]. Thus, promoting physical activity as an integral part of lifestyle has become a central aim of public health policy [3, 4].
Moderate intensity physical activity includes walking, which is a popular, accessible and acceptable form of activity particularly among populations who are the most physically inactive [7]. Walking also does not require special equipment and has low risk of injuries. Further, a meta-analysis of relevant research found that increased walking led to increased fitness, decreased body weight, Body Mass Index, percentage body fat and resting diastolic blood pressure in previously sedentary adults [8].
Group walking has become an increasingly popular form of promoting physical activity in many countries, especially among sedentary people and people with chronic diseases. For example, Walking for Health (WfH) is an initiative, which has established group walks across England with the aim to encourage more people to be physically active. During 2011 they ran 522 walk schemes across England with more than 57 585 walkers [9]. Likewise, the American Volkssport Association reports more than 300 walking clubs in the United States [10].
Several systematic literature reviews have described the efficacy of interventions to promote physical activity in different populations [11]. Despite this, no review exists on the efficacy of interventions to promote walking in groups in promoting physical activity. Currently, the best source of evidence on the efficacy of walking interventions is the 2007 systematic review by Ogilvie and colleagues [12]. This review included interventions to promote walking in groups under the umbrella of either group based walking interventions (as led walks) or community interventions (as formation of walking groups). However, in this review there is no distinct category of interventions to promote walking in groups. For example under group based interventions there are not only interventions where the behaviour is implemented in groups [13] but also interventions delivered to groups, as education sessions, but where the walking is not enacted in groups [14]. In the present review we focus solely on interventions to promote walking in groups, which are interventions where participants walk collectively in organised walking groups and thereby provide support relationships for behaviour change.
Given that previous research does not provide clear evidence of the efficacy of walking in groups interventions, the aim of the present study was to systematically appraise the efficacy of these interventions to promote physical activity for adults. Sensitivity analysis explored whether the quality of studies affected estimates of effect size. Secondary aims were to assess whether the efficacy of these interventions varied according to duration of follow-up measurements, participants’ gender, participants’ age and the person delivering the intervention.
Methods
Eligibility criteria
Randomized Control Trials (RCTs), non Randomized Control Trials (non-RCTs) and pre-post studies were included. Only studies with objective or self-reported measures of physical activity were eligible for inclusion. The outcome was assessed in terms of the frequency, duration or distance of physical activity performed. Studies with adults over 18 years old were included in the review. Only studies reported in English were eligible, due to lack of resources available for translation.
The following types of studies were included: (a) interventions in which people walk collectively in groups. In these studies walking in group might be the only component of the behavior change interventions or might be one component of wider behavior change intervention, (b) interventions where participants walk with or without leaders’ physical presence, and (c) interventions where people are allowed to choose a partner to walk with (i.e. group is defined as two people or more).
Studies were excluded for the following reasons: (a) interventions to promote walking in groups where the dependent variable measured was not physical activity behaviour, but the outcomes of the behaviour, such as heart rate, energy loss, exercise intensity, endurance and functional capacity, tolerance, energy loss, balance [15–17], (b) interventions which included walking groups as one component of a wider physical activity intervention but measured the total level of physical activity, not only effects of walking in groups [18–20], (c) interventions when group walking is taking place in a laboratory using physical activity equipment such as corridors, treadmill or mat walking [21], (d) interventions when people have a collective goal but walk individually/independently from each other [22], (e) interventions to promote walking in groups when compared the outcomes of one walking group with another walking group and not with a control group or did not have baseline measures for each of the intervention groups [23, 24], (f) studies when participants walk accompanied by the researcher but not with other participants, (g) group based walking interventions when participants did not enact walking behavior collectively [25, 26], (h) studies where participants exercise in groups or complete specified levels of other type of physical activities in groups in order to provide social support to each other but they do not walk in groups [27].
Information sources
Studies were identified through searches in the following electronic databases: Academic search complete, PsycINFO, Medline, CINAHL with full text, AMED, SportDiscus and Scopus (from January 1980 to March 2012).
Search
Search terms varied depending upon the database being searched, but in all cases the following terms were used: walking in groups, group walking, led walk, walking club, club walking, group physical activity, group exercise, interventions, pedometer interventions, and program (see Additional file 1).
All potentially relevant articles were screened by abstract and where appropriate articles were retrieved in full text for detailed examination. References from review articles [11, 12, 28–30] on walking and physical activity interventions were screened for relevant studies. Forward and backward citation searches of included papers were made. Authors of studies that satisfied the inclusion criteria were contacted by email asking for unpublished study data in order to identify grey literature. The first author performed the search and the selection of the studies.
Data extraction process
The first author and a second researcher extracteda the data independently, in a standardized manner using a coding frame (coding frame is provided in Additional file 2). Any discrepancies were resolved by discussion. Good agreement between coders was achieved (between κ = 0.84 and κ = 0.98).
Synthesis of results
The effect size used was the Standardized Mean Difference also known as Cohen’s d [31]. When physical activity was measured on more than two occasions, baseline and the last follow up measurement were extracted. Means and pooled standard deviation were used to calculate effect sizes. Data were analyzed using the meta-analysis program of Schwarzer [32]. A random effect model was used. Heterogeneity was assessed using Q coefficients, which assess between-studies variabilities. The Q test is computed by summing the squared deviations of each study’s effect estimate from the overall effect estimate, weighting the contribution of each study by its inverse variance [33]. Fail-safe N was calculated to explore the extent to which the “file drawer problem” may have affected study results [34]. The Fail-safe N specifies the number of hypothetical studies showing a zero effect that required to be included in the meta-analysis for the relationship between independent and dependent variables to become statistically non significant.
An assessment of the quality of the included studies was made using the guide by the Cochrane Consumers and Communication Review Group [35], to explore whether poor quality studies biased the results. Studies, which satisfied a quality criterion were awarded a point “yes”. If the criterion was not satisfied or details on the process followed to satisfy the criterion were not provided, then no points were given (more details is provided in Additional file 3). Studies scoring at least 4 points (i.e. “yes” on at least half the criteria) were classified as higher quality and studies scoring 0–3 points as lower quality. Quality criteria and assessment can be found in Table 1.
Sensitivity analysis and moderator analyses were performed by breaking down the data into two subsets with respect to a theoretically relevant variable. In order to classify as a moderator, the following requirements had to be met: (a) the effect size varies from subset to subset, and (b) the residual variance averages lower in the subsets than for the data as a whole [54]. Pair wise z tests were used to assess whether there was any statistically significant differences in effect size estimates for interventions that:
measure outcomes up to six months post baseline (0–6 months) vs measured outcome over six months after baseline (>6 months). When interventions had different measurements at baseline and follow up, only the follow up measurements were used for this analysis.
differ on participants’ gender. Originally we intended to compare whether there is any difference between women’s groups and men’s groups but the lack of interventions that targeted only men led us to change the moderator analysis. Instead, all studies were categorised into two groups, those that targeted only women and those that targeted both genders.
differ on participants’ age. Studies were categorised into two groups, younger adults (≤60 years old) and older adults (>61 years old).
were delivered by a lay person or by the research or other professionals.
Results
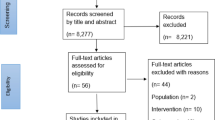
The systematic electronic search retrieved 2 946 unique papers. Based on examination of these papers, 151 papers describing 115 unique studies were retrieved in full text for detailed examination. Further searches and screening against inclusion criteria concluded in 19 studies (presented in 33 papers), which were included for quality appraisals and analysis in this review (see flow diagram in Figure 1).

Flow chart of searches conducted and study selection.
Nine of these 19 studies included were RCTs [13, 36, 37, 39–41, 51–53], six studies were non-RCTs [38, 45–47, 49, 50] and four had pre-post designs [42–44, 48]. Seventeen studies were community based [13, 36–38, 40, 42–53] and two were hospital-based [39, 41]. From the seventeen community-based studies, one study was in care retirementcommunity [40], one was in a centre for older people [53], one was based in a church [45], three were neighborhood based [13, 44, 47] and the rest eleven [36–38, 42, 43, 46, 48–52] were based in the general community. Based on available data, the overall mean age of participants was 59.8 years (ranged from 44 to 88).
Eleven studies were walking in groups only interventions [13, 36, 37, 42, 44, 47, 49–53], four studies involved walking in groups and other types of PA [38, 45, 46, 48], and four studies contained walking in groups and supportive patient education program on chronic diseases (e.g. self-management) or other lifestyle behaviors [39–41, 43]. Thirteen studies were conducted in US [13, 36–40, 43–46, 48, 49, 51], one in UK [41], one in Canada [42], one in Australia [47], two in Japan [50, 52] and one in China [53] (more details are given in Table 2).
Meta-analysis
A meta-analysis of the included studies indicated that interventions to promote walking in groups are efficacious at increasing physical activity (overall d = 0.52, 95%CI 0.32 to 0.71, N = 4752, k = 19, p < 0.0001). A forest plot showing physical activity effect sizes with 95% CI for each study ordered by quality assessment, is given in Figure 2. Fail-safe N was large: it would require that there would have to be an additional 753 studies showing a zero effect not included in the present study for the relationship between interventions and physical activity to become statistically non significant [34].

Forest plot showing changes in moderate physical activity for each study ordered by quality, as well as overall effect size (Cohen’s d) and 95% Confidence Intervals (CI).
Sensitivity analysis
Only one study [i.e. 53] of the 19 studies satisfied all of the quality criteria. There were twelve higher quality studies and seven lower quality studies (see Table 1). Overall, lower quality studies produced larger effect sizes (d = 0.59, 95%CI 0.28 to 0.91, n = 1610, k = 7, p < 0.0001) than higher quality studies (d = 0.49, 95%CI 0.24 to 0.75, n = 2962, k = 12, p < 0.0001) and that difference was statistical significant (z = 1.55, N = 4572, p = 0.05).
Moderator analyses
The homogeneity of the studies was low (amount of variance explained by sampling error: 23.21%), indicating that other factors were causing substantial variation in effect sizes between studies. A summary of characteristics of included studies with theoretically relevant variables for conducting moderator analyses is provided in Table 2.
Outcome measures from baseline to six months vs over six months
Thirteen studies reported outcomes from baseline to 6 months and six studies reported outcomes over 6 months (see Table 2). Studies reporting short-term outcomes had overall smaller effect size (d = 0.45, 95%CI 0.25 to 0.65, n = 2992, k = 13, p < 0.0001) than studies reporting long-term outcomes (d = 0.66, 95%CI 0.22 to 1.10, n = 1580, k = 6, p < 0.001) and that difference was statistically significant (z = 3.32, N = 4572, p = 0.0004).
Only women vs both genders
They were six studies that targeted only women and the remaining thirteen targeted both genders (see Table 2). Interventions that targeted only women were found to have smaller effect size (d = 0.18, 95%CI from 0.03 to 0.33, n = 702, k = 6, p < 0.01) than interventions that targeted both genders (d = 0.61, 95%CI from 0.35 to 0.88, n = 3870, k = 13, p < 0.0001) and that difference was statistically significant (z = 5.12, N = 4572, p < 0.0001).
Younger adults vs older adults
They were 12 studies targeted adults up to 60 years and seven studies that targeted older adults (see Table 2). Interventions which target adults from 18 to 59 years old had smaller effect sizes (d = 0.48, 95%CI from 0.27 to 0.69, n = 2548, k = 12, p < 0.0001) than interventions that target older adults (d = 0.57 95%CI from 0.17 to 0.98, n = 2024, k = 7, p < 0.005), and that difference was statistically significant (z = 1.55, N = 4752, p = 0.05).
Delivered by lay people vs by professionals
There were eight studies where groups were led by lay people, who had received at least a basic training to become walk leaders. In three studies the researcher delivered an intervention, but did not accompany walkers while group walking. In seven studies groups were led by professionals (e.g. trained staff), and in one study was not clear who supervised the walking group (see Table 2). Interventions delivered by a lay person had a similar effect size (d = 0.52, 95%CI from 0.25 to 0.79, n = 2843, k = 8, p < 0.0001) to interventions delivered by professionals (d = 0.51, 95%CI from 0.23 to 0.79, n = 1729, k = 11, p < 0.0001). The difference in effect size estimates was not statistically significant (z = 0.158, N = 4572, p = 0.43).
Discussion
Summary of evidence
The meta-analysis of 19 studies with 4 572 participants showed that interventions to promote walking in groups are efficacious at increasing physical activity. The overall effect was of medium size (d = 0.52, p < 0.001) when all eligible studies were examined and slightly lower when only higher quality studies were included (d = 0.49, p < 0.001). Thus, the overall effect size found in this analysis might be an overestimate due to the inclusion of lower quality studies. Despite this, the overall effect size of the twelve higher quality studies was still highly statistically significant, which gives us more confidence that this finding is not a spurious finding due to poor quality studies.
Strengths and limitations
A limitation of this systematic review was that several potentially eligible studies were identified, but no effect sizes could be calculated due to missing information. Even though authors of these studies were contacted, the necessary information was not provided by several authors. Thus, the true overall effect of the interventions to promote walking in groups might be slightly different from that estimated by the present study. However, there is every reason to believe that the overall effects would still be positive even if the results of these studies could have been included, as all studies from which we could not yield effect size estimates for this review reported positive changes in physical activity. Further, the large fail-safe N of 753 studies indicates that the finding of this meta-analysis is robust.
A related limitation might be that the searching of databases and selection of the studies was performed only by the first author due to resource limitations. This could have introduced bias into the selection of studies. However the large fail-safe N indicates that there would need to have been a substantial systematic bias in the selection of studies for the finding of positive effects of walking groups to be inaccurate.
Only studies reported in English language are reported, which limits the generalizability of the results of this review. Another issue was the limited generalizability of the study population. This was because the majority of the participants were white middle age women. No comparisons based on participants’ ethnicity or other possible confounders were performed, due to limited information provided in the primary studies. This limits our ability to draw conclusions about the effects of other characteristics of the study population on the outcome. We should therefore treat this evidence cautiously when translated in practice to different demographic groups.
This review is also limited by the heterogeneity of the studies included. In this review we conducted only a small number of moderator analyses, based on questions derived from the relevant literature. It seems likely that other factors which have not been explored in this review may account for the variance unexplained by these moderators, which future research should aim to identify (e.g. characteristics of participants at baseline, treatment of the control groups, quality of training of walk leaders). It is also worth noting that the moderator analyses reported were based on the entire set of studies, not just those of higher quality, due to the limited number of studies identified. Thus, it was possible that the results of some moderator analyses may have been affected by the moderating variables being associated with other variables responsible for heterogeneity of these studies (e.g. design, measures, etc.). However, the sensitivity analyses indicated that although the association between study quality and study physical activity effect size was significant (p = 0.05), it was not of sufficient size to be responsible for the results of the moderator analyses reported.
The outcome of this review might be limited by only five of the 19 studies having an objective measure of physical activity change (i.e. pedometer). However, two of them they were RCTs and all of them reported significant changes in physical activity, suggesting that the quality of outcome measure was not having a large effect on study outcome.
To our knowledge, this is the first systematic review and meta-analysis which has attempted to investigate whether interventions to promote walking in groups are efficacious and what are the characteristics of studies that are associated with being efficacious at promoting physical activity. The present review not only provides good evidence of behaviour change outcomes but also of the characteristics of these interventions that are associated larger changes in behaviour. Based on this, further recommendations on how walking in groups interventions could be more efficacious can be formed.
Implications for policy and practice
Taking into consideration the health benefits of physical activity [8] and the benefits of group interventions to target more people than individually based interventions, it seems worth considering devoting resources to designing and implementing interventions to promote walking in groups.
Interventions that had measures from baseline up to six months had significantly lower effect sizes than interventions that had measures over six months. This finding is not consistent with previous research, which suggests that maintenance of behavioral changes in long-term is challenging [12, 72]. The findings of the present review are therefore promising and support the idea that walking interventions which provide social support relationships for behaviour change may lead to greater maintenance of behaviour change [73]. Recent research using an objective measure of long-term maintenance at walking groups, suggested that participants maintain attendance at walking in groups for a long period of time when they have high self-efficacy and their outcomes expectations have been satisfied by the walking group intervention [74]. Thus future interventions might consider addressing participants’ self-efficacy and satisfying their outcome expectations in order to achieve long-term attendance at the behaviour change interventions.
Interventions that targeted both genders produced significantly higher effects on physical activity, compared with interventions that targeted only women. Unfortunately, we have no separate outcomes for men only to allow us comparison between women only and men only groups. Despite this, given the evidence about men’s low participation in walking groups [9], it is encouraging that interventions to promote walking in groups for both genders are more efficacious than interventions that target only women. Future interventions could assess men’s preferences for walking groups and tailor the interventions to their needs. This might attract more men at walking groups and promote the health benefits derived from walking groups to both genders.
Interventions that targeted older adults were found to be more efficacious than those that targeted younger adults. Although only seven of the 19 studies of this review targeted older adults they seem to be more efficacious than interventions that targeted younger adults. It has been estimated that more than half of the participants on led walks around UK are 65 and over [9], thus the results of this review indicates that this population benefits more from walking group interventions in terms of physical activity effects. This is a promising finding taking into account the growing proportion of people aged over 60 years and the challenge of public health to maximize the health and functional capacity of this population.
Interventions delivered by professionals were found not to have significant different effects than interventions delivered by lay people. This finding is in agreement with previous review on self-management interventions [75], suggesting that lay people when sufficiently trained can produce positive changes on walkers’ physical activity. Thus it might be worth training lay people on how to effectively deliver interventions to promote walking in groups.
Unanswered questions
Taking into consideration the deficiencies of primary studies, there is a need for studies of best quality, namely RCTs with objective and long-term measures of behavioral outcomes.
It is important to highlight that the results of this review with meta-analysis present evidence about the efficacy of interventions to promote walking in groups but no clear evidence is being supported about the effectiveness of these interventions outside research studies. More pragmatic research, with more reliable ways of measuring outcome effects in the long-term and more rigorous designs is needed to give an answer to whether and how long-term behaviour change can be achieved in real world. Identifying those intervention components important for short-term and long-term behaviour change would be worth considering. Moreover, future studies should test whether these interventions are cost-effective.
Endnote
aAll data from original search was extracted by two independent researchers, but only first author extracted data from five additional studies added following an update and extended search after revision.
Abbreviations
- RCT:
-
Randomized control trial
- CAPSPAQ:
-
Cross cultural activity participation study physical activity questionnaire
- IPAQ:
-
International physical activity questionnaire
- MLPAQ:
-
Minnesota leisure time physical activity questionnaire
- YPAS:
-
Yale physical activity survey
- AIMS:
-
Arthritis impact measurement scale
- WfH:
-
Walking for health
- CI:
-
Confidence intervals.
References
UK Department of Health: At least five a week: evidence on the impact of physical activity and its relationship to health. A report from the Chief Medical Officer. 2004, UK Department of Health, London
Physical Activity Guidelines Advisory Committee: Physical Activity Guidelines Advisory Committee Report, 2008. 2008, US Department of Health and Human Services, Washington, DC
UK Department of Health: Start Active, stay active. A report on physical activity for health from four home countries’ Chief Medical Officer. 2011, UK Department of Health, London
US Department of Health and Human Services: Physical Activity Guidelines for Americans. Be Active, Healthy and Happy. 2008, US Department of Health and Human Services, Washington
Health Survey for England: Physical activity and fitness. 2009, NHS Information Centre for health and social care, London
Healthy People Gov. Physical Activity: A Federal Government Web site managed by the U.S. Department of Health and Human Services. http://healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicid=33 accessed November, 2011
Morris JN, Hardman AE: Walking to health. Sports Med. 1997, 23: 306-332. 10.2165/00007256-199723050-00004.
Murphy MH, Nevill AM, Murtagh EM, Holder RL: The effect of walking on fitness, fatness and resting blood pressure: A meta-analysis of randomised, controlled trials. Prev Med. 2007, 44: 377-385. 10.1016/j.ypmed.2006.12.008.
Walking for Health: Key statistics Walking for Health. A web site managed by Natural England, http://www.walkingforhealth.org.uk/our-work/key-statistics accessed 2 October, 2012
American Volkssport Association: American Volkssport Association, fun, fitness, friendship. http://www2.ava.org/ accessed 2 October, 2012
Foster C, Hillsdon M, Thorogood M: Interventions for promoting physical activity. Cochrane Database Syst Rev. 2005, 25 (Issue 1): Art. No.: CD003180-10.1002/14651858.CD003180.pub2.
Ogilvie D, Foster CE, Rothnie H, et al: Interventions to promote walking: systematic review. BMJ. 2007, 334 (7605): 1204-1207. 10.1136/bmj.39198.722720.BE.
Fisher KJ, Li F: A Community-Based Walking Trial to Improve Neighbourhood Quality of Life in Older Adults: A Multilevel Analysis. Ann Behav Med. 2004, 28 (3): 186-194. 10.1207/s15324796abm2803_7.
Ferreira SRG, Gimeno SGA, Hirai AT, et al: Effects of an intervention in eating habits and physical activity in Japanese-Brazilian women with a high prevalence of metabolic syndrome in Bauru, São Paulo State, Brazil. Cad Saude Publica. 2008, 24 (Suppl2): S294-S302.
Lamb SE, Bartlett HP, Ashley A, et al: Can lay-led walking programmes increase physical activity in middle aged adults? A randomised controlled trial. J Epidemiol Community Health. 2002, 56 (4): 246-252. 10.1136/jech.56.4.246.
Negri C, Bacchi E, Morgante S, et al: Supervised walking groups to increase physical activity in type 2 diabetic patients. Diabetes Care. 2010, 33: 2333-2335. 10.2337/dc10-0877.
O’Halloran PD: Mood Changes in Weeks 2 and 6 of a Graduated Group Walking Program in Previously Sedentary People with Type 2 Diabetes. Aust J Prim Health. 2007, 13 (1): 68-73.
Lorentzen C, Ommundsen Y, Jenum AK, et al: The “Romsas in Motion” community intervention: mediating effects of psychosocial factors on forward transition in the stages of change in physical activity. Health Educ Behav. 2009, 36: 348-365.
Lorentzen C, Ommundsen Y, Jenum AK, et al: The “Romsas in Motion” community intervention: program exposure and psychosocial mediated relationships to change in stages of change in physical activity. Int J Behav Nutr Phys Act. 2007, 4: 13-19. 10.1186/1479-5868-4-13.
Warren BC, Maley M, Sugarwala LS, et al: Small steps are easier together: A goal- based intervention to increase walking by women in rural worksites. Prev Med. 2010, 50: 230-234. 10.1016/j.ypmed.2010.02.006.
Li F, Fisher KJ, Harmer P: Improving physical function and blood pressure in older adults through cobblestone mat walking: a randomized trial. J Am Geriatr Soc. 2005, 53 (8): 1305-1312. 10.1111/j.1532-5415.2005.53407.x.
Dishman RK, DeJoy DM, Wilson MG, et al: Move to Improve: a randomized workplace trial to increase physical activity. Am J Prev Med. 2009, 36 (2): 133-141. 10.1016/j.amepre.2008.09.038.
Duru KO, Sarkision CA, Legn M, Sisters in Motion, et al: A randomised controlled trials of a faith-based physical activity intervention. JAGS. 2010, 58 (10): 1863-1869. 10.1111/j.1532-5415.2010.03082.x.
Woolf-May K, Bird S, Owen A: Effects of an 18 week walking programme on cardiac function in previously sedentary or relatively inactive adults. Br J Sports Med. 1997, 31 (1): 48-53. 10.1136/bjsm.31.1.48.
Caperchione C, Mummery K: Psychosocial mediators of group cohesion on physical activity intention of older adults. Psychol Health Med. 2007, 12 (1): 81-93. 10.1080/13548500600768254.
MacMillan F, Fritzisimos C, Black K, West end walkers 65+, et al: a randomised controlled trial of primary care-based walking intervention for older adults: study rationale and design. BMC Publ Health. 2011, 11: 120-232. 10.1186/1471-2458-11-120.
Sarkisian CA, Prohaska T, Davis C, et al: Pilot test of an attribution retraining intervention to raise walking levels in sedentary older adults. JAGS. 2007, 55 (11): 1842-1846. 10.1111/j.1532-5415.2007.01427.x.
Burke S, Carron A, Eys M, et al: Group versus individual approach? A meta-analysis of the effectiveness of interventions to promote physical activity. Sport Exerc Psy Rev. 2006, 2 (1): 19-35.
Carron AV, Hausenblas HA, Mack D: Social influence and exercise: A meta-analysis. JSEP. 1996, 18 (1): 1-16.
Williams DM, Matthews CE, Rutt C, et al: Interventions to increase walking behaviour. Med Sci Sports Exerc. 2008, 40 (7): S567-S573.
Cohen J: Statistical power analysis for behaviour sciences. 1977, Academic Press, New York
Schwarzer R: Meta-analysis programs. 1989, http://userpage.fu-berlin.de/~health/meta_e.htm accessed December, 2009
Kulinskaya E, Dollinger MB, Bjorkestol K: Testing for Homogeneity in Meta-analysis I. The One-Parameter Case: Standardized Mean Difference. Biometrics. 2011, 67: 203-212. 10.1111/j.1541-0420.2010.01442.x.
Rosenthal R: Meta-analytic procedures for social research. 1984, Sage, Beverly Hills, CA, US
Ryan R, Hill S, Prictor M, McKenzie J: Cochrane Consumers and Communication Review Group. Study Quality Guide. http://www.latrobe.edu.au/chcp/assets/downloads/StudyQualityGuideMay2011.pdf accessed May, 2011
Kriska AM, Bayles C, Cauley JA, et al: A Randomized Exercise Trial in Older Women: Increased Activity Over Two Years and the Factors Associated with Compliance. Med Sci Sports Exerc. 1986, 18 (5): 557-562.
McAuley E, Courneya KS, Rudolph DL, Lox CL: Enhancing Exercise Adherence in Middle-Aged Males and Females. Prev Med. 1994, 23 (4): 498-506. 10.1006/pmed.1994.1068.
Rogers TM: Effectiveness of a Walking Club and a Self-Directed Physical Activity Program in Increasing Moderate Intensity Physical Activity among African-American Females. 1997, Microform Publications, University of Oregon, United States, PhD thesis
Sullivan T, Allegrante JP, Peterson MG, et al: One-Year Followup of Patients with Osteoarthritis of the Knee Who Participated in a Program of Supervised Fitness Walking and Supportive Patient Education. Arthritis Care and Res. 1998, 11 (4): 228-233. 10.1002/art.1790110403.
Resnick B: Testing the Effect of the WALC Intervention on Exercise Adherence in Older Adults. J Gerontol Nurs. 2002, 28 (6): 40-49.
Coull AJ, Taylor VH, Elton R, et al: A Randomised Controlled Trial of Senior Lay Health Mentoring in Older People with Ischaemic Heart Disease: The Braveheart Project. Age and Ageing. 2004, 33 (4): 348-354. 10.1093/ageing/afh098.
Nguyen M, Gauvin L, Martineau I, et al: Promoting Physical Activity at the Community Level: Insights into Health Promotion Practice from the Laval Walking Clubs Experience. Health Promotion Pract. 2002, 3 (4): 485-496. 10.1177/152483902236718.
Staten LK, Scheu LL, Bronson D, et al: Pasos Adelante: The Effectiveness of a Community-Based Chronic Disease Prevention Program. Prev Chronic Dis. 2005, 2 (1): A18-A18.
Banks-Wallace J: Outcomes from Walk the Talk: A Nursing Intervention for Black Women. ABNF Journal. 2007, 18 (1): 19-24.
Hogue PA: The effects of buddy support on physical activity in African American women. 2007, Thesis dissertation. University of Toledo, US
Estabrooks PA, Bradshaw M, Dzewaltowski DA, et al: Determining the Impact of Walk Kansas: Applying a Team-Building Approach to Community Physical Activity Promotion. Ann Behav Med. 2008, 36 (1): 1-12. 10.1007/s12160-008-9040-0.
Jancey JM, Lee AH, Howat PA, et al: The Effectiveness of a Physical Activity Intervention for Seniors. Am J Health Prom. 2008, 22 (5): 318-321. 10.4278/ajhp.22.5.318.
Krieger J, Rabkin J, Sharify D, et al: High Point Walking for Health: Creating Built and Social Environments that Support Walking in a Public Housing Community. Am J Public Health. 2009, 99: S593-S599. 10.2105/AJPH.2009.164384.
Zoellner J, Connell C, Powers A, et al: Does a Six-Month Pedometer Intervention Improve Physical Activity and Health Among Vulnerable African American? A feasibility Study. J Phys Act Health. 2010, 7: 224-231.
Takeda N, Koichiro O, Sakai K, et al: The Effects of a Group-Based Walking Program on Daily Physical Activity in Middle-Aged and Older Adults. Int J Sport Health Sci. 2011, 9: 39-48.
Lee RE, O’Connor DP, Smith-Ray R, et al: Mediating Effects of Group Cohesion on Physical Activity and Diet in Women of Color: Health is Power. Am J Health Promot. 2012, 26 (4): e116-e125. 10.4278/ajhp.101215-QUAN-400.
Maki Y, Ura C, Yamaguchi T, et al: Effects of Intervention Using a Community- Based Walking Program for Prevention of Mental Decline: A Randomized Controlled Trial. JAGS. 2012, 60: 505-510. 10.1111/j.1532-5415.2011.03838.x.
Thomas GN, Macfarlane DJ, Guo B, et al: Health Promotion in Older Chinese: A 12-Month Cluster Randomized Controlled Trial of Pedometry and “Peer Support”. Med Sci Sport Exer. 2012, 10.1249/MSS.0b013e318244314a.
Hunter JE, Schmidt FL, Jackson GB: Meta-analysis. Cumulating research findings across studies. 1982, Sage, Beverly Hills, US
Nguyen MN, Gauvin L, Martineau I, et al: Sustainability of the Impact of a Public Health Intervention: Lessons Learned from the Laval Walking Clubs Experience. Health Promotion Pract. 2005, 6 (1): 44-52. 10.1177/1524839903260144.
Pereira MA, Kriska AM, Day RD, et al: A Randomized Walking Trial in Postmenopausal Women: Effects on Physical Activity and Health 10 Years Later. Archiv Intern Med. 1998, 158 (15): 1695-1701. 10.1001/archinte.158.15.1695.
McAuley E, Jerome GJ, Marquez DX, et al: Exercise Self-Efficacy in Older Adults: Social, Affective, and Behavioral Influences. Ann Behav Med. 2003, 25 (1): 1-7. 10.1207/S15324796ABM2501_01.
Fisher KJ, Li F, Michael Y, et al: Neighborhood-Level Influences on Physical Activity among Older Adults: A Multilevel Analysis. J Aging Phys Act. 2004, 12 (1): 45-63.
Fisher KJ, Pickering MA, Li F: Healthy Aging through Active Leisure: Design and Methods of SHAPE - a Randomized Controlled Trial of a Neighborhood-Based Walking Project. World Leisure Journal. 2002, 44 (1): 19-28. 10.1080/04419057.2002.9674257.
Michael YL, Carlson NE: Analysis of Individual Social-Ecological Mediators and Moderators and their Ability to Explain Effect of a Randomized Neighbourhood Walking Intervention. Int J Behav Nutr Phys Act. 2009, 30 (6): 6-49.
Rowland RM, Fisher KJ, Green M, et al: Recruiting Inactive Older Adults to a Neighborhood Walking Trial: The SHAPE Project. J Aging Stud. 2004, 18 (3): 353-368. 10.1016/j.jaging.2004.03.001.
Banks-Wallace J, Conn V: Changes in Steps Per Day Over the Course of a Pilot Walking Intervention. ABNF Journal. 2005, 16 (2): 28-32.
Burke SM, Shapcott KM, Carron AV, et al: Group Goal Setting and Group Performance in a Physical Activity Context. IJSEP. 2010, 8 (3): 245-261.
Jancey JM, Clarke A, Howat PA, et al: A Physical Activity Program to Mobilize Older People: A Practical and Sustainable Approach. Gerontologist. 2008, 48 (2): 251-257. 10.1093/geront/48.2.251.
Jancey J, Howat P, Lee A, et al: Effective Recruitment and Retention of Older Adults in Physical Activity Research: PALS Study. Perth Active Living Seniors Project (PALS). Am J Health Behav. 2006, 30 (6): 626-635. 10.5993/AJHB.30.6.9.
Jancey J, Lee A, Howat P, et al: Reducing Attrition in Physical Activity Programs for Older Adults. J Aging Phys Act. 2007, 15 (2): 152-165.
Jancey J, Lee A, Howat P, et al: The Effectiveness of a Walking Booster Program for Seniors. Am J Health Promot. 2011, 25 (6): 363-367. 10.4278/ajhp.090512-ARB-164.
Zoellner J, Connell CL, Santell R, et al: Fit for Life Steps: Results of a Community Walking Intervention in the Rural Mississippi Delta. Prog Community Health Partnersh. 2007, 1 (1): 49-60. 10.1353/cpr.0.0009.
Zoellner J, Powers A, Avis-Williams A, et al: Compliance and Acceptability of Maintaining a 6-Month Pedometer Diary in a Rural, African American Community- Based Walking Intervention. J Phys Act Health. 2009, 6: 475-482.
Zoellner J, Connell C, Madson M, et al: H.U.B city steps: Methods and Early Findings from a community-based Participatory Research Trial to Reduce Blood Pressure among African Americans. IJBNPA. 2011, 8: 59-71.
Powers A: A Comprehensive Process Evaluation of a Community Based Participatory Research Intervention, Fit for Life Steps. 2007, University of Southern Mississippi, US, Thesis dissertation
Bravata DM, Smith-Spangler C, Sundaram V, et al: Using pedometers to increase physical activity and improve health: a systematic review. JAMA. 2007, 298 (19): 2296-2304. 10.1001/jama.298.19.2296.
Rothman AJ: Toward a Theory-Based Analysis of Behavioral Maintenance. Health Psychol. 2000, 19 (1): 64-69.
Kassavou A: Building an Evidence Base for Effective Walking Groups. 2012, Coventry University, UK, PhD Thesis
Foster G, Taylor SJC, Eldridge SE, et al: Self-management education programmes by lay leaders for people with chronic conditions. Cochrane Database Syst Rev. 2007, 17 (4): Art No.: CD005108-10.1002/14651858.CD005108.pub2.
Acknowledgements
The authors thank Claire Taylor for double coding the articles and Paolo Moghetti, Paul Estabrooks, Albert Carron, Michael Perri, Andrew Coull, Rodney Dishman, Nicole Culos-Reed, Neville Owen and Janet Curie, Barbour Waren, Cecille Thogersen-Ntoumani for their replies on queries about their studies. This research was funded by a Coventry University (Faculty of Health and Life Sciences) PhD studentship for the first author, supervised by the other authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
Authors’ contributions
AK and DF designed the study. AK identified the eligibility criteria, conducted the searches, also data extraction and analyses, and drafted the manuscript. DF participated in decisions regarding eligibility criteria and supervised data analyses and drafting the manuscript. AT participated in its coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Competing interest
The authors declare that they have no competing interest.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Kassavou, A., Turner, A. & French, D.P. Do interventions to promote walking in groups increase physical activity? A meta-analysis. Int J Behav Nutr Phys Act 10, 18 (2013). https://doi.org/10.1186/1479-5868-10-18
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1479-5868-10-18